

A Novel Detection Method of Breast Cancer through a Simple Panel of Biomarkers
 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Patients
2.2. Transcriptional Levels of Target Markers
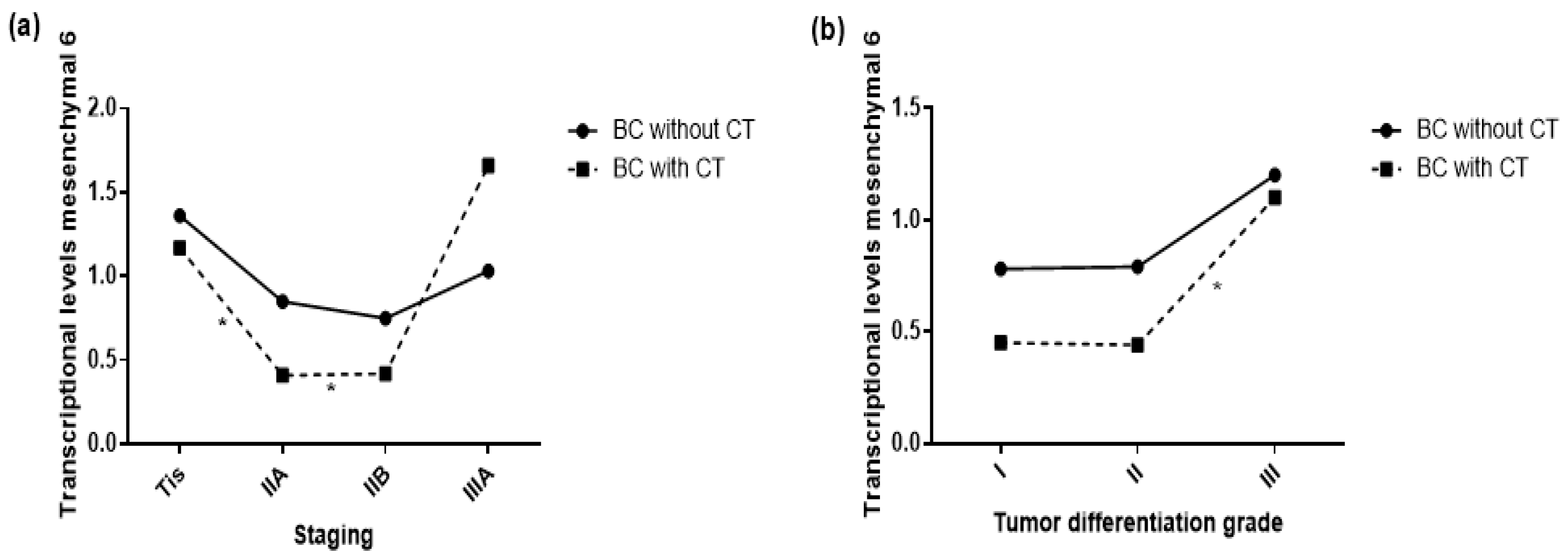
2.3. Transcriptional Levels of Target Markers and Primary Tumor Characteristics
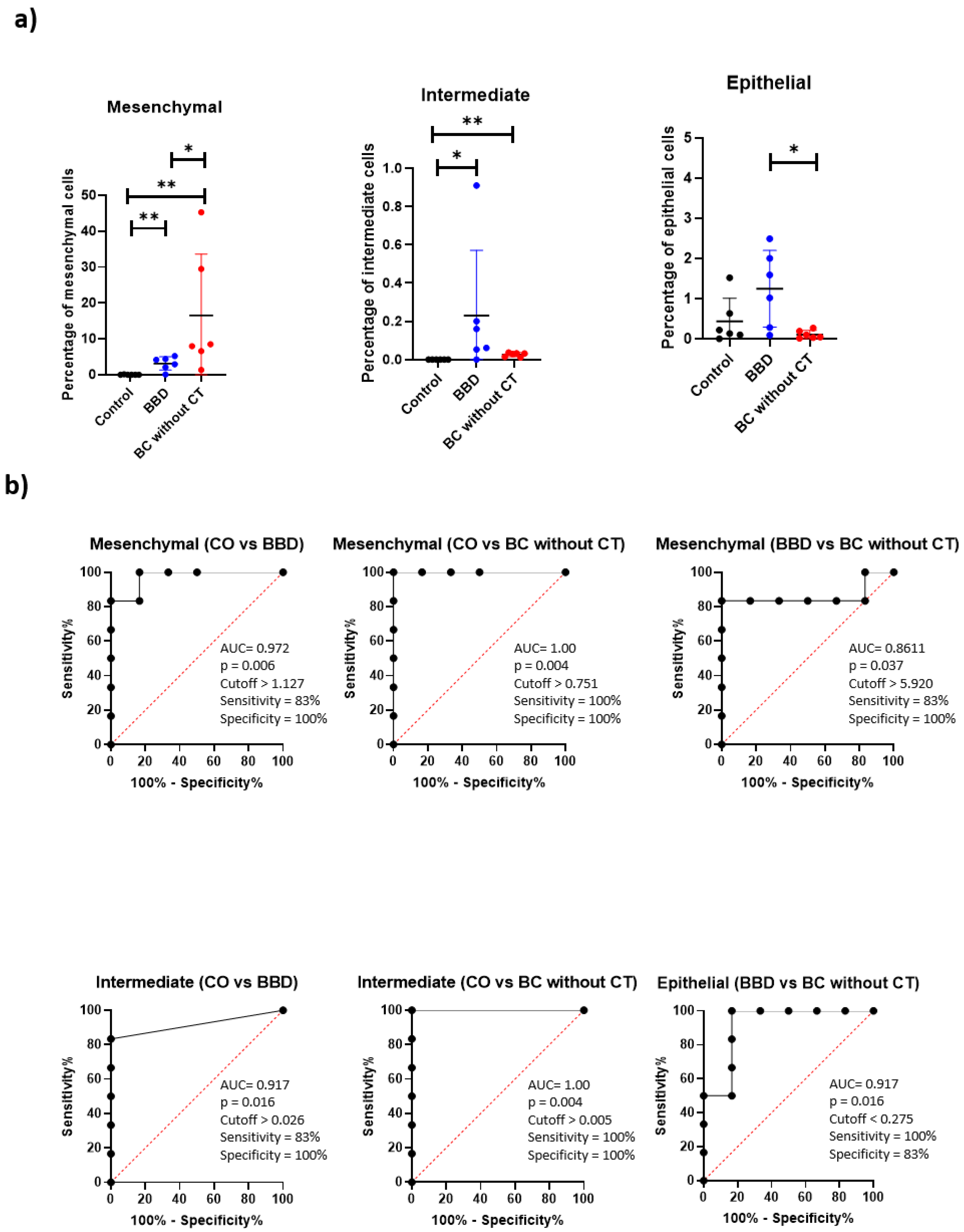
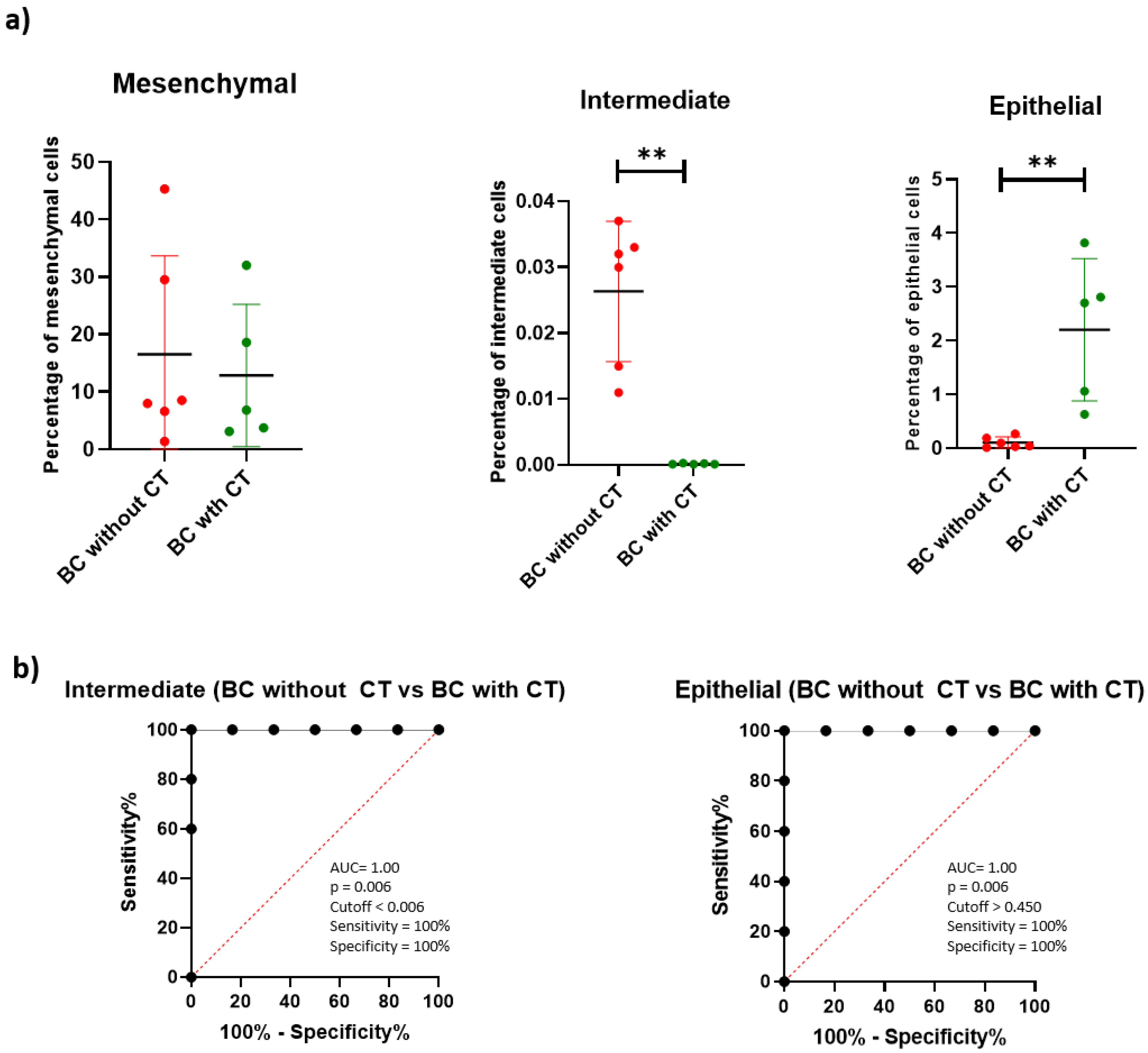
2.4. Populations of CTCs
2.5. Pre-Validation of Diagnostic Panel by ROC Curve
2.6. Pre-Validation of Treatment Monitoring Panel by ROC Curve
3. Discussion
4. Materials and Methods
4.1. Studied Patients
4.2. Analyses of Transcriptional Levels
4.2.1. Sample Collection
4.2.2. Extraction of Total RNA from Peripheral Blood and Tissue
4.2.3. Reverse Transcription
4.2.4. PCR for Sample Validation
4.2.5. Analysis of Specific Oligonucleotides
4.2.6. Relative Transcriptional Quantification by qPCR
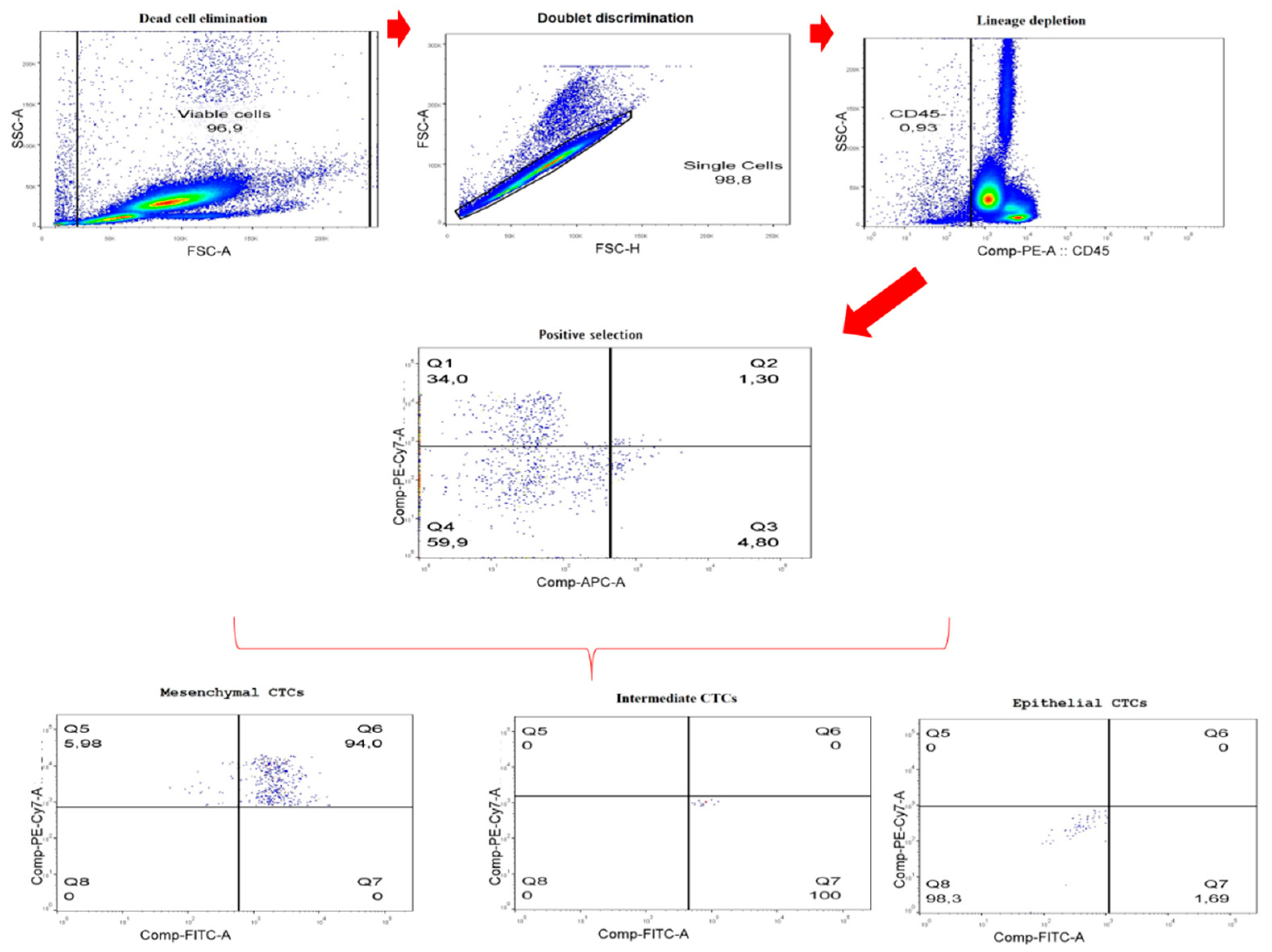
4.3. CTC Characterization by Flow Cytometry
4.4. Statistical Analysis
5. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahmad, A. Breast Cancer Statistics: Recent Trends. In Breast Cancer Metastasis and Drug Resistance: Challenges and Progress; Ahmad, A., Ed.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2019; pp. 1–7. ISBN 978-3-030-20301-6. [Google Scholar]
- Ksiazkiewicz, M.; Markiewicz, A.; Zaczek, A.J. Epithelial-Mesenchymal Transition: A Hallmark in Metastasis Formation Linking Circulating Tumor Cells and Cancer Stem Cells. Pathobiology 2012, 79, 195–208. [Google Scholar] [CrossRef]
- Lambert, A.W.; Pattabiraman, D.R.; Weinberg, R.A. Emerging Biological Principles of Metastasis. Cell 2017, 168, 670–691. [Google Scholar] [CrossRef] [Green Version]
- Khatcheressian, J.L.; Hurley, P.; Bantug, E.; Esserman, L.J.; Grunfeld, E.; Halberg, F.; Hantel, A.; Henry, N.L.; Muss, H.B.; Smith, T.J.; et al. Breast Cancer Follow-up and Management after Primary Treatment: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 961–965. [Google Scholar] [CrossRef]
- Yao, D.; Dai, C.; Peng, S. Mechanism of the Mesenchymal-Epithelial Transition and Its Relationship with Metastatic Tumor Formation. Mol. Cancer Res. 2011, 9, 1608–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhou, B.P. Epithelial-Mesenchymal Transition—A Hallmark of Breast Cancer Metastasis. Cancer Hallm. 2013, 1, 38–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foroni, C.; Broggini, M.; Generali, D.; Damia, G. Epithelial-Mesenchymal Transition and Breast Cancer: Role, Molecular Mechanisms and Clinical Impact. Cancer Treat. Rev. 2012, 38, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Ellsworth, R.E.; Blackburn, H.L.; Shriver, C.D.; Soon-Shiong, P.; Ellsworth, D.L. Molecular Heterogeneity in Breast Cancer: State of the Science and Implications for Patient Care. Semin. Cell Dev. Biol. 2017, 64, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Friedlander, T.W.; Premasekharan, G.; Paris, P.L. Looking Back, to the Future of Circulating Tumor Cells. Pharmacol. Ther. 2014, 142, 271–280. [Google Scholar] [CrossRef]
