

Potential Urine Proteomic Biomarkers for Focal Segmental Glomerulosclerosis and Minimal Change Disease
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Optimization of the Urine Preparation Protocol for Proteomic Analysis
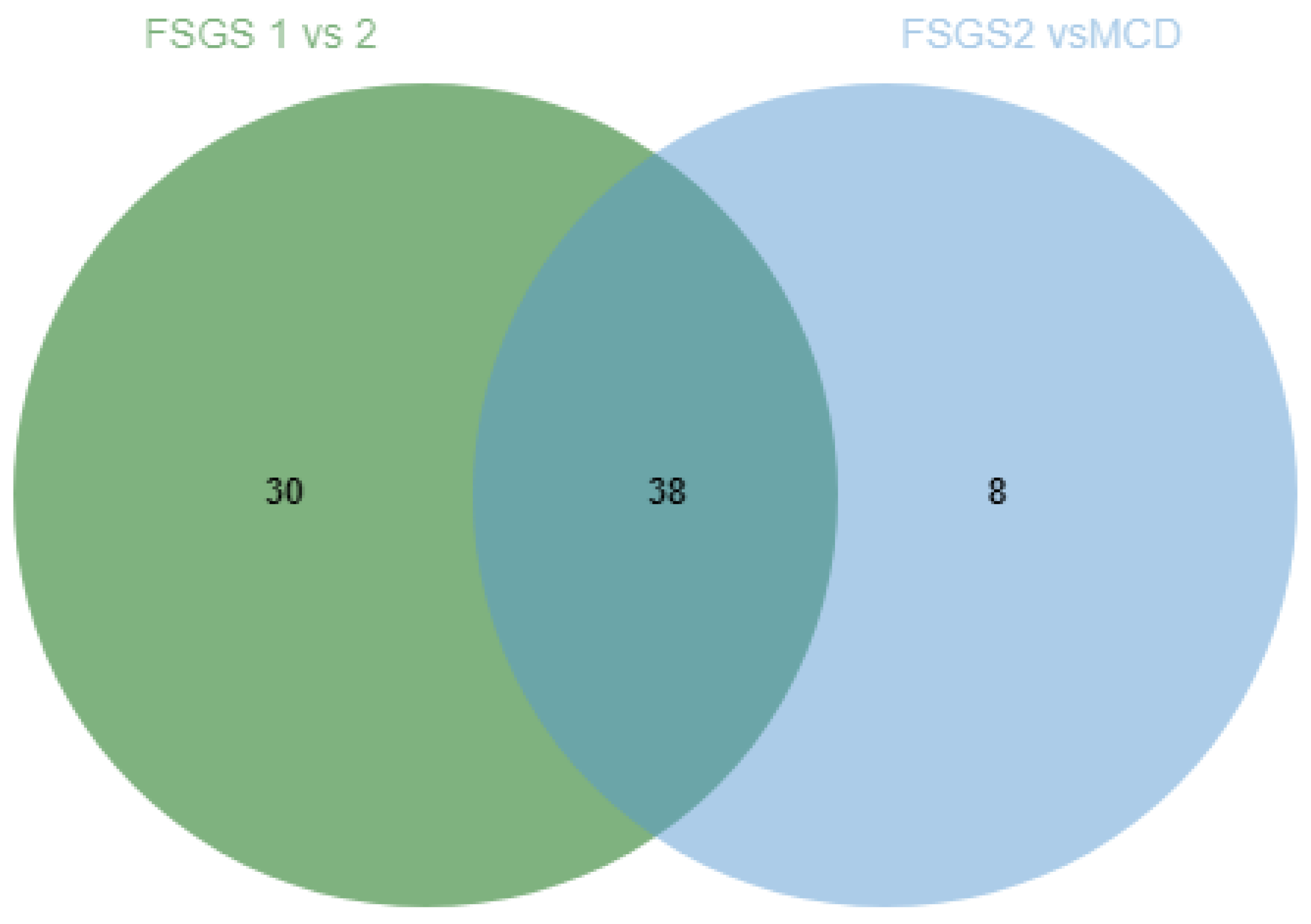
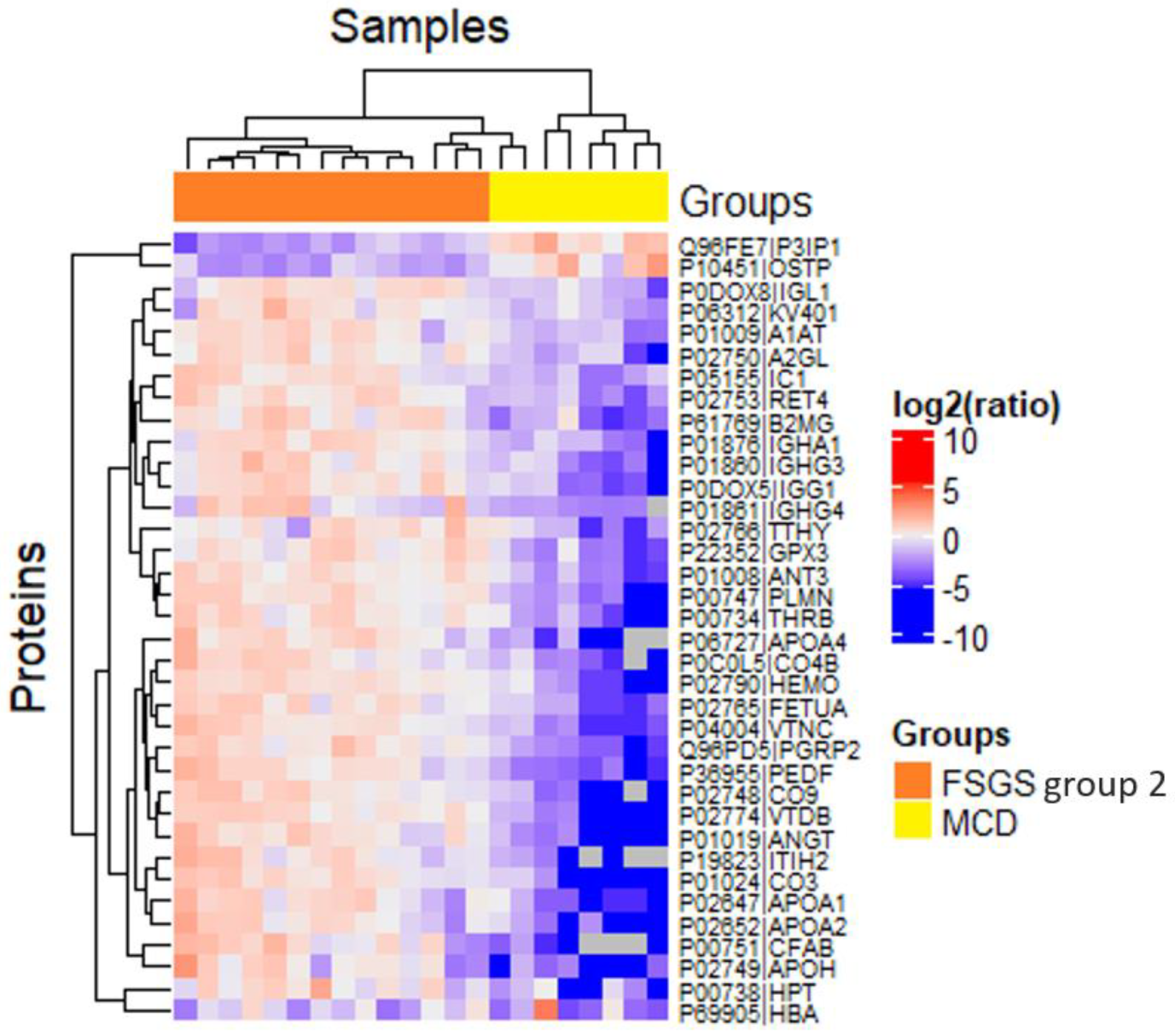
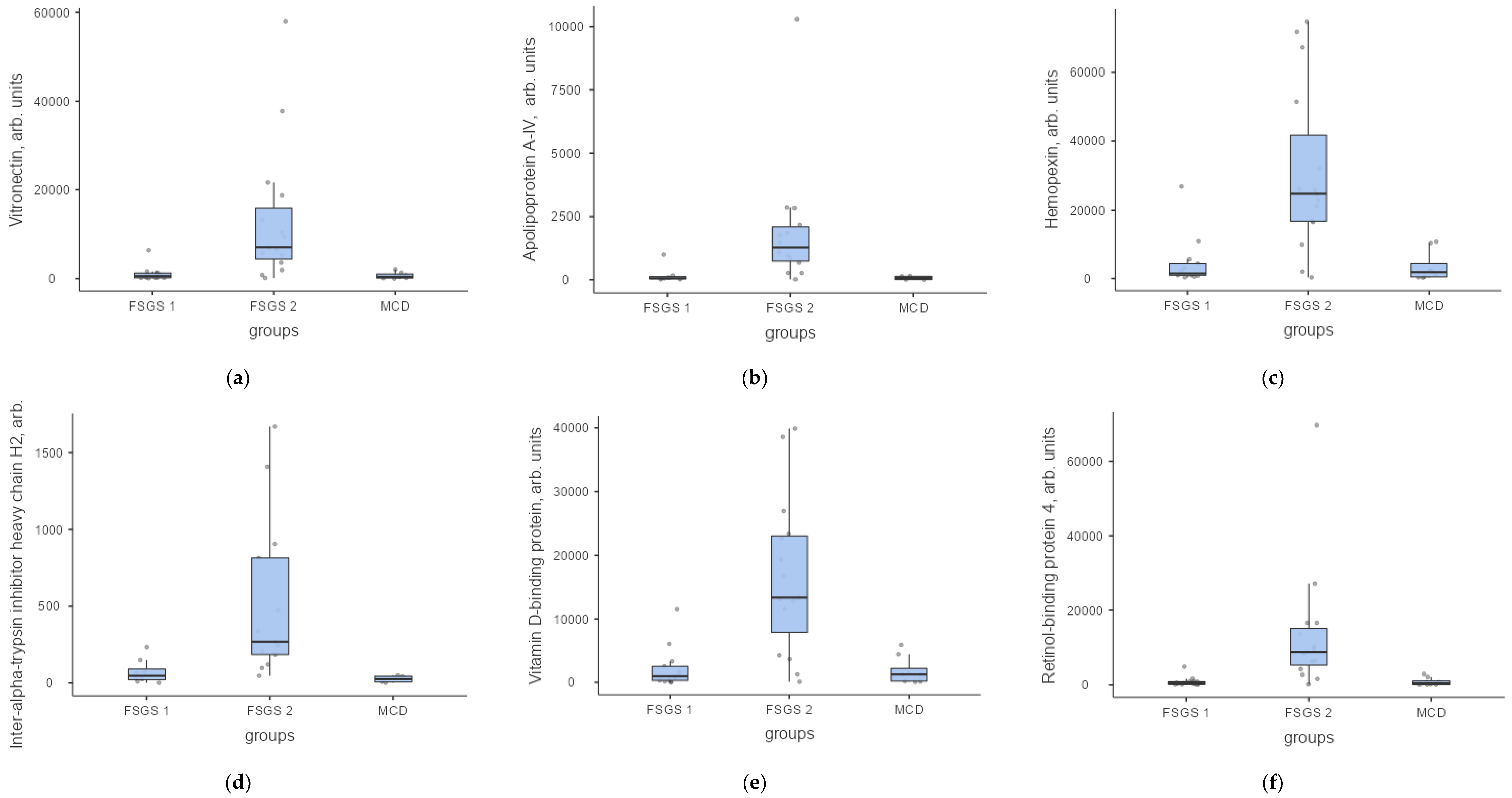
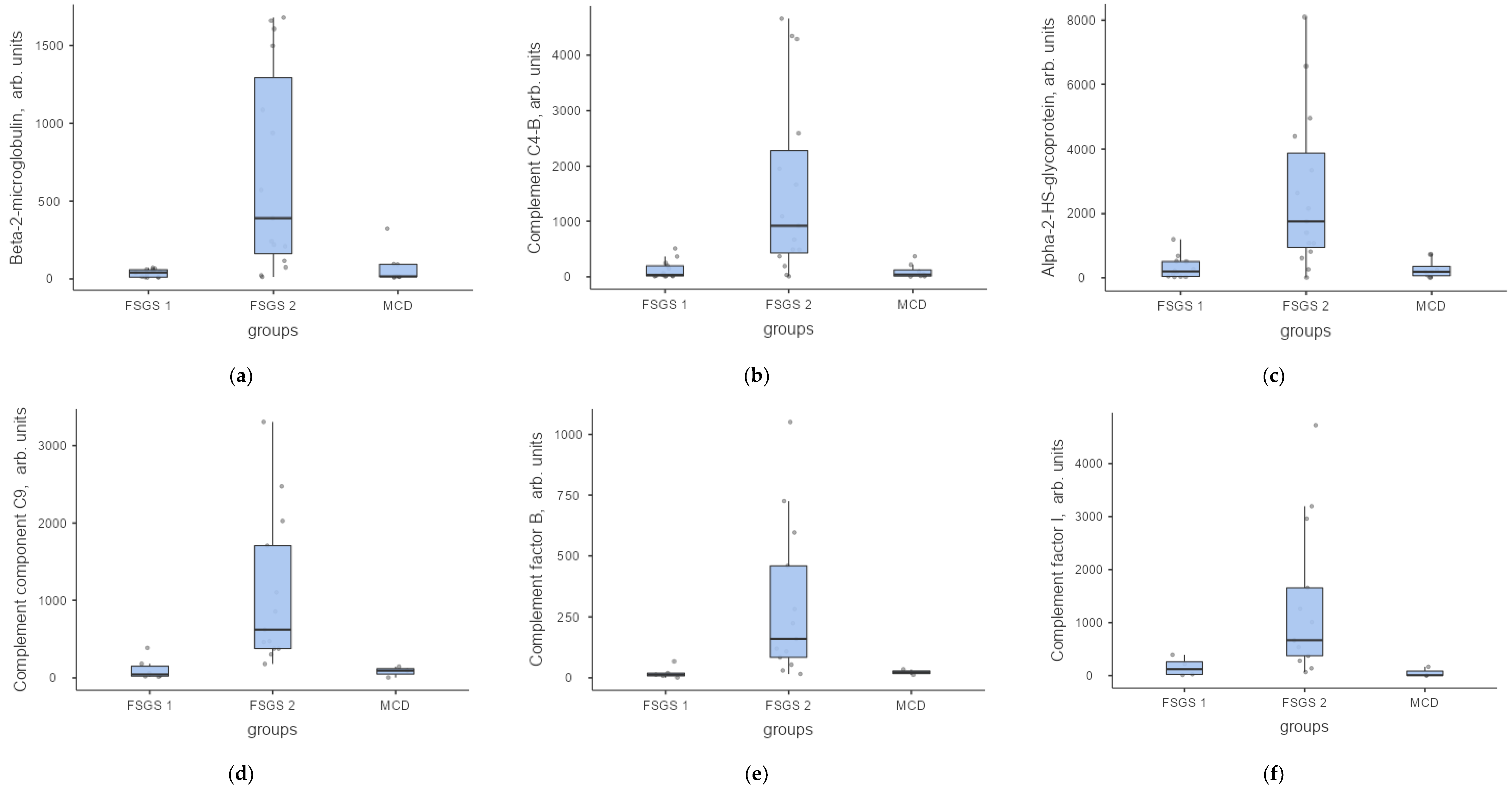
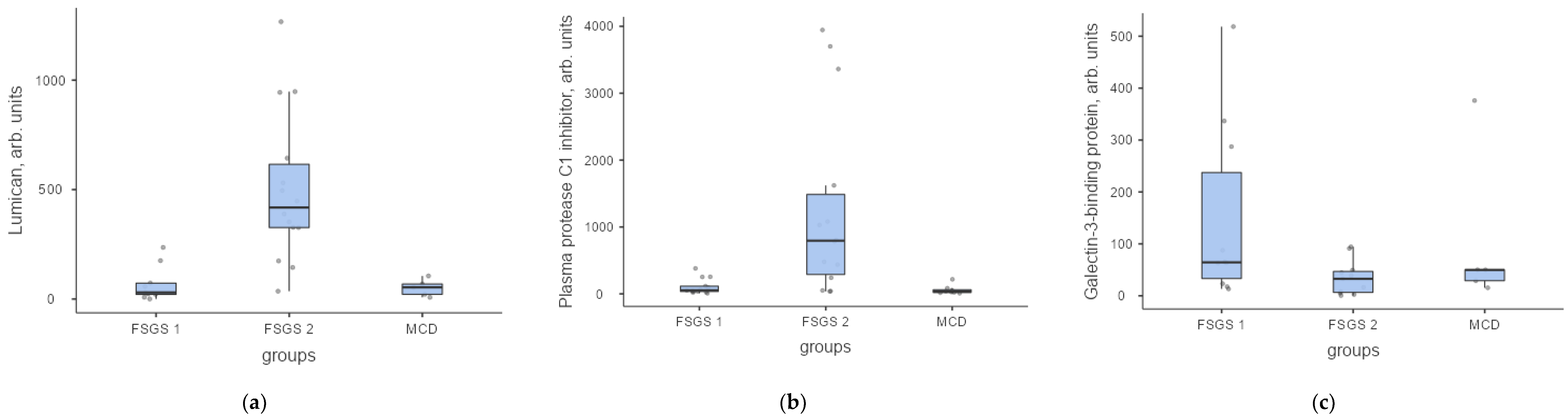
2.2. Label Free Analysis of the Urine Proteome for Patients with FSGS and MCD
3. Discussion
4. Materials and Methods
4.1. Clinical Characteristics of the Patients
4.2. Urine Sample Preparation for LC-MS/MS
4.3. Label-Free Untargeted LC-MS/MS Urine Proteomic Analysis
4.4. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| A1AT | Alpha-1 antitrypsin |
| ApoA-1 | Apolipoprotein A-1 |
| CD2AP | CD2 Associated Protein |
| CFP | Complement factor P (properdin) |
| CKD-EPI | Chronic Kidney Disease Epidemiology Collaboration formula |
| ECM | Extracellular matrix |
| ESI | Electrospray ionization |
| eGFR | Estimated glomerular filtration rate |
| FASP | Filter-aided sample preparation |
| FSGS | Focal segmental glomerulosclerosis |
| GBM | Glomerular basement membrane |
| HDL | High-density lipoprotein |
| HPLC | High-performance liquid chromatography |
| LC-MS | Liquid chromatography—mass spectrometry |
| LC-MS/MS | Liquid chromatography with tandem mass spectrometry |
| LC/MRM-MS | Liquid chromatography/Multiple reaction monitoring—mass spectrometry |
| LDL | Low density lipoproteins |
| MALDI-TOF MS | Matrix-Assisted Laser Desorption—Ionisation-Time of Flight Mass Spectrometry |
| MCD | Minimal change disease |
| MRM | Multiple reaction monitoring |
| MS | Mass spectrometry |
| NAT | Natural synthetic proteotypic peptides |
| NS | Nephrotic syndrome |
| PASEF | Parallel Accumulation—Serial Fragmentation method |
| PEDF | Pigment epithelium-derived factor |
| SIS | Stable isotope labelled peptide standards |
| TIF | Tubulointerstitial fibrosis |
References
- Praga, M.; Morales, E.; Herrero, J.C.; Campos, A.P.; Domínguez-Gil, B.; Alegre, R.; Vara, J.; Martínez, M.A. Absence of hypoalbuminemia despite massive proteinuria in focal segmental glomerulosclerosis secondary to hyperfiltration. Am. J. Kidney Dis. 1999, 33, 52–58. [Google Scholar] [CrossRef]
- Rydel, J.J.; Korbet, S.M.; Borok, R.Z.; Schwartz, M.M. Focal segmental glomerular sclerosis in adults: Presentation, course, and response to treatment. Am. J. Kidney Dis. 1995, 25, 534–542. [Google Scholar] [CrossRef]
- Vivarelli, M.; Massella, L.; Ruggiero, B.; Emma, F. Minimal Change Disease. Clin. J. Am. Soc. Nephrol. 2016, 12, 332–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, M.J.; Korbet, S.M.; Schwartz, M.M.; Lewis, E.J. Focal Segmental Glomerulosclerosis in Nephrotic Adults: Presentation, Prognosis, and Response to Therapy of the Histologic Variants. J. Am. Soc. Nephrol. 2004, 15, 2169–2177. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, M.; Katafuchi, R.; Yanase, T.; Ikeda, K.; Tanaka, H.; Fujimi, S. Steroid responsiveness and frequency of relapse in adult-onset minimal change nephrotic syndrome. Am. J. Kidney Dis. 2002, 39, 503–512. [Google Scholar] [CrossRef]
