

Topical Treatment of Actinic Keratosis and Metalloproteinase Expression: A Clinico-Pathological Retrospective Study
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Results
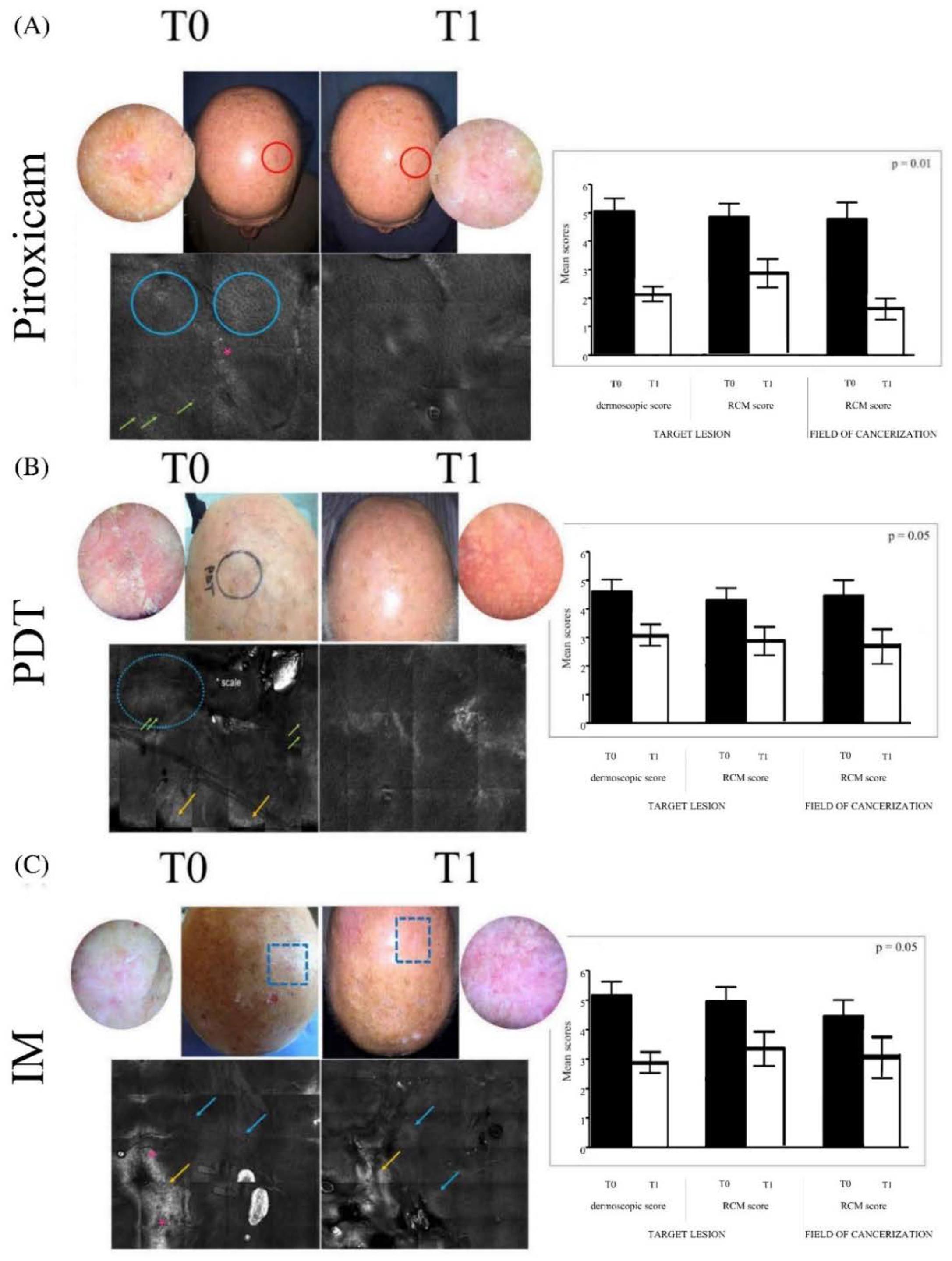
2.1. Dermoscopic and RCM Evaluations
2.2. Microscopic Features of Actinic Keratoses before and after Treatment
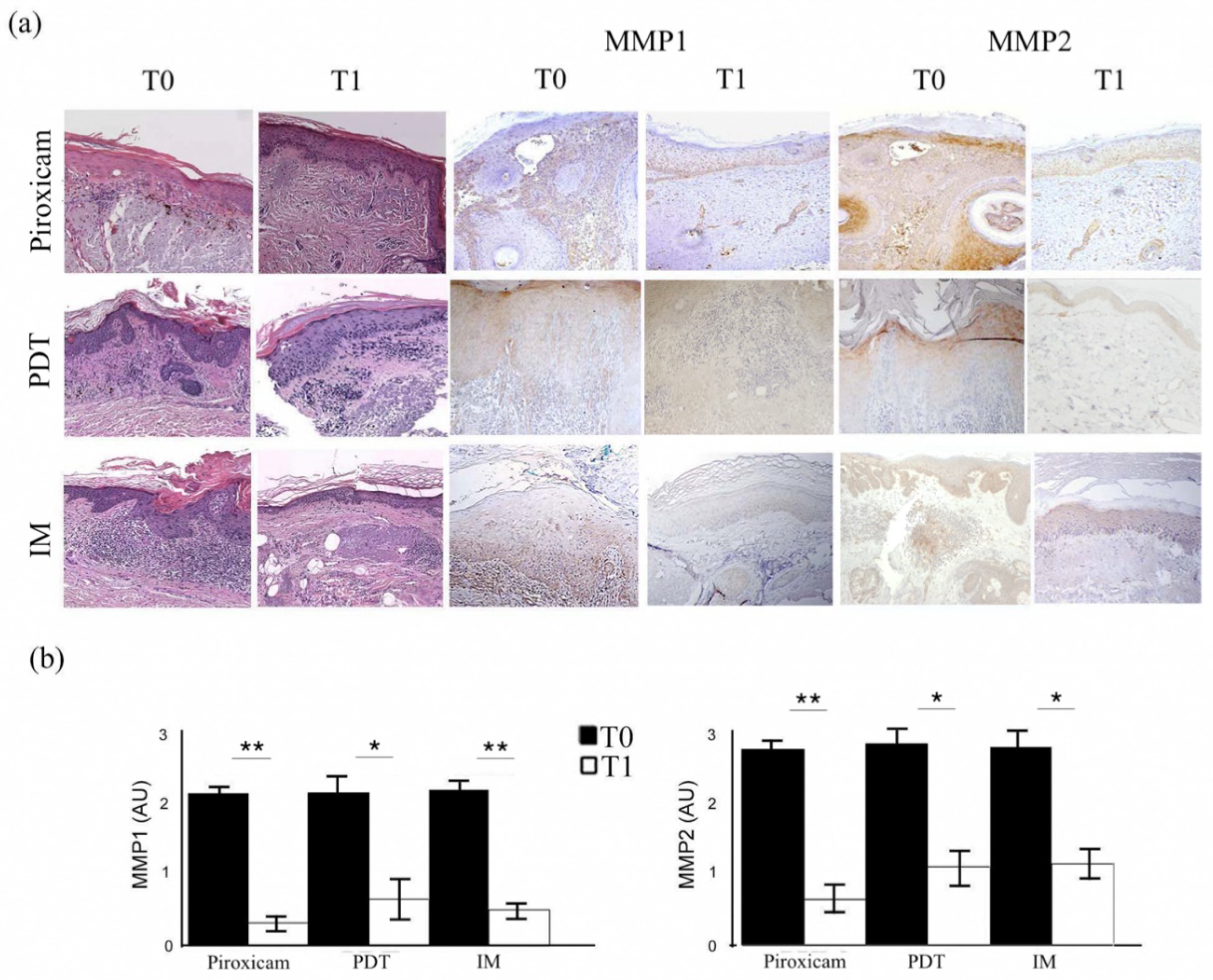
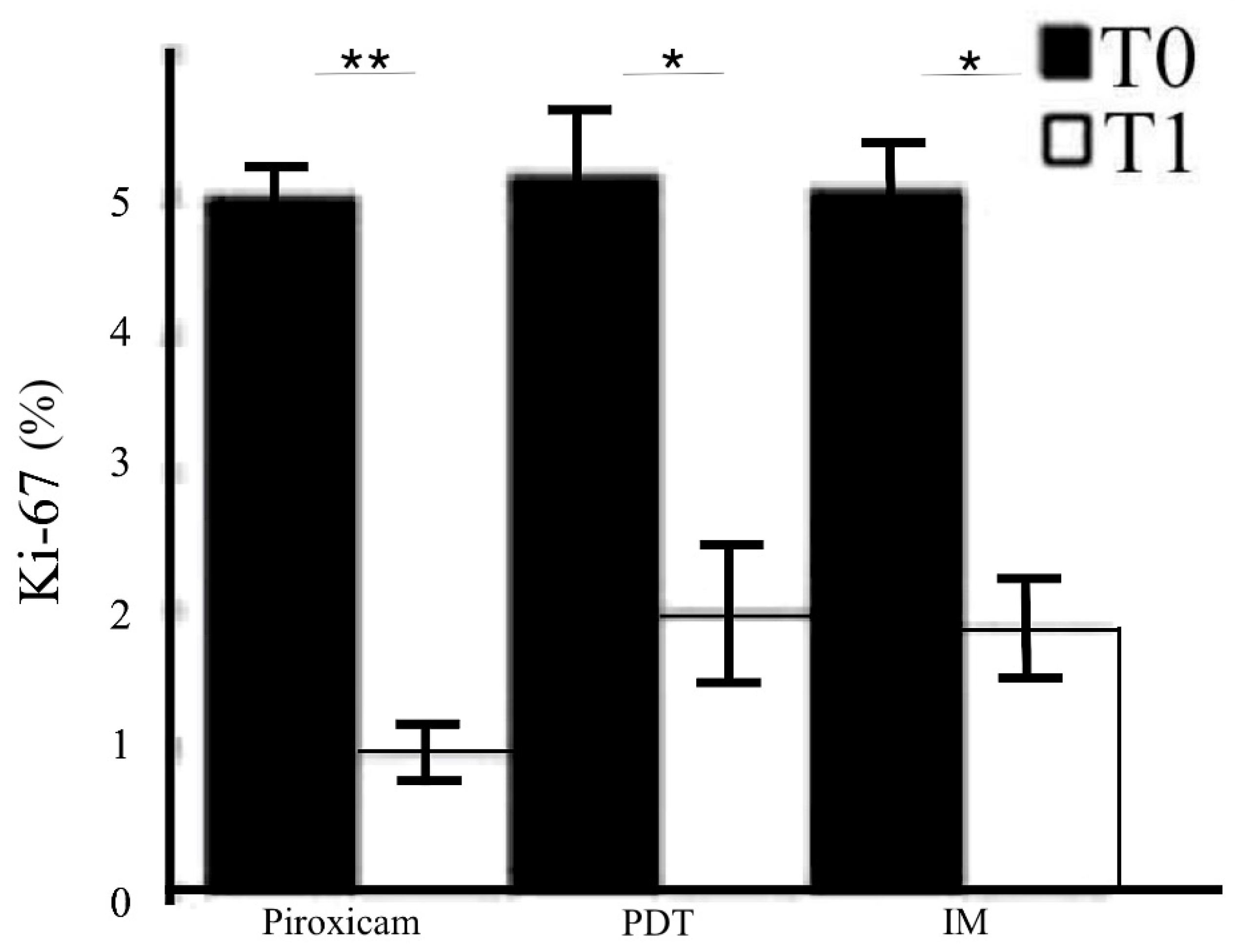
2.3. MMPs Evaluation before and after Treatments
2.4. Correlations between MMP Expression and Clinico-Pathological Features
3. Discussion
4. Methods and Patients
4.1. Patients
4.2. Dermoscopic and RCM Evaluation
4.3. Histopathological and Immunohistochemical Evaluation
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Röwert-Huber, J.; Patel, M.J.; Forschner, T.; Ulrich, C.; Eberle, J.; Kerl, H.; Sterry, W.; Stockfleth, E. Actinic keratosis is an early in situ squamous cell carcinoma: A proposal for reclassification. Br. J. Dermatol. 2007, 156 (Suppl. 3), 8–12, Erratum in Br. J. Dermatol. 2007, 157, 431. [Google Scholar] [CrossRef] [PubMed]
- Wood, D.L.A.; Lachner, N.; Tan, J.M.; Tang, S.; Angel, N.; Laino, A.; Linedale, R.; Lê Cao, K.A.; Morrison, M.; Frazer, I.H.; et al. A Natural History of Actinic Keratosis and Cutaneous Squamous Cell Carcinoma Microbiomes. mBio 2018, 9, e01432-18. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, E.C.V.; da Motta, V.R.V.; Pantoja, P.C.; Ilha, C.S.O.; Magalhães, R.F.; Galadari, H.; Leonardi, G.R. Actinic keratosis-review for clinical practice. Int. J. Dermatol. 2019, 58, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Lai, V.; Cranwell, W.; Sinclair, R. Epidemiology of skin cancer in the mature patient. Clin. Dermatol. 2018, 36, 167–176. [Google Scholar] [CrossRef]
- Werner, R.N.; Sammain, A.; Erdmann, R.; Hartmann, V.; Stockfleth, E.; Nast, A. The natural history of actinic keratosis: A systematic review. Br. J. Dermatol. 2013, 169, 502–518. [Google Scholar] [CrossRef]
- Siegel, J.A.; Korgavkar, K.; Weinstock, M.A. Current perspective on actinic keratosis: A review. Br. J. Dermatol. 2017, 177, 350–358. [Google Scholar] [CrossRef]
- Kupsa, R.; Deinlein, T.; Woltsche, N.; Hofmann-Wellenhof, R.; Zalaudek, I. Dermoscopy of keratinocyte skin cancer. G. Ital. Dermatol. Venereol. 2016, 151, 649–662. [Google Scholar]