- Videira, M.; Reis, R.L.; Brito, M.A. Deconstructing Breast Cancer Cell Biology and the Mechanisms of Multidrug Resistance. Biochim. Biophys. Acta 2014, 1846, 312–325. [Google Scholar] [CrossRef]
- Broersen, L.H.A.; van Pelt, G.W.; Tollenaar, R.A.E.M.; Mesker, W.E. Clinical Application of Circulating Tumor Cells in Breast Cancer. Cell. Oncol. 2014, 37, 9–15. [Google Scholar] [CrossRef]
- Reya, T.; Morrison, S.J.; Clarke, M.F.; Weissman, I.L. Stem Cells, Cancer, and Cancer Stem Cells. Nature 2001, 414, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Settleman, J. EMT, Cancer Stem Cells and Drug Resistance: An Emerging Axis of Evil in the War on Cancer. Oncogene 2010, 29, 4741–4751. [Google Scholar] [CrossRef] [Green Version]
- Shibue, T.; Weinberg, R.A. EMT, CSCs, and Drug Resistance: The Mechanistic Link and Clinical Implications. Nat. Rev. Clin. Oncol. 2017, 14, 611–629. [Google Scholar] [CrossRef] [Green Version]
- Jelski, W.; Chrostek, L.; Szmitkowski, M.; Markiewicz, W. The Activity of Class I, II, III and IV Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase in Breast Cancer. Clin. Exp. Med. 2006, 6, 89–93. [Google Scholar] [CrossRef]
- Jelski, W.; Chrostek, L.; Markiewicz, W.; Szmitkowski, M. Activity of Alcohol Dehydrogenase (ADH) Isoenzymes and Aldehyde Dehydrogenase (ALDH) in the Sera of Patients with Breast Cancer. J. Clin. Lab. Anal. 2006, 20, 105–108. [Google Scholar] [CrossRef]
- Moreb, J.S. Aldehyde Dehydrogenase as a Marker for Stem Cells. Curr. Stem Cell Res. Ther. 2008, 3, 237–246. [Google Scholar] [CrossRef]
- Vieira, R.R.; Campos, L.H.; Jesus, L.H.; Klabunde, C.; de Oliveira Gamba, T.; Flores, I.L.; Oliveira, M.G.; Rados, P.V. Overexpression of ALDH1 and EMT Marker Profile Are Linked with Unfavorable Outcome in Head and Neck Cancer. Med. Oral Patol. Oral Cirugía Bucal 2020, 25, e752–e761. [Google Scholar] [CrossRef]
- Ginestier, C.; Hur, M.H.; Charafe-Jauffret, E.; Monville, F.; Dutcher, J.; Brown, M.; Jacquemier, J.; Viens, P.; Kleer, C.G.; Liu, S.; et al. ALDH1 Is a Marker of Normal and Malignant Human Mammary Stem Cells and a Predictor of Poor Clinical Outcome. Cell Stem Cell 2007, 1, 555–567. [Google Scholar] [CrossRef] [Green Version]
- Koh, Y.W.; Han, J.-H.; Haam, S.; Jung, J. ALDH1 Expression Correlates with an Epithelial-like Phenotype and Favorable Prognosis in Lung Adenocarcinoma: A Study Based on Immunohistochemistry and MRNA Expression Data. J. Cancer Res. Clin. Oncol. 2019, 145, 1427–1436. [Google Scholar] [CrossRef]
- Liang, D.H.; Hall, C.; Lucci, A. Circulating Tumor Cells in Breast Cancer. In Tumor Liquid Biopsies; Schaffner, F., Merlin, J.-L., von Bubnoff, N., Eds.; Recent Results in Cancer Research; Springer International Publishing: Cham, Switzerland, 2020; Volume 215, pp. 127–145. ISBN 978-3-030-26438-3. [Google Scholar]
