
The Cytotoxic Effect of Isolated Cannabinoid Extracts on Polypoid Colorectal Tissue


Abstract
:1. Introduction
2. Results
2.1. Evaluation of the Toxicity of Cannabinoids on Colon-Polyp-Derived Cells
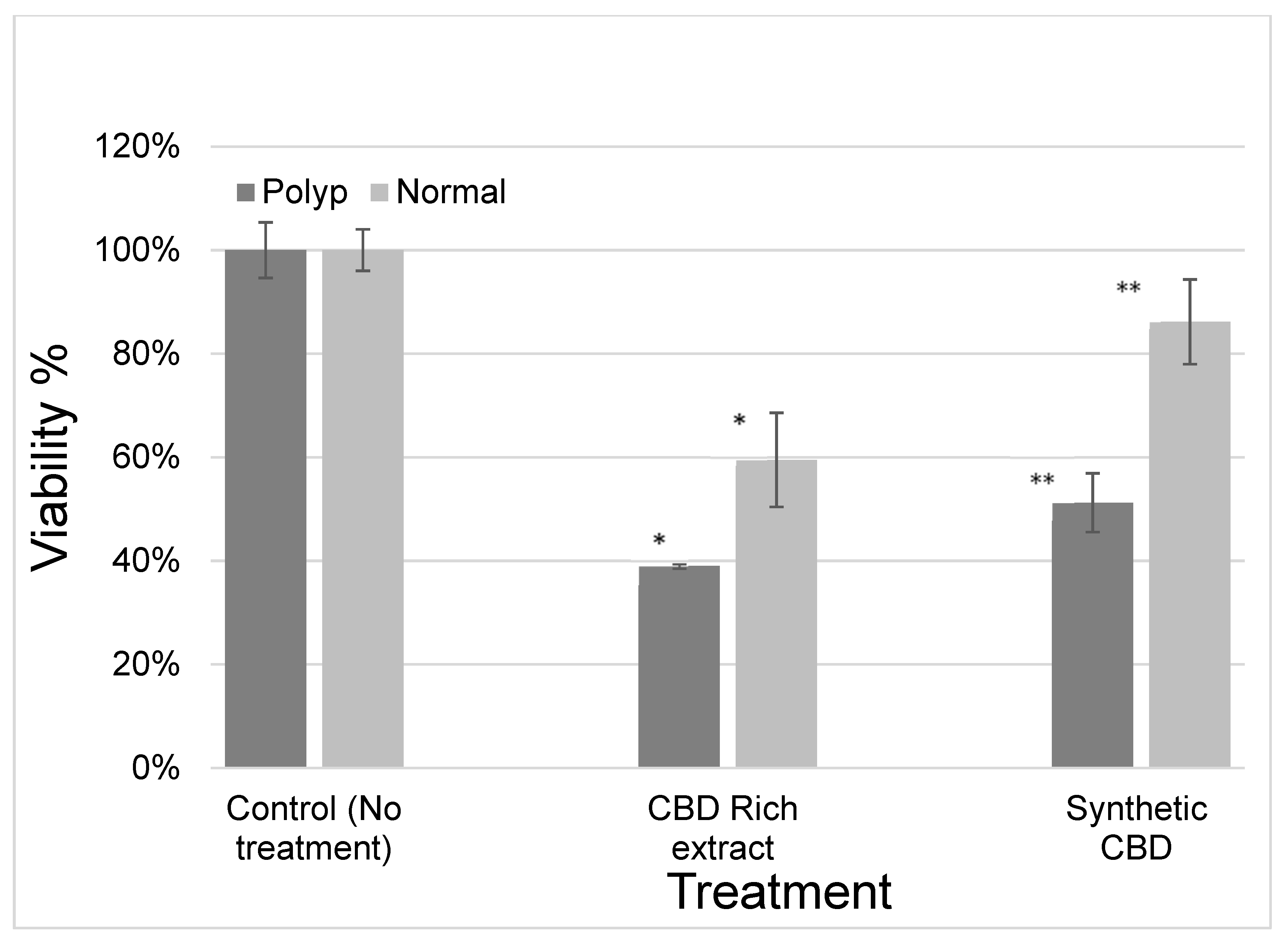
2.2. Evaluation of the Efficacy of Cannabinoids on the Viability of Cells Derived from Patient Colon Polyps and Adjacent Normal Cells
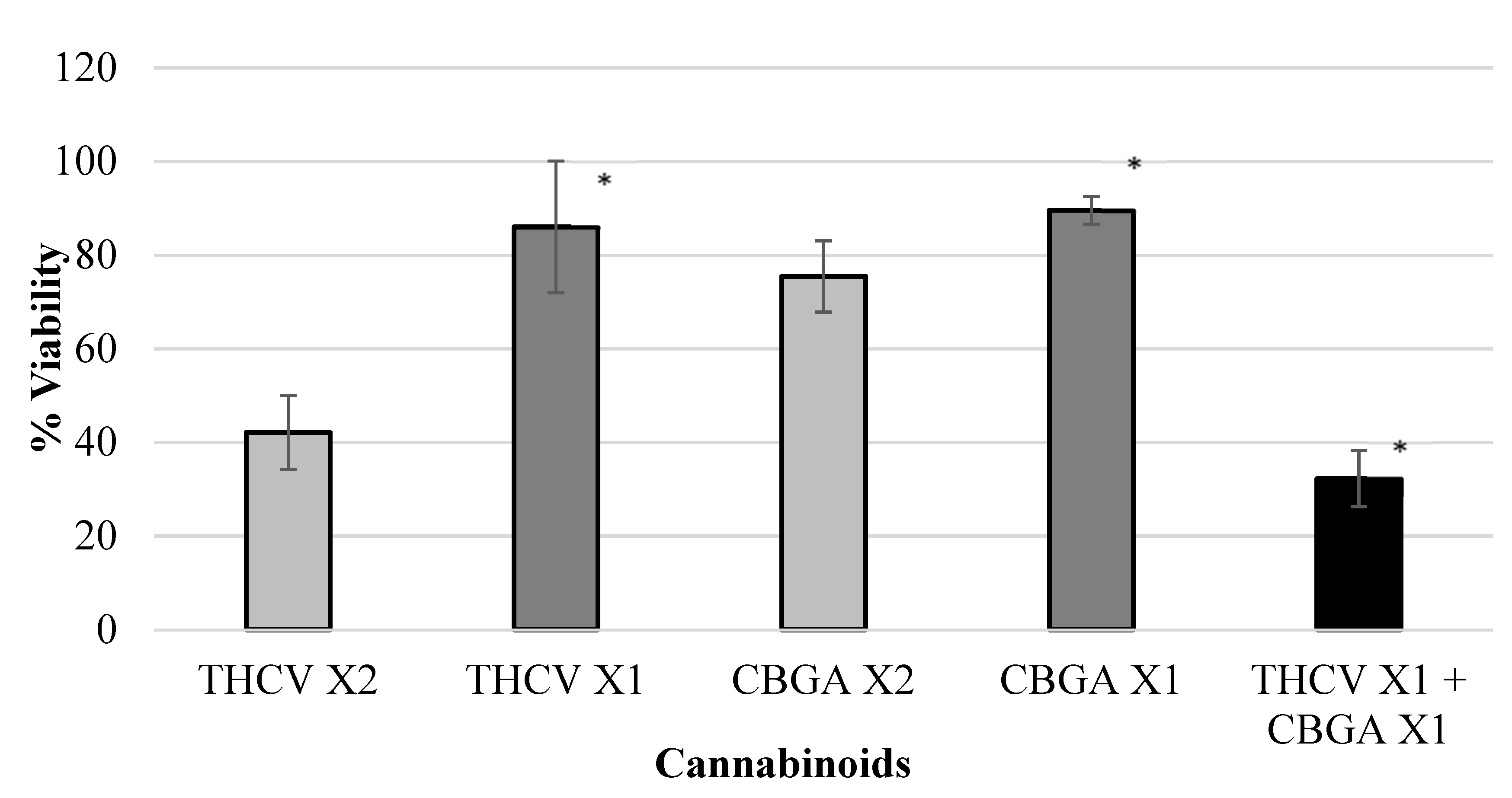
2.3. Evaluation of the Effect of Combinations of Cannabinoids on Colon Cancer Cell Viability
3. Discussion
4. Materials and Methods
4.1. Polyp and Normal Colon Derived Cells
4.2. Polyp Derived Cells Viability and Counting
4.3. Extraction of Cannabis Inflorescence
4.4. Isolated Cannabinoids
4.5. Cytotoxicity Assay
4.6. Cannabinoids Extracts and Compounds Cytotoxicity
4.7. Cannabinoids Differential Effects
4.8. Cannabinoids Combined Effects (Synergy)
4.9. Statistical Analyses
5. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Edwards, B.K.; Ward, E.; Kohler, B.A.; Eheman, C.; Zauber, A.G.; Anderson, R.N.; Jemal, A.; Schymura, M.J.; Lansdorp-Vogelaar, I.; Seeff, L.C.; et al. Annual report to the nation on the status of cancer, 1975–2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer 2010, 116, 544–573. [Google Scholar] [CrossRef] [PubMed]
- Linnekamp, J.F.; Wang, X.; Medema, J.P.; Vermeulen, L. Colorectal cancer heterogeneity and targeted therapy: A case for molecular disease subtypes. Cancer Res. 2015, 75, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, S.D.; Bertagnolli, M.M. Molecular origins of cancer: Molecular basis of colorectal cancer. N. Engl. J. Med. 2009, 361, 2449–2460. [Google Scholar] [CrossRef]
- Zauber, A.G.; Winawer, S.J.; O’Brien, M.J.; Lansdorp-Vogelaar, I.; van Ballegooijen, M.; Hankey, B.F.; Shi, W.; Bond, J.H.; Schapiro, M.; Panish, J.F.; et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N. Engl. J. Med. 2012, 366, 687–696. [Google Scholar] [CrossRef]
