
Rapid Discrimination of Neuromyelitis Optica Spectrum Disorder and Multiple Sclerosis Using Machine Learning on Infrared Spectra of Sera

 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
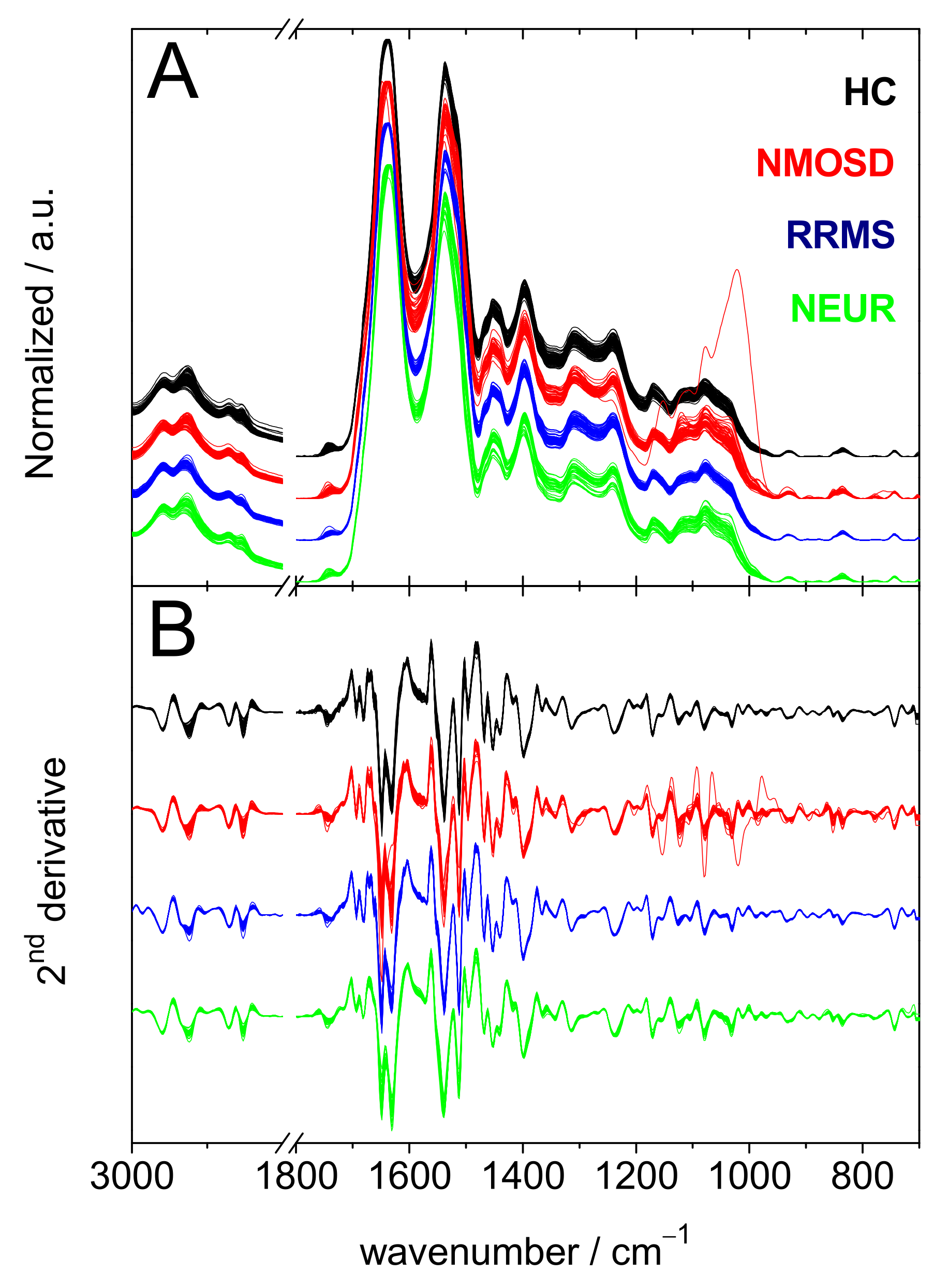
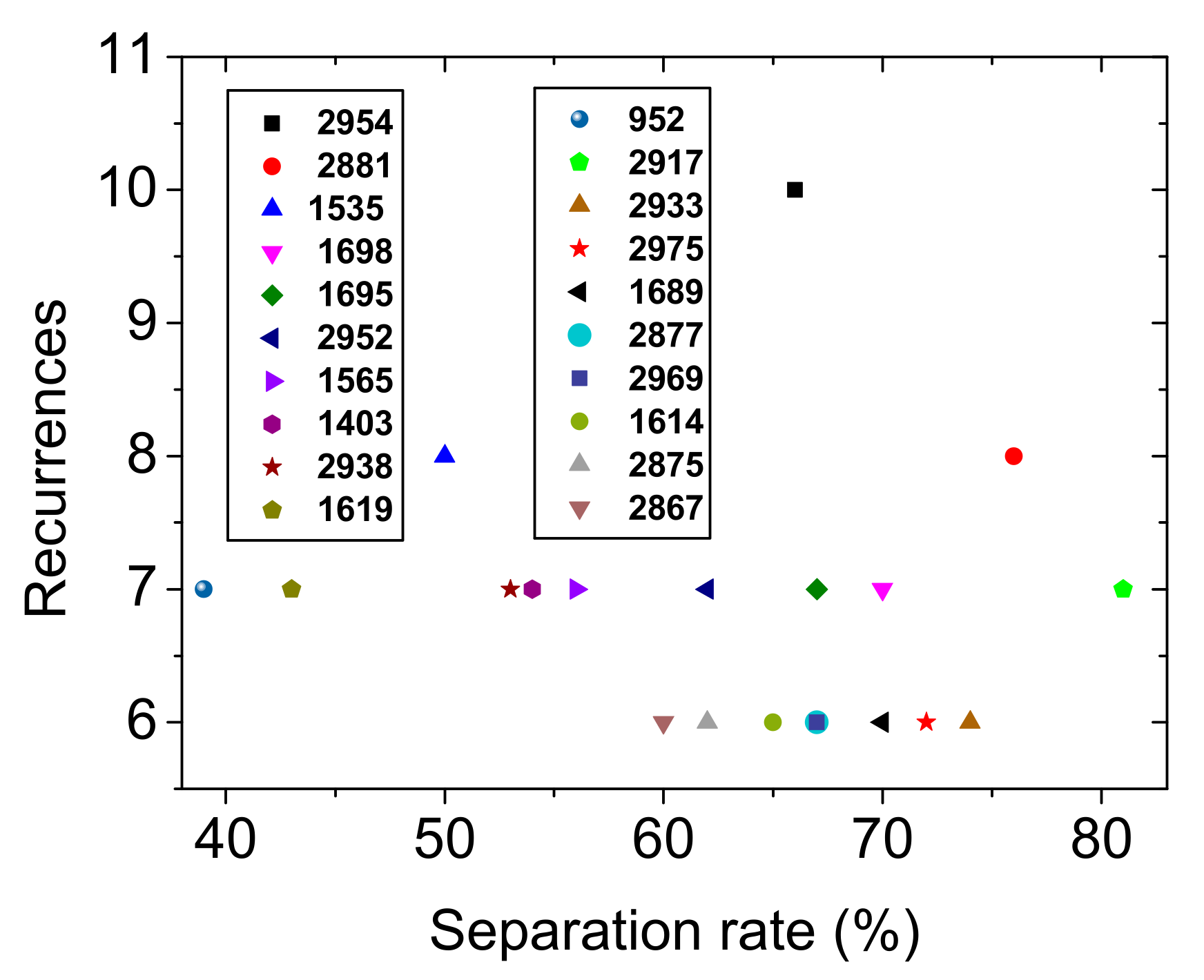
2.1. HC vs. NMOSD vs. RRMS vs. NEUR
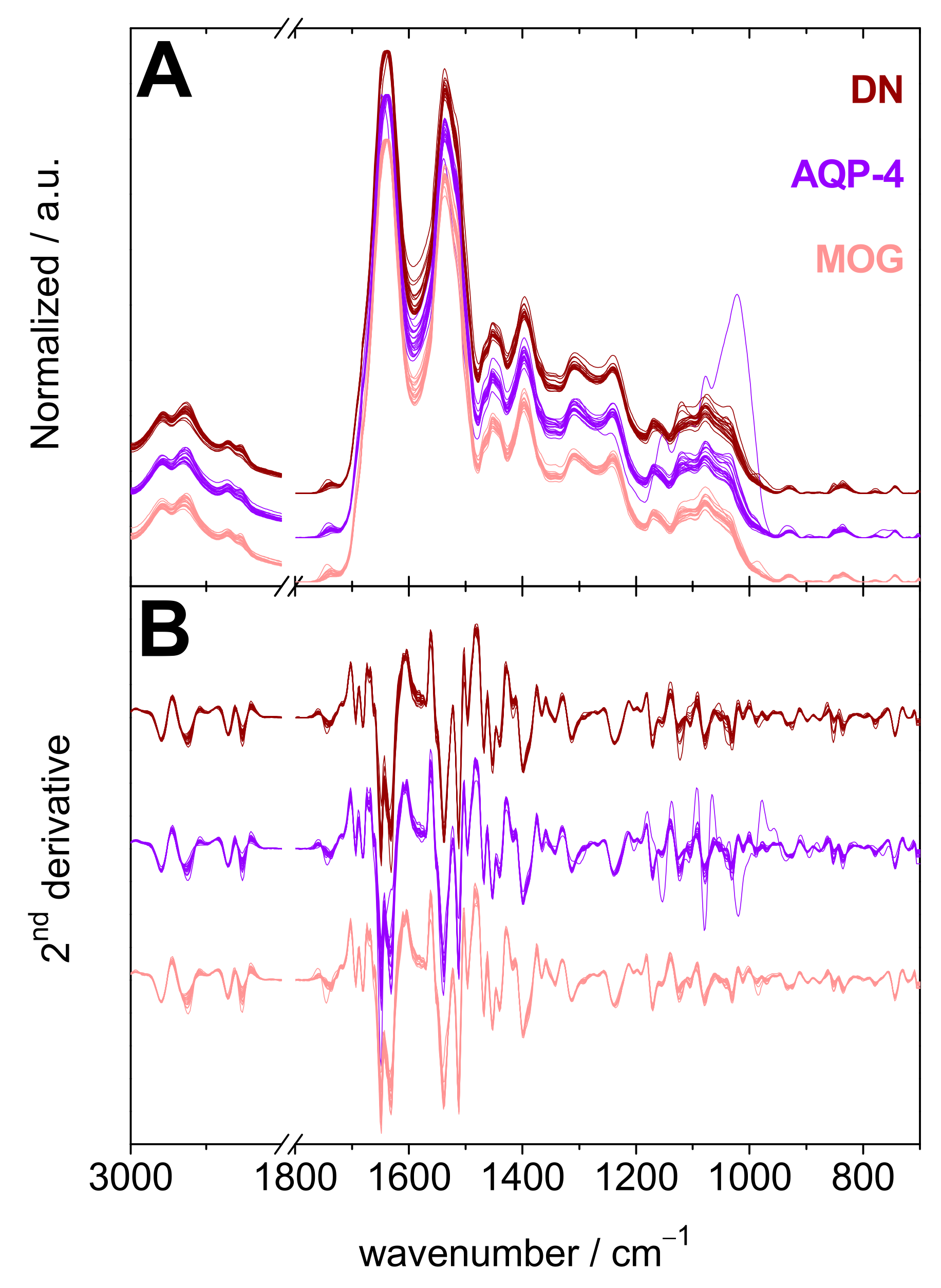
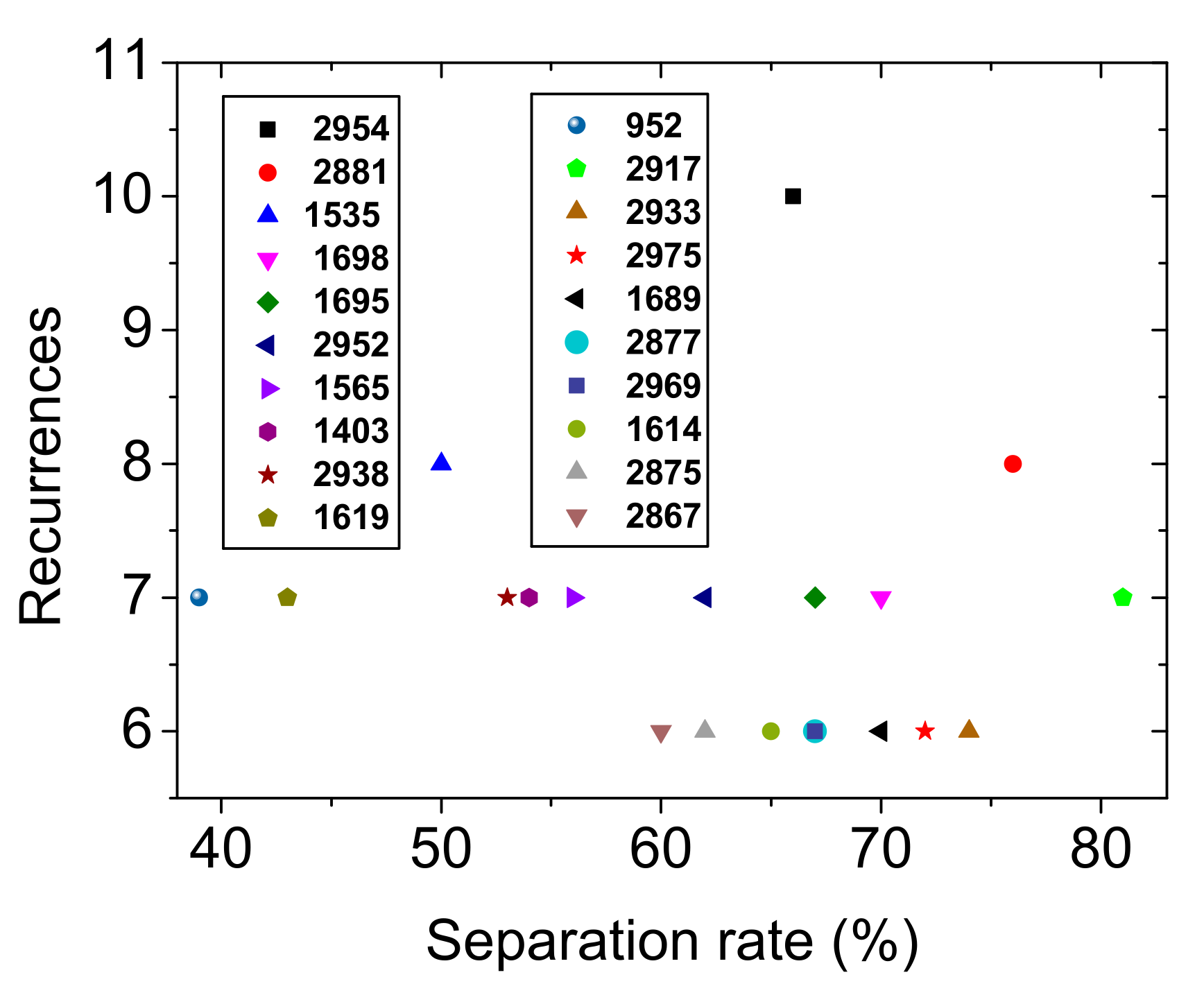
2.2. AQP-4 vs. MOG. vs. DN
2.3. RRMS vs. DN, RRMS vs. MOG and RRMS vs. AQP-4
3. Discussion
4. Materials and Methods
4.1. Sample Preparation
4.2. Fourier Transform Infrared Spectroscopy
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Wingerchuk, D.M.; Lennon, V.A.; Pittock, S.J.; Lucchinetti, C.F.; Weinshenker, B.G. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006, 66, 1485–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wingerchuk, D.M.; Banwell, B.; Bennett, J.L.; Cabre, P.; Carroll, W.; Chitnis, T.; de Seze, J.; Fujihara, K.; Greenberg, B.; Jacob, A.; et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015, 85, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Marignier, R.; Bernard-Valnet, R.; Giraudon, P.; Collongues, N.; Papeix, C.; Zephir, H.; Cavillon, G.; Rogemond, V.; Casey, R.; Frangoulis, B.; et al. Aquaporin-4 antibody-negative neuromyelitis optica Distinct assay sensitivity-dependent entity. Neurology 2013, 80, 2194–2200. [Google Scholar] [CrossRef] [PubMed]
- Probstel, A.K.; Rudolf, G.; Dornmair, K.; Collongues, N.; Chanson, J.B.; Sanderson, N.S.; Lindberg, R.L.; Kappos, L.; de Seze, J.; Derfuss, T. Anti-MOG antibodies are present in a subgroup of patients with a neuromyelitis optica phenotype. J. Neuroinflamm. 2015, 12, 46. [Google Scholar] [CrossRef] [Green Version]
