
Proteomic Profiling of Saliva and Tears in Radiated Head and Neck Cancer Patients as Compared to Primary Sjögren’s Syndrome Patients

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
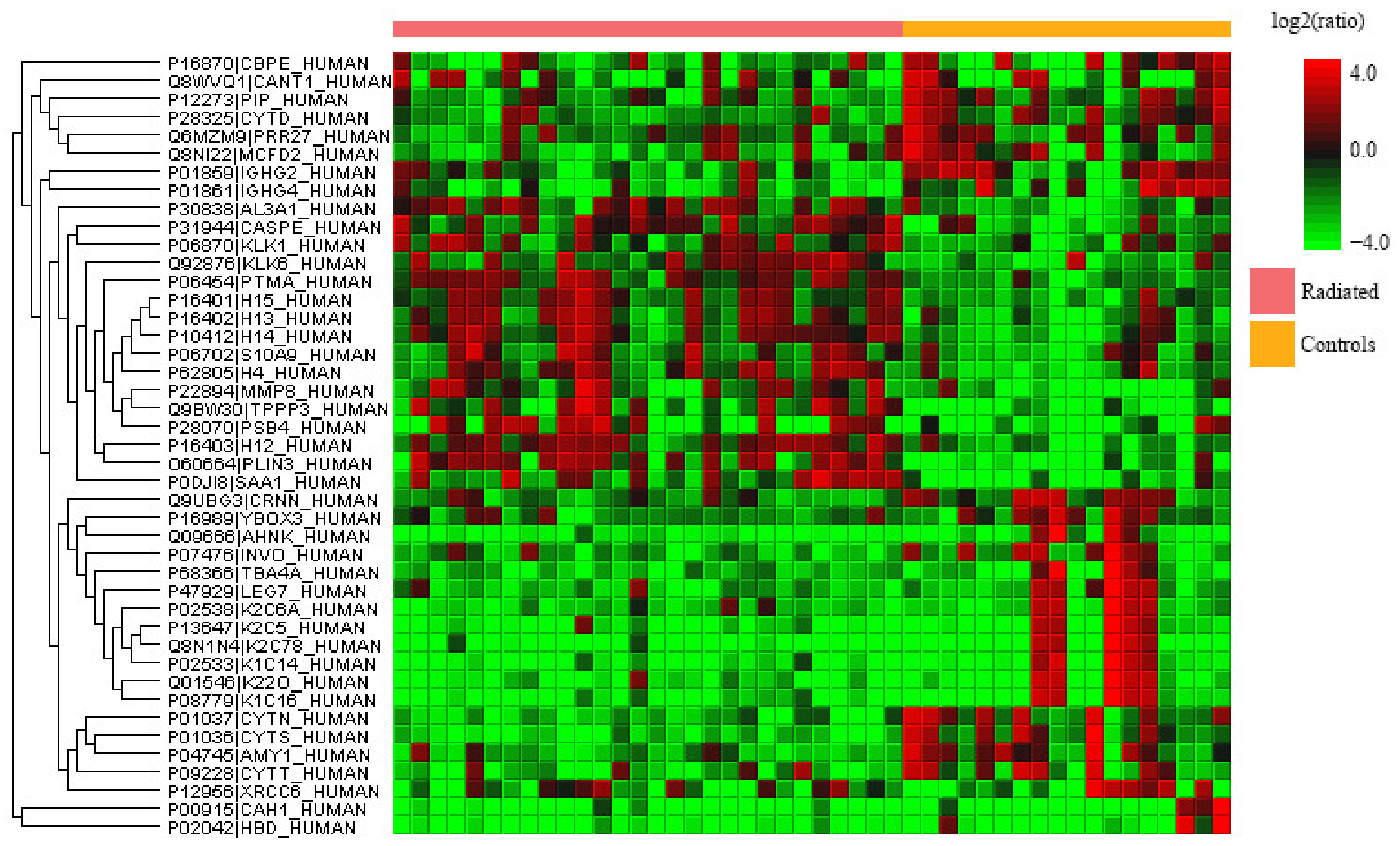
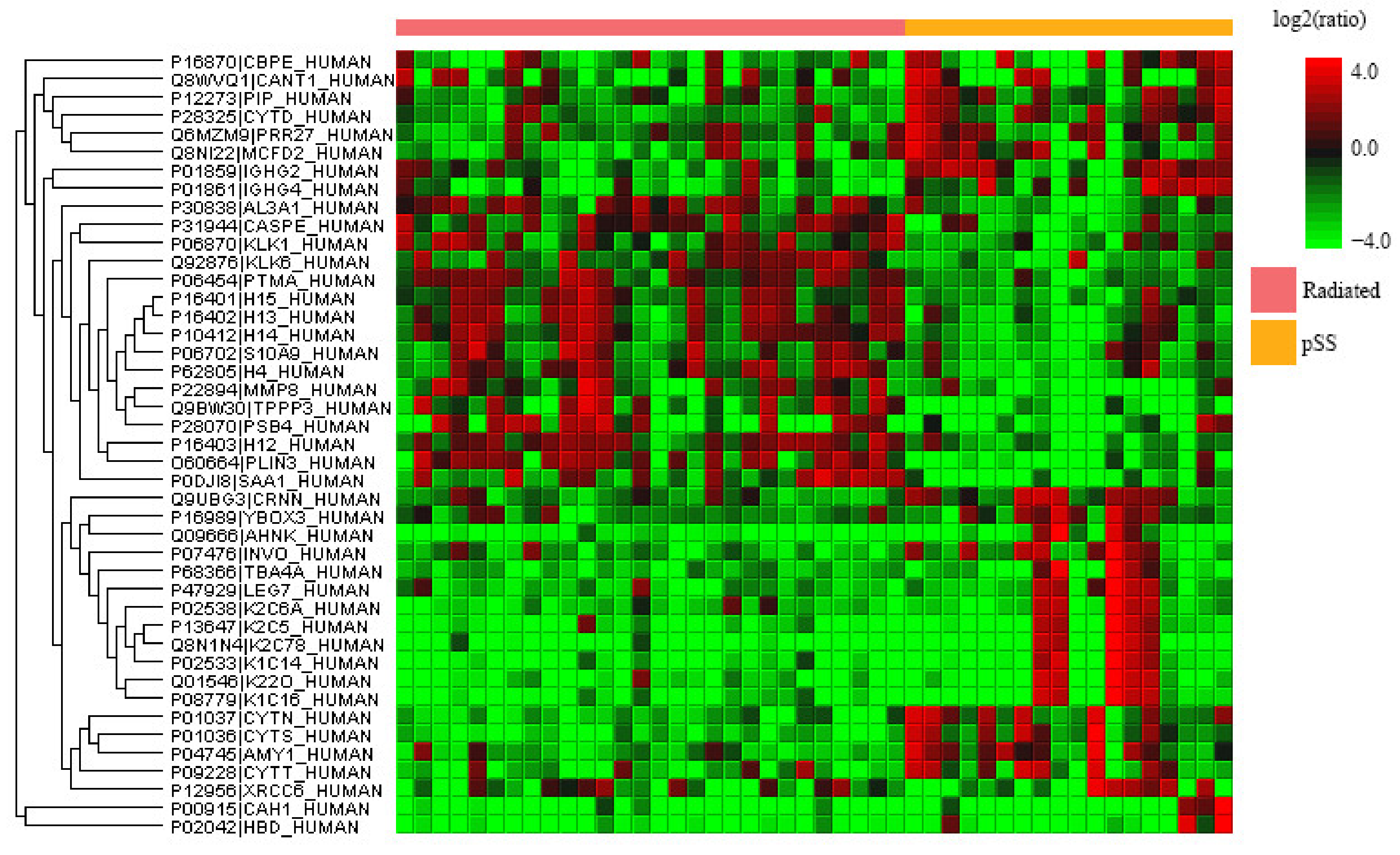
2.1. Quantitative Proteomics Analysis of Whole Saliva
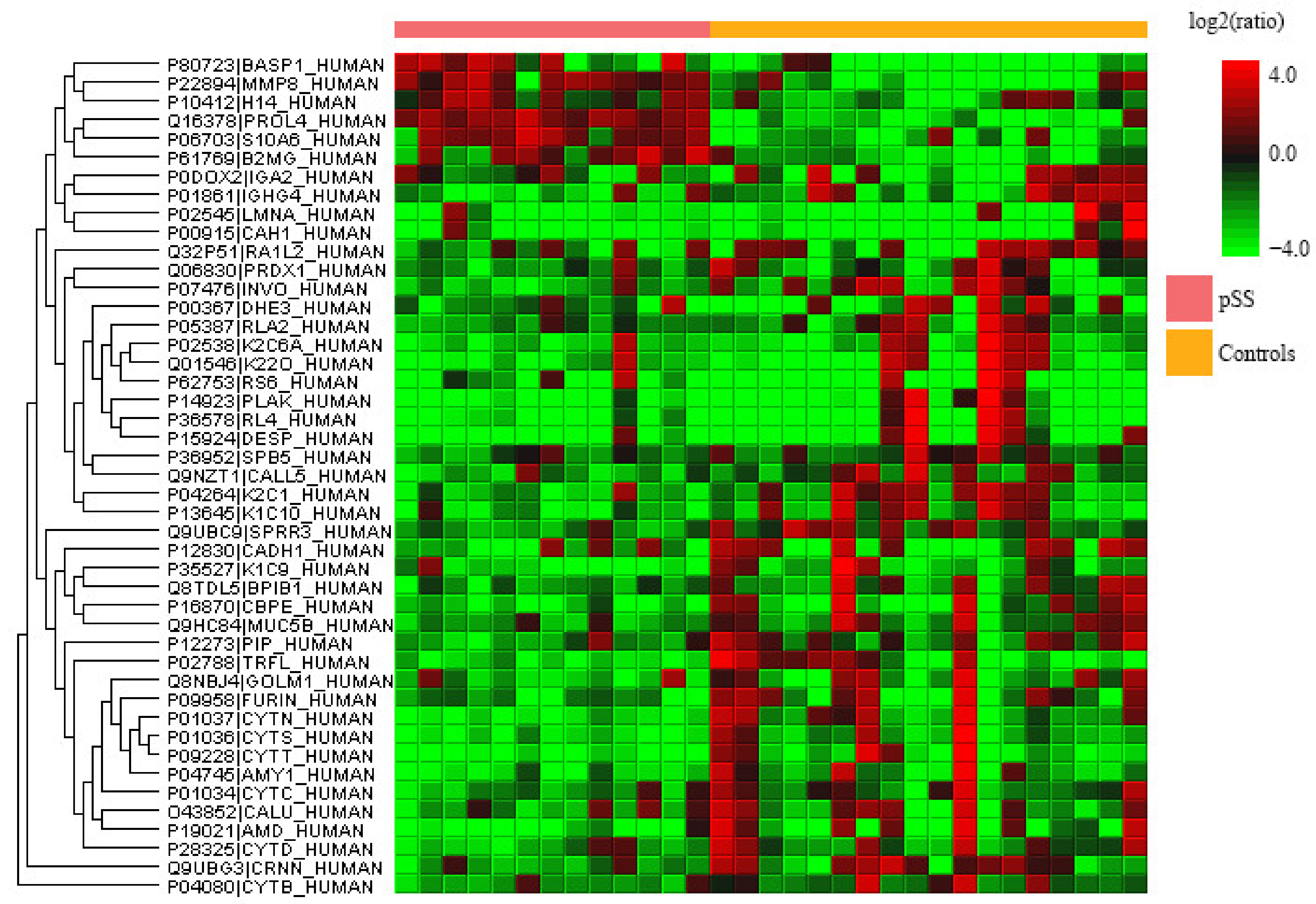
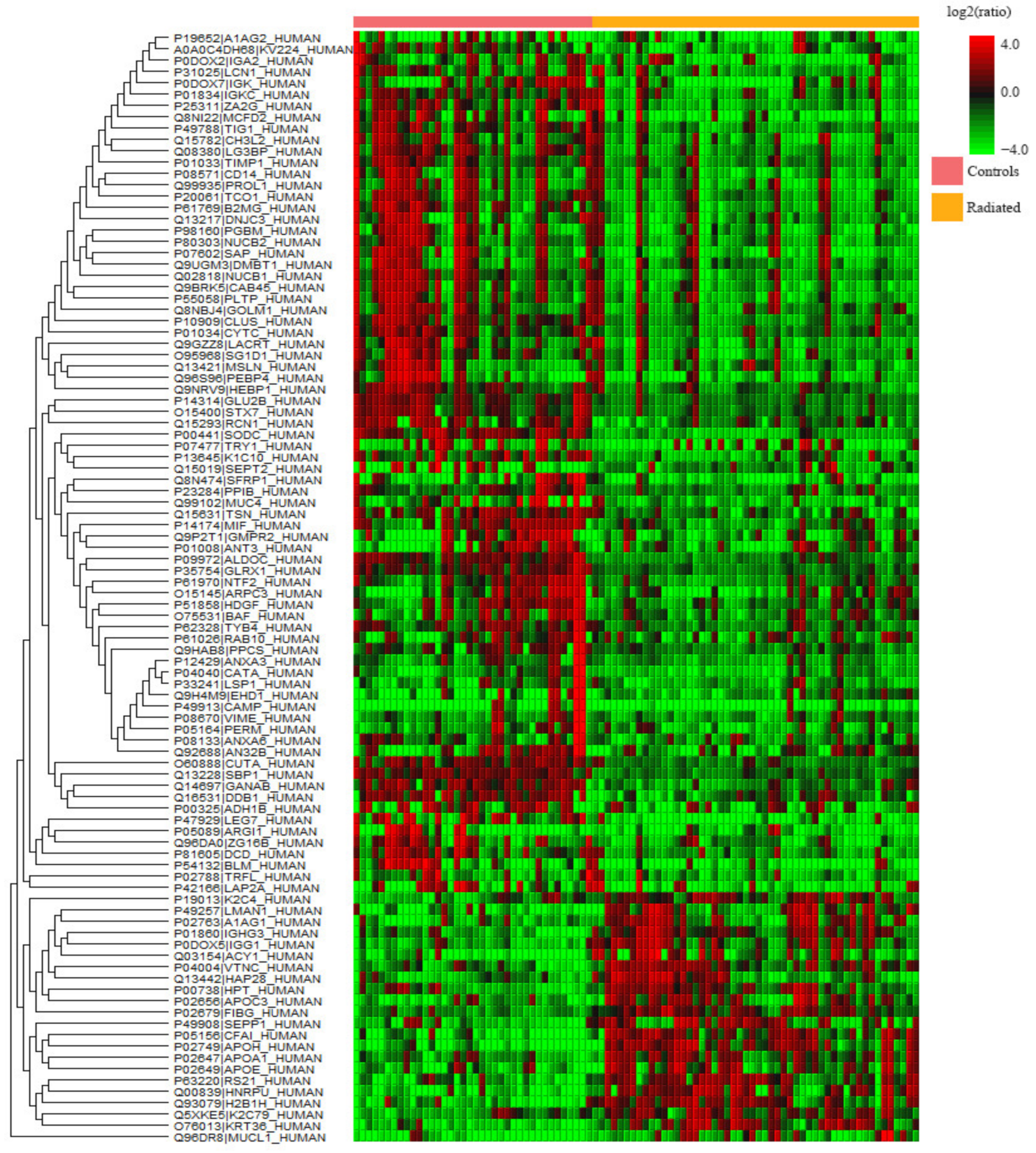
2.2. Quantitative Proteomics Analysis of Tear Fluid
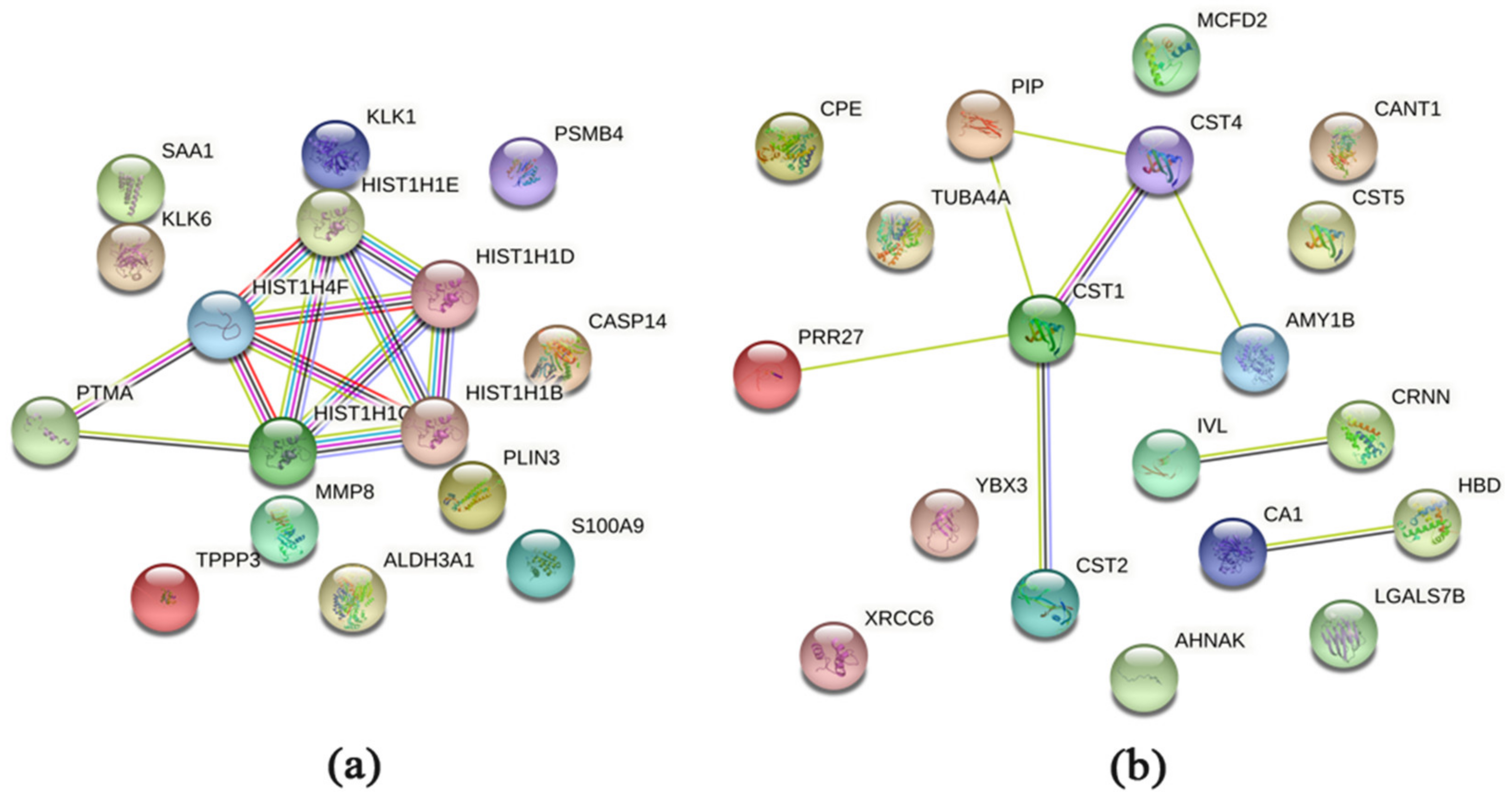
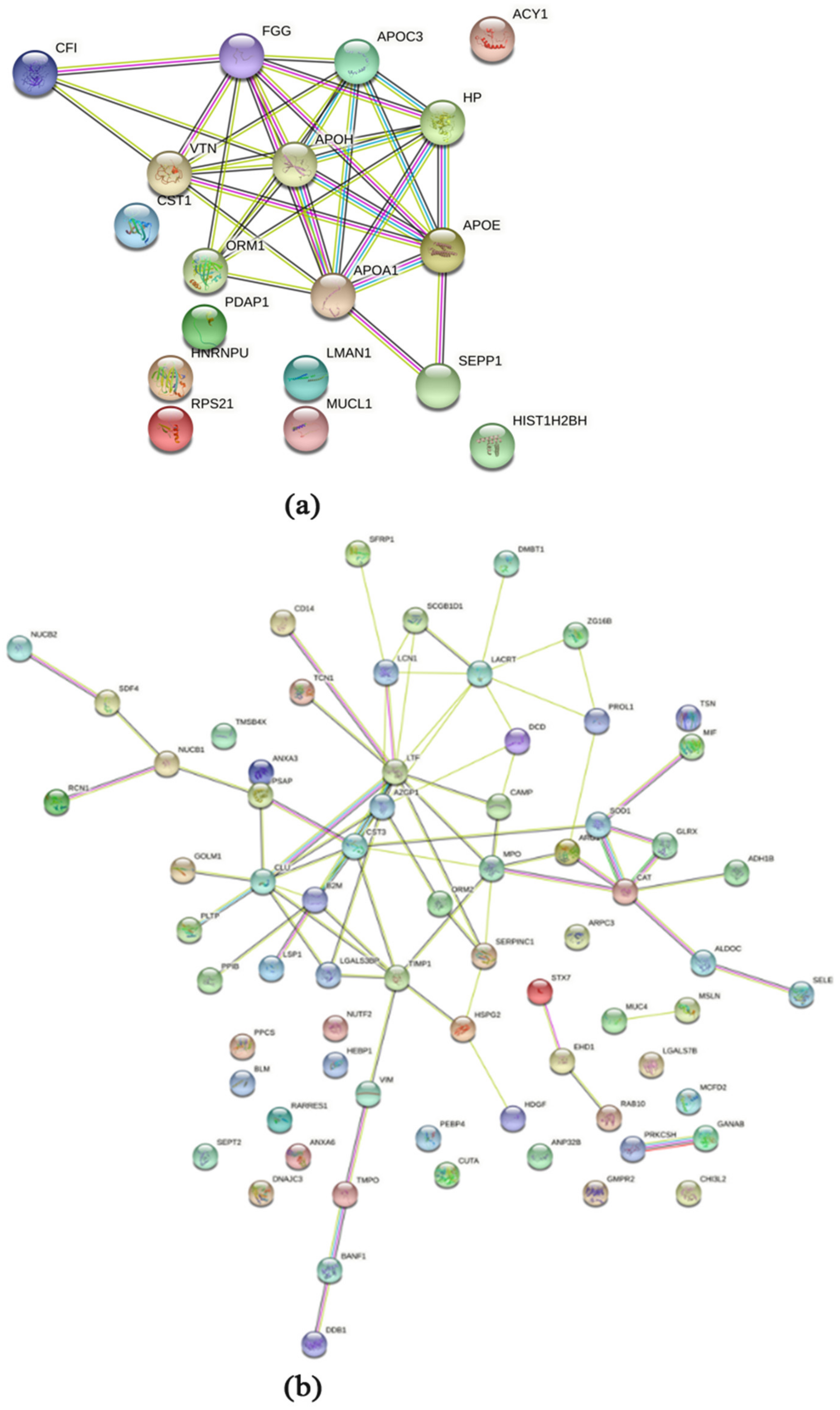
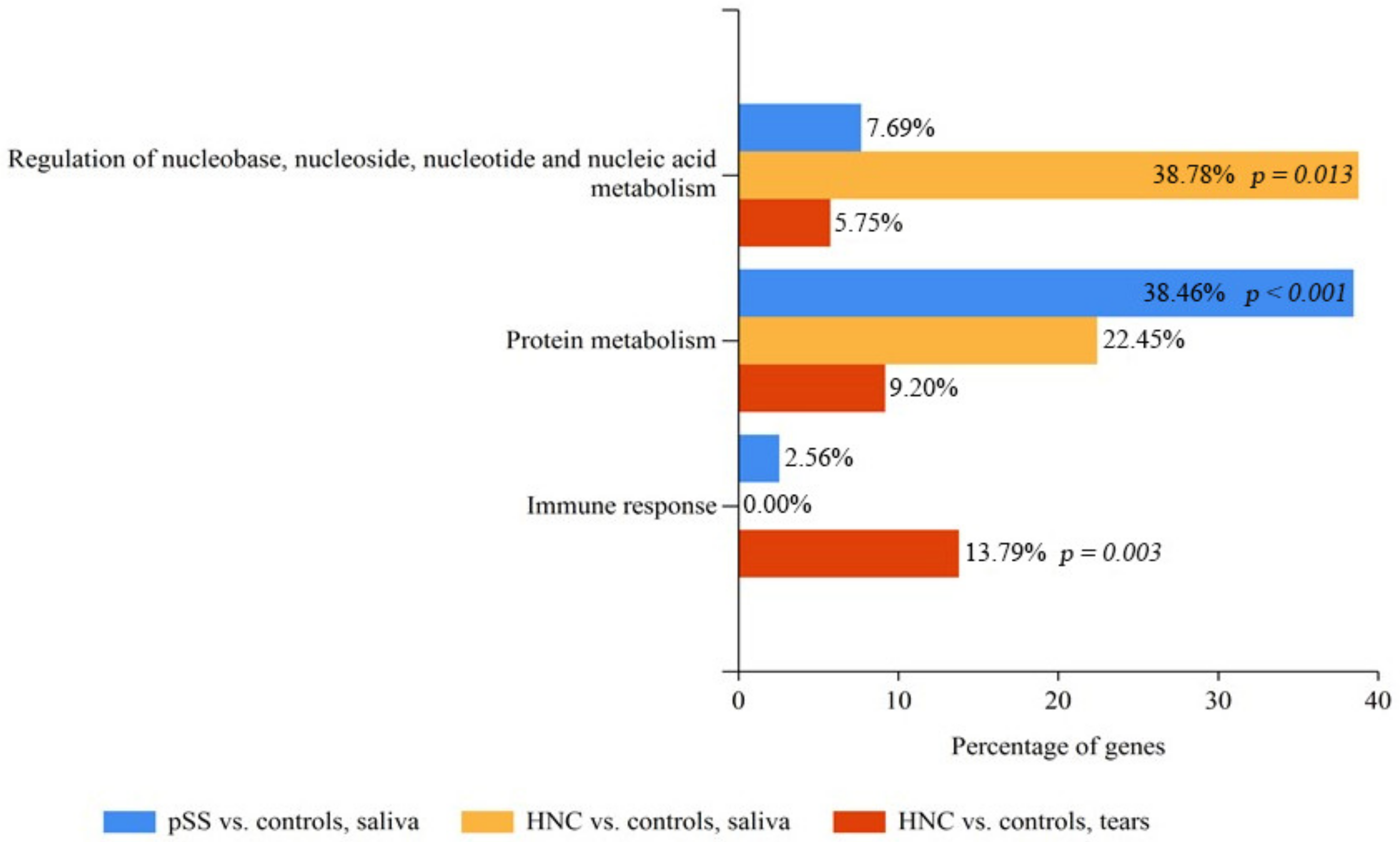
2.3. Pathway and Biological Processes Analysis of Saliva and Tear Material Using DAVID and FunRich
3. Discussion
4. Materials and Methods
4.1. Study Population
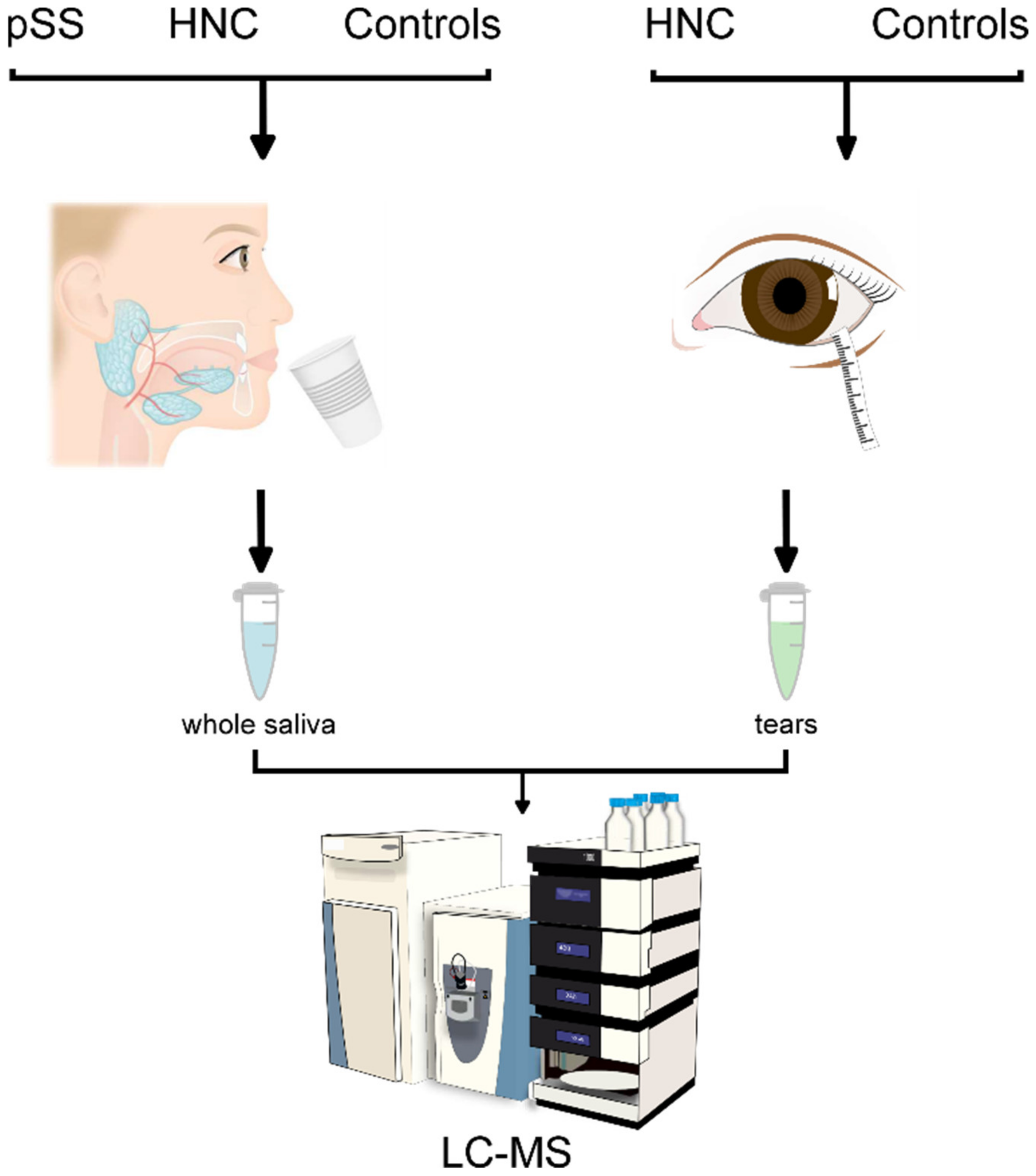
4.2. Whole Saliva and Tear Fluid Collection
4.3. Protein Profiling by LC-MS
4.4. LC-MS Data Processing and Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lo Nigro, C.; Denaro, N.; Merlotti, A.; Merlano, M. Head and neck cancer: Improving outcomes with a multidisciplinary approach. Cancer Manag. Res. 2017, 9, 363–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef] [PubMed]
- Roscher, I.; Falk, R.S.; Vos, L.; Clausen, O.P.F.; Helsing, P.; Gjersvik, P.; Robsahm, T.E. Notice of Retraction and Replacement: Roscher et al. Validating 4 Staging Systems for Cutaneous Squamous Cell Carcinoma Using Population-Based Data: A Nested Case-Control Study. JAMA Dermatol. 2018, 154, 1488–1489. [Google Scholar] [CrossRef]
- Jelonek, K.; Krzywon, A.; Jablonska, P.; Slominska, E.M.; Smolenski, R.T.; Polanska, J.; Rutkowski, T.; Mrochem-Kwarciak, J.; Skladowski, K.; Widlak, P. Systemic Effects of Radiotherapy and Concurrent Chemo-Radiotherapy in Head and Neck Cancer Patients—Comparison of Serum Metabolome Profiles. Metabolites 2020, 10, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirix, P.; Vanstraelen, B.; Jorissen, M.; Vander Poorten, V.; Nuyts, S. Intensity-modulated radiotherapy for sinonasal cancer: Improved outcome compared to conventional radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Nutting, C.M.; Morden, J.P.; Harrington, K.J.; Urbano, T.G.; Bhide, S.A.; Clark, C.; Miles, E.A.; Miah, A.B.; Newbold, K.; Tanay, M.; et al. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): A phase 3 multicentre randomised controlled trial. Lancet Oncol. 2011, 12, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Randall, K.; Stevens, J.; Yepes, J.F.; Randall, M.E.; Kudrimoti, M.; Feddock, J.; Xi, J.; Kryscio, R.J.; Miller, C.S. Analysis of factors influencing the development of xerostomia during intensity-modulated radiotherapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 772–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durkin, S.R.; Roos, D.; Higgs, B.; Casson, R.J.; Selva, D. Ophthalmic and adnexal complications of radiotherapy. Acta Ophthalmol. Scand. 2007, 85, 240–250. [Google Scholar] [CrossRef]
- Moore, H.D.; Ivey, R.G.; Voytovich, U.J.; Lin, C.; Stirewalt, D.L.; Pogosova-Agadjanyan, E.L.; Paulovich, A.G. The human salivary proteome is radiation responsive. Radiat. Res. 2014, 181, 521–530. [Google Scholar] [CrossRef] [Green Version]
- Westgaard, K.L.; Hynne, H.; Amdal, C.D.; Young, A.; Singh, P.B.; Chen, X.; Rykke, M.; Hove, L.H.; Aqrawi, L.A.; Utheim, T.P.; et al. Oral and ocular late effects in head and neck cancer patients treated with radiotherapy. Sci. Rep. 2021, 11, 4026. [Google Scholar] [CrossRef]
- Jonsson, R.; Bolstad, A.I.; Brokstad, K.A.; Brun, J.G. Sjogren’s syndrome--a plethora of clinical and immunological phenotypes with a complex genetic background. Ann. N. Y. Acad. Sci. 2007, 1108, 433–447. [Google Scholar] [CrossRef]
- Jonsson, R.; Vogelsang, P.; Volchenkov, R.; Espinosa, A.; Wahren-Herlenius, M.; Appel, S. The complexity of Sjogren’s syndrome: Novel aspects on pathogenesis. Immunol. Lett. 2011, 141, 1–9. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zeron, P.; Siso-Almirall, A.; Bosch, X.; Tzioufas, A.G. Topical and systemic medications for the treatment of primary Sjogren’s syndrome. Nat. Rev. Rheumatol. 2012, 8, 399–411. [Google Scholar] [CrossRef]
