
Disorders of the Cholinergic System in COVID-19 Era—A Review of the Latest Research

 ,
,  and
and
Abstract
:1. Introduction
2. Literature Analysis
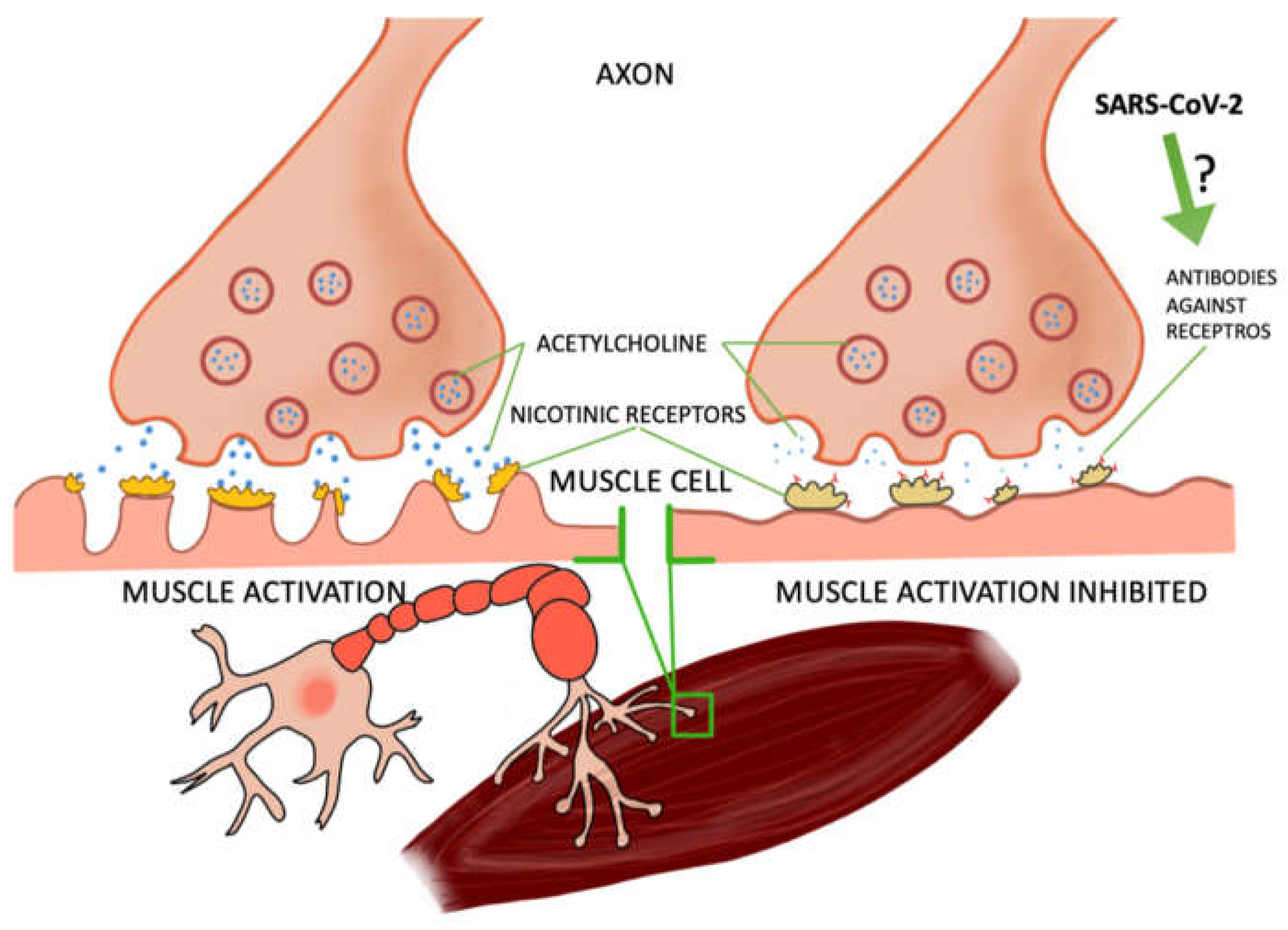
2.1. COVID-19 Can Cause Myasthenia Gravis
2.2. The Relationship between COVID-19 and Acetylcholinesterase Activity
2.3. Interactions between Proteins
2.4. Vagus Nerve Stimulation—A Potential Therapy for COVID-19
3. Cytokine Storm and COVID-19
4. Pediatric Multisystem Inflammatory Syndrome, Kawa-COVID-19, and Hyperinflammatory Syndrome in COVID-19
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fudim, M.; Qadri, Y.J.; Ghadimi, K.; MacLeod, D.B.; Molinger, J.; Piccini, J.P.; Whittle, J.; Wischmeyer, P.E.; Patel, M.R.; Ulloa, L. Implications for neuromodulation therapy to control inflammation and related organ dysfunction in COVID-19. J. Cardiovasc. Transl. Res. 2020, 13, 894–899. [Google Scholar] [CrossRef]
- Kruk-Słomka, M.; Budzyńska, B.; Biała, G. Involvement of cholinergic receptors in the different stages of memory measured in the modified elevated plus maze test in mice. Pharmacol Rep 2012, 64, 1066–1080. [Google Scholar] [CrossRef]
- Bonaz, B.; Sinniger, V.; Pellissier, S. Targeting the cholinergic anti-inflammatory pathway with vagus nerve stimulation in patients with COVID-19. Bioelectron. Med. 2020, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Hübers, A.; Lascano, A.M.; Lalive, P.H. Management of patients with generalised myasthenia gravis and COVID-19: Four case reports. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1124–1125. [Google Scholar] [CrossRef] [PubMed]
- Meriggioli, M.N.; Sanders, D.B. Autoimmune myasthenia gravis: Emerging clinical and biological heterogeneity. Lancet Neurol. 2009, 8, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Karimi, N.; Okhovat, A.A.; Ziaadini, B.; Ashtiani, B.H.; Nafissi, S.; Fatehi, F. Myasthenia gravis associated with novel coronavirus 2019 infection: A report of three cases. Clin. Neurol. Neurosurg. 2021, 208, 106834. [Google Scholar] [CrossRef]
- Sriwastava, S.; Tandon, M.; Kataria, S.; Daimee, M.; Sultan, S. New onset of ocular myasthenia gravis in a patient with COVID-19: A novel case report and literature review. J. Neurol. 2021, 268, 2690–2696. [Google Scholar] [CrossRef] [PubMed]
- Essajee, F.; Lishman, J.; Solomons, R.; Abraham, D.R.; Goussard, P.; van Toorn, R. Transient acetylcholine receptor-related myasthenia gravis, post multisystem inflammatory syndrome in children (MIS-C) temporally associated with COVID-19 infection. BMJ Case Rep. 2021, 14, e244102. [Google Scholar] [CrossRef]
- Beydon, M.; Chevalier, K.; al Tabaa, O.; Hamroun, S.; Delettre, A.; Thomas, M.; Herrou, J.; Riviere, E.; Mariette, X. Myositis as a manifestation of SARS-CoV-2. Ann. Rheum. Dis. 2020, 80, e42. [Google Scholar] [CrossRef] [Green Version]
- Restivo, D.A.; Centonze, D.; Alesina, A.; Marchese-Ragona, R. Myasthenia gravis associated with SARS-CoV-2 infection. Ann. Int. Med. 2020, 173, 1027–1028. [Google Scholar] [CrossRef]