- Korbet, S.M.; Schwartz, M.M.; Lewis, E.J. Primary Focal Segmental Glomerulosclerosis: Clinical Course and Response to Therapy. Am. J. Kidney Dis. 1994, 23, 773–783. [Google Scholar] [CrossRef]
- Wehrmann, M.; Bohle, A.; Held, H.; Schumm, G.; Kendziorra, H.; Pressler, H. Long-term prognosis of focal sclerosing glomerulonephritis. An analysis of 250 cases with particular regard to tubulointerstitial changes. Clin. Nephrol. 1990, 33, 115–122. [Google Scholar]
- Sethi, S.; Zand, L.; Nasr, S.H.; Glassock, R.J.; Fervenza, F.C. Focal and segmental glomerulosclerosis: Clinical and kidney biopsy correlations. Clin. Kidney J. 2014, 7, 531–537. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, R.; Ma, D.; Li, L. Mass spectrometry-based proteomics and peptidomics for systems biology and biomarker discovery. Front. Biol. 2012, 7, 313–335. [Google Scholar] [CrossRef]
- Di Meo, A.; Pasic, M.D.; Yousef, G.M. Proteomics and peptidomics: Moving toward precision medicine in urological malignancies. Oncotarget 2016, 7, 52460–52474. [Google Scholar] [CrossRef] [Green Version]
- Feist, P.; Hummon, A.B. Proteomic Challenges: Sample Preparation Techniques for Microgram-Quantity Protein Analysis from Biological Samples. Int. J. Mol. Sci. 2015, 16, 3537–3563. [Google Scholar] [CrossRef]
- Filip, S.; Pontillo, C.; Schanstra, J.P.; Vlahou, A.; Mischak, H.; Klein, J. Urinary proteomics and molecular determinants of chronic kidney disease: Possible link to proteases. Expert Rev. Proteom. 2014, 11, 535–548. [Google Scholar] [CrossRef]
- Mischak, H.; Delles, C.; Vlahou, A.; Vanholder, R. Proteomic biomarkers in kidney disease: Issues in development and implementation. Nat. Rev. Nephrol. 2015, 11, 221–232. [Google Scholar] [CrossRef]
- Decramer, S.; de Peredo, A.G.; Breuil, B.; Mischak, H.; Monsarrat, B.; Bascands, J.-L.; Schanstra, J.P. Urine in Clinical Proteomics. Mol. Cell. Proteom. 2008, 7, 1850–1862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, H.; Fazelinia, H.; Spruce, L.A.; Weiss, D.A.; Zderic, S.A.; Seeholzer, S.H. Urine Proteomics: Evaluation of Different Sample Preparation Workflows for Quantitative, Reproducible, and Improved Depth of Analysis. J. Proteome Res. 2020, 19, 1857–1862. [Google Scholar] [CrossRef] [PubMed]
- Wiśniewski, J. Filter-Aided Sample Preparation: The Versatile and Efficient Method for Proteomic Analysis. Methods Enzym. 2017, 585, 15–27. [Google Scholar] [CrossRef]
- Percy, A.J.; Yang, J.; Hardie, D.B.; Chambers, A.G.; Tamura-Wells, J.; Borchers, C.H. Precise quantitation of 136 urinary proteins by LC/MRM-MS using stable isotope labeled peptides as internal standards for biomarker discovery and/or verification studies. Methods 2015, 81, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.R.; Pordal, A.; Haffner, C.; Pleasant, L.; Ma, Q.; Devarajan, P. Urinary Vitamin D-Binding Protein as a Biomarker of Steroid-Resistant Nephrotic Syndrome. Biomark. Insights 2016, 11, 1–6. [Google Scholar] [CrossRef]
