

Cell-Free DNA as a Prognostic Biomarker for Monitoring Muscle-Invasive Bladder Cancer
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Clinicopathological Features of the Cohort
2.2. Mutation Analysis from Tissue and Plasma at Cystectomy
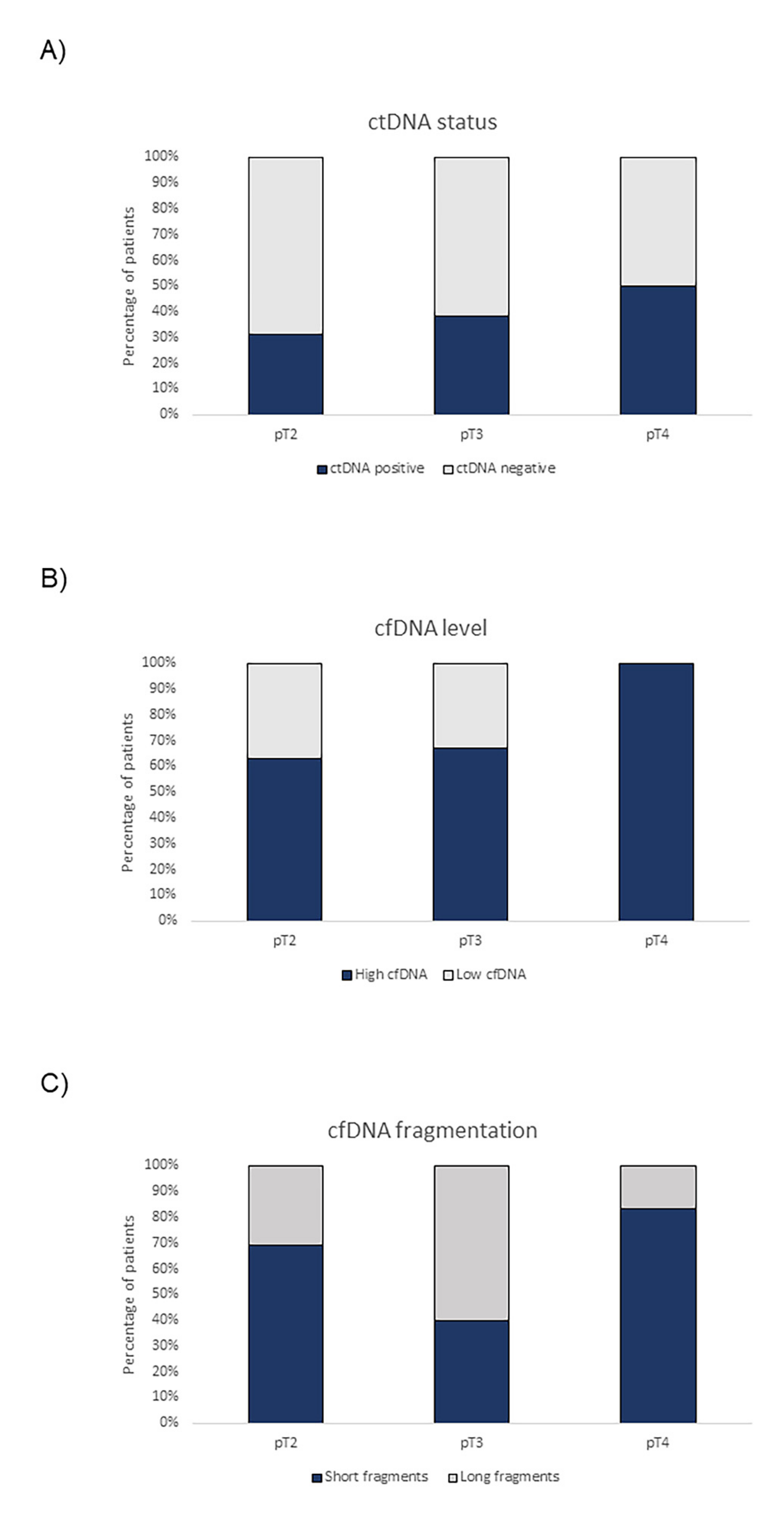
2.3. ctDNA Status and cfDNA Levels and Fragmentation Patterns during Follow-Up
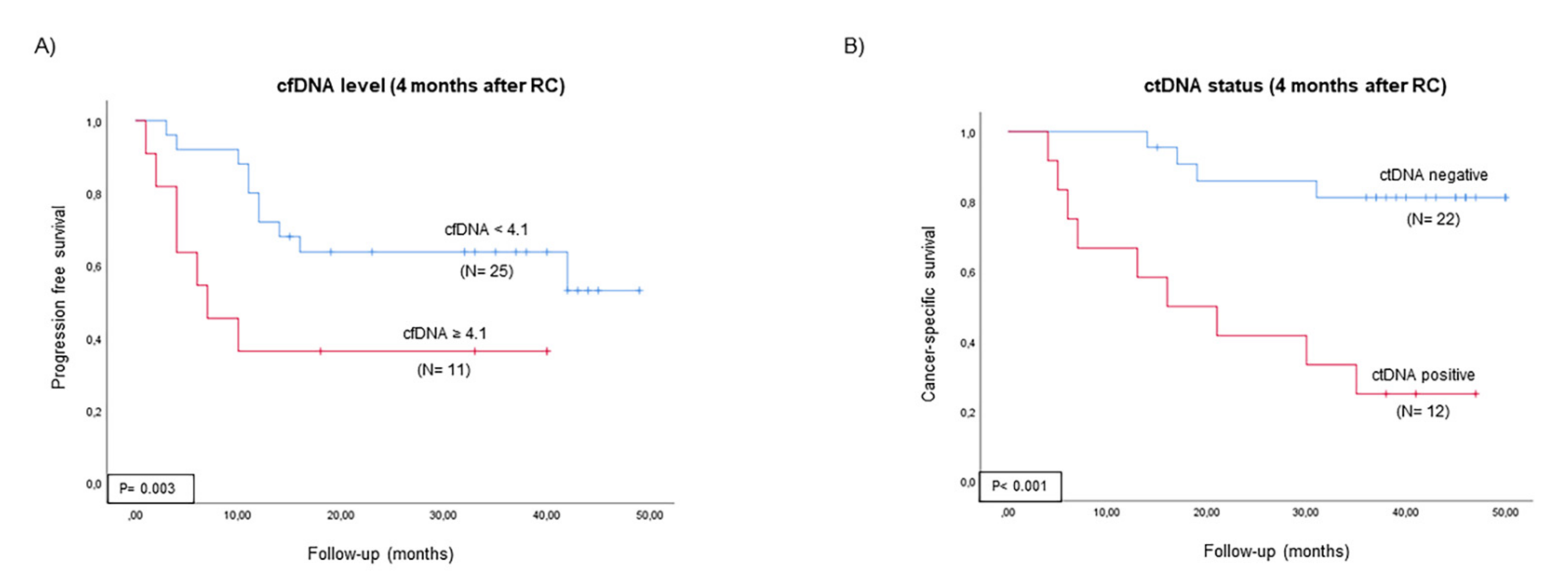
2.4. Prognostic Value of ctDNA and cfDNA
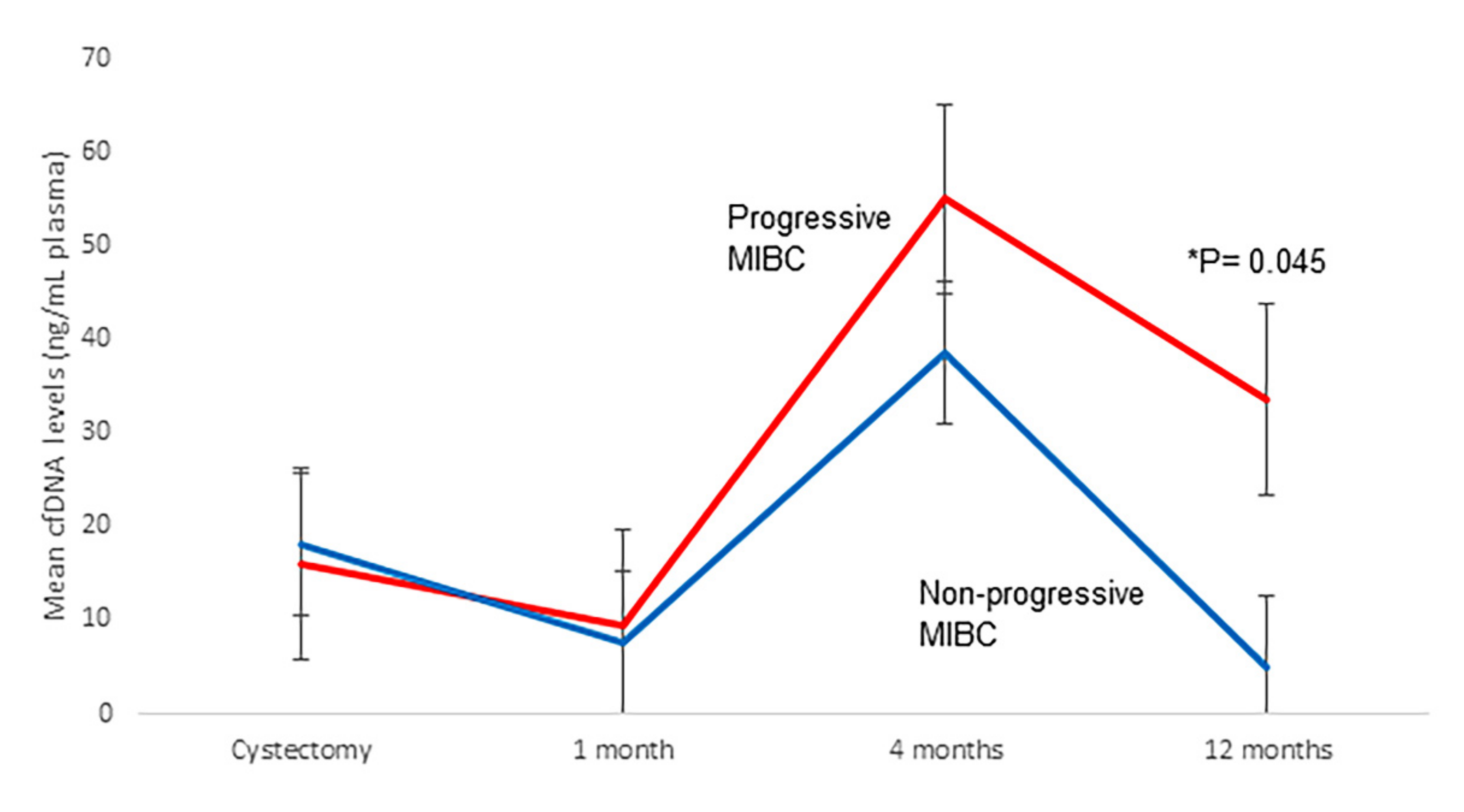
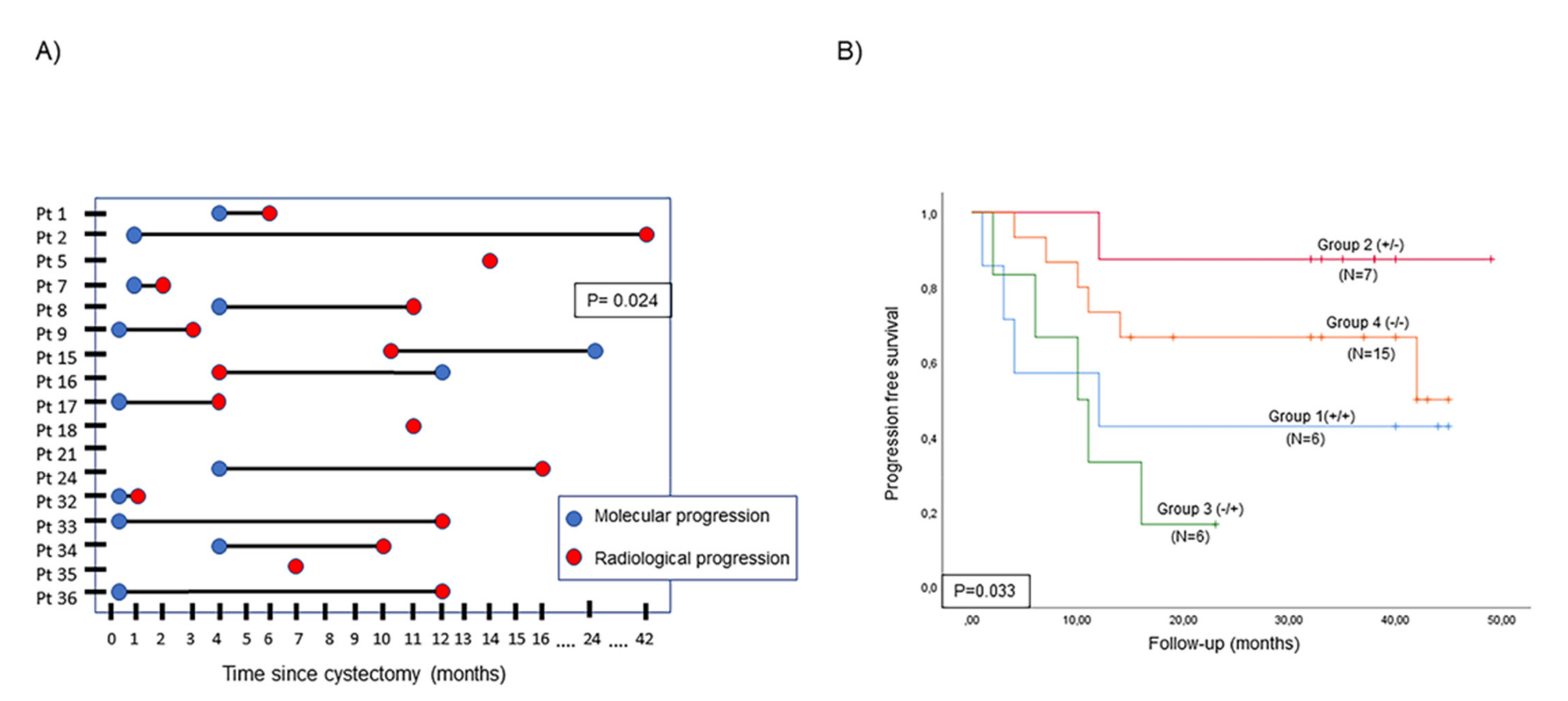
2.5. Detection of Tumor Progression According to Changes in ctDNA Status and cfDNA Level
2.6. Prognostic Value of Changes in ctDNA Status and cfDNA Level
3. Discussion
4. Materials and Methods
4.1. Patients and Samples
4.2. Targeted Next-Generation Sequencing of Tissue Samples
4.3. Blood Sample Procedures
4.4. Droplet Digital PCR
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.; Cowan, N.C.; Efstathiou, J.A.; Fietkau, R.; Gakis, G.; Hernández, V.; Lorch, A.; et al. European Association of Urology Guidelines on Muscle Invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, R.J.; Van Der Meijden, A.P.M.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-Muscle-Invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo Jiménez, G.; Herranz Amo, F.; Arranz Arija, J.A.; Rodríguez Fernández, E.; Subirá Ríos, D.; Lledó García, E.; Bueno Chomón, G.; Cancho Gil, M.J.; Carballido Rodríguez, J.; Hernández Fernández, C. Effect of Adjuvant Chemotherapy in Locally Advanced Urothelial Carcinoma of the Bladder Treated with Cystectomy. Actas Urológicas Españolas 2020, 44, 94–102. [Google Scholar] [CrossRef]