- Rotondano, G.; Bianco, M.A.; Buffoli, F.; Gizzi, G.; Tessari, F.; Cipolletta, L. The Cooperative Italian FLIN Study Group: Prevalence and clinico-pathological features of colorectal laterally spreading tumors. Endoscopy 2011, 43, 856–861. [Google Scholar] [CrossRef]
- Klein, A.; Bourke, M.J. Advanced polypectomy and resection techniques. Gastrointest. Endosc. Clin. 2015, 25, 303–333. [Google Scholar] [CrossRef]
- Christie, J.P. Colonoscopic excision of large sessile polyps. Am. J. Gastroenterol. 1977, 67, 430–438. [Google Scholar]
- Moss, A.; Williams, S.J.; Hourigan, L.F.; Brown, G.; Tam, W.; Singh, R.; Zanati, S.; Burgess, N.G.; Sonson, R.; Byth, K.; et al. Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: Results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut 2015, 64, 57–65. [Google Scholar] [CrossRef]
- Moss, A.; Bourke, M.J.; Williams, S.J.; Hourigan, L.F.; Brown, G.; Tam, W.; Singh, R.; Zanati, S.; Chen, R.Y.; Byth, K. Endosc.opic mucosal resection outcomes and prediction of submucosal cancer from advanced colonic mucosal neoplasia. Gastroenterology 2011, 140, 1909–1918. [Google Scholar] [CrossRef]
- Klein, A.; Tate, D.J.; Jayasekeran, V.; Hourigan, L.; Singh, R.; Brown, G.; Bahin, F.F.; Burgess, N.; Williams, S.J.; Lee, E.; et al. Thermal Ablation of Mucosal Defect Margins Reduces Adenoma Recurrence After Colonic Endoscopic Mucosal Resection. Gastroenterology 2019, 156, 604–613.e603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, J.A.; Cole, B.F.; Sandler, R.S.; Haile, R.W.; Ahnen, D.; Bresalier, R.; McKeown-Eyssen, G.; Summers, R.W.; Rothstein, R.; Burke, C.A.; et al. A randomized trial of aspirin to prevent colorectal adenomas. N. Engl. J. Med. 2003, 348, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.A.; Barry, E.L.; Mott, L.A.; Rees, J.R.; Sandler, R.S.; Snover, D.C.; Bostick, R.M.; Ivanova, A.; Cole, B.F.; Ahnen, D.J.; et al. A Trial of Calcium and Vitamin D for the Prevention of Colorectal Adenomas. N. Engl. J. Med. 2015, 373, 1519–1530. [Google Scholar] [CrossRef]