- Aqrawi, L.A.; Galtung, H.K.; Vestad, B.; Ovstebo, R.; Thiede, B.; Rusthen, S.; Young, A.; Guerreiro, E.M.; Utheim, T.P.; Chen, X.; et al. Identification of potential saliva and tear biomarkers in primary Sjogren’s syndrome, utilising the extraction of extracellular vesicles and proteomics analysis. Arthritis Res. 2017, 19, 14. [Google Scholar] [CrossRef] [Green Version]
- Roesch-Ely, M.; Nees, M.; Karsai, S.; Ruess, A.; Bogumil, R.; Warnken, U.; Schnolzer, M.; Dietz, A.; Plinkert, P.K.; Hofele, C.; et al. Proteomic analysis reveals successive aberrations in protein expression from healthy mucosa to invasive head and neck cancer. Oncogene 2007, 26, 54–64. [Google Scholar] [CrossRef] [Green Version]
- Jehmlich, N.; Stegmaier, P.; Golatowski, C.; Salazar, M.G.; Rischke, C.; Henke, M.; Volker, U. Differences in the whole saliva baseline proteome profile associated with development of oral mucositis in head and neck cancer patients undergoing radiotherapy. J. Proteom. 2015, 125, 98–103. [Google Scholar] [CrossRef]
- Jessie, K.; Jayapalan, J.J.; Ong, K.C.; Abdul Rahim, Z.H.; Zain, R.M.; Wong, K.T.; Hashim, O.H. Aberrant proteins in the saliva of patients with oral squamous cell carcinoma. Electrophoresis 2013, 34, 2495–2502. [Google Scholar] [CrossRef]
- Tung, C.L.; Lin, S.T.; Chou, H.C.; Chen, Y.W.; Lin, H.C.; Tung, C.L.; Huang, K.J.; Chen, Y.J.; Lee, Y.R.; Chan, H.L. Proteomics-based identification of plasma biomarkers in oral squamous cell carcinoma. J. Pharm. Biomed. Anal. 2013, 75, 7–17. [Google Scholar] [CrossRef]
- Laheij, A.M.; Rasch, C.N.; Brandt, B.W.; de Soet, J.J.; Schipper, R.G.; Loof, A.; Silletti, E.; van Loveren, C. Proteins and peptides in parotid saliva of irradiated patients compared to that of healthy controls using SELDI-TOF-MS. BMC Res. Notes 2015, 8, 639. [Google Scholar] [CrossRef] [Green Version]
- Guerra, E.N.; Rego, D.F.; Elias, S.T.; Coletta, R.D.; Mezzomo, L.A.; Gozal, D.; De Luca Canto, G. Diagnostic accuracy of serum biomarkers for head and neck cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 101, 93–118. [Google Scholar] [CrossRef]
- Aqrawi, L.A.; Galtung, H.K.; Guerreiro, E.M.; Ovstebo, R.; Thiede, B.; Utheim, T.P.; Chen, X.; Utheim, O.A.; Palm, O.; Skarstein, K.; et al. Proteomic and histopathological characterisation of sicca subjects and primary Sjogren’s syndrome patients reveals promising tear, saliva and extracellular vesicle disease biomarkers. Arthritis Res. 2019, 21, 181. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Aqrawi, L.A.; Utheim, T.P.; Tashbayev, B.; Utheim, Ø.A.; Reppe, S.; Hove, L.H.; Herlofson, B.B.; Singh, P.B.; Palm, Ø.; et al. Elevated cytokine levels in tears and saliva of patients with primary Sjögren’s syndrome correlate with clinical ocular and oral manifestations. Sci. Rep. 2019, 9, 7319. [Google Scholar] [CrossRef]
- Aqrawi, L.A.; Chen, X.; Hynne, H.; Amdal, C.; Reppe, S.; Aass, H.C.D.; Rykke, M.; Hove, L.H.; Young, A.; Herlofson, B.B.; et al. Cytokines Explored in Saliva and Tears from Radiated Cancer Patients Correlate with Clinical Manifestations, Influencing Important Immunoregulatory Cellular Pathways. Cells 2020, 9, 2050. [Google Scholar] [CrossRef]