- Paik, M.L.; Scolieri, M.J.; Brown, S.L.; Spirnak, J.P.; Resnick, M.I. Limitations of Computerized Tomography in Staging Invasive Bladder Cancer before Radical Cystectomy. J. Urol. 2000, 163, 1693–1696. [Google Scholar] [CrossRef]
- Martins, I.; Ribeiro, I.P.; Jorge, J.; Gonçalves, A.C.; Sarmento-Ribeiro, A.B.; Melo, J.B.; Carreira, I.M. Liquid Biopsies: Applications for Cancer Diagnosis and Monitoring. Genes 2021, 12, 349. [Google Scholar] [CrossRef]
- De Rubis, G.; Rajeev Krishnan, S.; Bebawy, M. Liquid Biopsies in Cancer Diagnosis, Monitoring, and Prognosis. Trends Pharmacol. Sci. 2019, 40, 172–186. [Google Scholar] [CrossRef]
- Stewart, C.M.; Tsui, D.W.Y. Circulating Cell-Free DNA for Non-Invasive Cancer Management. Cancer Genet. 2018, 228–229, 169–179. [Google Scholar] [CrossRef]
- Fernandez-Garcia, D.; Hills, A.; Page, K.; Hastings, R.K.; Toghill, B.; Goddard, K.S.; Ion, C.; Ogle, O.; Boydell, A.R.; Gleason, K.; et al. Plasma Cell-Free DNA (CfDNA) as a Predictive and Prognostic Marker in Patients with Metastatic Breast Cancer. Breast Cancer Res. 2019, 21, 149. [Google Scholar] [CrossRef]
- Lin, L.H.; Chang, K.W.; Kao, S.Y.; Cheng, H.W.; Liu, C.J. Increased Plasma Circulating Cell-Free DNA Could Be a Potential Marker for Oral Cancer. Int. J. Mol. Sci. 2018, 19, 3303. [Google Scholar] [CrossRef]
- Kienel, A.; Porres, D.; Heidenreich, A.; Pfister, D. CfDNA as a Prognostic Marker of Response to Taxane Based Chemotherapy in Patients with Prostate Cancer. J. Urol. 2015, 194, 966–971. [Google Scholar] [CrossRef]
- Green, E.A.; Li, R.; Albiges, L.; Choueiri, T.K.; Freedman, M.; Pal, S.; Dyrskjøt, L.; Kamat, A.M. Clinical Utility of Cell-Free and Circulating Tumor DNA in Kidney and Bladder Cancer: A Critical Review of Current Literature. Eur. Urol. Oncol. 2021, 4, 893–903. [Google Scholar] [CrossRef]