- Mirković, K.; Doorenbos, C.R.C.; Dam, W.A.; Heerspink, H.J.L.; Slagman, M.C.J.; Nauta, F.L.; Kramer, A.B.; Gansevoort, R.T.; Born, J.V.D.; Navis, G.; et al. Urinary Vitamin D Binding Protein: A Potential Novel Marker of Renal Interstitial Inflammation and Fibrosis. PLoS ONE 2013, 8, e55887. [Google Scholar] [CrossRef] [Green Version]
- Choudhary, A.; Mohanraj, P.S.; Krishnamurthy, S.; Rajappa, M. Association of Urinary Vitamin D Binding Protein and Neutrophil Gelatinase-Associated Lipocalin with Steroid Responsiveness in Idiopathic Nephrotic Syndrome of Childhood. Saudi J. Kidney Dis Transpl. 2020, 31, 946–956. [Google Scholar] [CrossRef]
- Kirsztajn, G.M.; Nishida, S.K.; Silva, M.S.; Ajzen, H.; Pereira, A.B. Urinary retinol-binding protein as a prognostic marker in the treatment of nephrotic syndrome. Nephron Exp. Nephrol. 2000, 86, 109–114. [Google Scholar] [CrossRef]
- Feng, S.; Gao, Y.; Yin, D.; Lv, L.; Wen, Y.; Li, Z.; Wang, B.; Wu, M.; Liu, B. Identification of Lumican and Fibromodulin as Hub Genes Associated with Accumulation of Extracellular Matrix in Diabetic Nephropathy. Kidney Blood Press Res. 2021, 46, 275–285. [Google Scholar] [CrossRef]
- Svenningsen, P.; Bistrup, C.; Friis, U.G.; Bertog, M.; Haerteis, S.; Krueger, B.; Stubbe, J.; Jensen, O.N.; Thiesson, H.C.; Uhrenholt, T.R.; et al. Plasmin in Nephrotic Urine Activates the Epithelial Sodium Channel. J. Am. Soc. Nephrol. 2008, 20, 299–310. [Google Scholar] [CrossRef] [Green Version]
- Lennon, R.; Singh, A.; Welsh, G.I.; Coward, R.J.; Satchell, S.; Ni, L.; Mathieson, P.W.; Bakker, W.W.; Saleem, M.A. Hemopexin Induces Nephrin-Dependent Reorganization of the Actin Cytoskeleton in Podocytes. J. Am. Soc. Nephrol. 2008, 19, 2140–2149. [Google Scholar] [CrossRef] [Green Version]
- Pukajło-Marczyk, A.; Zwolińska, D. Involvement of Hemopexin in the Pathogenesis of Proteinuria in Children with Idiopathic Nephrotic Syndrome. J. Clin. Med. 2021, 10, 3160. [Google Scholar] [CrossRef]
- Kapojos, J.J.; Poelstra, K.; Borghuis, T.; Banas, B.; Bakker, W.W. Regulation of Plasma Hemopexin Activity by Stimulated Endothelial or Mesangial Cells. Nephron Exp. Nephrol. 2004, 96, p1–p10. [Google Scholar] [CrossRef]
- Mambetsariev, N.; Mirzapoiazova, T.; Mambetsariev, B.; Sammani, S.; Lennon, F.E.; Garcia, J.G.; Singleton, P.A. Hyaluronic Acid Binding Protein 2 Is a Novel Regulator of Vascular Integrity. Arter. Thromb. Vasc. Biol. 2010, 30, 483–490. [Google Scholar] [CrossRef]
- Kaul, A.; Singampalli, K.L.; Parikh, U.M.; Yu, L.; Keswani, S.G.; Wang, X. Hyaluronan, a double-edged sword in kidney diseases. Pediatr. Nephrol. 2021, 37, 735–744. [Google Scholar] [CrossRef]
- Merchant, M.L.; Barati, M.T.; Caster, D.J.; Hata, J.L.; Hobeika, L.; Coventry, S.; Brier, M.E.; Wilkey, D.W.; Li, M.; Rood, I.M.; et al. Proteomic Analysis Identifies Distinct Glomerular Extracellular Matrix in Collapsing Focal Segmental Glomerulosclerosis. J. Am. Soc. Nephrol. 2020, 31, 1883–1904. [Google Scholar] [CrossRef]
- Thurman, J.M.; Wong, M.; Renner, B.; Frazer-Abel, A.; Giclas, P.C.; Joy, M.S.; Jalal, D.; Radeva, M.K.; Gassman, J.; Gipson, D.S.; et al. Complement Activation in Patients with Focal Segmental Glomerulosclerosis. PLoS ONE 2015, 10, e0136558. [Google Scholar] [CrossRef] [Green Version]