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.J.; Uhr, J.W.; Terstappen, L.W.M.M. Tumor Cells Circulate in the Peripheral Blood of All Major Carcinomas but Not in Healthy Subjects or Patients With Nonmalignant Diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.M.M.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Vardas, V.; Politaki, E.; Pantazaka, E.; Georgoulias, V.; Kallergi, G. Epithelial-to-Mesenchymal Transition of Tumor Cells: Cancer Progression and Metastasis. Int. J. Dev. Biol. 2021, 66, 277–283. [Google Scholar] [CrossRef]
- Franke, W.W.; Grund, C.; Kuhn, C.; Jackson, B.W.; Illmensee, K. Formation of Cytoskeletal Elements During Mouse Embryogenesis: III. Primary Mesenchymal Cells and the First Appearance of Vimentin Filaments. Differentiation 1982, 23, 43–59. [Google Scholar] [CrossRef]
- Thiery, J.P. Epithelial-Mesenchymal Transitions in Tumour Progression. Nat. Rev. Cancer 2002, 2, 442–454. [Google Scholar] [CrossRef]
- Todenhöfer, T.; Pantel, K.; Stenzl, A.; Werner, S. Pathophysiology of Tumor Cell Release into the Circulation and Characterization of CTC. In Tumor Liquid Biopsies; Schaffner, F., Merlin, J.-L., von Bubnoff, N., Eds.; Recent Results in Cancer Research; Springer International Publishing: Cham, Switzerland, 2020; pp. 3–24. ISBN 978-3-030-26439-0. [Google Scholar]
- Mendez, M.G.; Kojima, S.-I.; Goldman, R.D. Vimentin Induces Changes in Cell Shape, Motility, and Adhesion during the Epithelial to Mesenchymal Transition. FASEB J. 2010, 24, 1838. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Xu, G.; Wu, M.; Zhang, Y.; Li, Q.; Liu, P.; Zhu, T.; Song, A.; Zhao, L.; Han, Z.; et al. Overexpression of Vimentin Contributes to Prostate Cancer Invasion and Metastasis via Src Regulation. Anticancer Res. 2008, 28, 327–334. [Google Scholar]
- Zelenko, Z.; Gallagher, E.J.; Tobin-Hess, A.; Belardi, V.; Rostoker, R.; Blank, J.; Dina, Y.; LeRoith, D. Silencing Vimentin Expression Decreases Pulmonary Metastases in a Pre-Diabetic Mouse Model of Mammary Tumor Progression. Oncogene 2017, 36, 1394–1403. [Google Scholar] [CrossRef] [Green Version]
- Klingbeil, P.; Natrajan, R.; Everitt, G.; Vatcheva, R.; Marchio, C.; Palacios, J.; Buerger, H.; Reis-Filho, J.S.; Isacke, C.M. CD44 Is Overexpressed in Basal-like Breast Cancers but Is Not a Driver of 11p13 Amplification. Breast Cancer Res. Treat. 2009, 120, 95–109. [Google Scholar] [CrossRef] [Green Version]
- Naor, D.; Sionov, R.V.; Ish-Shalom, D. CD44: Structure, Function, and Association with the Malignant Process. Adv. Cancer Res. 1997, 71, 241–319. [Google Scholar] [CrossRef]
- Patrawala, L.; Calhoun, T.; Schneider-Broussard, R.; Li, H.; Bhatia, B.; Tang, S.; Reilly, J.G.; Chandra, D.; Zhou, J.; Claypool, K.; et al. Highly Purified CD44+ Prostate Cancer Cells from Xenograft Human Tumors Are Enriched in Tumorigenic and Metastatic Progenitor Cells. Oncogene 2006, 25, 1696–1708. [Google Scholar] [CrossRef] [Green Version]
- Senbanjo, L.T.; Chellaiah, M.A. CD44: A Multifunctional Cell Surface Adhesion Receptor Is a Regulator of Progression and Metastasis of Cancer Cells. Front. Cell Dev. Biol. 2017, 5, 18. [Google Scholar] [CrossRef]