- Bronkhorst, A.J.; Ungerer, V.; Holdenrieder, S. The emerging role of cell-free DNA as a molecular marker for cancer management. Biomol. Detect. Quantif. 2019, 17, 100087. [Google Scholar] [CrossRef]
- Toledano-Fonseca, M.; Cano, M.T.; Inga, E.; Rodríguez-Alonso, R.; Gómez-España, M.A.; Guil-Luna, S.; Mena-Osuna, R.; de la Haba-Rodríguez, J.R.; Rodríguez-Ariza, A.; Aranda, E. Circulating Cell-Free Dna-Based Liquid Biopsy Markers for the Non-Invasive Prognosis and Monitoring of Metastatic Pancreatic Cancer. Cancers 2020, 12, 1754. [Google Scholar] [CrossRef]
- González de Aledo-Castillo, J.M.; Arcocha, A.; Victoria, I.; Martinez-Puchol, A.I.; Sánchez, C.; Jares, P.; Rodríguez, G.F.; Viñolas, N.; Reyes, R.; Reguart, N.; et al. Molecular Characterization of Advanced Non-Small Cell Lung Cancer Patients by CfDNA Analysis: Experience from Routine Laboratory Practice. J. Thorac. Dis. 2021, 13, 1658–1670. [Google Scholar] [CrossRef]
- Fettke, H.; Kwan, E.M.; Bukczynska, P.; Ng, N.; Nguyen-Dumont, T.; Southey, M.C.; Davis, I.D.; Mant, A.; Parente, P.; Pezaro, C.; et al. Prognostic Impact of Total Plasma Cell-Free DNA Concentration in Androgen Receptor Pathway Inhibitor-Treated Metastatic Castration-Resistant Prostate Cancer. Eur. Urol. Focus 2021, 7, 1287–1291. [Google Scholar] [CrossRef]
- Alix-Panabières, C.; Schwarzenbach, H.; Pantel, K. Circulating Tumor Cells and Circulating Tumor DNA. Annu. Rev. Med. 2012, 63, 199–215. [Google Scholar] [CrossRef]
- Vandekerkhove, G.; Lavoie, J.M.; Annala, M.; Murtha, A.J.; Sundahl, N.; Walz, S.; Sano, T.; Taavitsainen, S.; Ritch, E.; Fazli, L.; et al. Plasma CtDNA Is a Tumor Tissue Surrogate and Enables Clinical-Genomic Stratification of Metastatic Bladder Cancer. Nat. Commun. 2021, 12, 184. [Google Scholar] [CrossRef]