- Zoshima, T.; Hara, S.; Yamagishi, M.; Pastan, I.; Matsusaka, T.; Kawano, M.; Nagata, M. Possible role of complement factor H in podocytes in clearing glomerular subendothelial immune complex deposits. Sci. Rep. 2019, 9, 7857. [Google Scholar] [CrossRef]
- Puig-Gay, N.; Jacobs-Cacha, C.; Sellarès, J.; Guirado, L.; Roncero, F.G.; Jiménez, C.; Zárraga, S.; Paul, J.; Lauzurica, R.; Alonso, Á.; et al. Apolipoprotein A-Ib as a biomarker of focal segmental glomerulosclerosis recurrence after kidney transplantation: Diagnostic performance and assessment of its prognostic value—A multi-centre cohort study. Transpl. Int. 2018, 32, 313–322. [Google Scholar] [CrossRef]
- Kopp, J.B.; Winkler, C.A.; Zhao, X.; Radeva, M.K.; Gassman, J.J.; D’Agati, V.D.; Nast, C.C.; Wei, C.; Reiser, J.; Guay-Woodford, L.M.; et al. Clinical Features and Histology of Apolipoprotein L1-Associated Nephropathy in the FSGS Clinical Trial. J. Am. Soc. Nephrol. 2015, 26, 1443–1448. [Google Scholar] [CrossRef] [Green Version]
- Jacobs-Cachá, C.; Puig-Gay, N.; Helm, D.; Rettel, M.; Sellarès, J.; Meseguer, A.; Savitski, M.M.; Moreso, F.J.; Soler, M.J.; Seron, D.; et al. A misprocessed form of Apolipoprotein A-I is specifically associated with recurrent Focal Segmental Glomerulosclerosis. Sci. Rep. 2020, 10, 1159. [Google Scholar] [CrossRef] [Green Version]
- Bukosza, E.N.; Kornauth, C.; Hummel, K.; Schachner, H.; Huttary, N.; Krieger, S.; Nöbauer, K.; Oszwald, A.; Fazeli, E.R.; Kratochwill, K.; et al. ECM Characterization Reveals a Massive Activation of Acute Phase Response during FSGS. Int. J. Mol. Sci. 2020, 21, 2095. [Google Scholar] [CrossRef] [Green Version]
- Catanese, L.; Siwy, J.; Mavrogeorgis, E.; Amann, K.; Mischak, H.; Beige, J.; Rupprecht, H. A Novel Urinary Proteomics Classifier for Non-Invasive Evaluation of Interstitial Fibrosis and Tubular Atrophy in Chronic Kidney Disease. Proteomes 2021, 9, 32. [Google Scholar] [CrossRef]
- Fischer, D.-C.; Schaible, J.; Wigger, M.; Staude, H.; Drueckler, E.; Kundt, G.; Haffner, D. Reduced Serum Fetuin-A in Nephrotic Children: A Consequence of Proteinuria? Am. J. Nephrol. 2011, 34, 373–380. [Google Scholar] [CrossRef]
- Shen, J.; Zhu, Y.; Zhang, S.; Lyu, S.; Lyu, C.; Feng, Z.; Hoyle, D.L.; Wang, Z.Z.; Cheng, T. Vitronectin-activated αvβ3 and αvβ5 integrin signalling specifies haematopoietic fate in human pluripotent stem cells. Cell Prolif. 2021, 54, e13012. [Google Scholar] [CrossRef]
- Urosev, D.; Ma, Q.; Tan, A.L.C.; Robinson, R.C.; Burtnick, L.D. The Structure of Gelsolin Bound to ATP. J. Mol. Biol. 2006, 357, 765–772. [Google Scholar] [CrossRef]
- Prochniewicz, E.; Zhang, Q.; Janmey, P.A.; Thomas, D.D. Cooperativity in F-Actin: Binding of Gelsolin at the Barbed End Affects Structure and Dynamics of the Whole Filament. J. Mol. Biol. 1996, 260, 756–766. [Google Scholar] [CrossRef] [Green Version]