- Cobo-Calvo, A.; Ruiz, A.; Marignier, R. Myelin oligodendrocyte glycoprotein antibody associated disease: About the importance of diagnostic assays and selection of the target population in retrospective studies. Eur. J. Neurol. 2019, 26, e58–e59. [Google Scholar] [CrossRef]
- Reindl, M.; Schanda, K.; Woodhall, M.; Tea, F.; Ramanathan, S.; Sagen, J.; Fryer, J.P.; Mills, J.; Teegen, B.; Mindorf, S.; et al. International multicenter examination of MOG antibody assays. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e674. [Google Scholar] [CrossRef] [Green Version]
- Jarius, S.; Paul, F.; Aktas, O.; Asgari, N.; Dale, R.C.; de Seze, J.; Franciotta, D.; Fujihara, K.; Jacob, A.; Kim, H.J.; et al. MOG encephalomyelitis: International recommendations on diagnosis and antibody testing. J. Neuroinflamm. 2018, 15, 134. [Google Scholar] [CrossRef]
- Hamid, S.H.M.; Whittam, D.; Mutch, K.; Linaker, S.; Solomon, T.; Das, K.; Bhojak, M.; Jacob, A. What proportion of AQP4-IgG-negative NMO spectrum disorder patients are MOG-IgG positive? A cross sectional study of 132 patients. J. Neurol. 2017, 264, 2088–2094. [Google Scholar] [CrossRef] [Green Version]
- Collongues, N.; Ayme-Dietrich, E.; Monassier, L.; de Seze, J. Pharmacotherapy for Neuromyelitis Optica Spectrum Disorders: Current Management and Future Options. Drugs 2019, 79, 125–142. [Google Scholar] [CrossRef]
- Collongues, N.; Cabre, P.; Marignier, R.; Zephir, H.; Papeix, C.; Audoin, B.; Lebrun-Frenay, C.; Pelletier, J.; Fontaine, B.; Vermersch, P.; et al. A benign form of neuromyelitis optica: Does it exist? Arch. Neurol. 2011, 68, 918–924. [Google Scholar] [CrossRef] [Green Version]
