
Effect of Cavity Disinfectants on Adhesion to Primary Teeth—A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
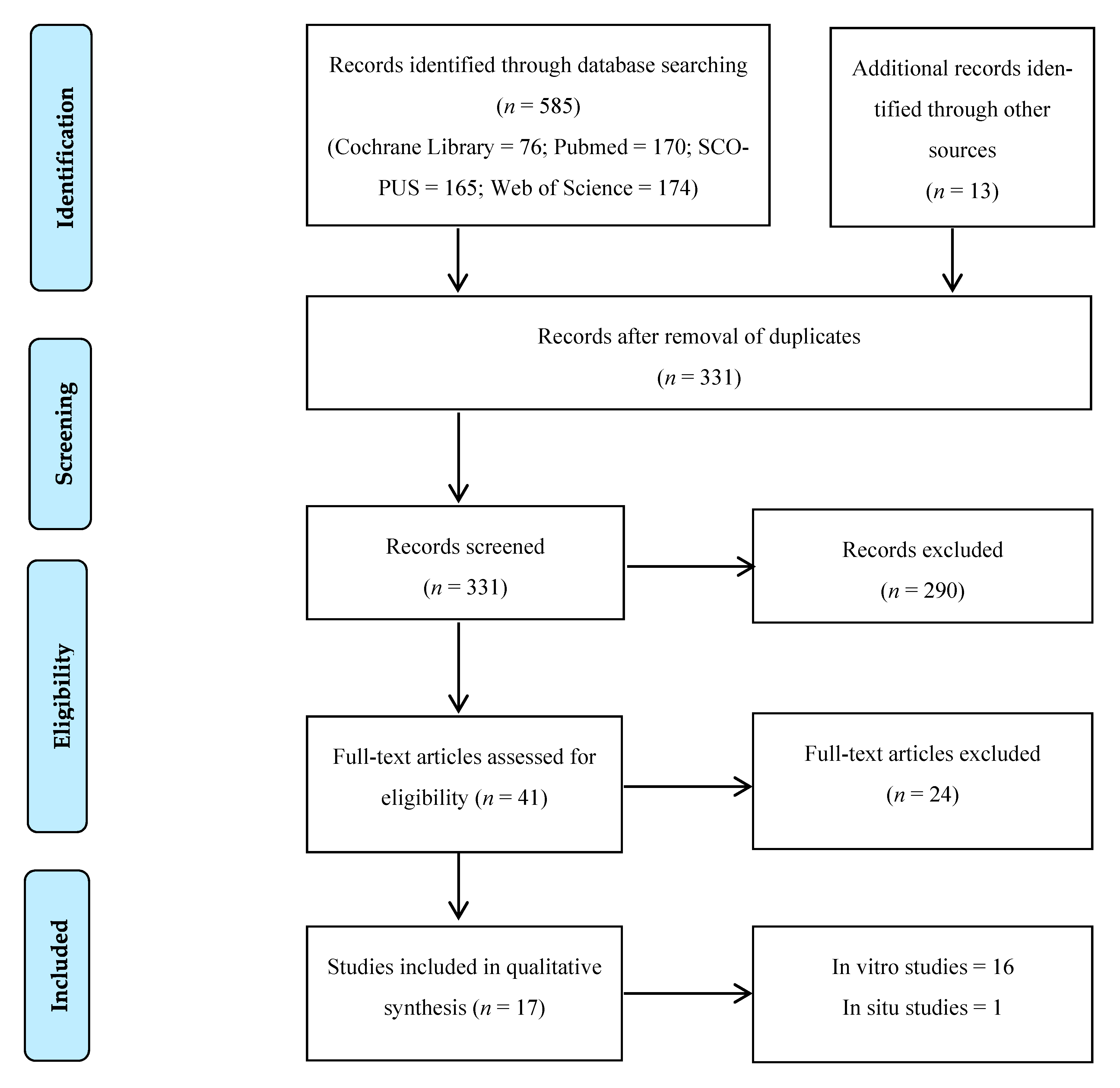
2. Results
Quality Assessment
3. Discussion
4. Materials and Methods
Quality Assessment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askar, H.; Krois, J.; Göstemeyer, G.; Bottenberg, P.; Zero, D.; Banerjee, A.; Schwendicke, F. Secondary caries: What is it, and how it can be controlled, detected, and managed? Clin. Oral Investig. 2020, 24, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Singhal, D.K.; Acharya, S.; Thakur, A.S. Microbiological analysis after complete or partial removal of carious dentin using two different techniques in primary teeth: A randomized clinical trial. Dent. Res. J. 2016, 13, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.H.; Loesche, W.J.; Charbeneau, G.T. Bacteriologic study of a basic fuchsin caries-disclosing dye. J. Prosthet. Dent. 1985, 54, 51–55. [Google Scholar] [CrossRef]
- Dalkilic, E.E.; Arisu, H.D.; Kivanc, B.H.; Uctasli, M.B.; Omurlu, H. Effect of different disinfectant methods on the initial microtensile bond strength of a self-etch adhesive to dentin. Lasers Med. Sci. 2012, 27, 819–825. [Google Scholar] [CrossRef]
- Elkassas, D.W.; Fawzi, E.M.; Zohairy, A. The effect of cavity disinfectants on the micro-shear bond strength of dentin adhesives. Eur. J. Dent. 2014, 8, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Say, E.C.; Koray, F.; Tarim, B.; Soyman, M.; Gülmez, T. In vitro effect of cavity disinfectants on the bond strength of dentin bonding systems. Quintessence Int. 2004, 35, 56–60. [Google Scholar]
- Hiraishi, N.; Yiu, C.K.Y.; King, N.M.; Tay, F.R. Effect of 2% chlorhexidine on dentin microtensile bond strengths and nanoleakage of luting cements. J. Dent. 2009, 37, 440–448. [Google Scholar] [CrossRef]
- Colares, V.; Franca, C.; Filho, H.A.A. O tratamento restaurador atraumático nas dentições decídua e permanente. Rev. Port. Estomatol. Med. Dentária Cir. Maxilofac. 2009, 50, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Suma, N.K.; Shashibhushan, K.K. Effect of Dentin Disinfection with 2% Chlorhexidine Gluconate and 0.3% Iodine on Dentin Bond Strength: An in vitro Study. Int. J. Clin. Pediatric Dent. 2017, 10, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Vieira, R.S.; Silva, I.A. Bond strength to primary tooth dentin following disinfection with a chlorhexidine solution: An in vitro study. Pediatric Dent. 2003, 25, 49–52. [Google Scholar]
- Franzon, R.; Opdam, N.J.; Guimarães, L.F.; Demarco, F.F.; Casagrande, L.; Haas, A.N.; Araújo, F.B. Randomized controlled clinical trial of the 24-months survival of composite resin restorations after one-step incomplete and complete excavation on primary teeth. J. Dent. 2015, 43, 235–1241. [Google Scholar] [CrossRef] [PubMed]
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J.M. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Sande, F.H.; Collares, K.; Correa, M.B.; Cenci, M.S.; Demarco, F.F.; Opdam, N. Restoration Survival: Revisiting Patients’ Risk Factors through a Systematic Literature Review. Oper. Dent. 2016, 41, S7–S26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correr, G.M.; Puppin-Rontani, R.M.; Correr-Sobrinho, L.; Sinhoret, M.A.C.; Consani, S. Effect of sodium hypochlorite on dentin bonding in primary teeth. J. Adhes. Dent. 2004, 6, 307–312. [Google Scholar] [PubMed]
- Monghini, E.M.; Wanderley, R.L.; Pécora, J.D.; Dibb, P.R.G.; Corona, S.A.M.; Borsatto, M.C. Bond Strength to Dentin of Primary Teeth Irradiated with Varying Er: YAG Laser Energies and SEM Examination of the Surface Morphology. Lasers Surg. Med. 2004, 34, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Ersin, N.K.; Candan, U.; Aykut, A.; Eronat, C.; Belli, S. No Adverse Effect to Bonding Following Caries. J. Dent. Child. 2009, 76, 20–27. [Google Scholar]