- Gires, O.; Pan, M.; Schinke, H.; Canis, M.; Baeuerle, P.A. Expression and Function of Epithelial Cell Adhesion Molecule EpCAM: Where Are We after 40 Years? Cancer Metastasis Rev. 2020, 39, 969–987. [Google Scholar] [CrossRef]
- Hyun, K.-A.; Koo, G.-B.; Han, H.; Sohn, J.; Choi, W.; Kim, S.-I.; Jung, H.-I.; Kim, Y.-S. Epithelial-to-Mesenchymal Transition Leads to Loss of EpCAM and Different Physical Properties in Circulating Tumor Cells from Metastatic Breast Cancer. Oncotarget 2016, 7, 24677–24687. [Google Scholar] [CrossRef] [Green Version]
- Keller, L.; Werner, S.; Pantel, K. Biology and Clinical Relevance of EpCAM. Cell Stress 2019, 3, 165–180. [Google Scholar] [CrossRef] [Green Version]
- Deryugina, E.I.; Kiosses, W.B. Intratumoral Cancer Cell Intravasation Can Occur Independent of Invasion into the Adjacent Stroma. Cell Rep. 2017, 19, 601–616. [Google Scholar] [CrossRef] [Green Version]
- Zavyalova, M.V.; Denisov, E.V.; Tashireva, L.A.; Savelieva, O.E.; Kaigorodova, E.V.; Krakhmal, N.V.; Perelmuter, V.M. Intravasation as a Key Step in Cancer Metastasis. Biochemistry 2019, 84, 762–772. [Google Scholar] [CrossRef]
- Savelieva, O.E.; Tashireva, L.A.; Kaigorodova, E.V.; Buzenkova, A.V.; Mukhamedzhanov, R.K.; Grigoryeva, E.S.; Zavyalova, M.V.; Tarabanovskaya, N.A.; Cherdyntseva, N.V.; Perelmuter, V.M. Heterogeneity of Stemlike Circulating Tumor Cells in Invasive Breast Cancer. Int. J. Mol. Sci. 2020, 21, E2780. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Lu, W.; Tang, C.; Liu, Y.; Sun, J.; Mu, X.; Zhang, L.; Dai, B.; Li, X.; Zhuo, H.; et al. Label-Free Isolation and MRNA Detection of Circulating Tumor Cells from Patients with Metastatic Lung Cancer for Disease Diagnosis and Monitoring Therapeutic Efficacy. Anal. Chem. 2015, 87, 11893–11900. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating Tumor Cells: Biology and Clinical Significance. Signal Transduct. Target. Ther. 2021, 6, 404. [Google Scholar] [CrossRef]
- Buono, G.; Gerratana, L.; Bulfoni, M.; Provinciali, N.; Basile, D.; Giuliano, M.; Corvaja, C.; Arpino, G.; Del Mastro, L.; De Placido, S.; et al. Circulating Tumor DNA Analysis in Breast Cancer: Is It Ready for Prime-Time? Cancer Treat. Rev. 2019, 73, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Løberg, M.; Lousdal, M.L.; Bretthauer, M.; Kalager, M. Benefits and Harms of Mammography Screening. Breast Cancer Res. 2015, 17, 63. [Google Scholar] [CrossRef] [PubMed]
- Agnoletto, C.; Corrà, F.; Minotti, L.; Baldassari, F.; Crudele, F.; Cook, W.J.J.; Leva, G.D.; d’Adamo, A.P.; Gasparini, P.; Volinia, S. Heterogeneity in Circulating Tumor Cells: The Relevance of the Stem-Cell Subset. Cancers 2019, 11, 483. [Google Scholar] [CrossRef] [Green Version]