- Eklund, K.K.; Niemi, K.; Kovanen, P.T. Immune functions of serum amyloid A. Crit. Rev. Immunol. 2012, 32, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, X.; Zhao, X.; Wang, J.; Xi, Q.; Hu, G. Study on the correlation of serum amyloid A level with overall survival and radiation pneumonitis in non-small cell lung cancer patients receiving thoracic radiotherapy. Precis. Radiat. Oncol. 2017, 1, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Wing, J.B.; Tanaka, A.; Sakaguchi, S. Human FOXP3+ Regulatory T Cell Heterogeneity and Function in Autoimmunity and Cancer. Immunity 2019, 50, 302–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knochelmann, H.M.; Dwyer, C.J.; Bailey, S.R.; Amaya, S.M.; Elston, D.M.; Mazza-McCrann, J.M.; Paulos, C.M. When worlds collide: Th17 and Treg cells in cancer and autoimmunity. Cell. Mol. Immunol. 2018, 15, 458–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Molodtsov, A.; Turk, M.J. Tissue Resident CD8 Memory T Cell Responses in Cancer and Autoimmunity. Front. Immunol. 2018, 9, 2810. [Google Scholar] [CrossRef] [PubMed]
- Tabrez, S.; Jabir, N.R.; Khan, M.I.; Khan, M.S.; Shakil, S.; Siddiqui, A.N.; Zaidi, S.K.; Ahmed, B.A.; Kamal, M.A. Association of autoimmunity and cancer: An emphasis on proteolytic enzymes. Semin. Cancer Biol. 2020, 64, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Zohar, Y.; Wildbaum, G.; Novak, R.; Salzman, A.L.; Thelen, M.; Alon, R.; Barsheshet, Y.; Karp, C.L.; Karin, N. CXCL11-dependent induction of FOXP3-negative regulatory T cells suppresses autoimmune encephalomyelitis. J. Clin. Investig. 2017, 127, 3913. [Google Scholar] [CrossRef] [Green Version]
- Shah, D.R.; Dholakia, S.; Shah, R.R. Effect of tyrosine kinase inhibitors on wound healing and tissue repair: Implications for surgery in cancer patients. Drug Saf. 2014, 37, 135–149. [Google Scholar] [CrossRef]
- Mozzati, M.; Gallesio, G.; Gassino, G.; Palomba, A.; Bergamasco, L. Can plasma rich in growth factors improve healing in patients who underwent radiotherapy for head and neck cancer? A split-mouth study. J. Craniofac. Surg. 2014, 25, 938–943. [Google Scholar] [CrossRef]
- Jensen, S.B.; Vissink, A.; Limesand, K.H.; Reyland, M.E. Salivary Gland Hypofunction and Xerostomia in Head and Neck Radiation Patients. J. Natl. Cancer Inst. Monogr. 2019, 2019, lgz016. [Google Scholar] [CrossRef]
- Sridharan, V.; Margalit, D.N.; Lynch, S.A.; Severgnini, M.; Zhou, J.; Chau, N.G.; Rabinowits, G.; Lorch, J.H.; Hammerman, P.S.; Hodi, F.S.; et al. Definitive chemoradiation alters the immunologic landscape and immune checkpoints in head and neck cancer. Br. J. Cancer 2016, 115, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Williamson, M.B.; Guschlbauer, W. Metabolism of nucleic acids during regeneration of wound tissue. J. Biol. Chem. 1961, 236, 1463–1466. [Google Scholar] [CrossRef]
- Biterge, B.; Schneider, R. Histone variants: Key players of chromatin. Cell Tissue Res. 2014, 356, 457–466. [Google Scholar] [CrossRef]
- Wang, T.; Chuffart, F.; Bourova-Flin, E.; Wang, J.; Mi, J.; Rousseaux, S.; Khochbin, S. Histone variants: Critical determinants in tumour heterogeneity. Front. Med. 2019, 13, 289–297. [Google Scholar] [CrossRef] [Green Version]
- Gould, T.J.; Lysov, Z.; Liaw, P.C. Extracellular DNA and histones: Double-edged swords in immunothrombosis. J. Thromb. Haemost. 2015, 13 (Suppl. S1), S82–S91. [Google Scholar] [CrossRef]
- Sollberger, G.; Streeck, R.; Apel, F.; Caffrey, B.E.; Skoultchi, A.I.; Zychlinsky, A. Linker histone H1.2 and H1.4 affect the neutrophil lineage determination. eLife 2020, 9, e52563. [Google Scholar] [CrossRef]
- Korpi, J.T.; Kervinen, V.; Mäklin, H.; Väänänen, A.; Lahtinen, M.; Läärä, E.; Ristimäki, A.; Thomas, G.; Ylipalosaari, M.; Aström, P.; et al. Collagenase-2 (matrix metalloproteinase-8) plays a protective role in tongue cancer. Br. J. Cancer 2008, 98, 766–775. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.H.; Starr, A.E.; Kappelhoff, R.; Yan, R.; Roberts, C.R.; Overall, C.M. Matrix metalloproteinase 8 deficiency in mice exacerbates inflammatory arthritis through delayed neutrophil apoptosis and reduced caspase 11 expression. Arthritis Rheum. 2010, 62, 3645–3655. [Google Scholar] [CrossRef]