- Ricci, H.A.; Sanabe, M.E.; Costa, C.A.S.; Hebling, J. Effect of chlorhexidine on bond strength of two-step etch-and-rinse adhesive systems to dentin of primary and permanent teeth. Am. J. Dent. 2010, 23, 128–132. [Google Scholar]
- Leitune, V.C.B.; Portella, F.F.; Bohn, P.V.; Collares, F.M.; Samuel, S.M.W. Influence of chlorhexidine application on longitudinal adhesive bond strength in deciduous teeth. Braz. Oral Res. 2011, 25, 388–392. [Google Scholar] [CrossRef] [Green Version]
- Scatena, C.; Torres, C.P.; Gomes-Silva, J.M.; Contente, M.; Pécora, J.D.; Palma-Dibb, R.G.; Borsatto, M.C. Shear strength of the bond to primary dentin: Influence of Er: YAG laser irradiation distance. Lasers Med. Sci. 2011, 26, 293–297. [Google Scholar] [CrossRef]
- Lenzi, T.L.; Tedesco, T.K.; Soares, F.Z.M.; Loguercio, A.D.; Rocha, R.O. Chlorhexidine does not increase immediate bond strength of etch-and-rinse adhesive to caries-affected dentin of primary and permanent teeth. Braz. Dent. J. 2012, 23, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Lenzi, T.L.; Tedesco, T.K.; Soares, F.Z.M.; Loguercio, A.D.; Rocha, R.O. Chlorhexidine application for bond strength preservation in artificially-created caries-affected primary dentin. Int. J. Adhes. Adhes. 2014, 54, 51–56. [Google Scholar] [CrossRef]
- Aras, S.; Küçükeçmen, H.C.; Öaroǧlu, S.I. Deproteinization treatment on bond strengths of primary, mature and immature permanent tooth enamel. J. Clin. Pediatric Dent. 2013, 37, 275–280. [Google Scholar] [CrossRef]
- Oznurhan, F.; Ozturk, C.; Ekci, E.S. Effects of different cavity-disinfectants and potassium titanyl phosphate laser on microtensile bond strength to primary dentin. Niger. J. Clin. Pract. 2015, 18, 400–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yildiz, E.; Karaarslan, E.S.; Simsek, M.; Cebe, F.; Ozsevik, A.S.; Ozturk, B. Effect of a re-wetting agent on bond strength of an adhesive to primary and permanent teeth dentin after different etching techniques. Niger. J. Clin. Pract. 2015, 18, 364–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahrololoomi, Z.; Dadkhah, A.; Alemrajabi, M. The Effect of Er: YAG laser irradiation and different concentrations of sodium hypochlorite on shear bond strength of composite to primary teeth’s dentin. J. Lasers Med. Sci. 2017, 8, 29–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebrahimi, M.; Naseh, A.; Abdollahi, M.; Shirazi, A.S. Can chlorhexidine enhance the bond strength of self-etch and etch-and-rinse systems to primary teeth dentin? J. Contemp. Dent. Pract. 2018, 19, 404–408. [Google Scholar]
- Mohammadi, N.; Parsaie, Z.; Jafarpour, D.; Bizolm, F. Effect of different matrix metalloproteinase inhibitors on shear bond strength of composite attached to primary teeth dentin. Eur. J. Gen. Dent. 2020, 9, 147–151. [Google Scholar] [CrossRef]
- Manfro, A.R.G.; Reis, A.; Loguercio, A.D.; Imparato, J.C.P.; Raggio, D.P. Effect of different concentrations of chlorhexidine on bond strength of primary dentin. Pediatric Dent. 2012, 34, 11E–15E. [Google Scholar]
- Ricci, H.A.; Sanabe, M.E.; Costa, C.A.S.; Pashley, D.H.; Hebling, J. Chlorhexidine increases the longevity of in vivo resin-dentin bonds. Eur. J. Oral Sci. 2010, 118, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Jowkar, Z.; Farpour, N.; Koohpeima, F.; Mokhtari, M.J.; Shafiei, F. Effect of silver nanoparticles, zinc oxide nanoparticles and titanium dioxide nanoparticles on microshear bond strength to enamel and dentin. J. Contemp. Dent. Pract. 2018, 19, 1405–1412. [Google Scholar]