- Conti, M.; Moutereau, S.; Zater, M.; Lallali, K.; Durrbach, A.; Manivet, P.; Eschwège, P.; Loric, S. Urinary cystatin C as a specific marker of tubular dysfunction. Clin. Chem Lab. Med. 2006, 44, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, A.R.; Yerbury, J.J.; Berghofer, P.; Greguric, I.; Katsifis, A.; Dobson, C.M.; Wilson, M.R. Clusterin facilitates in vivo clearance of extracellular misfolded proteins. Cell. Mol. Life Sci. 2011, 68, 3919–3931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Cui, Z.; Gu, Q.-H.; Zhang, Y.-M.; Qu, Z.; Wang, X.; Wang, F.; Cheng, X.-Y.; Meng, L.-Q.; Liu, G.; et al. Complement activation profile of patients with primary focal segmental glomerulosclerosis. PLoS ONE 2020, 15, e0234934. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Shen, Y.; Lin, C.; Qin, L.; He, S.; Dai, M.; Okitsu, S.L.; DeMartino, J.A.; Guo, Q.; Shen, N. Urinary galectin-3 binding protein (G3BP) as a biomarker for disease activity and renal pathology characteristics in lupus nephritis. Arthritis Res. Ther. 2022, 24, 77. [Google Scholar] [CrossRef]
- Ostalska-Nowicka, D.; Nowicki, M.; Kondraciuk, B.; Partyka, M.; Samulak, D.; Witt, M. Expression of galectin-3 in nephrotic syndrome glomerulopaties in children. Folia Histochem. Cytobiol. 2009, 47, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Sidenius, N.; Andolfo, A.; Fesce, R.; Blasi, F. Urokinase regulates vitronectin binding by controlling urokinase receptor oligomerization. J. Biol. Chem. 2002, 277, 27982–27990. [Google Scholar] [CrossRef] [Green Version]
- Chavakis, T.; Kanse, S.N.; Yutzy, B.; Lijnen, H.R.; Preissner, K.T. Vitronectin Concentrates Proteolytic Activity on the Cell Surface and Extracellular Matrix by Trapping Soluble Urokinase Receptor-Urokinase Complexes. Blood 1998, 91, 2305–2312. [Google Scholar] [CrossRef] [Green Version]
- Nafar, M.; Kalantari, S.; Samavat, S.; Rezaei-Tavirani, M.; Rutishuser, D.; Zubarev, R.A. The Novel Diagnostic Biomarkers for Focal Segmental Glomerulosclerosis. Int. J. Nephrol. 2014, 2014, 574261. [Google Scholar] [CrossRef] [Green Version]
- Medyńska, A.; Chrzanowska, J.; Kościelska-Kasprzak, K.; Bartoszek, D.; Żabińska, M.; Zwolińska, D. Alpha-1 Acid Glycoprotein and Podocin mRNA as Novel Biomarkers for Early Glomerular Injury in Obese Children. J. Clin. Med. 2021, 10, 4129. [Google Scholar] [CrossRef]
- Gomo, Z.A.; Henderson, L.O.; Myrick, J.E. High-density lipoprotein apolipoproteins in urine: I. Characterization in normal subjects and in patients with proteinuria. Clin. Chem. 1988, 34, 1775–1780. [Google Scholar] [CrossRef]
- Kalantari, S.; Nafar, M.; Rutishauser, D.; Samavat, S.; Rezaei-Tavirani, M.; Yang, H.; Zubarev, R.A. Predictive urinary biomarkers for steroid-resistant and steroid-sensitive focal segmental glomerulosclerosis using high resolution mass spectrometry and multivariate statistical analysis. BMC Nephrol. 2014, 15, 141. [Google Scholar] [CrossRef]
- Zhao, M.; Li, M.; Li, X.; Shao, C.; Yin, J.; Gao, Y. Dynamic changes of urinary proteins in a focal segmental glomerulosclerosis rat model. Proteome Sci. 2014, 12, 42. [Google Scholar] [CrossRef] [Green Version]
- Pérez, V.; Ibernón, M.; López, D.; Pastor, M.C.; Navarro, M.; Navarro-Muñoz, M.; Bonet, J.; Romero, R. Urinary Peptide Profiling to Differentiate between Minimal Change Disease and Focal Segmental Glomerulosclerosis. PLoS ONE 2014, 9, e87731. [Google Scholar] [CrossRef] [Green Version]