- Konsta, O.; Thabet, Y.; Le Dantec, C.; Brooks, W.; Tzioufas, A.; Pers, J.-O.; Renaudineau, Y. The contribution of epigenetics in Sjögren’s Syndrome. Front. Genet. 2014, 5, 71. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, K.; Hiraishi, M.; Haneoka, M.; Fujinaka, H.; Yano, Y. Protease inhibitor concentrations in the saliva of individuals experiencing oral dryness. BMC Oral Health 2021, 21, 661. [Google Scholar] [CrossRef]
- Visvanathan, V.; Nix, P. Managing the patient presenting with xerostomia: A review. Int. J. Clin. Pract. 2010, 64, 404–407. [Google Scholar] [CrossRef]
- Xiao, H.; Fan, Y.; Li, Y.; Dong, J.; Zhang, S.; Wang, B.; Liu, J.; Liu, X.; Fan, S.; Guan, J.; et al. Oral microbiota transplantation fights against head and neck radiotherapy-induced oral mucositis in mice. Comput. Struct. Biotechnol. J. 2021, 19, 5898–5910. [Google Scholar] [CrossRef] [PubMed]
- Jazzar, A.A.; Shirlaw, P.J.; Carpenter, G.H.; Challacombe, S.J.; Proctor, G.B. Salivary S100A8/A9 in Sjögren’s syndrome accompanied by lymphoma. J. Oral Pathol. Med. 2018, 47, 900–906. [Google Scholar] [CrossRef] [Green Version]
- Lippens, S.; Kockx, M.; Knaapen, M.; Mortier, L.; Polakowska, R.; Verheyen, A.; Garmyn, M.; Zwijsen, A.; Formstecher, P.; Huylebroeck, D.; et al. Epidermal differentiation does not involve the pro-apoptotic executioner caspases, but is associated with caspase-14 induction and processing. Cell Death Differ. 2000, 7, 1218–1224. [Google Scholar] [CrossRef]
- Wu, M.; Kodani, I.; Dickinson, D.; Huff, F.; Ogbureke, K.U.; Qin, H.; Arun, S.; Dulebohn, R.; Al-Shabrawey, M.; Tawfik, A.; et al. Exogenous expression of caspase-14 induces tumor suppression in human salivary cancer cells by inhibiting tumor vascularization. Anticancer Res. 2009, 29, 3811–3818. [Google Scholar] [PubMed]
- Ni, Q.; Zhao, J.; Gao, Y.; Qin, D.; Chen, X.; Ainiwaer, X. Prediction of potential drugs and targets based on meibomian gland dysfunction module classification to guide individualized treatment. J. Cell. Biochem. 2019, 120, 14813–14821. [Google Scholar] [CrossRef]
- Chen, X.; Badian, R.A.; Hynne, H.; Amdal, C.D.; Herlofson, B.B.; Utheim, Ø.A.; Westgaard, K.L.; Fineide, F.; Jensen, J.L.; Utheim, T.P. Alterations in meibomian glands in patients treated with intensity-modulated radiotherapy for head and neck cancer. Sci. Rep. 2021, 11, 22419. [Google Scholar] [CrossRef] [PubMed]
- Gipson, I.K.; Spurr-Michaud, S.J.; Senchyna, M.; Ritter, R., 3rd; Schaumberg, D. Comparison of mucin levels at the ocular surface of postmenopausal women with and without a history of dry eye. Cornea 2011, 30, 1346–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widlak, P.; Jelonek, K.; Wojakowska, A.; Pietrowska, M.; Polanska, J.; Marczak, Ł.; Miszczyk, L.; Składowski, K. Serum Proteome Signature of Radiation Response: Upregulation of Inflammation-Related Factors and Downregulation of Apolipoproteins and Coagulation Factors in Cancer Patients Treated with Radiation Therapy—A Pilot Study. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 1108–1115. [Google Scholar] [CrossRef]
- Zewinger, S.; Reiser, J.; Jankowski, V.; Alansary, D.; Hahm, E.; Triem, S.; Klug, M.; Schunk, S.J.; Schmit, D.; Kramann, R.; et al. Apolipoprotein C3 induces inflammation and organ damage by alternative inflammasome activation. Nat. Immunol. 2020, 21, 30–41. [Google Scholar] [CrossRef]
- Robbesyn, F.; Augé, N.; Vindis, C.; Cantero, A.V.; Barbaras, R.; Negre-Salvayre, A.; Salvayre, R. High-density lipoproteins prevent the oxidized low-density lipoprotein-induced epidermal growth factor receptor activation and subsequent matrix metalloproteinase-2 upregulation. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1206–1212. [Google Scholar] [CrossRef] [Green Version]
- Dartt, D.A. Signal transduction and control of lacrimal gland protein secretion: A review. Curr. Eye Res. 1989, 8, 619–636. [Google Scholar] [CrossRef]
- Vitali, C.; Bombardieri, S.; Jonsson, R.; Moutsopoulos, H.M.; Alexander, E.L.; Carsons, S.E.; Daniels, T.E.; Fox, P.C.; Fox, R.I.; Kassan, S.S.; et al. Classification criteria for Sjögren’s syndrome: A revised version of the European criteria proposed by the American-European Consensus Group. Ann. Rheum. Dis. 2002, 61, 554–558. [Google Scholar] [CrossRef] [Green Version]