- Higurashi, T.; Hosono, K.; Takahashi, H.; Komiya, Y.; Umezawa, S.; Sakai, E.; Uchiyama, T.; Taniguchi, L.; Hata, Y.; Uchiyama, S.; et al. Metformin for chemoprevention of metachronous colorectal adenoma or polyps in post-polypectomy patients without diabetes: A multicentre double-blind, placebo-controlled, randomised phase 3 trial. Lancet Oncol. 2016, 17, 475–483. [Google Scholar] [CrossRef]
- Radwan, M.M.; ElSohly, M.A.; El-Alfy, A.T.; Ahmed, S.A.; Slade, D.; Husni, A.S.; Manly, S.P.; Wilson, L.; Seale, S.; Cutler, S.J.; et al. Isolation and Pharmacol.ogical Evaluation of Minor Cannabinoids from High-Potency Cannabis sativa. J. Nat. Prod. 2015, 78, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Howlett, A.C.; Abood, M.E. CB1 and CB2 Receptor Pharmacology. Adv. Pharmacol. 2017, 80, 169–206. [Google Scholar] [CrossRef]
- Javid, F.A.; Phillips, R.M.; Afshinjavid, S.; Verde, R.; Ligresti, A. Cannabinoid pharmacology in cancer research: A new hope for cancer patients? Eur. J. Pharmacol. 2016, 775, 1–14. [Google Scholar] [CrossRef]
- Greenhough, A.; Patsos, H.A.; Williams, A.C.; Paraskeva, C. The cannabinoid delta(9)-tetrahydrocannabinol inhibits RAS-MAPK and PI3K-AKT survival signalling and induces BAD-mediated apoptosis in colorectal cancer cells. Int. J. Cancer 2007, 121, 2172–2180. [Google Scholar] [CrossRef]
- Aviello, G.; Romano, B.; Borrelli, F.; Capasso, R.; Gallo, L.; Piscitelli, F.; Di Marzo, V.; Izzo, A.A. Chemopreventive effect of the non-psychotropic phytocannabinoid cannabidiol on experimental colon cancer. J. Mol. Med. 2012, 90, 925–934. [Google Scholar] [CrossRef]
- Romano, B.; Borrelli, F.; Pagano, E.; Cascio, M.G.; Pertwee, R.G.; Izzo, A.A. Inhibition of colon carcinogenesis by a standardized Cannabis sativa extract with high content of cannabidiol. Phytomedicine 2014, 21, 631–639. [Google Scholar] [CrossRef]
