
AcidoCEST-UTE MRI Reveals an Acidic Microenvironment in Knee Osteoarthritis
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Participants, Demographics, and KOOS Score Comparisons among Groups
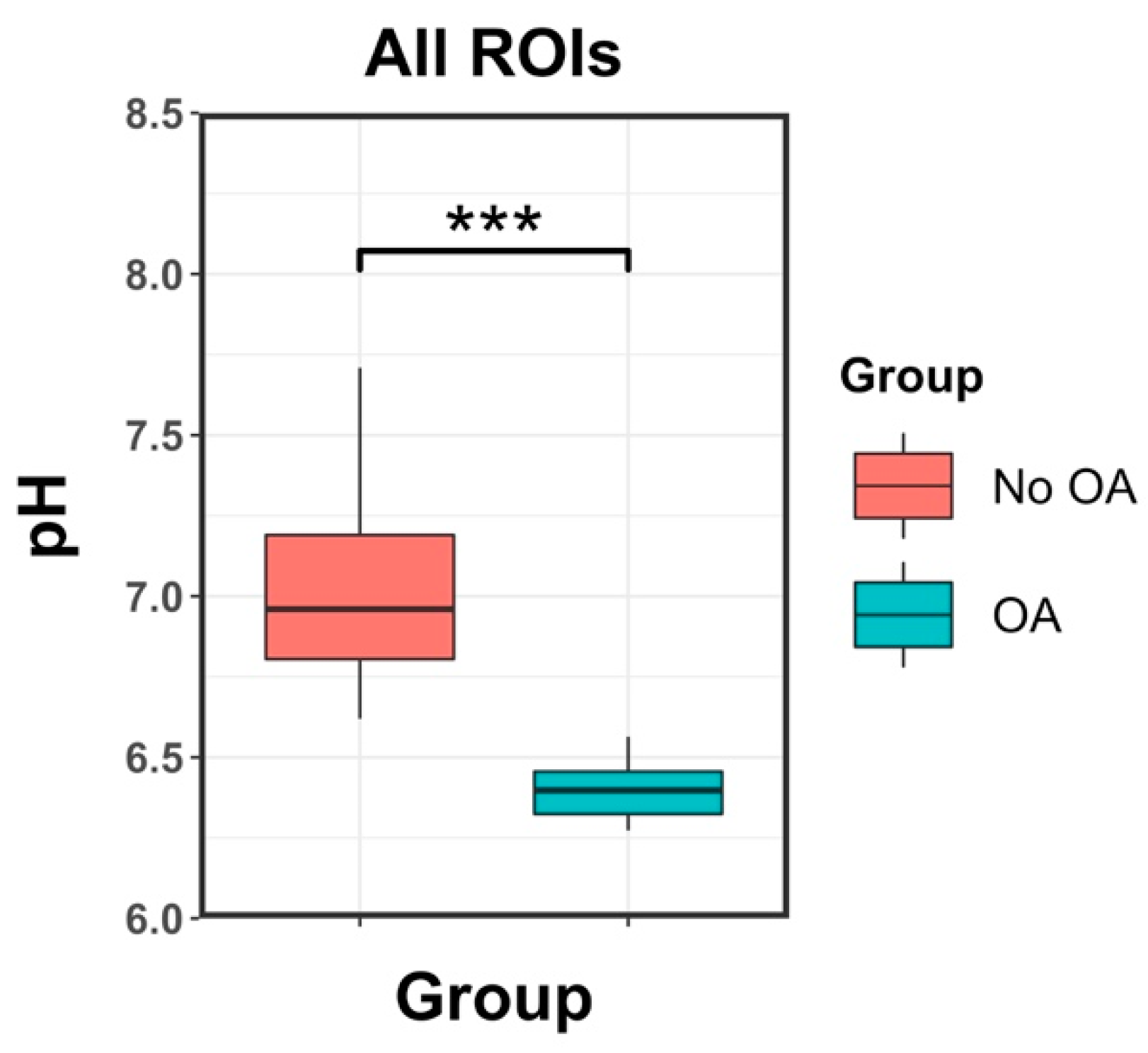
2.2. pH Measurements
2.3. Correlations between the pH Measurements and the KOOS Score
3. Discussion
4. Materials and Methods
4.1. Volunteers and Patients
4.2. Imaging with Acidocest-UTE MRI
4.3. Data Processing and pH Calculations
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Kiadaliri, A.; Englund, M. Trajectory of excess healthcare consultations, medication use, and work disability in newly diagnosed knee osteoarthritis: A matched longitudinal register-based study. Osteoarthr. Cartil. 2021, 29, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Wang, D.; Zhang, H.; Liang, J.; Feng, X.; Zhao, J.; Sun, L. Incidence trend of five common musculoskeletal disorders from 1990 to 2017 at the global, regional and national level: Results from the global burden of disease study 2017. Ann. Rheum. Dis. 2020, 79, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Quicke, J.G.; Conaghan, P.G.; Corp, N.; Peat, G. Osteoarthritis year in review 2021: Epidemiology & therapy. Osteoarthr. Cartil. 2022, 30, 196–206. [Google Scholar]
- Eckstein, F.; Peterfy, C. A 20 years of progress and future of quantitative magnetic resonance imaging (qMRI) of cartilage and articular tissues-personal perspective. Semin. Arthritis Rheum. 2016, 45, 639–647. [Google Scholar] [CrossRef]
- Roemer, F.W.; Demehri, S.; Omoumi, P.; Link, T.M.; Kijowski, R.; Saarakkala, S.; Crema, M.D.; Guermazi, A. State of the Art: Imaging of Osteoarthritis-Revisited 2020. Radiology 2020, 296, 5–21. [Google Scholar] [CrossRef]
- Kogan, F.; Fan, A.P.; Monu, U.; Iagaru, A.; Hargreaves, B.A.; Gold, G.E. Quantitative imaging of bone-cartilage interactions in ACL-injured patients with PET-MRI. Osteoarthr. Cartil. 2018, 26, 790–796. [Google Scholar] [CrossRef]
- Zarringam, D.; Saris, D.B.F.; Bekkers, J.E.J. The Value of SPECT/CT for Knee Osteoarthritis: A Systematic Review. Cartilage 2021, 12, 431–437. [Google Scholar] [CrossRef]
- Colotti, R.; Omoumi, P.; Bonanno, G.; Ledoux, J.B.; van Heeswijk, R.B. Isotropic three-dimensional T(2) mapping of knee cartilage: Development and validation. J. Magn. Reson. Imaging 2018, 47, 362–371. [Google Scholar] [CrossRef]
- Gallo, M.C.; Wyatt, C.; Pedoia, V.; Kumar, D.; Lee, S.; Nardo, L.; Link, T.M.; Souza, R.B.; Majumdar, S. T1ρ and T2 relaxation times are associated with progression of hip osteoarthritis. Osteoarthr. Cartil. 2016, 24, 1399–1407. [Google Scholar] [CrossRef]