- Collongues, N.; Marignier, R.; Zephir, H.; Papeix, C.; Blanc, F.; Ritleng, C.; Tchikviladze, M.; Outteryck, O.; Vukusic, S.; Fleury, M.; et al. Neuromyelitis optica in France: A multicenter study of 125 patients. Neurology 2010, 74, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Papeix, C.; Vidal, J.S.; de Seze, J.; Pierrot-Deseilligny, C.; Tourbah, A.; Stankoff, B.; Lebrun, C.; Moreau, T.; Vermersch, P.; Fontaine, B.; et al. Immunosuppressive therapy is more effective than interferon in neuromyelitis optica. Mult. Scler. 2007, 13, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Jurynczyk, M.; Weinshenker, B.; Akman-Demir, G.; Asgari, N.; Barnes, D.; Boggild, M.; Chaudhuri, A.; D’hooghe, M.; Evangelou, N.; Geraldes, R.; et al. Status of diagnostic approaches to AQP4-IgG seronegative NMO and NMO/MS overlap syndromes. J. Neurol. 2016, 263, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Jurynczyk, M.; Tackley, G.; Kong, Y.; Geraldes, R.; Matthews, L.; Woodhall, M.; Waters, P.; Kuker, W.; Craner, M.; Weir, A.; et al. Brain lesion distribution criteria distinguish MS from AQP4-antibody NMOSD and MOG-antibody disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Brilot, F.; Dale, R.C.; Selter, R.C.; Grummel, V.; Kalluri, S.R.; Aslam, M.; Busch, V.; Zhou, D.; Cepok, S.; Hemmer, B. Antibodies to Native Myelin Oligodendrocyte Glycoprotein in Children with Inflammatory Demyelinating Central Nervous System Disease. Ann. Neurol. 2009, 66, 833–842. [Google Scholar] [CrossRef]