- Christensen, E.; Birkenkamp-Demtröder, K.; Nordentoft, I.; Høyer, S.; van der Keur, K.; van Kessel, K.; Zwarthoff, E.; Agerbæk, M.; Ørntoft, T.F.; Jensen, J.B.; et al. Liquid Biopsy Analysis of FGFR3 and PIK3CA Hotspot Mutations for Disease Surveillance in Bladder Cancer. Eur. Urol. 2017, 71, 961–969. [Google Scholar] [CrossRef]
- Christensen, E.; Nordentoft, I.; Vang, S.; Birkenkamp-Demtröder, K.; Jensen, J.B.; Agerbæk, M.; Pedersen, J.S.; Dyrskjøt, L. Optimized Targeted Sequencing of Cell-Free Plasma DNA from Bladder Cancer Patients. Sci. Rep. 2018, 8, 1917. [Google Scholar] [CrossRef]
- Birkenkamp-Demtröder, K.; Christensen, E.; Nordentoft, I.; Knudsen, M.; Taber, A.; Høyer, S.; Lamy, P.; Agerbæk, M.; Jensen, J.B.; Dyrskjøt, L. Monitoring Treatment Response and Metastatic Relapse in Advanced Bladder Cancer by Liquid Biopsy Analysis. Eur. Urol. 2018, 73, 535–540. [Google Scholar] [CrossRef]
- Pritchard, J.J.G.; Hamilton, G.; Hurst, C.D.; Fraser, S.; Orange, C.; Knowles, M.A.; Jones, R.J.; Leung, H.Y.; Iwata, T. Monitoring of Urothelial Cancer Disease Status after Treatment by Digital Droplet PCR Liquid Biopsy Assays. Urol. Oncol. 2020, 38, 737. [Google Scholar] [CrossRef]
- Tan, M.P.; Attard, G.; Huddart, R.A. Circulating Tumour DNA in Muscle-Invasive Bladder Cancer. Int. J. Mol. Sci. 2018, 19, 2568. [Google Scholar] [CrossRef] [Green Version]
- Carrasco, R.; Ingelmo-Torres, M.; Gómez, A.; Roldán, F.L.; Segura, N.; Ribal, M.J.; Alcaraz, A.; Izquierdo, L.; Mengual, L. Prognostic Implication of TERT Promoter Mutation and Circulating Tumor Cells in Muscle-Invasive Bladder Cancer. World J. Urol. 2022, 40, 2033–2039. [Google Scholar] [CrossRef]