- Pérez, V.; López, D.; Boixadera, E.; Ibernón, M.; Espinal, A.; Bonet, J.; Romero, R. Comparative differential proteomic analysis of minimal change disease and focal segmental glomerulosclerosis. BMC Nephrol. 2017, 18, 49. [Google Scholar] [CrossRef] [Green Version]
- Kuzyk, M.A.; Parker, C.E.; Domanski, D.; Borchers, C.H. Development of MRM-based assays for the absolute quantitation of plasma proteins. Methods Mol. Biol. 2013, 1023, 53–82. [Google Scholar] [CrossRef]
- Kononikhin, A.S.; Zakharova, N.V.; Semenov, S.D.; Bugrova, A.E.; Brzhozovskiy, A.G.; Indeykina, M.I.; Fedorova, Y.B.; Kolykhalov, I.V.; Strelnikova, P.A.; Ikonnikova, A.Y.; et al. Prognosis of Alzheimer’s Disease Using Quantitative Mass Spectrometry of Human Blood Plasma Proteins and Machine Learning. Int. J. Mol. Sci. 2022, 23, 7907. [Google Scholar] [CrossRef]
- R Studio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020; Available online: http://www.rstudio.com/ (accessed on 6 July 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 6 July 2022).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Score |
|---|---|
| eGFR CKD-EPI, mL/min/1.73 m2 | |
| >60 | 0 |
| 45–59 | 1 |
| 35–45 | 2 |
| <35 | 3 |
| Proteinuria, g/24 h | |
| >2 | 0 |
| 2–3 | 0.5 |
| 3–4 | 1 |
| 4–5 | 1.5 |
| 5–6 | 2 |
| 6–7 | 2.5 |
| >7 | 3 |
| Steroid resistance | |
| Absent | 0 |
| Present | 1 |
| Method | Sample 1 (5 mg/mL) | Sample 1 (7 mg/mL) | Sample 1 (10 mg/mL) |
|---|---|---|---|
| Acetone precipitation | 439 | 520 | 530 |
| FASP | 362 | 456 | 441 |
| Protein ID | Description | FSGS 1 vs. FSGS 2 | FSGS 2 vs. MCD | Direction Change in FSGS 2 | Average Fold Change between Groups | Validated in at Least 1 Group | Validated in Both Groups | |||
|---|---|---|---|---|---|---|---|---|---|---|
| TIMS LFQ (Discovery Phase) | QQQ SIS MRM (Validation Phase) | TIMS LFQ (Discovery Phase) | QQQ SIS MRM (Validation Phase) | |||||||
| Significant FSGS 1 vs. FSGS 2 (−10 × LOG(p) > 20) | Significant FSGS 1 vs. FSGS 2 (p < 0.05) | Significant FSGS 2 vs. MCD (−10 × LOG(p) > 20) | Significant FSGS 2 vs. MCD (p < 0.05) | |||||||
| 1 | P04004 | Vitronectin | + | + | + | + | up | 10 | + | + |
| 2 | P06727 | Apolipoprotein A-IV | + | + | + | + | up | 10 | + | + |
| 3 | P19823 | Inter-alpha-trypsin inhibitor heavy chain H2 | + | + | + | + | up | 9 | + | + |
| 4 | P02774 | Vitamin D-binding protein | + | + | + | + | up | 8 | + | + |
| 5 | P61769 | Beta-2-microglobulin | + | + | + | + | up | 8 | + | + |
| 6 | P0C0L5 | Complement C4-B | + | + | + | + | up | 7 | + | + |
| 7 | P02765 | Alpha-2-HS-glycoprotein | + | + | + | + | up | 6 | + | + |
| 8 | P02790 | Hemopexin | + | + | + | + | up | 6 | + | + |
| 9 | P05155 | Plasma protease C1 inhibitor | + | + | + | + | up | 6 | + | + |
| 10 | P02753 | Retinol-binding protein 4 | + | + | + | + | up | 6 | + | + |
| 11 | P00747 | Plasminogen | + | + | + | + | up | 6 | + | + |
| 12 | P00734 | Prothrombin | + | + | + | + | up | 6 | + | + |
| 13 | P02766 | Transthyretin | + | + | + | + | up | 5 | + | + |
| 14 | P06312 | Immunoglobulin kappa variable 4-1 | + | + | + | + | up | 3 | + | + |
| 15 | P10909 | Clusterin | + | + | + | up | 3 | + | ||
| 16 | P02748 | Complement component C9 | + | + | + | up | 11 | + | ||