- El Khoury, Y.; Collongues, N.; De Seze, J.; Gulsari, V.; Patte-Mensah, C.; Marcou, G.; Varnek, A.; Mensah-Nyagan, A.G.; Hellwig, P. Serum-based differentiation between multiple sclerosis and amyotrophic lateral sclerosis by Random Forest classification of FTIR spectra. Analyst 2019, 144, 4647–4652. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.J.; Trevisan, J.; Bassan, P.; Bhargava, R.; Butler, H.J.; Dorling, K.M.; Fielden, P.R.; Fogarty, S.W.; Fullwood, N.J.; Heys, K.A.; et al. Using Fourier transform IR spectroscopy to analyze biological materials. Nat. Protoc. 2014, 9, 1771–1791. [Google Scholar] [CrossRef] [Green Version]
- Bonnier, F.; Blasco, H.; Wasselet, C.; Brachet, G.; Respaud, R.; Carvalho, L.F.; Bertrand, D.; Baker, M.J.; Byrne, H.J.; Chourpa, I. Ultra-filtration of human serum for improved quantitative analysis of low molecular weight biomarkers using ATR-IR spectroscopy. Analyst 2017, 142, 1285–1298. [Google Scholar] [CrossRef] [Green Version]
- Rehman, I.U.; Movasaghi, Z.; Rehman, S. Vibrational Spectroscopy for Tissue Analysis, 1st ed.; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- Ghomi, M.; Letellier, R.; Liquier, J.; Taillandier, E. Interpretation of DNA vibrational spectra by normal coordinate analysis. Int. J. Biochem. 1990, 22, 691–699. [Google Scholar] [CrossRef]
- Martin, W.B.; Mirov, S.; Venugopalan, R. Using two discrete frequencies within the middle infrared to quantitatively determine glucose in serum. J. Biomed. Opt. 2002, 7, 613–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hands, J.R.; Dorling, K.M.; Abel, P.; Ashton, K.M.; Brodbelt, A.; Davis, C.; Dawson, T.; Jenkinson, M.D.; Lea, R.W.; Walker, C.; et al. Attenuated total reflection fourier transform infrared (ATR-FTIR) spectral discrimination of brain tumour severity from serum samples. J. Biophotonics 2014, 7, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Ollesch, J.; Heinze, M.; Heise, H.M.; Behrens, T.; Brüning, T.; Gerwert, K. It’s in your blood: Spectral biomarker candidates for urinary bladder cancer from automated FTIR spectroscopy. J. Biophotonics 2014, 7, 210–221. [Google Scholar] [CrossRef]
- Paraskevaidi, M.; Morais, C.L.M.; Lima, K.M.G.; Snowden, J.S.; Saxon, J.A.; Richardson, A.M.T.; Jones, M.; Mann, D.M.A.; Allsop, D.; Martin-Hirsch, P.L.; et al. Differential diagnosis of Alzheimer’s disease using spectrochemical analysis of blood. Proc. Natl. Acad. Sci. USA 2017, 114, E7929–E7938. [Google Scholar] [CrossRef] [Green Version]
- Heraud, P.; Chatchawal, P.; Wongwattanakul, M.; Tippayawat, P.; Doerig, C.; Jearanaikoon, P.; Perez-Guaita, D.; Wood, B.R. Infrared spectroscopy coupled to cloud-based data management as a tool to diagnose malaria: A pilot study in a malaria-endemic country. Malar. J. 2019, 18, 348. [Google Scholar] [CrossRef]
- Butler, H.J.; Brennan, P.M.; Cameron, J.M.; Finlayson, D.; Hegarty, M.G.; Jenkinson, M.D.; Palmer, D.S.; Smith, B.R.; Baker, M.J. Development of high-throughput ATR-FTIR technology for rapid triage of brain cancer. Nat. Comm. 2019, 10, 4501. [Google Scholar] [CrossRef] [Green Version]
- Naseer, K.; Ali, S.; Qazi, J. ATR-FTIR spectroscopy as the future of diagnostics: A systematic review of the approach using bio-fluids. Appl. Spectrosc. Rev. 2021, 56, 85–97. [Google Scholar] [CrossRef]
- Byrne, H.J.; Bonnier, F.; McIntyre, J.; Parachalil, D.R. Quantitative analysis of human blood serum using vibrational spectroscopy. Clin. Spectrosc. 2020, 2, 100004. [Google Scholar] [CrossRef]