- Tashbayev, B.; Rusthen, S.; Young, A.; Herlofson, B.B.; Hove, L.H.; Singh, P.B.; Rykke, M.; Aqrawi, L.A.; Chen, X.; Utheim, O.A.; et al. Interdisciplinary, Comprehensive Oral and Ocular Evaluation of Patients with Primary Sjogren’s Syndrome. Sci. Rep. 2017, 7, 10761. [Google Scholar] [CrossRef]
- Fonseka, P.; Pathan, M.; Chitti, S.V.; Kang, T.; Mathivanan, S. FunRich enables enrichment analysis of OMICs datasets. J. Mol. Biol. 2021, 433, 166747. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protein Name | Gene | Comparison | Significance | Fold Change |
|---|---|---|---|---|
| Aldehyde dehydrogenase dimeric NADP-preferring | ALDH3A1 | HNC:C | 30.3 | 2.09 |
| Alpha-2-macroglobulin | A2M | HNC:pSS | 200 | 3.14 |
| Beta-2-microglobulin | B2M | pSS:C | 19.35 | 3.47 |
| BPI fold-containing family B member 2 | BPIFB2 | HNC:pSS | 92.23 | 2.76 |
| Brain acid soluble protein 1 | BASP1 | pSS:C | 17.82 | 3.61 |
| Calumenin | CALU | HNC:pSS | 101.61 | 2.37 |
| Caspase-14 | CASP14 | HNC:C HNC:pSS | 26.35 200 | 2.39 3.09 |
| Chitinase-3-like protein 2 | CHI3L2 | HNC:pSS | 200 | 3.32 |
| Desmoglein-1 | DSG1 | HNC:pSS | 86.71 | 2.10 |
| Galectin-3-binding protein | LGALS3BP | HNC:pSS | 89.19 | 2.42 |
| Gamma-glutamylcyclotransferase | GGCT | HNC:pSS | 58.86 | 3.10 |
| Glutathione S-transferase Mu 1 | GSTM1 | HNC:pSS | 25.14 | 8.39 |
| Glyceraldehyde-3-phosphate dehydrogenase | GAPDH | HNC:pSS | 92.68 | 2.42 |
| Histone H1.2 | H1-2 | HNC:C | 26.44 | 2.44 |
| Histone H1.3 | H1-3 | HNC:C | 22.01 | 2.16 |
| Histone H1.4 | H1-4 | HNC:C pSS:C | 33.38 27.94 | 2.77 2.14 |
| Histone H1.5 | H1-5 | HNC:C | 30.78 | 2.08 |
| Histone H4 | H4C1 | HNC:C HNC:pSS | 30.46 104.63 | 2.28 2.37 |
| Integrin alpha-M | ITGAM | HNC:pSS | 200 | 2.82 |
| Inter-alpha-trypsin inhibitor heavy chain H1 | ITIH1 | HNC:pSS | 25.79 | 2.54 |
| Kallikrein-1 | KLK1 | HNC:C | 17.74 | 2.01 |
| Kallikrein-6 | KLK6 | HNC:C | 26.49 | 2.03 |
| Neutrophil collagenase | MMP8 | HNC:C pSS:C | 13.65 19.19 | 2.52 2.08 |
| Olfactomedin-4 | OLFM4 | HNC:pSS | 27.69 | 2.25 |
| Perilipin-3 | PLIN3 | HNC:C | 16.47 | 2.82 |
| Proline-rich protein 4 | PRR4 | pSS:C | 57.75 | 6.40 |
| Proteasome subunit beta type-4 | PSMB4 | HNC:C | 14.06 | 2.20 |
| Protein S100-A6 | S100A6 | pSS:C | 21.56 | 2.67 |
| Protein S100-A7 | S100A7 | HNC:pSS | 29.11 | 3.25 |
| Protein S100-A8 | S100A8 | HNC:pSS | 200 | 3.27 |
| Protein S100-A9 | S100A9 | HNC:C HNC:pSS | 21.67 101.13 | 2.20 2.43 |
| Prothymosin alpha | PTMA | HNC:C | 46.53 | 2.40 |
| Serotransferrin | TF | HNC:pSS | 55.52 | 2.06 |
| Serpin B13 | SERPINB13 | HNC:pSS | 88.91 | 2.25 |
| Serum amyloid A-1 protein | SAA1 | HNC:C | 11.58 | 2.78 |
| SH3 domain-binding glutamic acid-rich-like protein 3 | SH3BGRL3 | HNC:pSS | 115.6 | 2.43 |
| Small proline-rich protein 3 | SPRR3 | HNC:pSS | 84.54 | 2.24 |
| Transcobalamin-1 | TCN1 | HNC:pSS | 106.55 | 2.47 |
| Translationally-controlled tumor protein | TPT1 | HNC:pSS | 112.35 | 2.60 |
| Vitamin D-binding protein | GC | HNC:pSS | 103.79 | 2.22 |
| Protein Name | Gene | Comparison | Significance | Fold Change |
|---|---|---|---|---|
| 40S ribosomal protein S6 | RPS6 | pSS:C | 11.96 | 0.15 |
| 60S acidic ribosomal protein P2 | RPLP2 | pSS:C | 13.74 | 0.39 |
| 60S ribosomal protein L4 | RPL4 | pSS:C | 18.81 | 0.06 |
| Alpha-amylase 1 | AMY1 | HNC:C | 26.68 | 0.21 |
| pSS:C | 20.27 | 0.15 | ||
| Annexin A1 | ANXA1 | HNC:pSS | 67.13 | 0.49 |
| Annexin A2 | ANXA2 | HNC:pSS | 105.7 | 0.39 |
| BPI fold-containing family B member 1 | BPIFB1 | pSS:C | 13.9 | 0.37 |
| Cadherin-1 | CDH1 | pSS:C | 13.69 | 0.39 |
| Calmodulin-like protein 5 | CALML5 | pSS:C | 20.17 | 0.49 |
| Calumenin | CALU | pSS:C | 10.92 | 0.43 |
| Carbonic anhydrase 1 | CA1 | HNC:C | 10.62 | 0.04 |
| pSS:C | 11.59 | 0.07 | ||