- Koutsi, V.; Noonan, R.G.; Horner, J.A.; Simpson, M.D.; Matthews, W.G.; Pashley, D.H. The effect of dentin depth on the permeability and ultrastructure of primary molars. Pediatric Dent. 1994, 16, 29–35. [Google Scholar]
- Dourda, A.O.; Moule, A.J.; Young, W.G. A morphometric analysis of the cross-sectional area of dentine occupied by dentinal tubules in human third molar teeth. Int. Endod. J. 1994, 27, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, M.; Ohno, H.; Endo, K.; Kaga, M.; Sano, H.; Oguchi, H. The effect of hybrid layer thickness on bond strength: Demineralized dentin zone of the hybrid layer. Dent. Mater. 2000, 16, 406–411. [Google Scholar] [CrossRef]
- Angker, L.; Nockolds, C.; Swain, M.V.; Kilpatrick, N. Quantitative analysis of the mineral content of sound and carious primary dentine using BSE imaging. Arch. Oral Biol. 2004, 49, 99–107. [Google Scholar] [CrossRef]
- Nor, J.; Dennison, J.; Edwardsa, C.; Feigal, R. Dentin bonding: SEM comparison teeth. Am. Acad. Pediatric Dent. 1997, 19, 246–252. [Google Scholar]
- Sung, E.C.; Chenard, T.; Caputo, A.A.; Amodeo, M.; Chung, E.M.; Rizoiu, I.M. Composite resin bond strength to primary dentin prepared with ER, CR: YSSG laser. J. Clin. Pediatric Dent. 2005, 30, 45–50. [Google Scholar] [CrossRef] [Green Version]
- ISO/TS 11405:2015 Dental Materials—Testing of Adhesion to Tooth Structure; International Organisation for Standardization: Geneva, Switzerland, 2015.
- Uceda-Gómez, N.; Reis, A.; Carrilho, M.R.O.; Loguercio, A.D.; Filho, L.E.R. Effect of sodium hypochlorite on the bond strength of an adhesive system to superficial and deep dentin. J. Appl. Oral Sci. 2003, 11, 223–228. [Google Scholar] [CrossRef]
- Ramos, R.P.; Chimello, D.T.; Chinelatti, M.A.; Nonaka, T.; Pécora, J.D.; Dibb, R.G.P. Effect of Er: YAG laser on bond strength to dentin of a self-etching primer and two single-bottle adhesive systems. Lasers Surg. Med. 2002, 31, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.H.; Zhang, L.; Yu, F.; Li, F.; Liu, Z.Y.; Chen, J.H. Epigallocatechin-3-gallate and Epigallocatechin-3-O-(3-O-methyl)-gallate Enhance the Bonding Stability of an Etch-and-Rinse Adhesive to Dentin. Materials 2017, 10, 183. [Google Scholar] [CrossRef] [PubMed]
- Pashley, D.H.; Carvalho, R.M. Dentine permeability and dentine adhesion. J. Dent. 1997, 25, 355–372. [Google Scholar] [CrossRef]
- Pashley, E.L.; Talman, R.; Horner, J.A.; Pashley, D.H. Permeability of normal versus carious dentin. Dent. Traumatol. 1991, 7, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Swift, E.J.J. Dentin/enamel adhesives: Review of the literature. Pediatric Dent. 2002, 24, 456–461. [Google Scholar]
- Powers, J.M.; O’Keefe, K.L.; Pinzon, L.M. Factores affecting in vitro bond strength of bonding agents to human dentin. Odontology 2003, 91, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.M.; Mendonça, J.S.; Santiago, S.L.; Silveira, R.R.; Garcia, F.C.P.; Tay, F.R.; Pashley, D.H. Effects of HEMA/Solvent combinations on bond strength to dentin. J. Dent. Res. 2003, 82, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, L.; Zhu, J.; Yang, J.; Zhu, H. Impact of dentinal tubule orientation on dentin bond strength. Curr. Med. Sci. 2018, 38, 721–726. [Google Scholar] [CrossRef]
- Lima, D.M.; Candido, M.S.M. Effect of dentin on the shear bond strength of different adhesive systems. Rev. Gaúcha Odontol. 2012, 60, 149–161. [Google Scholar]
- Santana, F.R.; Pereira, J.C.; Pereira, C.A.; Neto, F.A.J.; Soares, C.J. Influence of method and period of storage on the microtensile bond strength of indirect composite resin restorations to dentine. Braz. Oral Res. 2008, 22, 352–357. [Google Scholar] [CrossRef] [Green Version]
- ISO 3696:1987—Water for Analytical Laboratory Use—Specification and Test Methods; International Organisation for Standardization: Geneva, Switzerland, 1987.