- Schmitt, B.; Zbýn, S.; Stelzeneder, D.; Jellus, V.; Paul, D.; Lauer, L.; Bachert, P.; Trattnig, S. Cartilage quality assessment by using glycosaminoglycan chemical exchange saturation transfer and (23)Na MR imaging at 7 T. Radiology 2011, 260, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Brinkhof, S.; Nizak, R.; Khlebnikov, V.; Prompers, J.J.; Klomp, D.W.J.; Saris, D.B.F. Detection of early cartilage damage: Feasibility and potential of gagCEST imaging at 7T. Eur. Radiol. 2018, 28, 2874–2881. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.Q.; Howison, C.M.; Jeffery, J.J.; Robey, I.F.; Kuo, P.H.; Pagel, M.D. Evaluations of extracellular pH within in vivo tumors using acidoCEST MRI. Magn. Reson. Med. 2014, 72, 1408–1417. [Google Scholar] [CrossRef]
- Konttinen, Y.T.; Mandelin, J.; Li, T.F.; Salo, J.; Lassus, J.; Liljestrom, M.; Hukkanen, M.; Takagi, M.; Virtanen, I.; Santavirta, S. Acidic cysteine endoproteinase cathepsin K in the degeneration of the superficial articular hyaline cartilage in osteoarthritis. Arthritis Rheum. 2002, 46, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Deval, E.; Noël, J.; Lay, N.; Alloui, A.; Diochot, S.; Friend, V.; Jodar, M.; Lazdunski, M.; Lingueglia, E. ASIC3, a sensor of acidic and primary inflammatory pain. EMBO J. 2008, 27, 3047–3055. [Google Scholar] [CrossRef] [PubMed]
- Izumi, M.; Ikeuchi, M.; Ji, Q.; Tani, T. Local ASIC3 modulates pain and disease progression in a rat model of osteoarthritis. J. Biomed. Sci. 2012, 19, 77. [Google Scholar] [CrossRef] [PubMed]
- Walsh, D.A.; McWilliams, D.F.; Turley, M.J.; Dixon, M.R.; Franses, R.E.; Mapp, P.I.; Wilson, D. Angiogenesis and nerve growth factor at the osteochondral junction in rheumatoid arthritis and osteoarthritis. Rheumatology 2010, 49, 1852–1861. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.Y.; Du, J.; Chung, C.B. UTE imaging in the musculoskeletal system. J. Magn. Reson. Imaging 2015, 41, 870–883. [Google Scholar] [CrossRef]
- Lombardi, A.F.; Jang, H.; Wei, Z.; Jerban, S.; Wallace, M.; Masuda, K.; Ma, Y.J. High-contrast osteochondral junction imaging using a 3D dual adiabatic inversion recovery-prepared ultrashort echo time cones sequence. NMR Biomed. 2021, 34, e4559. [Google Scholar] [CrossRef]
- Ma, Y.; Jerban, S.; Carl, M.; Wan, L.; Gou, T.; Jang, H.; Bydder, G.M.; Chang, E.Y.; Du, J. Imaging of the region of the osteochondral junction (OCJ) using a 3D adiabatic inversion recovery prepared ultrashort echo time cones (3D IR UTe cones) sequence at 3 T. NMR Biomed. 2019, 32, e4080. [Google Scholar] [CrossRef]
- Recht, M.P.; Zbontar, J.; Sodickson, D.K.; Knoll, F.; Yakubova, N.; Sriram, A.; Murrell, T.; Defazio, A.; Rabbat, M.; Rybak, L.; et al. Using Deep Learning to Accelerate Knee MRI at 3 T: Results of an Interchangeability Study. Am. J. Roentgenol. 2020, 215, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.J.; High, R.A.; Tang, Q.; Wan, L.; Jerban, S.; Du, J.; Chang, E.Y. AcidoCEST-UTE MRI for the Assessment of Extracellular pH of Joint Tissues at 3 T. Investig. Radiol. 2019, 54, 565–571. [Google Scholar] [CrossRef] [PubMed]