| Carboxypeptidase E | CPE | HNC:C | 25.26 | 0.40 |
| pSS:C | 27.13 | 0.17 | ||
| Cornulin | CRNN | HNC:C | 25.67 | 0.35 |
| pSS:C | 11.21 | 0.35 | ||
| Cystatin-B | CSTB | pSS:C | 24.08 | 0.38 |
| Cystatin-C | CST3 | pSS:C | 12.91 | 0.37 |
| Cystatin-D | CST5 | HNC:C | 27.49 | 0.38 |
| pSS:C | 20.87 | 0.32 | ||
| Cystatin-S | CST4 | HNC:C | 64.6 | 0.09 |
| pSS:C | 29.93 | 0.10 | ||
| Cystatin-SA | CST2 | pSS:C | 31.21 | 0.04 |
| HNC:C | 26.2 | 0.23 | ||
| Cystatin-SN | CST1 | HNC:C | 49.59 | 0.16 |
| pSS:C | 41.96 | 0.08 | ||
| Desmoplakin | DSP | pSS:C | 13.7 | 0.08 |
| EF-hand domain-containing protein D2 | EFHD2 | HNC:pSS | 22.24 | 0.37 |
| Extracellular glycoprotein lacritin | LACRT | HNC:pSS | 200 | 0.23 |
| Furin | FURIN | pSS:C | 29.1 | 0.30 |
| Galectin-7 | LGALS7 | HNC:C | 15.04 | 0.19 |
| Glutamate dehydrogenase 1 mitochondrial | GLUD1 | pSS:C | 14.06 | 0.43 |
| Golgi membrane protein 1 | GOLM1 | pSS:C | 21.08 | 0.37 |
| Hemoglobin subunit alpha | HBA1 | HNC:pSS | 200 | 0.29 |
| Hemoglobin subunit beta | HBB | HNC:pSS | 93.61 | 0.46 |
| Hemoglobin subunit delta | HBD | HNC:C | 11.6 | 0.03 |
| HNC:pSS | 26.64 | 0.39 | ||
| Heterogeneous nuclear ribonucleoprotein A1 | HNRNPA1 | pSS:C | 22.89 | 0.43 |
| Immunoglobulin alpha-2 heavy chain | N/A | pSS:C | 17.37 | 0.48 |
| Immunoglobulin heavy constant gamma 1 | IGHG1 | HNC:pSS | 78.3 | 0.46 |
| Immunoglobulin heavy constant gamma 2 | IGHG2 | HNC:C | 16.84 | 0.41 |
| Immunoglobulin heavy constant gamma 4 | IGHG4 | HNC:C | 31.52 | 0.22 |
| pSS:C | 12.46 | 0.36 | ||
| Involucrin | IVL | pSS:C | 12.97 | 0.26 |
| Junction plakoglobin | JUP | pSS:C | 14.57 | 0.06 |
| Lactotransferrin | LTF | pSS:C | 37.83 | 0.10 |
| Mammaglobin-B | SCGB2A1 | HNC:pSS | 200 | 0.31 |
| Mucin-5B | MUC5B | pSS:C | 13.84 | 0.35 |
| Multiple coagulation factor deficiency protein 2 | MCFD2 | HNC:C | 22.59 | 0.33 |
| Neuroblast differentiation-associated protein AHNAK | AHNAK | HNC:C | 14.22 | 0.04 |
| Peptidyl-glycine alpha-amidating monooxygenase | PAM | pSS:C | 18.26 | 0.14 |
| Peroxiredoxin-1 | PRDX1 | pSS:C | 12.08 | 0.43 |
| Prelamin-A/C | LMNA | pSS:C | 13.58 | 0.08 |
| Prolactin-inducible protein | PIP | HNC:C | 16.76 | 0.39 |
| pSS:C | 10.49 | 0.43 | ||
| Proline-rich protein 27 | PRR27 | HNC:C | 10.77 | 0.48 |
| Proline-rich protein 4 | PRR4 | HNC:pSS | 200 | 0.22 |
| Serpin B5 | SERPINB5 | pSS:C | 15.96 | 0.49 |
| Small proline-rich protein 3 | SPRR3 | pSS:C | 33.66 | 0.37 |
| Soluble calcium-activated nucleotidase 1 | CANT1 | HNC:C | 13.12 | 0.50 |
| Tubulin alpha-4A chain | TUBA4A | HNC:C | 16.01 | 0.09 |
| X-ray repair cross-complementing protein 6 | XRCC6 | HNC:C | 11.13 | 0.34 |
| Y-box-binding protein 3 | YBX3 | HNC:C | 11.48 | 0.43 |
| Comparison | Regulation | Enrichment Score | Enriched Term (Number) | Genes |
|---|---|---|---|---|
| HCN:C | up | 4.59 | Histones (5) | H1-2, H1-3, H1-4, H1-5, H4C9 |
| HCN:C | up | 3.22 | Proteases (5) | CASP14, KLK1, KLK6, MMP8, PSMB4 |
| HCN:C | down | 5.64 | Cystatins (4) | CST1, CST2, CST4, CST5 |
| pSS:C | down | 9.20 | Cystatins (6) | CST1, CST2, CST3, CST4, CST5, CSTB |
| Protein Name | Gene | Significance | Fold Change HNC:C |
|---|---|---|---|
| 28 kDa heat- and acid-stable phosphoprotein | PDAP1 | 24.19 | 2.90 |
| 40S ribosomal protein S21 | RPS21 | 49.76 | 2.24 |
| Alpha-1-acid glycoprotein 1 | ORM1 | 46.59 | 2.39 |
| Aminoacylase-1 | ACY1 | 12.23 | 3.42 |
| Apolipoprotein A-I | APOA1 | 54.4 | 2.34 |
| Apolipoprotein C-III | APOC3 | 36.22 | 2.53 |
| Apolipoprotein E | APOE | 25.12 | 2.21 |
| Beta-2-glycoprotein 1 | APOH | 41.01 | 3.33 |
| Complement factor I | CFI | 27.1 | 2.27 |
| Fibrinogen gamma chain | FGG | 104.54 | 2.18 |
| Haptoglobin | HP | 59.74 | 2.01 |
| Heterogeneous nuclear ribonucleoprotein U | HNRNPU | 79.08 | 3.80 |
| Histone H2B type 1-H | HIST1H2BH | 46.89 | 2.66 |
| Immunoglobulin gamma-1 heavy chain | IGHG1 | 81.74 | 2.67 |