- Kröger, C.; Afeyan, A.; Mraz, J.; Eaton, E.N.; Reinhardt, F.; Khodor, Y.L.; Thiru, P.; Bierie, B.; Ye, X.; Burge, C.B.; et al. Acquisition of a Hybrid E/M State Is Essential for Tumorigenicity of Basal Breast Cancer Cells. Proc. Natl. Acad. Sci. USA 2019, 116, 7353–7362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, D.; Gupta, D.; Shankar, S.; Srivastava, R.K. Biomolecular Characterization of Exosomes Released from Cancer Stem Cells: Possible Implications for Biomarker and Treatment of Cancer. Oncotarget 2014, 6, 3280–3291. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-J.; Wei, L.; Li, J.; Zheng, Y.-Q.; Li, X.-R. Status Quo and Development Trend of Breast Biopsy Technology. Gland Surg. 2013, 2, 15–24. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Position Paper on Mammography Screening; World Health Organization: Geneva, Switzerland, 2014; ISBN 978-92-4-150793-6. [Google Scholar]
- Smerage, J.B.; Barlow, W.E.; Hortobagyi, G.N.; Winer, E.P.; Leyland-Jones, B.; Srkalovic, G.; Tejwani, S.; Schott, A.F.; O’Rourke, M.A.; Lew, D.L.; et al. Circulating Tumor Cells and Response to Chemotherapy in Metastatic Breast Cancer: SWOG S0500. J. Clin. Oncol. 2014, 32, 3483–3489. [Google Scholar] [CrossRef]
- Araújo, T.G.; Paiva, C.E.; Rocha, R.M.; Maia, Y.C.; Sena, A.A.; Ueira-Vieira, C.; Carneiro, A.P.; Almeida, J.F.; de Faria, P.R.; Santos, D.W.; et al. A novel highly reactive Fab antibody for breast cancer tissue diagnostics and staging also discriminates a subset of good prognostic triple-negative breast cancers. Cancer Lett. 2014, 343, 275–285. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1º Phase | 2º Phase | |||
|---|---|---|---|---|
| Variable | Patients (n = 62) | Patients (n = 11) | ||
| n | % | n | % | |
| Age (years) | ||||
| Mean ± SD | 54.76 ± 11.00 | 53.80 ± 9.13 | ||
| Tumor size | ||||
| pTis | 9 | 14.5 | 0 | 0.0 |
| pT1 | 16 | 25.8 | 0 | 0.0 |
| pT2 | 24 | 38.7 | 7 | 63.6 |
| pT3 | 4 | 6.5 | 3 | 27.3 |
| pT4 | 1 | 1.6 | 0 | 0.0 |
| NR | 8 | 12.9 | 1 | 9.1 |
| Regional Lymph nodes | ||||
| pN0 | 31 | 50.0 | 5 | 45.4 |
| pN1 | 14 | 22.6 | 3 | 27.3 |
| pN2 | 5 | 8.1 | 1 | 9.1 |
| pN3 | 2 | 3.2 | 0 | 0.0 |
| NR | 10 | 16.1 | 2 | 18.2 |
| Tumor Stage | ||||
| 0 | 10 | 16.1 | 0 | 0 |
| IA | 10 | 16.1 | 0 | 0 |
| IIA | 15 | 24.2 | 5 | 45.4 |
| IIB | 8 | 12.9 | 4 | 36.4 |
| IIIA | 7 | 11.3 | 1 | 9.1 |
| IIIC | 2 | 3.2 | 0 | 0.0 |
| NR | 10 | 16.1 | 1 | 9.1 |
| Histological grade | ||||
| G1 | 7 | 11.3 | 0 | 0.0 |
| G2 | 27 | 43.5 | 3 | 27.3 |
| G3 | 16 | 25.8 | 7 | 63.6 |
| NR | 12 | 19.4 | 1 | 9.1 |
| Molecular subtyp | ||||
| ER-, PR-, HER2-, and CK5/6+ or EGFR+ | 8 | 12.9 | 2 | 18.2 |
| ER-, PR-, and HER2+ | 8 | 12.9 | 1 | 9.1 |
| ER+ and/or PR+, HER2-, and Ki67 < 14 | 21 | 33.9 | 1 | 9.1 |
| ER+ and/or PR+, HER2-, and Ki67 ≥ 14 | 7 | 11.3 | 3 | 27.2 |
| ER+ and/or PR+ and HER2+ | 16 | 25.8 | 2 | 18.2 |
| NR | 2 | 3.2 | 2 | 18.2 |
| Chemotherapy | ||||
| No | 49 | 79.0 | 6 | 54.5 |
| Yes | 13 | 21.0 | 5 | 45.5 |
| Markers | BC | BBD | p Value | ||
|---|---|---|---|---|---|
| n | Median (p25-p75)/Mean(±SD) | n | Median (p25-p75)/Mean(±SD) | ||
| Bloodstream | |||||
| Epithelial 1 1 | 36 | 0.45 (0.16–0.90) | 15 | 0.60 (0.44–1.77) | 0.097 |