- High, R.A.; Ji, Y.; Ma, Y.J.; Tang, Q.; Murphy, M.E.; Du, J.; Chang, E.Y. In vivo assessment of extracellular pH of joint tissues using acidoCEST-UTE MRI. Quant. Imaging Med. Surg. 2019, 9, 1664–1673. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Andreisek, G.; Weiger, M. T2* mapping of articular cartilage: Current status of research and first clinical applications. Invest. Radiol. 2014, 49, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Haris, M.; Cai, K.; Kogan, F.; Hariharan, H.; Reddy, R. High resolution T1ρ mapping of in vivo human knee cartilage at 7T. PLoS ONE 2014, 9, e97486. [Google Scholar] [CrossRef] [PubMed]
- Soellner, S.T.; Welsch, G.H.; Gelse, K.; Goldmann, A.; Kleyer, A.; Schett, G.; Pachowsky, M.L. gagCEST imaging at 3 T MRI in patients with articular cartilage lesions of the knee and intraoperative validation. Osteoarthr. Cartil. 2021, 29, 1163–1172. [Google Scholar] [CrossRef]
- Brinkhof, S.; Nizak, R.; Sim, S.; Khlebnikov, V.; Quenneville, E.; Garon, M.; Klomp, D.W.J.; Saris, D. In vivo biochemical assessment of cartilage with gagCEST MRI: Correlation with cartilage properties. NMR Biomed. 2021, 34, e4463. [Google Scholar] [CrossRef]
- Abrar, D.B.; Schleich, C.; Radke, K.L.; Frenken, M.; Stabinska, J.; Ljimani, A.; Wittsack, H.-J.; Antoch, G.; Bittersohl, B.; Hesper, T.; et al. Detection of early cartilage degeneration in the tibiotalar joint using 3 T gagCEST imaging: A feasibility study. Magn. Reson. Mater. Phys. Biol. Med. 2021, 34, 249–260. [Google Scholar] [CrossRef]
- Emanuel, K.S.; Kellner, L.J.; Peters, M.J.M.; Haartmans, M.J.J.; Hooijmans, M.T.; Emans, P.J. The relation between the biochemical composition of knee articular cartilage and quantitative MRI: A systematic review and meta-analysis. Osteoarthr. Cartil. 2021. [Google Scholar] [CrossRef]
- Owman, H.; Ericsson, Y.B.; Englund, M.; Tiderius, C.J.; Tjornstrand, J.; Roos, E.M.; Dahlberg, L.E. Association between delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) and joint space narrowing and osteophytes: A cohort study in patients with partial meniscectomy with 11 years of follow-up. Osteoarthr. Cartil. 2014, 22, 1537–1541. [Google Scholar] [CrossRef] [PubMed]
- Queney, M.S.; Amegadzie, B.Y.; D’Alessio, K.; Hanning, C.R.; Laughlin, M.M.; Nulty, D.; Carr, S.A.; Ljames, C.; Kurdyla, J.; Jones, C.S.; et al. Autocatalytic activation of human cathepsin K. J. Biol. Chem. 1997, 272, 13955–13960. [Google Scholar]
- KAFIENAH, W.E.; BRÖMME, D.; BUTTLE, D.J.; CROUCHER, L.J.; HOLLANDER, A.P. Human cathepsin K cleaves native type I and II collagens at the N-terminal end of the triple helix. Biochem. J. 1998, 331, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Barrett, A.J.; Woessner, J.F.; Rawlings, N.D. Handbook of Proteolytic Enzymes; Elsevier: Amsterdam, The Netherlands, 2012; Volume 1. [Google Scholar]