- Ignatiadis, M.; Sledge, G.W.; Jeffrey, S.S. Liquid Biopsy Enters the Clinic—Implementation Issues and Future Challenges. Nat. Rev. Clin. Oncol. 2021, 18, 297–312. [Google Scholar] [CrossRef]
- Cheng, M.L.; Pectasides, E.; Hanna, G.J.; Parsons, H.A.; Choudhury, A.D.; Oxnard, G.R. Circulating Tumor DNA in Advanced Solid Tumors: Clinical Relevance and Future Directions. CA Cancer J. Clin. 2021, 71, 176–190. [Google Scholar] [CrossRef]
- Heitzer, E.; van den Broek, D.; Denis, M.G.; Hofman, P.; Hubank, M.; Mouliere, F.; Paz-Ares, L.; Schuuring, E.; Sültmann, H.; Vainer, G.; et al. Recommendations for a Practical Implementation of Circulating Tumor DNA Mutation Testing in Metastatic Non-Small-Cell Lung Cancer. ESMO Open 2022, 7, 100399. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, T.; Wang, J.; Wang, J.; Xu, Y.; Zhao, X.; Ou, Q.; Shao, Y.; Wang, X.; Wu, Y.; et al. The Clinical Utility of Dynamic CtDNA Monitoring in Inoperable Localized NSCLC Patients. Mol. Cancer 2022, 21, 117. [Google Scholar] [CrossRef]
- Kinde, I.; Munari, E.; Faraj, S.F.; Hruban, R.H.; Schoenberg, M.; Bivalacqua, T.; Allaf, M.; Springer, S.; Wang, Y.; Diaz, L.A.; et al. TERT Promoter Mutations Occur Early in Urothelial Neoplasia and Are Biomarkers of Early Disease and Disease Recurrence in Urine. Cancer Res. 2013, 73, 7162. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, Y.; Fujita, K.; Matsuzaki, K.; Eich, M.L.; Tomiyama, E.; Matsushita, M.; Koh, Y.; Nakano, K.; Wang, C.; Ishizuya, Y.; et al. Clinical Significance of Hotspot Mutation Analysis of Urinary Cell-Free DNA in Urothelial Bladder Cancer. Front. Oncol. 2020, 10, 755. [Google Scholar] [CrossRef]