- Borrelli, F.; Pagano, E.; Romano, B.; Panzera, S.; Maiello, F.; Coppola, D.; De Petrocellis, L.; Buono, L.; Orlando, P.; Izzo, A.A. Colon carcinogenesis is inhibited by the TRPM8 antagonist cannabigerol, a Cannabis-derived non-psychotropic cannabinoid. Carcinogenesis 2014, 35, 2787–2797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pertwee, R.G. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. Br. J. Pharmacol. 2008, 153, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Nallathambi, R.; Mazuz, M.; Namdar, D.; Shik, M.; Namintzer, D.; Vinayaka, A.C.; Ion, A.; Faigenboim, A.; Nasser, A.; Laish, I.; et al. Identification of Synergistic Interaction Between Cannabis-Derived Compounds for Cytotoxic Activity in Colorectal Cancer Cell Lines and Colon Polyps That Induces Apoptosis-Related Cell Death and Distinct Gene Expression. Cannabis Cannabinoid. Res. 2018, 3, 120–135. [Google Scholar] [CrossRef] [PubMed]
- Winawer, S.; Fletcher, R.; Rex, D.; Bond, J.; Burt, R.; Ferrucci, J.; Ganiats, T.; Levin, T.; Woolf, S.; Johnson, D.; et al. Colorectal cancer screening and surveillance: Clinical guidelines and rationale-Update based on new evidence. Gastroenterology 2003, 124, 544–560. [Google Scholar] [CrossRef]
- Ben-Shabat, S.; Fride, E.; Sheskin, T.; Tamiri, T.; Rhee, M.H.; Vogel, Z.; Bisogno, T.; De Petrocellis, L.; Di Marzo, V.; Mechoulam, R. An entourage effect: Inactive endogenous fatty acid glycerol esters enhance 2-arachidonoyl-glycerol cannabinoid activity. Eur. J. Pharmacol. 1998, 353, 23–31. [Google Scholar] [CrossRef]
- Russo, E.B. Taming THC: Potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 2011, 163, 1344–1364. [Google Scholar] [CrossRef]
- Blasco-Benito, S.; Seijo-Vila, M.; Caro-Villalobos, M.; Tundidor, I.; Andradas, C.; Garcia-Taboada, E.; Wade, J.; Smith, S.; Guzman, M.; Perez-Gomez, E.; et al. Appraising the “entourage effect”: Antitumor action of a pure cannabinoid versus a botanical drug preparation in preclinical models of breast cancer. Biochem. Pharmacol. 2018, 157, 285–293. [Google Scholar] [CrossRef]
- Larsen, C.; Shahinas, J. Dosage, Efficacy and Safety of Cannabidiol Administration in Adults: A Systematic Review of Human Trials. J. Clin. Med. Res. 2020, 12, 129–141. [Google Scholar] [CrossRef]