- Kang, H.J.; Moon, H.J.; Shin, D.H. Effect of different chlorhexidine application times on microtensile bond strength to dentin in Class I cavities. Restor. Dent. Endod. 2012, 37, 9. [Google Scholar] [CrossRef]
- Coelho, A.; Paula, A.; Carrilho, T.; Silva, M.J.; Botelho, M.F.; Carrilho, E. Chlorhexidine mouthwash as an anticaries agent: A systematic review. Quintessence Int. 2017, 48, 585–591. [Google Scholar]
- Haydari, M.; Bardakci, A.G.; Koldsland, O.C.; Aass, A.M.; Sandvik, L.; Preus, H.R. Comparing the effect of 0.06%, 0.12% and 0.2% Chlorhexidine on plaque, bleeding and side effects in an experimental gingivitis model: A parallel group, double masked randomized clinical trial. BMC Oral Health 2017, 17, 1–8. [Google Scholar] [CrossRef]
- Kandaswamy, S.K.; Sharath, A.; Priya, P.G. Comparison of the Effectiveness of Probiotic, Chlorhexidine-based Mouthwashes, and Oil Pulling Therapy on Plaque Accumulation and Gingival Inflammation in 10- to 12-year-old Schoolchildren: A Randomized Controlled Trial. Int. J. Clin. Pediatric Dent. 2018, 11, 66–70. [Google Scholar] [CrossRef]
- Hebling, J.; Pashley, D.H.; Tjäderhane, L.; Tay, F.R. Chlorhexidine arrests subclinical degradation of dentin hybrid layers in vivo. J. Dent. Res. 2005, 84, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Pashley, D.H.; Tay, F.R.; Yiu, C.; Hashimoto, M.; Breschi, L.; Carvalho, R.M.; Ito, S. Collagen Degradation by Host-derived Enzymes during Aging. J. Dent. Res. 2004, 83, 216–221. [Google Scholar] [CrossRef]
- Coelho, A.; Amaro, I.; Rascão, B.; Marcelino, I.; Paula, A.; Saraiva, J.; Spagnuolo, G.; Ferreira, M.M.; Marto, C.M.; Carrilho, E. Effect of Cavity Disinfectants on Dentin Bond. Strength and Clinical Success of Composite Restorations—A Systematic Review of In Vitro, In Situ and Clinical Studies. Int. J. Mol. Sci. 2020, 22, 353. [Google Scholar] [CrossRef]
- Pappas, M.; Burns, D.R.; Moon, P.C.; Coffey, J.P. Influence of a 3-step tooth disinfection procedure on dentin bond strength. J. Prosthet. Dent. 2005, 93, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Carrilho, M.R.O.; Carvalho, R.M.; Goes, M.F.; Hipólito, V.; Geraldeli, S.; Tay, F.R.; Pashley, D.H.; Tjäderhane, L. Chlorhexidine preserves dentin bond in vitro. J. Dent. Res. 2007, 86, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salles, M.M.; Badaró, M.M.; Arruda, C.N.F.; Leite, V.; Silva, C.; Watanabe, E.; Oliveira, V.; Paranhos, H. Antimicrobial activity of complete denture cleanser solutions based on sodium hypochlorite and Ricinus communis—A randomized clinical study. J. Appl. Oral Sci. 2015, 23, 637–6342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estrela, C.; Estrela, C.R.A.; Decurcio, D.A.; Hollanda, A.C.B.; Silva, J.A. Antimicrobial efficacy of ozonated water, gaseous ozone, sodium hypochlorite and chlorhexidine in infected human root canals. Int. Endod. J. 2007, 40, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Arslan, S.; Ozbilge, H.; Kaya, E.G.; Er, O. In vitro antimicrobial activity of propolis, BioPure MTAD, sodium hypochlorite, and chlorhexidine on Enterococcus faecalis and Candida albicans. Saudi Med. J. 2011, 32, 479–483. [Google Scholar]
- Cha, H.S.; Shin, D.H. Antibacterial capacity of cavity disinfectants against Streptococcus mutans and their effects on shear bond strength of a self-etch adhesive. Dent. Mater. J. 2016, 35, 147–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahuja, B.; Yeluri, R.; Baliga, S.; Munshi, A.K. Enamel deproteinization before acid etching--a scanning electron microscopic observation. J. Clin. Pediatric Dent. 2010, 35, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Hibst, R.; Keller, U. Experimental studies of the application of the Er: YAG laser on dental hard substances: I. Measurement of the ablation rate. Lasers Surg. Med. 1989, 9, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Franke, M.; Taylor, A.W.; Lago, A.; Fredel, M.C. Influence of Nd: YAG laser irradiation on an adhesive restorative procedure. Oper. Dent. 2006, 31, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Keller, U.; Hibst, R. Experimental studies of the application of the Er: YAG laser on dental hard substances: II. Light microscopic and SEM investigations. Lasers Surg. Med. 1989, 9, 345–351. [Google Scholar] [CrossRef]
- Tokonabe, H.; Kouji, R.; Watanabe, H.; Nakamura, Y.; Matsumoto, K. Morphological changes of human teeth with Er: YAG laser irradiation. J. Clin. Laser Med. Surg. 1999, 17, 7–12. [Google Scholar] [CrossRef]