| Epithelial 2 1 | 36 | 0.60 (0.27–1.49) | 15 | 0.96 (0.24–1.84) | 0.656 |
| Epithelial 3 1 | 36 | 1.11 (0.49–2.27) | 16 | 0.74 (0.59–1.56) | 0.868 |
| Epithelial 4 1 | 35 | 1.71 (0.84–3.43) | 15 | 0.82 (0.38–1.82) | 0.113 |
| Epithelial 5 1 | 29 | 1.68 (0.83–3.46) | 12 | 1.04 (0.78–2.25) | 0.271 |
| Epithelial 6 1 | 28 | 1.39 (0.35–3.22) | 13 | 1.31 (0.43–5.14) | 0.746 |
| Mesenchymal 1 2 | 17 | 0.84 (0.95) | 8 | 1.09 (1.07) | 0.574 |
| Mesenchymal 2 1 | 24 | 2.07 (0.86–4.11) | 9 | 0.92 (0.45–1.99) | 0.154 |
| Mesenchymal 3 1 | 28 | 1.69 (0.70–3.69) | 12 | 1.08 (0.73–2.45) | 0.590 |
| Mesenchymal 4 1 | 27 | 1.75 (0.66–4.35) | 12 | 0.74 (0.38–2.47) | 0.086 |
| Mesenchymal 5 1 | 29 | 0.78 (0.47–1.17) | 13 | 0.64 (0.18–1.06) | 0.174 |
| Mesenchymal 6 2 | 29 | 0.78 (0.51) | 12 | 0.54 (0.38) | 0.148 |
| Tissue | |||||
| Epithelial 5 1 | 25 | 0.56 (0.20–1.14) | 11 | 0.83 (0.44–2.85) | 0.359 |
| Epithelial 6 1 | 20 | 0.63 (0.36–1.57) | 11 | 1.46 (0.35–2.08) | 0.427 |
| Mesenchymal 1 1 | 28 | 0.96 (0.17–58.42) | 13 | 1.22 (0.23–3.34) | 0.628 |
| Mesenchymal 2 1 | 16 | 0.66 (0.54–2.66) | 10 | 1.24 (0.24–2.66) | 0.897 |
| Mesenchymal 4 1 | 18 | 0.91 (0.35–8.38) | 11 | 0.45 (0.23–3.66) | 0.550 |
| Mesenchymal 5 1 | 19 | 0.56 (0.05–6.66) | 10 | 2.17 (0.12–6.54) | 0.573 |
| Markers | BC without CT | BC with CT | BBD | |||
|---|---|---|---|---|---|---|
| n | Median (p25-p75)/Mean(±SD) | n | Median (p25-p75)/Mean(±SD) | n | Median (p25-p75)/Mean(±SD) | |
| Bloodstream | ||||||
| Epithelial 1 1 | 15 | 0.57 (0.23–1.02) | 21 | 0.33 (0.12–0.84) | 15 | 0.60 (0.44–1.77) |
| Epithelial 2 1 | 15 | 1.05 (0.46–1.97) a | 21 | 0.59 (0.13–0.65) b | 15 | 0.96 (0.24–1.84) a |
| Epithelial 3 1 | 15 | 1.63 (0.61–2.30) | 21 | 0.83 (0.45–2.10) | 16 | 0.74 (0.59–1.56) |
| Epithelial 4 1 | 15 | 2.21 (0.95–2.77) a | 20 | 1.59 (0.65–3.67) a,b | 15 | 0.82 (0.38–1.82) b |
| Epithelial 5 1 | 13 | 1.78 (0.68–4.91) | 16 | 1.64 (0.97–2.18) | 12 | 1.04 (0.78–2.25) |
| Epithelial 6 1 | 12 | 1.80 (0.80–2.76) | 16 | 0.89 (0.15–5.20) | 13 | 1.31 (0.43–5.14) |
| Mesenchymal 1 2 | 10 | 0.94 (1.20) | 7 | 0.70 (0.46) | 8 | 1.09 (1.07) |
| Mesenchymal 2 1 | 13 | 2.65 (1.79–6.09) a | 11 | 1.27 (0.53–2.05) b | 9 | 0.92 (0.45–1.99) b |
| Mesenchymal 3 1 | 13 | 1.79 (0.87–5.54) | 15 | 1.61 (0.58–2.41) | 12 | 1.08 (0.73–2.45) |
| Mesenchymal 4 1 | 12 | 2.16 (0.88–5.72) a | 15 | 1.24 (0.64–2.58) a,b | 12 | 0.74 (0.38–2.47) b |
| Mesenchymal 5 1 | 13 | 0.83 (0.53–1.25) | 16 | 0.70 (0.37–1.17) | 13 | 0.64 (0.18–1.06) |
| Mesenchymal 6 2 | 13 | 1.04 (0.49) a | 16 | 0.58 (0.44) a,b | 12 | 0.54 (0.38) b |
| Tissue | a | |||||
| Epithelial 5 1 | 20 | 0.48 (0.20–0.88) | 5 | 0.78 (0.20–23.4) | 11 | 0.83 (0.44–2.85) |
| Epithelial 6 1 | 15 | 0.64 (0.34–1.66) | 5 | 0.50 (0.32–4.6) | 11 | 1.46 (0.35–2.08) |
| Mesenchymal 1 1 | 21 | 0.59 (0.15–66.85) | 7 | 9.33 (0.15–62.03) | 13 | 1.22 (0.23–3.34) |
| Mesenchymal 2 1 | 12 | 0.66 (0.53–4.90) | 4 | 1.55 (0.56–2.66) | 10 | 1.24 (0.24–2.66) |