- The Paris endoscopic classification of superficial neoplastic lesions: Esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest. Endosc. 2003, 58, S3–S43. [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Sex (F = Female, M = Male) | Age | Histology | Polyp Site | Polyp Size |
|---|---|---|---|---|---|
| 1 | F | 57 | VA w LGD | Cecum | 25 mm |
| 2 | M | 69 | TVA w LGD | Cecum | 20 mm |
| 3 | M | 77 | TVA w HGD | Descending colon | 40 mm |
| 4 | F | 52 | TSA | Sigmoid colon | 70 mm |
| 5 | F | 50 | VA w LGD | Sigmoid colon | 50 mm |
| 6 | M | 62 | TVA w LGD | Ascending colon | 30 mm |
| 7 | F | 66 | SSA w LGD | Transverse colon | 25 mm |
| 8 | F | 64 | TVA w LGD | Ascending colon | 30 mm |
| 9 | M | 60 | TVA w LGD | Ascending colon | 20 mm |
| 10 | M | 62 | TVA w LGD | Ascending colon | 40 mm |
| 11 * | M | 80 | TVA w LGD | Cecum | 20 mm |
| 12 | F | 55 | TVA w HGD | Ascending colon | 30 mm |
| 13 | F | 50 | SSA no dysplasia | Ascending colon | 20 mm |
| 14 | F | 74 | SSA no dysplasia | Ascending colon | 20 mm |
| 15 * | F | 73 | VA w LGD | Ascending colon | 40 mm |
| 16 | M | 63 | TA w HGD | Cecum | 50 mm |
| 17 | F | 71 | TA w LGD + SSA | Splenic flexure | 25 mm |
| 18 | M | 60 | TA w LGD | Ascending colon | 25 mm |
| 19 | M | 80 | VA w LGD | Hepatic flexure | 30 mm |
| 20 | F | 66 | VA w LGD | Cecum | 70 mm |
| 21 | M | 51 | TVA w LGD | Rectum | 30 mm |
| 22 | M | 80 | TA w LGD | Transverse colon | 30 mm |
| Cannabinoid | P004 | P005 | P006 | P008 | P009 | P010 | Average Viability |
|---|---|---|---|---|---|---|---|
| THC-d8 | 10% | 23% | 44% | 4% | 7% | 5% | 15% |
| THC-d9 | 20% | 20% | 47% | 13% | 21% | 8% | 21% |
| CBC | 21% | 21% | 61% | 15% | 22% | 11% | 25% |
| CBN | 24% | 32% | 54% | 18% | 16% | 13% | 26% |
| CBDV | 37% | 63% | 62% | 23% | 39% | 9% | 39% |
| CBD | 21% | 41% | 54% | 35% | 62% | 24% | 40% |
| THCV | 59% | 74% | 70% | 47% | 40% | 18% | 51% |
| CBL | 73% | 55% | 89% | 55% | 63% | 29% | 61% |
| CBG | 75% | 69% | 58% | 69% | 65% | 37% | 62% |
| THCA | 59% | 91% | 99% | 52% | 60% | 32% | 66% |