- Fargnoli, M.C.; Kostaki, D.; Piccioni, A.; Micantonio, T.; Peris, K. Dermoscopy in the diagnosis and management of non-melanoma skin cancers. Eur. J. Dermatol. 2012, 22, 456–463. [Google Scholar] [CrossRef]
- Zalaudek, I.; Argenziano, G. Dermoscopy of actinic keratosis, intraepidermal carcinoma and squamous cell carcinoma. Curr. Probl. Dermatol. 2015, 46, 70–76. [Google Scholar] [CrossRef]
- Longo, C.; Casari, A.; Pepe, P.; Moscarella, E.; Zalaudek, I.; Argenziano, G.; Pellacani, G. Confocal microscopy insights into the treatment and cellular immune response of Basal cell carcinoma to photodynamic therapy. Dermatology 2012, 225, 264–270. [Google Scholar] [CrossRef]
- Nissinen, L.; Farshchian, M.; Riihilä, P.; Kähäri, V.M. New perspectives on role of tumor microenvironment in progression of cutaneous squamous cell carcinoma. Cell Tissue Res. 2016, 365, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Pérez, M.; El-hajahmad, M.; Massaro, J.; Mahalingam, M. Expression of gelatinases (MMP-2, MMP-9) and gelatinase activator (MMP-14) in actinic keratosis and in in situ and invasive squamous cell carcinoma. Am. J. Dermatopathol. 2012, 34, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Pittayapruek, P.; Meephansan, J.; Prapapan, O.; Komine, M.; Ohtsuki, M. Role of Matrix Metalloproteinases in Photoaging and Photocarcinogenesis. Int. J. Mol. Sci. 2016, 17, 868. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, G.; Wlaschek, M.; Lange, T.S.; Prenzel, K.; Goerz, G.; Scharffetter-Kochanek, K. UVA irradiation stimulates the synthesis of various matrix-metalloproteinases (MMPs) in cultured human fibroblasts. Exp. Dermatol. 1993, 2, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Koivukangas, V.; Kallioinen, M.; Autio-Harmainen, H.; Oikarinen, A. UV irradiation induces the expression of gelatinases in human skin in vivo. Acta Derm. Venereol. 1994, 74, 279–282. [Google Scholar] [CrossRef]
- de Oliveira Poswar, F.; de Carvalho Fraga, C.A.; Gomes, E.S.B.; Farias, L.C.; Souza, L.W.F.; Santos, S.H.S.; Gomez, R.S.; de-Paula, A.M.B.; Guimarães, A.L.S. Protein expression of MMP-2 and MT1-MMP in actinic keratosis, squamous cell carcinoma of the skin, and basal cell carcinoma. Int. J. Surg. Pathol. 2015, 23, 20–25. [Google Scholar] [CrossRef]