| Mesenchymal 4 1 | 15 | 2.75 (0.36–10.09) | 3 | 0.45 (0.014–NA) | 11 | 0.45 (0.23–3.66) |
| Mesenchymal 5 1 | 19 | 0.74 (0.05–7.69) | 4 | 0.38 (0.06–0.92) | 10 | 2.17 (0.12–6.54) |
| Markers | n | 0 Median (p25-p75) Mean (±SD) | n | IA Median (p25-p75) Mean (±SD) | n | IIA Median (p25-p75) Mean (±SD) | n | IIB Median (p25-p75) Mean (±SD) | n | IIIA Median (p25-p75) Mean (±SD) | p Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bloodstream | |||||||||||
| Epithelial 1 1 | 6 | 0.86 (0.28–5.47) | 5 | 0.33 (0.15–0.71) | 7 | 0.77 (0.04–2.28) | 6 | 0.42 (0.14–0.76) | 4 | 0.63 (0.16–1.46) | 0.77 |
| Epithelial 2 1 | 6 | 1.28 (0.44–4.39) | 5 | 0.90 (0.15–1.74) | 7 | 0.59 (0.01–2.06) | 6 | 0.82 (0.14–2.74) | 4 | 1.08 (0.66–1.45) | 0.66 |
| Epithelial 3 1 | 6 | 1.61 (0.59–4.39) | 5 | 1.88 (0.24–3.29) | 7 | 0.51 (0.03–3.14) | 6 | 1.24 (0.44–3.16) | 4 | 1.86 (1.02–2.20) | 0.56 |
| Epithelial 4 1 | 6 | 1.51 (0.58–7.56) | 5 | 2.21 (0.38–4.37) | 7 | 1.28 (0.06–2.39) | 6 | 1.65 (0.97–4.57) | 4 | 3.26 (1.98–7.76) | 0.42 |
| Epithelial 5 1 | 5 | 1.28 (0.33–2.36) | 2 | 1.24 (0.70–NA) | 7 | 1.96 (0.03–3.50) | 5 | 4.29 (1.28–7.09) | 3 | 1.02 (0.10–NA) | 0.44 |
| Epithelial 6 1 | 4 | 0.46 (0.05–1.40) | 2 | 1.01 (0.02–NA) | 7 | 0.50 (0.00–8.90) | 5 | 1.67 (1.09–4.84) | 3 | 2.86 (1.01–NA) | 0.37 |
| Mesenchymal 1 2 | 4 | 1.14 (1.77) | 1 | 0.69 (NA) | 4 | 0.53 (0.42) | 3 | 0.63 (0.50) | 2 | 1.88 (0.47) | 0.66 |
| Mesenchymal 2 1 | 4 | 2.01 (1.14–2.62) | 2 | 1.11 (0.11–NA) | 5 | 1.27 (0.04–2.57) | 5 | 3.31 (1.39–10.20) | 3 | 5.84 (0.53–NA) | 0.27 |
| Mesenchymal 3 1 | 5 | 5.41 (0.26–11.59) | 2 | 0.45 (0.20–NA) | 7 | 1.05 (0.03–3.98) | 4 | 2.91 (1.68–5.25) | 3 | 1.39 (0.75–NA) | 0.32 |
| Mesenchymal 4 1 | 4 | 1.16 (0.19–3.68) | 2 | 5.82 (3.66–NA) | 7 | 4.53 (0.81–6.18) | 5 | 0.64 (0.43–1.69) | 3 | 1.75 (0.58–NA) | 0.11 |
| Mesenchymal 5 1 | 6 | 0.93 (0.69–3.23) | 2 | 0.66 (0.55–NA) | 8 | 1.05 (0.44–46.14) | 5 | 0.49 (0.21–1.02) | 3 | 1.43 (0.25–NA) | 0.38 |
| Mesenchymal 6 2 | 6 | 1.32(0.63) a | 2 | 0.81 (0.03) | 7 | 0.47 (0.30) b | 5 | 0.55 (0.19) b | 3 | 1.24 (0.40) | 0.01 |
| Tissue | |||||||||||
| Epithelial 5 1 | 4 | 0.53 (0.12–0.76) | 4 | 0.28 (0.06–0.74) | 6 | 4.92 (0.16–45.41) | 5 | 0.64 (0.11–4.77) | 3 | 1.39 (0.35–NA) | 0.35 |
| Epithelial 6 1 | 4 | 0.48 (0.10–0.79) | 3 | 0.86 (0.18–NA) | 6 | 4.62 (0.03–8.40) | 2 | 0.26 (0.01–NA) | 2 | 1.06 (0.47–NA) | 0.27 |
| Mesenchymal 1 2 | 4 | 21.92 (42.41) | 6 | 76.65 (158.67) | 8 | 100.16 (163.64) | 4 | 45.30 (56.67) | 3 | 45.63 (71.66) | 0.84 |
| Mesenchymal 2 1 | 3 | 0.65 (0.65–NA) | 3 | 0.86 (0.18–NA) | 4 | 1.69 (0.52–10.34) | 1 | 9.10 (NA) | 2 | 1.31 (0.17–NA) | 0.64 |
| Mesenchymal 4 1 | 3 | 0.93 (0.63–NA) | 3 | 0.09 (0.01–NA) | 4 | 13.41(0.46–45.95) | 2 | 5.49 (0.89–NA) | 3 | 0.45 (0.36–NA) | 0.32 |
| Mesenchymal 5 1 | 3 | 6.65 (0.20–NA) | 4 | 0.02 (0.02–1.25) | 5 | 0.56(0.11–30.85) | 3 | 16.75 (0.74–NA) | 2 | 0.59 (0.15–NA) | 0.17 |