| CBDA | 104% | 97% | 66% | 38% | 73% | 26% | 67% |
| CBDVA | 72% | 90% | 83% | 48% | 69% | 56% | 70% |
| CBNA | 66% | 94% | 76% | 83% | 70% | 60% | 75% |
| CBCA | 63% | 86% | 105% | 91% | 72% | 80% | 83% |
| CBGA | 71% | 96% | 84% | 116% | 70% | 97% | 89% |
| Cannab. A | Cannab. B | Cells Viability at ×2 Conc. of Cannab. A | Cells Viability at ×1 Conc. of Cannab. A | Cells Viability at ×2 Conc. of Cannab. B | Cells Viability at ×1 Conc. of Cannab. B | Cells Viability at ×1 Conc. of Cannab. A + Cannab. B |
|---|---|---|---|---|---|---|
| CBCA | CBDV | 67 | 101 | 54 | 98 | 39 |
| CBDV | CBDVA | 54 | 98 | 79 | 94 | 39 |
| CBDV | CBGA | 54 | 98 | 75 | 90 | 38 |
| CBCA | THCV | 67 | 101 | 42 | 86 | 39 |
| CBCA | CBGA | 67 | 101 | 75 | 90 | 61 |
| CBGA | THCV | 75 | 90 | 42 | 86 | 32 |
| CBCA | CBDVA | 67 | 101 | 79 | 94 | 79 |
| CBDVA | CBGA | 79 | 94 | 75 | 90 | 61 |
| CBDVA | THCV | 79 | 94 | 42 | 86 | 72 |
| CBDV | THCV | CBD | CBG | CBDA | CBGA | CBN | THC-d9 | THC-d8 | CBC | THCA | CBDVA | CBCA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0.3 | 3.1 | 76.0 | 1.6 | 0.1 | 0.1 | 0.1 | 2.9 | 0.0 | 5.6 | 0.0 | 0.0 | 5.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ben-Ami Shor, D.; Hochman, I.; Gluck, N.; Shibolet, O.; Scapa, E. The Cytotoxic Effect of Isolated Cannabinoid Extracts on Polypoid Colorectal Tissue. Int. J. Mol. Sci. 2022, 23, 11366. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911366
Ben-Ami Shor D, Hochman I, Gluck N, Shibolet O, Scapa E. The Cytotoxic Effect of Isolated Cannabinoid Extracts on Polypoid Colorectal Tissue. International Journal of Molecular Sciences. 2022; 23(19):11366. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911366
Chicago/Turabian StyleBen-Ami Shor, Dana, Ilan Hochman, Nathan Gluck, Oren Shibolet, and Erez Scapa. 2022. "The Cytotoxic Effect of Isolated Cannabinoid Extracts on Polypoid Colorectal Tissue" International Journal of Molecular Sciences 23, no. 19: 11366. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911366