- Assini, A.; Gandoglia, I.; Damato, V.; Rikani, K.; Evoli, A.; del Sette, M. Myasthenia gravis associated with anti-MuSK antibodies developed after SARS-CoV-2 infection. Eur. J. Neurol. 2021, 28, 3537–3539. [Google Scholar] [CrossRef]
- Dunsire, M.F.; Clarke, S.G.; Stedmon, J.J. Undiagnosed myasthenia gravis unmasked by neuromuscular blockade. Br. J. Anaesth. 2001, 86, 727–730. [Google Scholar] [CrossRef] [Green Version]
- Webb, K.; Abraham, D.; Faleye, A.; McCulloch, M.; Rabie, H.; Scott, C. Cape town MISC-team, multisystem inflammatory syndrome in children in South Africa. Lancet Child Adolesc. Health 2020, 4, e38. [Google Scholar] [CrossRef]
- Courties, A.; Boussier, J.; Hadjadj, J.; Yatim, N.; Barnabei, L.; Péré, H.; Veyer, D.; Kernéis, S.; Carlier, N.; Pène, F.; et al. Regulation of the acetylcholine/α7nAChR anti-inflammatory pathway in COVID-19 patients. Sci. Rep. 2021, 11, 11886. [Google Scholar] [CrossRef]
- Tracey, K.J. Physiology and immunology of the cholinergic antiinflammatory pathway. J. Clin. Investig. 2007, 117, 289–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Rubio, J.; Navarro-Lopez, C.; Lopez-Najera, E.; Lopez-Najera, A.; Jimenez-Diaz, L.; Navarro-Lopez, J.D.; Najera, A. Cytokine release syndrome (CRS) and nicotine in COVID-19 patients: Trying to calm the storm. Front. Immunol. 2020, 11, 1359. [Google Scholar] [CrossRef] [PubMed]
- Ciaglia, E.; Vecchione, C.; Puca, A.A. COVID-19 infection and circulating ACE2 levels: Protective role in women and children. Front. Pediatrics 2020, 8, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadi, S.; Heidarizadeh, M.; Entesari, M.; Esmailpour, A.; Esmailpour, M.; Moradi, R.; Sakhaee, N.; Doustkhah, E. In silico investigation on the inhibiting role of nicotine/caffeine by blocking the S protein of SARS-CoV-2 versus ACE2 receptor. Microorganisms 2020, 8, 1600. [Google Scholar] [CrossRef]
- Oliveira, A.S.F.; Ibarra, A.A.; Bermudez, I.; Casalino, L.; Gaieb, Z.; Shoemark, D.K.; Gallagher, T.; Sessions, R.B.; Amaro, R.E.; Mulholland, A.J. A potential interaction between the SARS-CoV-2 spike protein and nicotinic acetylcholine receptors. Biophys. J. 2021, 120, 983–993. [Google Scholar] [CrossRef]
- Farsalinos, K.; Eliopoulos, E.; Leonidas, D.D.; Papadopoulos, G.E.; Tzartos, S.; Poulas, K. Nicotinic cholinergic system and COVID-19: In silico identification of an interaction between SARS-CoV-2 and nicotinic receptors with potential therapeutic targeting implications. Int. J. Mol. Sci. 2020, 21, 5807. [Google Scholar] [CrossRef]
- Lagoumintzis, G.; Chasapis, C.T.; Alexandris, N.; Kouretas, D.; Tzartos, S.; Eliopoulos, E. Konstantinos farsalinos, konstantinos poulas, nicotinic cholinergic system and COVID-19: In silico identification of interactions between α7 nicotinic acetylcholine receptor and the cryptic epitopes of SARS-Co-V and SARS-CoV-2 spike glycoproteins. Food Chem. Toxicol. 2021, 149, 112009. [Google Scholar] [CrossRef]