- Nelson, D.G.; Jongebloed, W.L.; Featherstone, J.D. Laser irradiation of human dental enamel and dentine. N. Z. Dent. J. 1986, 82, 74–77. [Google Scholar]
- Hossain, M.; Nakamura, Y.; Yamada, Y.; Kimura, Y.; Nakamura, G.; Matsumoto, K. Ablation depths and morphological changes in human enamel and dentin after Er: YAG laser irradiation with or without water mist. J. Clin. Laser Med. Surg. 1999, 17, 105–109. [Google Scholar] [CrossRef]
- Armengol, V.; Jean, A.; Rohanizadeh, R.; Hamel, H. Scanning electron microscopic analysis of diseased and healthy dental hard tissues after Er: YAG laser irradiation: In vitro study. J. Endod. 1999, 25, 543–546. [Google Scholar] [CrossRef]
- Gonçalves, M.; Corona, S.A.M.; Palma-Dibb, R.G.; Pécora, J.D. Influence of pulse repetition rate of Er: YAG laser and dentin depth on tensile bond strength of dentin-resin interface. J. Biomed. Mater. Res. 2008, 86, 477–482. [Google Scholar] [CrossRef]
- Ferreira, L.S.; Apel, C.; Francci, C.; Simoes, A.; Eduardo, C.P.; Gutknecht, N. Influence of etching time on bond strength in dentin irradiated with erbium lasers. Lasers Med. Sci. 2010, 25, 849–854. [Google Scholar] [CrossRef]
- Martínez-Insua, A.; Dominguez, L.S.; Rivera, F.G.; Santana-Penín, U.A. Differences in bonding to acid-etched or Er: YAG-laser-treated enamel and dentin surfaces. J. Prosthet. Dent. 2000, 84, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Munck, J.; Meerbeek, B.; Yudhira, R.; Lambrechts, P.; Vanherle, G. Micro-tensile bond strength of two adhesives to Erbium:YAG-lased vs. bur-cut enamel and dentin. Eur. J. Oral Sci. 2002, 110, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Polydorou, O.; Pelz, K.; Hahn, P. Antibacterial effect of an ozone device and its comparison with two dentin-bonding systems. Eur. J. Oral Sci. 2006, 114, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Bocci, V.A. Scientific and medical aspects of ozone therapy. State of the art. Arch. Med. Res. 2006, 37, 425–435. [Google Scholar] [CrossRef]
- Nagayoshi, M.; Kitamura, C.; Fukuizumi, T.; Nishihara, T.; Terashita, M. Antimicrobial effect of ozonated water on bacteria invading dentinal tubules. J. Endod. 2004, 30, 778–781. [Google Scholar] [CrossRef]
- Baysan, A.; Lynch, E. Effect of ozone on the oral microbiota and clinical severity of primary root caries. Am. J. Dent. 2004, 17, 56–60. [Google Scholar] [PubMed]
- Baysan, A.; Whiley, R.A.; Lynch, E. Antimicrobial effect of a novel ozone-generating device on micro-organisms associated with primary root carious lesions in vitro. Caries Res. 2000, 34, 498–501. [Google Scholar] [CrossRef]
- Castillo, A.; Galindo-Moreno, P.; Avila, G.; Valderrama, M.; Liébana, J.; Baca, P. In vitro reduction of mutans streptococci by means of ozone gas application. Quintessence Int. 2008, 39, 827–831. [Google Scholar]
- Fagrell, T.G.; Dietz, W.; Lingström, P.; Steiniger, F.; Norén, J.G. Effect of ozone treatment on different cariogenic microorganisms in vitro. Swed. Dent. J. 2008, 32, 139–147. [Google Scholar] [PubMed]
- Wang, J.; Song, W.; Zhu, L.; Wei, X. A comparative study of the microtensile bond strength and microstructural differences between sclerotic and Normal dentine after surface pretreatment. BMC Oral Health 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.M.; Agee, K.; Sidow, S.; McNally, K.; Lindsey, K.; Borke, J.; Elsalanty, M.; Tay, F.R. Inhibition of endogenous dentin matrix metalloproteinases by ethylenediaminetetraacetic acid. J. Endod. 2012, 38, 62–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youm, S.H.; Jung, K.H.; Son, S.A.; Kwon, Y.H.; Park, J.K. Effect of dentin pretreatment and curing mode on the microtensile bond strength of self-adhesive resin cements. J. Adv. Prosthodont. 2015, 7, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 62, 1–34. [Google Scholar]
- Faggion, C.M. Guidelines for reporting pre-clinical in vitro studies on dental materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors, Year | Groups (n) | Teeth | Storage | Materials | Results (MPa) |
|---|---|---|---|---|---|
| Vieira et al., 2003 [12] | G1—37% phosphoric acid + adhesive (10) + resin G2—2% CHX + 37% phosphoric acid + adhesive (10) + resin | Molars | 0.1% Thymol | Adhesive: 3M Single Bond (3M, USA) Resin: FiltekTM Z250 (3M, USA) | G1: 19.88 ± 1.04 G2: 17.99 ± 1.15 G1*/G2 |
| Correr et al., 2004 [16] | G1—35% phosphoric acid + adhesive 1 (15) G2—35% phosphoric acid + 10% NaOCl + adhesive 1 (15) G3—37% phosphoric acid + adhesive 2 (15) G4—37% phosphoric acid + 10% NaOCl + adhesive 2 (15) G5–Adhesive 3 (15) G6—10% NaOCl + adhesive 3 (15) + resin | Molars | 0.5% Chloramine | Adhesive: 1–3M Single Bond; 2–Prime & Bond 2.1® (Dentsply, Brazil); 3–ClearfillTM SE Bond (Kuraray, Houston, TX, USA) Resin: FiltekTM Z250 (3M, USA) | G1: 15.8 ± 1.9 G2: 14.6 ± 1.3 G3: 10.2 ± 0.7 G4: 9.9 ± 0.2 G5: 13.3 ± 1.2 G6: 10.7 ± 1.0 G1*/G3 |