- Leal, L.B.; Nogueira, M.S.; Canevari, R.A.; Carvalho, L. Vibration spectroscopy and body biofluids: Literature review for clinical applications. Photodiagnosis Photodyn. Ther. 2018, 24, 237–244. [Google Scholar] [CrossRef]
- Baker, M.J.; Hussain, S.R.; Lovergne, L.; Untereiner, V.; Hughes, C.; Lukaszewski, R.A.; Thiefin, G.; Sockalingum, G.D. Developing and understanding biofluid vibrational spectroscopy: A critical review. Chem. Soc. Rev. 2016, 45, 1803–1818. [Google Scholar] [CrossRef] [Green Version]
- Witten, I.H.; Frank, E.; Hall, M.A.; Pal, C.J. Data Mining: Practical Machine Learning Tools and Techniques; Morgan Kaufmann: Burlington, MA, USA, 2016. [Google Scholar]
- Alves Do Rego, C.; Collongues, N. Neuromyelitis optica spectrum disorders: Features of aquaporin-4, myelin oligodendrocyte glycoprotein and double-seronegative-mediated subtypes. Rev. Neurol. 2018, 174, 458–470. [Google Scholar] [CrossRef] [PubMed]
- Barth, A. Infrared spectroscopy of proteins. Biochim. Biophy. Acta 2007, 1767, 1073–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathology | Classified as | ROC AUC (%) | Sensitivity (%) | Specificity (%) | Precision (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| HC | NMOSD | RRMS | NEUR | ||||||
| 2-fold cross-validation | HC | 68 | 2 | 0 | 0 | 99.8 (99.5 ± 0.5) | 97.1 (99.4 ± 0.9) | 98.6 (93.3 ± 5.1) | 97.1 (96.7 ± 2.4) |
| NMOSD | 1 | 53 | 0 | 0 | 99.6 (98.7 ± 0.9) | 98.1 (99.0 ± 1.3) | 98.7 (78.3 ± 7.3) | 96.4 (92.9 ± 2.3) | |
| RRMS | 0 | 0 | 54 | 0 | 100 (100 ± 0.0) | 100 (100 ± 0.0) | 100 (96.9 ± 2.8) | 100 (98.9 ± 0.9) | |
| NEUR | 1 | 0 | 0 | 29 | 100 (100 ± 0.0) | 100 (99.9 ± 0.3) | 100 (92.7 ± 10.8) | 100 (98.8 ± 1.7) | |
| Validation set | HC | 10 | 0 | 0 | 0 | 100 | 100 | 100 | 100 |