- Smith, M.; Smith, J.C. Repurposing therapeutics for COVID-19: Supercomputer-based docking to the SARS-CoV-2 viral spike protein and viral spike protein-human ACE2 interface. ChemRxiv 2020. [Google Scholar] [CrossRef]
- Farsalinosab, K.; Niaura, R.; le Houezec, J.; Barbouni, A.; Tsatsakis, A.; Kouretas, D.; Vantarakis, A.; Poulas, K. Editorial: Nicotine and SARS-CoV-2: COVID-19 may be a disease of the nicotinic cholinergic system. Toxicol. Rep. 2020, 7, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tizabi, Y.; Getachew, B.; Copeland, R.L.; Aschner, M. Nicotine and the nicotinic cholinergic system in COVID-19. FEBS J. 2020, 287, 3656–3663. [Google Scholar] [CrossRef]
- Changeux, J.P.; Amoura, Z.; Rey, F.A.; Miyara, M. A nicotinic hypothesis for COVID-19 with preventive and therapeutic implications. C. R. Biol. 2020, 1, 33–39. [Google Scholar]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. HLH across speciality collaboration, COVID-19: Consider cytokine storm syndromes and immunosuppression. UK Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Staats, P.; Giannakopoulos, G.; Blake, J.; Liebler, E.; Levy, R.M. The use of non-invasive vagus nerve stimulation to treat respiratory symptoms associated with COVID-19: A theoretical hypothesis and early clinical experience. Neuromodul. Technol. Neural Interface 2020, 23, 784–788. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef]
- Sims, J.T.; Krishnan, V.; Chang, C.-Y.; Engle, S.M.; Casalini, G.; Rodgers, G.H.; Bivi, N.; Nickoloff, B.J.; Konrad, R.J.; de Bono, S.; et al. Characterization of the cytokine storm reflects hyperinflammatory endothelial dysfunction in COVID-19. J. Allergy Clin. Immunol. 2020, 147, 107–111. [Google Scholar] [CrossRef]
- Elkahloun, A.G.; Saavedra, J.M. Candesartan could ameliorate the COVID-19 cytokine storm. Biomed. Pharmacother. 2020, 131, 110653. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xiang, L.; Lin, F.; Cai, Z.; Ruan, H.; Wang, J.; Liang, J.; Wang, F.; Lu, M.; Cui, W. 456 inhaled ACE2-engineered microfluidic microsphere for intatacheal neutralization of COVID-19 and calming of the cytokine 457 storm. Matter 2021. [Google Scholar] [CrossRef]
- Rossi, M.; Piagnerelli, M.; van Meerhaeghe, A.; Bodjeltia, K.Z. Heme oxygenase-1 (HO-1) cytoprotective pathway: A potential treatment strategy against coronavirus disease 2019 (COVID-19)-induced cytokine storm syndrome. Med. Hypotheses 2020, 144, 110242. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, C.; Bucci, I.; Napolitano, G. Phenylomethimazole is a candidate drug for treatment of serve forms of coronavirus disease 2019 (COVID-19) as well as other virus-induced “cytokine storm”. Med. Hypotheses 2021, 146, 110473. [Google Scholar] [CrossRef] [PubMed]