- Zheng, L.Q.; Wang, R.; Chi, S.M.; Li, C.X. Matrix metalloproteinase 1: A better biomarker for squamous cell carcinoma by multiple microarray analyses. G. Ital. Dermatol. Venereol. 2019, 154, 327–337. [Google Scholar] [CrossRef]
- Gupta, A.; Kaur, C.D.; Jangdey, M.; Saraf, S. Matrix metalloproteinase enzymes and their naturally derived inhibitors: Novel targets in photocarcinoma therapy. Ageing Res. Rev. 2014, 13, 65–74. [Google Scholar] [CrossRef]
- Roy, R.; Yang, J.; Moses, M.A. Matrix metalloproteinases as novel biomarkers and potential therapeutic targets in human cancer. J. Clin. Oncol. 2009, 27, 5287–5297. [Google Scholar] [CrossRef]
- Diluvio, L.; Bavetta, M.; Costanza, G.; Orlandi, A.; Bianchi, L.; Campione, E. Monitoring treatment response in patients affected by actinic keratosis: Dermoscopic assessment and metalloproteinases evaluation after piroxicam 0.8% and sunfilter cream. Dermatol. Ther. 2019, 32, e12772. [Google Scholar] [CrossRef]
- Richard, M.A.; Amici, J.M.; Basset-Seguin, N.; Claudel, J.P.; Cribier, B.; Dreno, B. Management of actinic keratosis at specific body sites in patients at high risk of carcinoma lesions: Expert consensus from the AKTeam™ of expert clinicians. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Dirschka, T.; Gupta, G.; Micali, G.; Stockfleth, E.; Basset-Séguin, N.; Del Marmol, V.; Dummer, R.; Jemec, G.B.E.; Malvehy, J.; Peris, K.; et al. Real-world approach to actinic keratosis management: Practical treatment algorithm for office-based dermatology. J. Dermatolog. Treat. 2017, 28, 431–442. [Google Scholar] [CrossRef]
- Campione, E.; Ventura, A.; Diluvio, L.; Mazzeo, M.; Mazzilli, S.; Garofalo, V.; Di Prete, M.; Bianchi, L. Current developments in pharmacotherapy for actinic keratosis. Expert Opin. Pharmacother. 2018, 19, 1693–1704. [Google Scholar] [CrossRef] [PubMed]