| Markers | n | 1 Median (p25-p75) Mean (±SD) | n | 2 Median (p25-p75) Mean (±SD) | n | 3 Median (p25-p75) Mean (±SD) | p Value |
|---|---|---|---|---|---|---|---|
| Bloodstream | |||||||
| Epithelial 1 1 | 3 | 0.23 (0.17–NA) | 16 | 0.51 (0.14–0.87) | 7 | 0.33 (0.05–1.03) | 0.848 |
| Epithelial 2 1 | 3 | 0.59 (0.17–NA) | 16 | 0.60 (0.17–1.86) | 7 | 0.60 (0.25–1.49) | 0.823 |
| Epithelial 3 1 | 3 | 1.41 (0.45–NA) | 16 | 0.73 (0.45–2.27) | 7 | 1.90 (0.52–2.71) | 0.633 |
| Epithelial 4 1 | 3 | 2.02 (1.01–NA) | 16 | 1.63 (0.72–4.15) | 7 | 2.76 (0.84–3.75) | 0.745 |
| Epithelial 5 1 | 3 | 4.29 (0.10–NA) | 14 | 1.99 (1.56–4.00) | 5 | 0.95 (0.02–3.28) | 0.226 |
| Epithelial 6 1 | 3 | 2.46 (0.01–NA) | 14 | 1.82 (0.36–5.86) | 5 | 1.15 (0.0 5–3.10) | 0.645 |
| Mesenchymal 1 2 | 2 | 0.35 (0.17) | 6 | 0.52 (0.42) | 4 | 1.18 (0.86) | 0.200 |
| Mesenchymal 2 1 | 3 | 7.86 (5.84–NA) | 10 | 1.80 (0.15–2.76) | 4 | 1.95 (0.72–5.41) | 0.091 |
| Mesenchymal 3 1 | 2 | 3.53 (1.39–NA) | 14 | 1.78 (0.62–2.21) | 5 | 1.61 (0.40–3.52) | 0.632 |
| Mesenchymal 4 1 | 3 | 1.16 (0.60–NA) | 13 | 2.57 (1.63–5.19) | 5 | 0.64 (0.31–4.83) | 0.117 |
| Mesenchymal 5 1 | 3 | 1.04 (0.49–NA) | 15 | 0.65 (0.35–1.03) | 5 | 1.03 (0.21–24.07) | 0.668 |
| Mesenchymal 6 2 | 3 | 0.67 (0.21) ª,b | 15 | 0.56 (0.33) a | 4 | 1.12 (0.49) b | 0.032 |
| Tissue | |||||||
| Epithelial 5 1 | 6 | 0.50 (0.15–33.60) | 11 | 0.82 (0.21–1.39) | 6 | 0.39 (0.29–6.21) | 0.886 |
| Epithelial 6 1 | 4 | 0.68 (0.13–6.51) | 8 | 0.66 (0.25–2.24) | 6 | 0.54 (0.41–3.01) | 0.993 |
| Mesenchymal 1 2 | 6 | 35.88 (48.86) | 12 | 51.38 (95.64) | 8 | 104.45 (181.85) | 0.602 |
| Mesenchymal 2 1 | 3 | 2.73 (0.94–NA) | 6 | 1.20 (0.53–4.43) | 5 | 0.56 (0.10–0.68) | 0.067 |
| Mesenchymal 4 1 | 3 | 10.09 (0.09–NA) | 7 | 0.89 (0.45–4.34) | 6 | 2.67 (0.26–17.34) | 0.833 |
| Mesenchymal 5 1 | 4 | 0.65 (0.15–21.03) | 8 | 0.69 (0.04–2.19) | 5 | 0.15 (0.04–18.75) | 0.928 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, A.T.F.; Rodrigues, C.M.; Ferreira, I.C.C.; Santos, L.L.D.; Santos, D.W.; Araújo, T.G.; Canto, P.P.L.; Paiva, C.E.; Goulart, L.R.; Maia, Y.C.P. A Novel Detection Method of Breast Cancer through a Simple Panel of Biomarkers. Int. J. Mol. Sci. 2022, 23, 11983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911983
Silva ATF, Rodrigues CM, Ferreira ICC, Santos LLD, Santos DW, Araújo TG, Canto PPL, Paiva CE, Goulart LR, Maia YCP. A Novel Detection Method of Breast Cancer through a Simple Panel of Biomarkers. International Journal of Molecular Sciences. 2022; 23(19):11983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911983
Chicago/Turabian StyleSilva, Alinne T. F., Cláudia M. Rodrigues, Izabella C. C. Ferreira, Letícia L. D. Santos, Donizeti W. Santos, Thaise G. Araújo, Paula P. L. Canto, Carlos E. Paiva, Luiz R. Goulart, and Yara C. P. Maia. 2022. "A Novel Detection Method of Breast Cancer through a Simple Panel of Biomarkers" International Journal of Molecular Sciences 23, no. 19: 11983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231911983