| Monghini et al., 2004 [17] | G1—None (12) G2—Laser Er;YAG 60 mJ/2 Hz (12) G3—Laser Er;YAG 80 mJ/2 Hz (12) G4—Laser Er;YAG 100 mJ/2 Hz (12) + 35% phosphoric acid + adhesive + resin | Canines | 0.9% Saline solution with 0.4% sodium azide | Adhesive: 3M Single Bond Laser: Kavo Key Laser 2 (Kavo Dental, Germany) Resin: FiltekTM Z250 | G1:17.89 ± 4.75 G2:12.34 ± 4.85 G3:10.30 ± 3.67 G4:10.41 ± 4.20 G1*/G2;G3;G4 |
| Ersin et al., 2009 [18] | G1—25% polyacrlylic acid + 2% CHX + GIC 1 (sound dentin) (3) G2—25% polyacrlylic acid + 2% CHX + GIC 1 (carious dentin) (3) G3—25% polyacrlylic acid + GIC 1 (sound dentin) (3) G4—25% polyacrlylic acid + GIC 1 (carious dentin) (3) G5—2% CHX + GIC 2 (sound dentin) (3) G6—2% CHX + GIC 2 (carious dentin) (3) G7—GIC 2 (sound dentin) (3) G8—GIC 2 (carious dentin) (3) G9—37% phosphoric acid + 2% CHX + adhesive + resin (sound dentin) (3) G10–37% phosphoric acid + 2% CHX + adhesive + resin (carious dentin) (3) G11—37% phosphoric acid + adhesive + resin (sound dentin) (3) G12—37% phosphoric acid + adhesive + resin (carious dentin) (3) | Molars | 0.1% Thymol | Adhesive: Prime & Bond®; GIC: 1–KetacTM Molar (3M, Germany); 2–VitremerTM (3M, USA) Resin–SurefilTM (Dentsply, USA) | G1: 8.7 ± 4.3 G2: 7.1 ± 5.2 G3: 9.2 ± 5.2 G4: 10.3 ± 6.6 G5: 12.4 ± 5.7 G6: 14.4 ± 6.6 G7: 11.2 ± 4.8 G8: 13.8 ± 4.9 G9: 22.9 ± 6.9 G10: 23.2 ± 6.2 G11: 20.2 ± 5.8 G12: 22.1 ± 6.2 G9*/G1;G2;G3;G4;G5;G6;G7;G8 G10*/G1;G2;G3;G4;G5;G6;G7;G8 G11*/G1;G2;G3;G4;G5;G6;G7;G8 G12*/G1;G2;G3;G4;G5;G6;G7;G8 |
| Ricci et al., 2010 [19] | 35% phosphoric acid + G1—2% CHX + adhesive 1 (4) G2—deionized water + adhesive 1 (4) G3—2% CHX + adhesive 2 (4) G4—deionized water + adhesive 2 (4) G5—2% CHX + adhesive 3 (4) G6—deionized water + adhesive 3 (4) + resin | Molars | NA | Adhesive: 1–AdperTM Single Bond (3M, USA); 2–Prime & Bond NT® (Dentsply, USA); 3–Excite® DSC (Ivoclar, Liechtenstein) Resin: FiltekTM Z250 | G1: 47.4 ± 9.5 G2: 41.4 ± 11.9 G3: 48.0 ± 9.8 G4: 40.8 ± 13.4 G5: 45.2 ± 9.2 G6: 43.4 ± 12.0 G1*/G2; G3*/G4 |
| Leitune et al., 2011 [20] | 37% phosphoric acid + G1—Adhesive (24 h) (10) G2—Adhesive (6 months) (10) G3—2% CHX + Adhesive (24 h) (10) G4—2% CHX + Adhesive (6 months) (10) | Molars | Distilled water | Adhesive: AdperTM ScotchbondTM Multi Purpose (3M, USA) Resin: FiltekTM Z250 | G1: 22.37 ± 3.69 G2: 19.93 ± 2.05 G3: 22.30 ± 3.66 G4: 24.48 ± 2.24 G2*/G4 |
| Scatena et al., 2011 [21] | G1–None (10) G2—Laser Er:YAG (80 mJ, 11 mm) (10) G3—Laser Er:YAG (80 mJ, 12 mm) (10) G4—Laser Er:YAG (80 mJ, 16 mm) (10) G5—Laser Er:YAG (80 mJ, 17 mm) (10) G6—Laser Er:YAG (80 mJ, 20 mm) (10) + 37% phosphoric acid + adhesive + resin | Molars | 0.4% Sodium azide | Laser: Kavo Key Laser 2 Adhesive: 3M Single Bond Resin: FiltekTM Z250 | G1: 7.32 ± 3.83 G2: 5.07 ± 2.62 G3: 6.49 ± 1.64 G4: 7.71 ± 0.66 G5: 7.33 ± 0.02 G6: 9.65 ± 2.41 G2*/G4;G6 |
| Manfro et al., 2012 [30] | 37% phosphoric acid + G1—water + adhesive (7) G2—water + adhesive (12 months) (7) G3—0.5% CHX + adhesive (7) G4—0.5% CHX + adhesive (12 months) (7) G5—2% CHX + adhesive (7) G6—2% CHX + adhesive (12 months) (7) + resin | Molars | 0.5% Chloramine | Adhesive: 3M Single Bond Resin: FiltekTM Z250 | G1: 50.8 ± 12.8 G2: 20.4 ± 3.7 G3: 49.3 ± 2.6 G4: 32.3 ± 7.9 G5: 44.0 ± 8.7 G6: 34.6 ± 5.1 G1*/G2; G2*/G4;G6; G3*/G4; G5*/G6 |
| Lenzi et al., 2012 [22] | 35% phosphoric acid + G1—distilled water + adhesive (sound dentin) (5) G2—2% CHX + adhesive (sound dentin) (5) G3—distilled water + adhesive (artificial caries) (5) G4—2% CHX + adhesive (artificial caries) (5) | Molars | 0.5% Chloramine | Adhesive: AdperTM Single Bond 2 Resin: FiltekTM Z250 | G1: 30.8 ± 2.2 G2: 32.8 ± 3.8 G3: 24.5 ± 3.8 G4: 25.6 ± 3.6 G1*/G3;G4; G2*/G3;G4 |
| Aras et al., 2013 [24] | G1—37% phosphoric acid (10) G2—37% phosphoric acid + 5% NaOCl (10) G3—5% NaOCl + 37% phosphoric acid (10) + adhesive + resin | Molars | Distilled water | Adhesive: Gluma® Confort Bond (Herause-Kulzer, Germany) Resin: Charisma® (Herause-Kulzer, Germany) | G1: 14.51 ± 2.89 G2: 18.45 ± 2.30 G3: 17.06 ± 2.99 G1*/G2 |