| Immunoglobulin heavy constant gamma 3 | IGHG3 | 73.67 | 2.77 |
| Mucin-like protein 1 | MUCL1 | 31.53 | 5.47 |
| Protein ERGIC-53 | LMAN1 | 22.49 | 2.55 |
| Selenoprotein P | SELENOP | 33.11 | 2.84 |
| Vitronectin | VTN | 66.06 | 2.28 |
| Protein Name | Gene | Significance | Fold Change |
|---|---|---|---|
| 45 kDa calcium-binding protein | SDF4 | 62.15 | 0.36 |
| Acidic leucine-rich nuclear phosphoprotein 32 family member B | ANP32B | 13.01 | 0.44 |
| Actin-related protein 2/3 complex subunit 3 | ARPC3 | 41.68 | 0.39 |
| All-trans-retinol dehydrogenase [NAD(+)] ADH1B | ADH1B | 23.19 | 0.5 |
| Alpha-1-acid glycoprotein 2 | ORM2 | 19.26 | 0.26 |
| Annexin A3 | ANXA3 | 19.31 | 0.26 |
| Annexin A6 | ANXA6 | 13.92 | 0.44 |
| Antithrombin-III | SERPINC1 | 14.47 | 0.44 |
| Arginase-1 | ARG1 | 17.3 | 0.14 |
| Barrier-to-autointegration factor | BANF1 | 12.13 | 0.44 |
| Basement membrane-specific heparan sulfate proteoglycan core protein | HSPG2 | 33.77 | 0.32 |
| Beta-2-microglobulin | B2M | 34.45 | 0.29 |
| Bloom syndrome protein | BLM | 27.56 | 0.24 |
| Catalase | CAT | 15.55 | 0.18 |
| Cathelicidin antimicrobial peptide | CAMP | 24.11 | 0.04 |
| Chitinase-3-like protein 2 | CHI3L2 | 55.28 | 0.35 |
| Clusterin | CLU | 84.78 | 0.42 |
| Cystatin-C | CST3 | 44.94 | 0.48 |
| Deleted in malignant brain tumors 1 protein | DMBT1 | 17.29 | 0.42 |
| DNA damage-binding protein 1 | DDB1 | 90.01 | 0.49 |
| DnaJ homolog subfamily C member 3 | DNAJC3 | 46.44 | 0.39 |
| EH domain-containing protein 1 | EHD1 | 20 | 0.17 |
| Extracellular glycoprotein lacritin | LACRT | 45.83 | 0.42 |
| Fructose-bisphosphate aldolase C | ALDOC | 118.69 | 0.38 |
| Galectin-3-binding protein | LGALS3BP | 76.28 | 0.36 |
| Galectin-7 | LGALS7 | 54.61 | 0.18 |
| Glucosidase 2 subunit beta | PRKCSH | 103.78 | 0.48 |
| Glutaredoxin-1 | GLRX | 97.34 | 0.48 |
| GMP reductase 2 | GMPR2 | 51.85 | 0.33 |
| Golgi membrane protein 1 | GOLM1 | 28.43 | 0.49 |
| Heme-binding protein 1 | HEBP1 | 69.87 | 0.49 |
| Hepatoma-derived growth factor | HDGF | 26.23 | 0.46 |
| Immunoglobulin alpha-2 heavy chain | N/A | 34.06 | 0.35 |
| Immunoglobulin kappa constant | IGKC | 74.47 | 0.45 |
| Immunoglobulin kappa light chain | N/A | 34.97 | 0.34 |
| Immunoglobulin kappa variable 2-24 | IGKV2-24 | 51.08 | 0.36 |
| Lactotransferrin | LTF | 10.37 | 0.32 |
| Lamina-associated polypeptide 2 isoform alpha | TMPO | 18.11 | 0.44 |
| Lipocalin-1 | LCN1 | 24.74 | 0.48 |
| Lymphocyte-specific protein 1 | LSP1 | 10.97 | 0.27 |
| Macrophage migration inhibitory factor | MIF | 75.87 | 0.39 |
| Mesothelin | MSLN | 10.08 | 0.48 |
| Metalloproteinase inhibitor 1 | TIMP1 | 51.11 | 0.46 |
| Methanethiol oxidase | SELENBP1 | 200 | 0.47 |
| Monocyte differentiation antigen CD14 | CD14 | 35.97 | 0.32 |
| Mucin-4 | MUC4 | 24.6 | 0.2 |
| Multiple coagulation factor deficiency protein 2 | MCFD2 | 23.01 | 0.47 |
| Myeloperoxidase | MPO | 27.16 | 0.27 |
| Neutral alpha-glucosidase AB | GANAB | 126.44 | 0.43 |
| Nuclear transport factor 2 | NUTF2 | 43.48 | 0.38 |
| Nucleobindin-1 | NUCB1 | 89.2 | 0.38 |
| Nucleobindin-2 | NUCB2 | 44.99 | 0.42 |
| Opiorphin prepropeptide | OPRPN | 36.14 | 0.37 |
| Peptidyl-prolyl cis-trans isomerase B | PPIB | 44.3 | 0.47 |
| Phosphatidylethanolamine-binding protein 4 | PEBP4 | 38.46 | 0.2 |
| Phospholipid transfer protein | PLTP | 44.98 | 0.4 |
| Phosphopantothenate--cysteine ligase | PPCS | 50.18 | 0.4 |
| Prosaposin | PSAP | 56.15 | 0.32 |
| Protein CutA | CUTA | 104.42 | 0.47 |
| Ras-related protein Rab-10 | RAB10 | 22.09 | 0.5 |
| Reticulocalbin-1 | RCN1 | 58.89 | 0.43 |
| Retinoic acid receptor responder protein 1 | RARRES1 | 77.82 | 0.35 |
| Secreted frizzled-related protein 1 | SFRP1 | 25.9 | 0.19 |
| Secretoglobin family 1D member 1 | SCGB1D1 | 45.53 | 0.39 |
| Septin-2 | SEPTIN2 | 27.53 | 0.29 |
| Superoxide dismutase [Cu-Zn] | SOD1 | 200 | 0.19 |
| Syntaxin-7 | STX7 | 91.29 | 0.46 |
| Thymosin beta-4 | TMSB4X | 52.28 | 0.47 |