- Wang, R. Etoricoxib may inhibit cytokine storm to treat COVID-19. Med. Hypotheses 2021, 150, 110557. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Zhu, Y.; Zhang, J.; Li, Y.; Peng, Z. Intravenous high-dose vitamin C for the treatment of serve COVID-19: Study protocol for a multicentre randomized controlled trial. BMJ Open 2020, 8, 10. [Google Scholar]
- Ebina-Shibuya, R.; Namkoong, H.; Shibuya, Y.; Horita, N. Multisystem inflammatory syndrome in children (MIS-C) with COVID-19: Insights from simultaneous familial Kawasaki Disease cases. Int. J. Infect. Dis. 2020, 97, 371–373. [Google Scholar] [CrossRef]
- Pouletty, M.; Borocco, C.; Ouldali, N.; Caseris, M.; Basmaci, R.; Lachaume, N.; Bensaid, P.; Pichard, S.; Kouider, H.; Morelle, G.; et al. Pediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): A multicentre cohort. Ann. Rheum. Dis. 2020, 79, 999–1006. [Google Scholar] [CrossRef]
- Simpson, J.M.; Newburger, J.W. Multisystem inflammatory syndrome in children in association with COVID-19. Circulation 2020, 142, 437–440. [Google Scholar] [CrossRef]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American college of rheumatology clinical guidance for multisystem inflammatory syndrome in childern associated with SARS-CoV-2 and hyperinflammatrion in pediatric COVID-19. Arthritis Rheumatol. 2021, 73, e13–e29. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Typical Symptoms for KD | Number of Patients | Less Common Symptoms | Number of Patients | Less Common Neurological Symptoms | Number of Patients |
|---|---|---|---|---|---|
| Fever over 39 °C | 16 | Gastrointestinal symptoms | 13 | Headache | 6 |
| Fever over 40 °C | 7 | Hemodynamic failure | 11 | Aseptic meningitis | 3 |
| Mucocutaneous involvement | 15 | Inflammation of the testicles | 2 | Respiratory symptoms | 2 |
| Skin rash | 13 | - | - | Raynaud Syndrome | 2 |
| Rash/swelling of the feet and hands | 11 | - | - | Retained | 1 |
| Conjunctivitis | 15 | - | - | - | - |
| Dry and chapped lips | 14 | - | - | - | - |
| Cervical lymphadenopathy | 6 | - | - | - | - |
| Arthritis | 1 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopańska, M.; Batoryna, M.; Bartman, P.; Szczygielski, J.; Banaś-Ząbczyk, A. Disorders of the Cholinergic System in COVID-19 Era—A Review of the Latest Research. Int. J. Mol. Sci. 2022, 23, 672. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23020672
Kopańska M, Batoryna M, Bartman P, Szczygielski J, Banaś-Ząbczyk A. Disorders of the Cholinergic System in COVID-19 Era—A Review of the Latest Research. International Journal of Molecular Sciences. 2022; 23(2):672. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23020672
Chicago/Turabian StyleKopańska, Marta, Marta Batoryna, Paulina Bartman, Jacek Szczygielski, and Agnieszka Banaś-Ząbczyk. 2022. "Disorders of the Cholinergic System in COVID-19 Era—A Review of the Latest Research" International Journal of Molecular Sciences 23, no. 2: 672. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23020672