- Jetter, N.; Chandan, N.; Wang, S.; Tsoukas, M. Field Cancerization Therapies for Management of Actinic Keratosis: A Narrative Review. Am. J. Clin. Dermatol. 2018, 19, 543–557. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.N.; Stockfleth, E.; Connolly, S.M.; Correia, O.; Erdmann, R.; Foley, P.; Gupta, A.K.; Jacobs, A.; Kerl, H.; Lim, H.W. International League of Dermatological Societies; European Dermatology Forum. Evidence- and consensus-based (S3) Guidelines for the Treatment of Actinic Keratosis-International League of Dermatological Societies in cooperation with the European Dermatology Forum-Short version. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2069–2079. [Google Scholar] [CrossRef] [PubMed]
- Mazzeo, M.; Diluvio, L.; Di Prete, M.; Mazzilli, S.; Garofalo, V.; Coniglione, F.; Orlandi, A.; Bianchi, L.; Campione, E. New local treatment for photoaging using a formulation containing piroxicam 0.8% and sunscreen. J. Int. Med. Res. 2019, 47, 3127–3132. [Google Scholar] [CrossRef] [PubMed]
- Campione, E.; Di Prete, M.; Diluvio, L.; Bianchi, L.; Orlandi, A. Efficacy of ingenol mebutate gel for actinic keratosis in patients treated by thiazide diuretics. Clin. Cosmet. Investig. Dermatol. 2016, 9, 405–409. [Google Scholar] [CrossRef]
- Babino, G.; Diluvio, L.; Bianchi, L.; Orlandi, A.; Di Prete, M.; Chimenti, S.; Milani, M.; Campione, E. Long-term use of a new topical formulation containing piroxicam 0.8% and sunscreen: Efficacy and tolerability on actinic keratosis. A proof of concept study. Curr. Med. Res. Opin. 2016, 32, 1345–1349. [Google Scholar] [CrossRef]
- EMA suspends licence for ingenol mebutate (Picato). Drug Ther. Bull. 2020, 58, 51. [CrossRef] [PubMed]
- Farnetani, F.; Manfredini, M.; Chester, J.; Ciardo, S.; Gonzalez, S.; Pellacani, G. Reflectance confocal microscopy in the diagnosis of pigmented macules of the face: Differential diagnosis and margin definition. Photochem. Photobiol. Sci. 2019, 18, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Quan, T.; Qin, Z.; Xia, W.; Shao, Y.; Voorhees, J.J.; Fisher, G.J. Matrix-degrading metalloproteinases in photoaging. J. Investig. Dermatol. Symp. Proc. 2009, 14, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Sbardella, D.; Fasciglione, G.F.; Gioia, M.; Ciaccio, C.; Tundo, G.R.; Marini, S.; Coletta, M. Human matrix metalloproteinases: An ubiquitarian class of enzymes involved in several pathological processes. Mol. Asp. Med. 2012, 33, 119–208. [Google Scholar] [CrossRef] [PubMed]