| NMOSD | 0 | 6 | 0 | 0 | 100 | 100 | 100 | 100 | |
| RRMS | 0 | 0 | 6 | 0 | 100 | 100 | 100 | 100 | |
| NEUR | 0 | 0 | 0 | 5 | 100 | 100 | 100 | 100 | |
| Pathology | Classified as | ROC AUC (%) | Sensitivity (%) | Specificity (%) | Precision (%) | |||
|---|---|---|---|---|---|---|---|---|
| DN | MOG | AQP-4 | ||||||
| 2-fold cross-validation | DN | 10 | 4 | 4 | 61.4 (69.4 ± 6.6) | 55.6 (92.5 ± 8.7) | 66.7 (33.3 ± 13.0) | 45.5 (73.6 ± 3.6) |
| MOG | 5 | 7 | 6 | 58.6 (66.9 ± 7.9) | 38.9 (93.1 ± 5.4) | 72.2 (16.1 ± 12.2) | 41.2 (69.0 ± 3.3) | |
| AQP-4 | 7 | 6 | 5 | 57.9 (61.3 ± 8.9) | 27.8 (85.0 ± 9.2) | 72.2 (26.1 ± 14.1) | 33.3 (69.8 ± 4.3) | |
| Validation set | DN | 1 | 1 | 0 | 75 | 50 | 75 | 50 |
| MOG | 0 | 2 | 0 | 100 | 100 | 5 | 66.7 | |
| AQP-4 | 1 | 0 | 1 | 87.5 | 50 | 0 | 100 | |
| Pathology | Classified as | ROC AUC (%) | Sensitivity (%) | Specificity (%) | Precision (%) | ||
|---|---|---|---|---|---|---|---|
| RRMS | DN | ||||||
| 2-fold cross-validation | RRMS | 54 | 0 | 100 (99.9 ± 0.3) | 100 (95.0 ± 6.7) | 100 (98.9 ± 1.7) | 100 (96.9 ± 4.8) |
| DN | 0 | 18 | 100 (99.8 ± 0.4) | 100 (98.7 ± 1.8) | 100 (95.0 ± 7.6) | 100 (98.4 ± 2.4) | |
| Validation set | RRMS | 6 | 0 | 100 | 100 | 100 | 100 |
| DN | 0 | 2 | 100 | 100 | 100 | 100 | |
| Pathology | Classified as | ROC AUC (%) | Sensitivity (%) | Specificity (%) | Precision (%) | ||
| RRMS | MOG | ||||||
| 2-fold cross-validation | RRMS | 54 | 0 | 100 (99.9 ± 0.3) | 100 (95.0 ± 6.7) | 99.4 (98.9 ± 1.7) | 98.2 (96.9 ± 4.8) |
| MOG | 1 | 17 | 100 (100 ± 0.0) | 99.4 (95.0 ± 10.5) | 100 (99.8 ± 0.8) | 100 (99.5 ± 2.2) | |
| Validation set | RRMS | 6 | 0 | 100 | 100 | 100 | 100 |
| MOG | 0 | 2 | 100 | 100 | 100 | 100 | |