| 17 | P00751 | Complement factor B | + | + | + | up | 11 | + | ||
| 18 | P51884 | Lumican | + | + | + | up | 9 | + | ||
| 19 | P05156 | Complement factor I | + | + | + | up | 6 | + | ||
| 20 | P01034 | Cystatin-C | + | + | + | up | 3 | + | ||
| 21 | P06396 | Gelsolin | + | + | up | 2 | + | |||
| 22 | Q08380 | Galectin-3-binding protein | + | + | down | 6 | + | |||
| Protein Group | Description | Clinical/Histological Form | Pathogenetic Role |
|---|---|---|---|
| 1 | Lumican | FSGS 2 group | Lumican, an extracellular matrix proteoglycan, related to ECM accumulation [22] |
| 2 | Vitamin D-binding protein | FSGS 2 group | Potential marker of renal interstitial inflammation and fibrosis, and steroid-resistant nephrotic syndrome [18,19,20] |
| 3 | Plasminogen | FSGS 2 group | Plasma abundant protein. Converts to plasmin, may activate epithelial sodium channels causing sodium retention and edema [23] |
| 4 | Hemopexin | FSGS 2 group | Hemopexin induces nephrin-dependent reorganization of the actin cytoskeleton in podocytes [24,25,26] |
| 5 | Prothrombin | FSGS 2 group | Plasma abundant protein |
| 6 | Complement factor I | FSGS 2 group | Plasma abundant protein |
| 7 | Inter-alpha-trypsin inhibitor heavy chain H2 | FSGS 2 group | The inter-alpha-trypsin inhibitors (ITI) are a family of structurally related plasma serine protease inhibitors involved in extracellular matrix stabilization. ITIs are involved in the accumulation of tubulo-interstitial fibrosis in severe forms of FSGS and it activates CD44 + parietal profibrogenic cells in FSGS [27,28,29] |
| 8 | Transthyretin | FSGS 2 group | Plasma abundant protein |
| 9 | Complement factor B | FSGS 2 group | The complement components C4B showed a massive increase in protein abundance in FSGS [30,31] |
| 10 | Apolipoprotein A-I | FSGS 2 group | ApoA-1b is noted to be present in the urine of recurrent FSGS possibly correlating with disease activity [32,33,34] |
| Apolipoprotein A-IV | FSGS 2 | Plasma abundant protein | |
| 11 | Complement component C9 | FSGS 2 | The complement components C1 and C4B, properdin (CFP) showed a massive increase in protein abundance in FSGS [30] |
| 12 | Plasma protease C1 inhibitor | FSGS 2 | Activation of the C1 complex is under control of the C1-inhibitor. It forms a proteolytically inactive complex with the C1r or C1s proteases. May play a potentially crucial role in regulating important physiological pathways including complement activation, blood coagulation, fibrinolysis and the generation of kinins. Acute phase marker [35] |
| 14 | Alpha-2-HS-glycoprotein/Fetuin A | FSGS 2 | In proteinuric patients, significant urinary losses of fetuin-A may cause low serum fetuin-A levels. However, its peptides are elevated in the urine of patients with a high percentage of TIF [36,37] |
| 15 | Retinol-binding protein 4 | FSGS 2 | It is filtered through the GBM and reabsorbed in the tubules, reflecting lysosomal proteolysis in the tubular epithelium. Its increase primarily indicates tubular damage. In addition, its level is associated with response to therapy. [21] |