| Transcobalamin-1 | TCN1 | 47.57 | 0.38 |
| Translin | TSN | 45.01 | 0.48 |
| Vimentin | VIM | 11.23 | 0.39 |
| Zinc-alpha-2-glycoprotein | AZGP1 | 75.58 | 0.4 |
| Zymogen granule protein 16 homolog B | ZG16B | 35.01 | 0.31 |
| Comparison | Regulation | Enrichment Score | Enriched Term (Number) | Genes |
|---|---|---|---|---|
| HCN:C | down | 3.66 | EF-hand domain (7) | EHD1, MCFD2, NUCB1, NUCB2, PRKCSH, RCN1, SDF4 |
| HCN:C | up | 6.72 | Secreted/ extracellular (12) | APOA1, APOC3, APOE, APOH, CFI, FGG, HP, IGHG3, MUCL1, ORM1, SELENOP, VTN |
| HCN:C | up | 5.13 | Lipid-binding (4) | APOA1, APOC3, APOE, APOH |
| Patient No. | Age | Sex | Type of Radiotherapy Treatment | Total Radiation Dose (Gy) | Chemotherapy |
|---|---|---|---|---|---|
| 1 | 54 | M | Primary | 68 | + |
| 2 | 75 | M | Primary | 68 | − |
| 3 | 63 | F | Primary | 70 | + |
| 4 | 82 | F | Primary | 68 | − |
| 5 | 61 | M | Primary | 68 | + |
| 6 | 70 | M | Primary | 68 | + |
| 7 | 69 | F | Primary | 68 | − |
| 8 | 58 | M | Primary | 68 | + |
| 9 | 67 | M | Primary | 68 | + |
| 10 | 59 | M | Primary | 68 | − |
| 11 | 53 | M | Primary | 68 | + |
| 12 | 64 | M | Primary | 68 | + |
| 13 | 57 | M | Primary | 68 | + |
| 14 | 68 | M | Primary | 68 | + |
| 15 | 73 | M | Postoperative | 56 | − |
| 16 | 66 | F | Postoperative | 66 | − |
| 17 | 65 | F | Postoperative | 60 | − |
| 18 | 73 | F | Postoperative | 66 | − |
| 19 | 71 | F | Postoperative | 60 | − |
| 20 | 66 | F | Postoperative | 66 | − |
| 21 | 51 | F | Postoperative | 66 | − |
| 22 | 58 | M | Postoperative | 60 | − |
| 23 | 41 | F | Postoperative | 60 | + |
| 24 | 82 | M | Postoperative | 60 | − |
| 25 | 51 | F | Postoperative | 60 | + |
| 26 | 65 | F | Postoperative | 66 | − |
| 27 | 58 | M | Postoperative | 60 | − |
| 28 | 60 | F | Postoperative | 50 | − |
| 29 | 82 | M | Postoperative | 60 | − |
| Patient No. | Age | Sex | Anti- SSA * | Anti- SSB * | Focus Score ** | Schirmer Test *** | Saliva Secretion **** | Dry Mouth | Dry Eyes |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 64 | F | + | − | NT | − | + | + | + |
| 2 | 68 | F | + | + | 1 | + | + | + | + |
| 3 | 72 | F | + | + | NT | NT | + | + | + |
| 4 | 71 | F | + | − | NT | + | − | + | + |
| 5 | 57 | F | + | + | NT | + | + | + | + |
| 6 | 57 | F | + | − | 0 | + | + | − | + |
| 7 | 73 | F | + | − | <1 | + | + | + | + |
| 8 | 65 | F | + | − | <1 | + | + | + | + |
| 9 | 56 | F | + | − | 1 | + | + | + | + |
| 10 | 68 | F | + | + | NT | − | + | + | + |
| 11 | 75 | F | + | + | NT | + | − | + | + |
| 12 | 50 | F | + | + | NT | NT | + | + | + |
| 13 | 60 | F | + | + | 2 | + | − | + | − |
| 14 | 51 | F | + | − | 8 | + | − | − | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hynne, H.; Aqrawi, L.A.; Jensen, J.L.; Thiede, B.; Palm, Ø.; Amdal, C.D.; Westgaard, K.L.; Herlofson, B.B.; Utheim, T.P.; Galtung, H.K. Proteomic Profiling of Saliva and Tears in Radiated Head and Neck Cancer Patients as Compared to Primary Sjögren’s Syndrome Patients. Int. J. Mol. Sci. 2022, 23, 3714. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23073714
Hynne H, Aqrawi LA, Jensen JL, Thiede B, Palm Ø, Amdal CD, Westgaard KL, Herlofson BB, Utheim TP, Galtung HK. Proteomic Profiling of Saliva and Tears in Radiated Head and Neck Cancer Patients as Compared to Primary Sjögren’s Syndrome Patients. International Journal of Molecular Sciences. 2022; 23(7):3714. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23073714
Chicago/Turabian StyleHynne, Håvard, Lara A. Aqrawi, Janicke Liaaen Jensen, Bernd Thiede, Øyvind Palm, Cecilie Delphin Amdal, Kristine Løken Westgaard, Bente Brokstad Herlofson, Tor P. Utheim, and Hilde Kanli Galtung. 2022. "Proteomic Profiling of Saliva and Tears in Radiated Head and Neck Cancer Patients as Compared to Primary Sjögren’s Syndrome Patients" International Journal of Molecular Sciences 23, no. 7: 3714. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23073714