- Roh, M.R.; Zheng, Z.; Kim, H.S.; Kwon, J.E.; Jeung, H.C.; Rha, S.Y.; Chung, K.Y. Differential expression patterns of MMPs and their role in the invasion of epithelial premalignant tumors and invasive cutaneous squamous cell carcinoma. Exp. Mol. Pathol. 2012, 92, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Kessenbrock, K.; Wang, C.Y.; Werb, Z. Matrix metalloproteinases in stem cell regulation and cancer. Matrix Biol. 2015, 44–46, 184–190. [Google Scholar] [CrossRef]
- Polette, M.; Nawrocki-Raby, B.; Gilles, C.; Clavel, C.; Birembaut, P. Tumour invasion and matrix metalloproteinases. Crit. Rev. Oncol. Hematol. 2004, 49, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, L.; Gambichler, T.; Kost, C.; Gupta, G.; Stücker, M.; Stockfleth, E.; Dirschka, T. Cutaneous squamous cell carcinomas are associated with basal proliferating actinic keratoses. Br. J. Dermatol. 2019, 180, 916–921. [Google Scholar] [CrossRef]
- Campione, E.; Paternò, E.J.; Candi, E.; Falconi, M.; Costanza, G.; Diluvio, L.; Terrinoni, A.; Bianchi, L.; Orlandi, A. The relevance of piroxicam for the prevention and treatment of nonmelanoma skin cancer and its precursors. Drug Des. Devel. Ther. 2015, 9, 5843–5850. [Google Scholar] [CrossRef] [PubMed]
- Campione, E.; Diluvio, L.; Paternò, E.J.; Chimenti, S. Topical treatment of actinic keratoses with piroxicam 1% gel: A preliminary open-label study utilizing a new clinical score. Am. J. Clin. Dermatol. 2010, 11, 45–50. [Google Scholar] [CrossRef]
- Lozzi, F.; Lanna, C.; Mazzeo, M.; Garofalo, V.; Palumbo, V.; Mazzilli, S.; Diluvio, L.; Terrinoni, A.; Bianchi, L.; Campione, E. Investig. ational drugs currently in phase II clinical trials for actinic keratosis. Expert Opin. Investig. Drugs 2019, 28, 629–642. [Google Scholar] [CrossRef]
- Agozzino, M.; Russo, T.; Franceschini, C.; Mazzilli, S.; Garofalo, V.; Campione, E.; Bianchi, L.; Milani, M.; Argenziano, G. Effects of topical piroxicam and sun filters in actinic keratosis evolution and field cancerization: A two-center, assessor-blinded, clinical, confocal microscopy and dermoscopy evaluation trial. Curr. Med. Res. Opin. 2019, 35, 1785–1792. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, V.; Ventura, A.; Mazzilli, S.; Diluvio, L.; Bianchi, L.; Toti, L.; Tisone, G.; Milani, M.; Campione, E. Treatment of Multiple Actinic Keratosis and Field of Cancerization with Topical Piroxicam 0.8% and Sunscreen 50+ in Organ Transplant Recipients: A Series of 10 Cases. Case Rep. Dermatol. 2017, 9, 211–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paolino, G.; Donati, M.; Didona, D.; Mercuri, S.R.; Cantisani, C. Histology of Non-Melanoma Skin Cancers: An Update. Biomedicines 2017, 5, 71. [Google Scholar] [CrossRef] [PubMed]
- Zalaudek, I.; Piana, S.; Moscarella, E.; Longo, C.; Zendri, E.; Castagnetti, F.; Pellacani, G.; Lallas, A.; Argenziano, G. Morphologic grading and treatment of facial actinic keratosis. Clin. Dermatol. 2014, 32, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.M.; Lambie, D.; Sinnya, S.; Sahebian, A.; Soyer, H.P.; Prow, T.W.; Ardigò, M. Histopathology and reflectance confocal microscopy features of photodamaged skin and actinic keratosis. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1901–1911. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | N | Group A (Medical Device 0.8% Piroxicam + 10+ Sunscreen) (n = 10) | Group B (Photodynamic Therapy) (n = 10) | Group C (Ingenol Mebutate Gel) (n = 10) | |
|---|---|---|---|---|---|
| Age (mean = 74.5; range 60–88) | >74.5 | 11 | 74.8 | 74.0 | 74.2 |
| <74.5 | 19 | ||||
| Sex | Male | 24 | 8 | 8 | 8 |
| Female | 6 | 2 | 2 | 2 | |
| Anatomic location | Head/neck | 21 | 7 | 7 | 7 |
| Extremities | 9 | 3 | 3 | 3 | |
| AK clinical grade (according to Olsen) | 1 | 13 | 4 | 4 | 5 |
| 2 | 17 | 6 | 6 | 5 | |
| 3 | 0 | 0 | 0 | 0 | |
| AK histopathologic grade (according to Rowert-Huber) | I | 6 | 2 | 2 | 2 |
| II | 18 | 6 | 6 | 6 | |
| III | 6 | 2 | 2 | 2 | |
| Solar elastosis | Mild | 5 | 2 | 1 | 2 |
| Moderate | 11 | 3 | 4 | 4 | |
| Severe | 13 | 5 | 4 | 4 | |
| Peritumoral inflammatory infiltrate | Mild | 8 | 3 | 3 | 2 |
| Moderate | 13 | 4 | 4 | 5 | |
| Severe | 9 | 3 | 3 | 3 |
| Grade | Clinical Classification (Olsen’s) | Dermoscopic Classification [43] |
|---|---|---|
| 1 | Skin-colored macule without hyperkeratosis (easier felt than seen) |
|
| 2 | Moderate hyperkeratotic lesion in an erythematous background (easily felt and seen) |
|