| 16 | Vitronectin | FSGS 2 | Vitronectin activates integrins, through which podocytes are attached to the GBM. Possibly vitronectin activation is involved in podocyte detachment from GBM [38] |
| 17 | Beta-2-microglobulin | FSGS 2 | Plasma abundant protein |
| 18 | Immunoglobulin kappa variable 4-1 | FSGS 2 | Plasma abundant protein |
| 19 | Gelsolin | FSGS 2 | Gelsolin, a Ca-dependent actin-binding protein, induces a change in the orientation of the actin filament, indicating a conformational change in actin [39,40] |
| 20 | Cystatin | FSGS 2 | Urinary cystatin C as a specific marker of tubular dysfunction [41] |
| 21 | Clusterin | FSGS 2 | Clusterin facilitates in vivo clearance of extracellular misfolded proteins and apoptosis. Clusterin has been postulated as a down modulator of the inflammatory response [42] |
| 22 | Complement C4-B | FSGS 2 | The complement components C1 and C4B, properdin (CFP) showed a massive increase in protein abundance in FSGS [30,43] |
| 23 | Galectin-3-binding protein | FSGS 1 and MCD | Galectin-3-binding protein is a secreted, hyperglycosylated protein expressed by the majority of human cells. Urinary G3BP is a non-invasive biomarker for clinically and histologically reflecting lupus nephritis activity [44,45] |
| total 22 proteins | |||
| Parameters | FSGS 1 (n = 30) | MCD 2 (n = 9) |
|---|---|---|
| Age, years | 40 (27.3; 57.8) | 35 (28; 59) |
| Gender (male), n (%) | 18 (60) | 2 (22.2) |
| Arterial hypetension, n (%) | 22 (73.3) | 2 (22.2) |
| Proteinuria, g/24h | 3.66 (2.50; 5.00) | 3.24 (2.03; 3.5) |
| Serum albumin, g/L | 26.55 (20.85; 33.68) | 29.3 (20.00; 35.80) |
| Serum protein, g/L | 50.8 (40.86; 58.23) | 61.4 (46.5; 65.3) |
| Nephrotic syndrome, n (%) | 21 (70) | 9 (100) |
| Creatinine, mkmol/L | 109.31 (77.57; 152.65) | 85.9 (71.8; 115.9) |
| eGFR2 CKD-EPI 3,mL/min/1.73 m2 | 64.68 (41.4; 97.09) | 73 (55.58; 105.00) |
| eGFR< 60 mL/min/1.73 m2, n (%) | 12 (40.0) | 4 (44.4) |
| Steroid-resistant NS, n (%) | 14 (46.7) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chebotareva, N.V.; Vinogradov, A.; Brzhozovskiy, A.G.; Kashirina, D.N.; Indeykina, M.I.; Bugrova, A.E.; Lebedeva, M.; Moiseev, S.; Nikolaev, E.N.; Kononikhin, A.S. Potential Urine Proteomic Biomarkers for Focal Segmental Glomerulosclerosis and Minimal Change Disease. Int. J. Mol. Sci. 2022, 23, 12607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232012607
Chebotareva NV, Vinogradov A, Brzhozovskiy AG, Kashirina DN, Indeykina MI, Bugrova AE, Lebedeva M, Moiseev S, Nikolaev EN, Kononikhin AS. Potential Urine Proteomic Biomarkers for Focal Segmental Glomerulosclerosis and Minimal Change Disease. International Journal of Molecular Sciences. 2022; 23(20):12607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232012607
Chicago/Turabian StyleChebotareva, Natalia V., Anatoliy Vinogradov, Alexander G. Brzhozovskiy, Daria N. Kashirina, Maria I. Indeykina, Anna E. Bugrova, Marina Lebedeva, Sergey Moiseev, Evgeny N. Nikolaev, and Alexey S. Kononikhin. 2022. "Potential Urine Proteomic Biomarkers for Focal Segmental Glomerulosclerosis and Minimal Change Disease" International Journal of Molecular Sciences 23, no. 20: 12607. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms232012607