- Hayashi, Y.; Fujita, K.; Nojima, S.; Tomiyama, E.; Matsushita, M.; Koh, Y.; Nakano, K.; Wang, C.; Ishizuya, Y.; Kato, T.; et al. TERT C228T Mutation in Non-malignant Bladder Urothelium Is Associated with Intravesical Recurrence for Patients with Non-muscle Invasive Bladder Cancer. Mol. Oncol. 2020, 14, 2375. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, A.C.; Calapre, L.; Pereira, M.R.; Giardina, T.; Robinson, C.; Khattak, M.A.; Meniawy, T.M.; Pritchard, A.L.; Hayward, N.K.; Amanuel, B.; et al. Sensitive Droplet Digital PCR Method for Detection of TERT Promoter Mutations in Cell Free DNA from Patients with Metastatic Melanoma. Oncotarget 2017, 8, 78890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oversoe, S.K.; Clement, M.S.; Pedersen, M.H.; Weber, B.; Aagaard, N.K.; Villadsen, G.E.; Grønbæk, H.; Hamilton-Dutoit, S.J.; Sorensen, B.S.; Kelsen, J. TERT Promoter Mutated Circulating Tumor DNA as a Biomarker for Prognosis in Hepatocellular Carcinoma. Scand. J. Gastroenterol. 2020, 55, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Hirai, M.; Kinugasa, H.; Nouso, K.; Yamamoto, S.; Terasawa, H.; Onishi, Y.; Oyama, A.; Adachi, T.; Wada, N.; Sakata, M.; et al. Prediction of the Prognosis of Advanced Hepatocellular Carcinoma by TERT Promoter Mutations in Circulating Tumor DNA. J. Gastroenterol. Hepatol. 2021, 36, 1118–1125. [Google Scholar] [CrossRef]
- Min, J.; Shay, J.W. TERT Promoter Mutations Enhance Telomerase Activation by Long-Range Chromatin Interactions. Cancer Discov. 2016, 6, 1212–1214. [Google Scholar] [CrossRef] [Green Version]
- Tie, J.; Cohen, J.D.; Wang, Y.; Christie, M.; Simons, K.; Lee, M.; Wong, R.; Kosmider, S.; Ananda, S.; McKendrick, J.; et al. Circulating Tumor DNA Analyses as Markers of Recurrence Risk and Benefit of Adjuvant Therapy for Stage III Colon Cancer Supplemental Content. JAMA Oncol. 2019, 5, 1710–1717. [Google Scholar] [CrossRef]