| 3 | Very thick and hyperkeratotic lesion, which may include SCC in the differential diagnoses |
|
| Erythema | 0 = absent from 1 to 4 = present (4 = maximum erythema) |
| Scaling | 0 = absent from 1 to 4 = present (4 = maximum scaling) |
| Pigmentation | 0 = absent 1 = light and focal pigmentation from 2 to 4 = increasing level of brownish pigmentation 5 = dark pigmentation |
| Follicular plugs | 0 = absent 1 = few plugs in just one of the evaluated areas 2 and 3 = increasing number of plugs in several areas 4 = diffuse presence of follicular plugs |
| Corneum Layer | Absence | Presence |
|---|---|---|
| Scale | 0 | 1 |
| Dysruption/detached corneocytes | 0 | 1 |
| Parakeratosis | 0 | 1 |
| Polygonal keratinocytes | 0 | 1 |
| Granular and spinous layers | ||
| Atypical honeycomb | 0 | 1 |
| Inflammatory cells | 0 | 1 |
| Round nucleated cells | 0 | 1 |
| Dermis | ||
| Curled fibres | 0 | 1 |
| Collagen alterations | 0 | 1 |
| Increased vascularity | 0 | 1 |
| Inflammatory cells | 0 | 1 |
| Melanophages | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campione, E.; Di Prete, M.; Di Raimondo, C.; Costanza, G.; Palumbo, V.; Garofalo, V.; Mazzilli, S.; Franceschini, C.; Dika, E.; Bianchi, L.; et al. Topical Treatment of Actinic Keratosis and Metalloproteinase Expression: A Clinico-Pathological Retrospective Study. Int. J. Mol. Sci. 2022, 23, 11351. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911351
Campione E, Di Prete M, Di Raimondo C, Costanza G, Palumbo V, Garofalo V, Mazzilli S, Franceschini C, Dika E, Bianchi L, et al. Topical Treatment of Actinic Keratosis and Metalloproteinase Expression: A Clinico-Pathological Retrospective Study. International Journal of Molecular Sciences. 2022; 23(19):11351. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911351
Chicago/Turabian StyleCampione, Elena, Monia Di Prete, Cosimo Di Raimondo, Gaetana Costanza, Vincenzo Palumbo, Virginia Garofalo, Sara Mazzilli, Chiara Franceschini, Emi Dika, Luca Bianchi, and et al. 2022. "Topical Treatment of Actinic Keratosis and Metalloproteinase Expression: A Clinico-Pathological Retrospective Study" International Journal of Molecular Sciences 23, no. 19: 11351. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911351