| Lenzi et al., 2014 [23] | 35% phosphoric acid + G1—distilled water + adhesive (sound dentin) (5) G2—distilled water + adhesive (sound dentin) (6 months) (5) G3—2% CHX (without rinsing) + adhesive (sound dentin) (5) G4—2% CHX (without rinsing) + adhesive (sound dentin) (6 months) (5) G5—distilled water + adhesive (artificial lesion) (5) G6—distilled water + adhesive (artificial lesion) (6 months) (5) G7—2% CHX (without rinsing) + adhesive (artificial lesion) (5) G8—2% CHX (without rinsing) + adhesive (artificial lesion) (6 months) (5) | Molars | Distilled water | Adhesive: AdperTM Single Bond Resin: FiltekTM Z250 | G1: 30.7 ± 2.2 G2: 25.9 ± 5.7 G3: 32.8 ± 3.8 G4: 31.3 ± 2.6 G5: 26.2 ± 5.4 G6: 20.0 ± 3.9 G7: 28.3 ± 3.4 G8: 26.9 ± 5.9 G1*/G5;G7; G2*/G6;G8 G3*/G5;G7 G4*/G6;G8 |
| Oznurhan et al., 2015 [25] | G1—2% CHX (2) G2—30% propolis (2) G3—Gaseous ozone (2) G4—Ozonated water (2) G5—Laser KTP (2) G6—None (2) + adhesive + resin | Molars | Distilled water | Adhesive: AdperTM Prime & Bond NT® Resin: Tetric® N-Ceram (Ivoclar Vivadent, Liechenstein) Laser: Smartlite D (Deka, Italy) | G1: 7.58 ± 3.18 G2: 7.42 ± 2.28 G3: 5.84 ± 2.62 G4: 11.12 ± 2.41 G5: 9.58 ± 2.92 G6: 6.38 ± 2.47 G3*/G5; G4*/G1/G2/G3/G6 |
| Yildiz et al., 2015 [26] | G1—37% phosphoric acid (3) G2—37% phosphoric acid + Aqua-Prep™ (without rinsing) (3) G3—Laser Er:YAG (10 Hz, 8 mm) (3) + adhesive + resin | Molars | Saline solution | Adhesive: AdperTM Single Bond 2 Resin: FiltekTM Z250 Laser: Fidelis Plus III (Fotona, Slovenia) Aqua-PrepTM (Bisco, USA) | G1: 14.28 ± 5.22 G2: 18.35 ± 7.94 G3: 20.57 ± 9.02 G1*/G3 |
| Bahrololoomi et al., 2017 [27] | 35% phosphoric acid + G1–none (14) G2–2.5% NaOCl (14) G3–5.25% NaOCl (14) + adhesive + resin | Molars | 0.5% Chloramine | Adhesive: One-Step® Plus (Bisco, USA) Resin: AELITE (Bisco, USA) | G1: 13.56 ± 3.36 G2: 13.53 ± 3.64 G3: 14.36 ± 3.64 |
| Ebrahimi et al., 2018 [28] | G1—37% phosphoric acid + adhesive 1 (20) G2—37% phosphoric acid + adhesive 1 (3 months) (20) G3—37% phosphoric acid + adhesive 1 + 2% CHX (without rinsing) (20) G4—37% phosphoric acid + adhesive 1 + 2% CHX (without rinsing) (3 months) (20) G5—Adhesive 2 (20) G6—Adhesive 2 (3 months) (20) G7—Adhesive 2 (Primer) + 2% CHX (without rinsing) + adhesive 2 (bond) (20) G8—Adhesive 2 (primer) + 2% CHX (without rinsing) + adhesive 2 (bond) (3months) (20) | Molars | 0.1% Thymol + water | Adhesive: 1–AdperTM Single Bond 2–ClearfilTM SE Bond Resin: FiltekTM Z250 | G1: 25.43 ± 12.94 G2: 39.96 ± 21.75 G3: 66.45 ± 8.3 G4: 39.02 ± 23.29 G5: 47.83 ± 19.83 G6: 53.36 ± 18.05 G7: 46.25 ± 9.34 G8: 56.4 ± 22.18 G1*/G3 |
| Mohammadi et al., 2020 [29] | 37% phosphoric acid + G1–PBS (15) G2—2% CHX (without rinsing) (15) G3—2% Doxycycline (without rinsing) (15) G4—17% EDTA (15) + adhesive | Anterior teeth | - | Adhesive: AdperTM Single Bond 2 Resin: FiltekTM Z250 | G1: 6.20 ± 2.11 G2: 5.60 ± 2.69 G3: 8.82 ± 3.29 G4: 7.50 ± 3.94 G2*/G3 |
| Studies | Item | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 Abstract | 2a Introduction (Background) | 2b Introduction (Objectives) | 3 Methods (Intervention) | 4 Methods (Outcomes) | 10 Methods (Statistical Methods) | 11 Results (Outcomes and Estimation) | 12 Discussion (Limitations) | 13 Other Information (Funding) | 14 Other Information (Protocol) | |
| Vieira et al., 2003 [12] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | No | No |
| Correr et al., 2004 [16] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | No | No |
| Monghini et al., 2004 [17] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | No | No |
| Ersin et al., 2009 [18] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | No | No |
| Ricci et al., 2010 [19] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | Yes | No |
| Leitune et al., 2011 [20] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | No | No |
| Scatena et al., 2011 [21] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | No | No |
| Manfro et al., 2012 [30] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | No | No |
| Lenzi et al., 2012 [22] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | Yes | No |
| Aras et al., 2013 [24] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | Yes | No |
| Lenzi et al., 2014 [23] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | Yes | No |
| Oznurhan et al., 2015 [25] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | Yes | No |
| Yildiz et al., 2015 [26] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | Yes | Yes | No |
| Bahrololoomi et al., 2017 [27] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | Yes | No |
| Ebrahimi et al., 2018 [28] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | No | Yes | No |
| Mohammadi et al., 2020 [29] | Yes | Yes | Yes | Yes | Yes | Yes | Yes a | Yes | Yes | No |
| Parameter | In Vitro Studies | Clinical/In Situ Studies |
|---|---|---|