- Christensen, E.; Birkenkamp-Demtröder, K.; Sethi, H.; Shchegrova, S.; Salari, R.; Nordentoft, I.; Wu, H.T.; Knudsen, M.; Lamy, P.; Lindskrog, S.V.; et al. Early Detection of Metastatic Relapse and Monitoring of Therapeutic Efficacy by Ultra-Deep Sequencing of Plasma Cell-Free DNA in Patients with Urothelial Bladder Carcinoma. J. Clin. Oncol. 2019, 37, 1547–1557. [Google Scholar] [CrossRef]
- Shohdy, K.S.; Villamar, D.M.; Cao, Y.; Trieu, J.; Price, K.S.; Nagy, R.; Tagawa, S.T.; Molina, A.M.; Sternberg, C.N.; Nanus, D.M.; et al. Serial CtDNA Analysis Predicts Clinical Progression in Patients with Advanced Urothelial Carcinoma. Br. J. Cancer 2022, 126, 430–439. [Google Scholar] [CrossRef]
- Magbanua, M.J.M.; Swigart, L.B.; Wu, H.T.; Hirst, G.L.; Yau, C.; Wolf, D.M.; Tin, A.; Salari, R.; Shchegrova, S.; Pawar, H.; et al. Circulating Tumor DNA in Neoadjuvant-Treated Breast Cancer Reflects Response and Survival. Ann. Oncol. 2021, 32, 229–239. [Google Scholar] [CrossRef]
- Tie, J.; Wang, Y.; Tomasetti, C.; Li, L.; Springer, S.; Kinde, I.; Silliman, N.; Tacey, M.; Wong, H.L.; Christie, M.; et al. Circulating Tumor DNA Analysis Detects Minimal Residual Disease and Predicts Recurrence in Patients with Stage II Colon Cancer. Sci. Transl. Med. 2016, 8, 346ra92. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TOTAL MIBCN (% or Range) | Progressive MIBCN (% or Range) | Non-Progressive MIBC N (% or Range) | |
|---|---|---|---|
| (N = 37) | (N = 17) | (N = 20) | |
| Gender | |||
| Male | 30 (81) | 13 (76.4) | 17 (85) |
| Female | 7 (19) | 4 (23.6) | 3 (15) |
| Median Age (yr) | 71 (51–85) | 72 (51–85) | 70 (59–83) |
| Pathological Stage | |||
| <pT2 | 7 (19) | 1 (5.9) | 6 (30) |
| pT2 | 9 (24) | 4 (23.6) | 5 (25) |
| pT3 | 15 (41) | 7 (41.2) | 8 (40) |