| Pathology | Classified as | ROC AUC (%) | Sensitivity (%) | Specificity (%) | Precision (%) | ||
| RRMS | DN | ||||||
| 2-fold cross-validation | RRMS | 51 | 0 | 99.4 (99.6 ± 0.1) | 100 (93.3 ± 8.4) | 83.3 (100 ± 0.0) | 94.7 (100 ± 0.0) |
| AQP-4 | 3 | 15 | 99.4 (99.9 ± 0.1) | 83.3 (100 ± 0.0) | 100 (91.9 ± 9.9) | 100 (97.2 ± 3.0) | |
| Validation set | RRMS | 6 | 0 | 100 | 100 | 100 | 100 |
| AQP-4 | 0 | 2 | 100 | 100 | 100 | 100 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Khoury, Y.; Gebelin, M.; de Sèze, J.; Patte-Mensah, C.; Marcou, G.; Varnek, A.; Mensah-Nyagan, A.-G.; Hellwig, P.; Collongues, N. Rapid Discrimination of Neuromyelitis Optica Spectrum Disorder and Multiple Sclerosis Using Machine Learning on Infrared Spectra of Sera. Int. J. Mol. Sci. 2022, 23, 2791. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23052791
El Khoury Y, Gebelin M, de Sèze J, Patte-Mensah C, Marcou G, Varnek A, Mensah-Nyagan A-G, Hellwig P, Collongues N. Rapid Discrimination of Neuromyelitis Optica Spectrum Disorder and Multiple Sclerosis Using Machine Learning on Infrared Spectra of Sera. International Journal of Molecular Sciences. 2022; 23(5):2791. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23052791
Chicago/Turabian StyleEl Khoury, Youssef, Marie Gebelin, Jérôme de Sèze, Christine Patte-Mensah, Gilles Marcou, Alexandre Varnek, Ayikoé-Guy Mensah-Nyagan, Petra Hellwig, and Nicolas Collongues. 2022. "Rapid Discrimination of Neuromyelitis Optica Spectrum Disorder and Multiple Sclerosis Using Machine Learning on Infrared Spectra of Sera" International Journal of Molecular Sciences 23, no. 5: 2791. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23052791