| P (Population) | Primary teeth / dentin discs | Children in need of a restoration |
| I (Intervention) | Restoration with prior application of a cavity disinfectant | |
| C (Comparison) | Conventional restoration | |
| O (Outcome) | Effect of cavity disinfection on dentin bond strength | Effect of cavity disinfection on clinical success |
| Inclusion Criteria | Primary teeth evaluation |
| Bond strength/clinical success evaluation | |
| Existence of a control group | |
| Evaluation of commercially available adhesive systems and composite resins or glass ionomer | |
| Application of only one cavity disinfectant per experimental group | |
| Report of results as mean and standard deviation | |
| Exclusion Criteria | Permanent teeth evaluation |
| Evaluation of teeth with endodontic treatment | |
| Evaluation of adhesion of cements, posts, sealants, or brackets | |
| Use of experimental adhesive systems or of mixtures of adhesives with disinfectants | |
| Revisions, animal or cell studies, letters, abstracts, comments, and clinical cases |
| Database | Search keys |
|---|---|
| Cochrane Library | #1 MeSH descriptor: [Dentin] explode all trees |
| #2 dentin | |
| #3 cavity | |
| #4 MeSH descriptor: [Disinfection] explode all trees | |
| #5 disinfect* | |
| #6 antibacteria* | |
| #7 MeSH descriptor: [Anti-Bacterial Agents] explode all trees | |
| #8 chlorhexidine | |
| #9 MeSH descriptor: [Chlorhexidine] explode all trees | |
| #10 “sodium hypochlorite” | |
| #11 MeSH descriptor: [Sodium Hypochlorite] explode all trees | |
| #12 laser | |
| #13 MeSH descriptor: [Lasers] explode all trees | |
| #14 ozone | |
| #15 MeSH descriptor: [Ozone] explode all trees | |
| #16 “aloe vera” | |
| #17 MeSH descriptor: [Aloe] explode all trees | |
| #18 ethanol | |
| #19 MeSH descriptor: [Ethanol] explode all trees | |
| #20 EDTA | |
| #21 MeSH descriptor: [Edetic Acid] explode all trees | |
| #22 “green tea” | |
| #23 EGCG | |
| #24 “bond strength” | |
| #25 adhesion | |
| #26 adhesive | |
| #27 MeSH descriptor: [Dental Cements] explode all trees | |
| #28 primary | |
| #29 deciduous | |
| #30 MeSH descriptor: [Tooth, Deciduous] explode all trees | |
| #31 temporary | |
| #32 #1 OR #2 OR #3 | |
| #33 #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 | |
| #34 #24 OR #25 OR #26 OR #27 | |
| #35 #28 OR #29 OR #30 OR #31 | |
| #36 #32 AND #33 AND #34 AND #35 | |
| PubMed | (dentin[MeSH Terms] OR dentin OR cavity) AND (disinfection[MeSH Terms] OR disinfect* OR antibacteria* OR agents, antibacterial[MeSH Terms] OR chlorhexidine[MeSH Terms] OR chlorhexidine OR “sodium hypochlorite” OR sodium hypochlorite[MeSH Terms] OR laser OR lasers[MeSH Terms] OR ozone OR ozone[MeSH Terms] OR “aloe vera” OR aloe[MeSH Terms] OR ethanol OR ethanol[MeSH Terms] OR EDTA OR Edetic acid[MeSH Terms] OR “green tea” OR EGCG) AND (“bond strength” OR adhesion OR adhesive OR adhesives[MeSH Terms]) AND (deciduous tooth[MeSH Terms] OR deciduous OR primary OR temporary) |
| SCOPUS | TITLE-ABS-KEY (dentin OR cavity) AND TITLE-ABS-KEY (disinfect* OR antibacterial* OR chlorhexidine OR “sodium hypochlorite” OR laser OR ozone OR “aloe vera” OR ethanol OR EDTA OR “green tea” OR EGCG) AND TITLE-ABS-KEY (“bond strength” OR adhesion OR adhesive) AND TITLE-ABS-KEY (primary OR deciduous OR temporary) |
| Web of Science | TS= ((dentin[MeSH Terms] OR dentin OR cavity) AND (disinfect* OR antibacteria* OR chlorhexidine OR “sodium hypochlorite” OR laser OR ozone OR “aloe vera” OR ethanol OR EDTA OR “green tea” OR EGCG) AND (“bond strength” OR adhesion or adhesive) AND (primary OR deciduous OR temporary)) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, A.; Amaro, I.; Apolónio, A.; Paula, A.; Saraiva, J.; Ferreira, M.M.; Marto, C.M.; Carrilho, E. Effect of Cavity Disinfectants on Adhesion to Primary Teeth—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 4398. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094398
Coelho A, Amaro I, Apolónio A, Paula A, Saraiva J, Ferreira MM, Marto CM, Carrilho E. Effect of Cavity Disinfectants on Adhesion to Primary Teeth—A Systematic Review. International Journal of Molecular Sciences. 2021; 22(9):4398. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094398
Chicago/Turabian StyleCoelho, Ana, Inês Amaro, Ana Apolónio, Anabela Paula, José Saraiva, Manuel Marques Ferreira, Carlos Miguel Marto, and Eunice Carrilho. 2021. "Effect of Cavity Disinfectants on Adhesion to Primary Teeth—A Systematic Review" International Journal of Molecular Sciences 22, no. 9: 4398. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094398