| pT4 | 6 (16) | 5 (29.4) | 1 (5) |
| Lymph Nodes (LN) | |||
| LN+ | 4 (11) | 2 (11.8) | 2 (10) |
| pT2 | 1 (2.7) | - | 1 (5) |
| pT3 | 2 (5.4) | 1 (5.9) | 1 (5) |
| pT4 | 1 (2.7) | 1 (5.9) | - |
| LN- | 33 (89) | 15 (88.2) | 18 (90) |
| Neoadjuvant Chemotherapy | 7 (19) | 4 (23.6) | 3 (15) |
| <pT2 | 2 (5.4) | 1 (5.9) | 1 (5) |
| pT2 | - | - | - |
| pT3 | 3 (8.1) | 1 (5.9) | 2 (10) |
| pT4 | 2 (5.4) | 2 (11.8) | - |
| Adjuvant Chemotherapy | 6 (16) | 1 (5.9) | 5 (25) |
| <pT2 | - | - | - |
| pT2 | 1 (2.7) | - | 1 (5) |
| pT3 | 3 (8.1) | - | 3 (15) |
| pT4 | 2 (5.4) | 1 (5.9) | 1 (5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrasco, R.; Ingelmo-Torres, M.; Gómez, A.; Trullas, R.; Roldán, F.L.; Ajami, T.; Moreno, D.; Rodríguez-Carunchio, L.; Alcaraz, A.; Izquierdo, L.; et al. Cell-Free DNA as a Prognostic Biomarker for Monitoring Muscle-Invasive Bladder Cancer. Int. J. Mol. Sci. 2022, 23, 11732. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911732
Carrasco R, Ingelmo-Torres M, Gómez A, Trullas R, Roldán FL, Ajami T, Moreno D, Rodríguez-Carunchio L, Alcaraz A, Izquierdo L, et al. Cell-Free DNA as a Prognostic Biomarker for Monitoring Muscle-Invasive Bladder Cancer. International Journal of Molecular Sciences. 2022; 23(19):11732. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911732
Chicago/Turabian StyleCarrasco, Raquel, Mercedes Ingelmo-Torres, Ascensión Gómez, Ramón Trullas, Fiorella L. Roldán, Tarek Ajami, Davinia Moreno, Leonardo Rodríguez-Carunchio, Antonio Alcaraz, Laura Izquierdo, and et al. 2022. "Cell-Free DNA as a Prognostic Biomarker for Monitoring Muscle-Invasive Bladder Cancer" International Journal of Molecular Sciences 23, no. 19: 11732. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911732