- Ikeuchi, M.; Kolker, S.J.; Sluka, K.A. Acid-sensing ion channel 3 expression in mouse knee joint afferents and effects of carrageenan-induced arthritis. J. Pain 2009, 10, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Ren, G.; Zhou, R.; Ge, J.; Chen, F.-H. The role of Ca 2+ in acid-sensing ion channel 1a-mediated chondrocyte pyroptosis in rat adjuvant arthritis. Lab. Investig. 2019, 99, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Su, J.-W.; Li, S.-F.; Tao, J.-J.; Xu, Y.-Y.; Wang, K.; Qian, X.-W.; Deng, G.; Peng, X.-Q.; Chen, F.-H. Estrogen protects against acidosis-mediated articular chondrocyte injury by promoting ASIC1a protein degradation. Eur. J. Pharmacol. 2021, 908, 174381. [Google Scholar] [CrossRef]
- Jones, K.M.; Randtke, E.A.; Yoshimaru, E.S.; Howison, C.M.; Chalasani, P.; Klein, R.R.; Chambers, S.K.; Kou, P.H.; Pagel, M.D. Clinical translation of tumor acidosis measurements with AcidoCEST MRI. Mol. Imaging Biol. 2017, 19, 617–625. [Google Scholar] [CrossRef]
- Lombardi, A.F.; Wong, J.H.; High, R.; Ma, Y.; Jerban, S.; Tang, Q.; Du, J.; Frost, P.; Pagel, M.D.; Chang, E.Y. AcidoCEST MRI Evaluates the Bone Microenvironment in Multiple Myeloma. Mol. Imaging Biol. 2021, 23, 865–873. [Google Scholar] [CrossRef]
- Schieker, M.; Conaghan, P.G.; Mindeholm, L.; Praestgaard, J.; Solomon, D.H.; Scotti, C.; Gram, H.; Thuren, T.; Roubenoff, R.; Ridker, P.M. Effects of interleukin-1β inhibition on incident hip and knee replacement: Exploratory analyses from a randomized, double-blind, placebo-controlled trial. Ann. Intern. Med. 2020, 173, 509–515. [Google Scholar] [CrossRef]
- Kim, S.H.; Djaja, Y.P.; Park, Y.-B.; Park, J.-G.; Ko, Y.-B.; Ha, C.-W. Intra-articular injection of culture-expanded mesenchymal stem cells without adjuvant surgery in knee osteoarthritis: A systematic review and meta-analysis. Am. J. Sports Med. 2020, 48, 2839–2849. [Google Scholar] [CrossRef]
- Szwedowski, D.; Szczepanek, J.; Paczesny, Ł.; Zabrzynski, J.; Gagat, M.; Mobasheri, A.; Jeka, S. The Effect of Platelet-Rich Plasma on the Intra-Articular Microenvironment in Knee Osteoarthritis. Int. J. Mol. Sci. 2021, 22, 5492. [Google Scholar] [CrossRef] [PubMed]
- Jebens, E.H.; Monk-Jones, M.E. On the viscosity and pH of synovial fluid and the pH of blood. J. Bone Jt. Surg. Br. 1959, 41-b, 388–400. [Google Scholar] [CrossRef]
- Cummings, N.A.; Nordby, G.L. Measurement of synovial fluid pH in normal and arthritic knees. Arthritis Rheum. 1966, 9, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Farr, M.; Garvey, K.; Bold, A.M.; Kendall, M.J.; Bacon, P.A. Significance of the hydrogen ion concentration in synovial fluid in rheumatoid arthritis. Clin. Exp. Rheumatol. 1985, 3, 99–104. [Google Scholar] [PubMed]
- Zu, Z.; Li, K.; Janve, V.A.; Does, M.D.; Gochberg, D.F. Optimizing pulsed-chemical exchange saturation transfer imaging sequences. Magn. Reson. Med. 2011, 66, 1100–1108. [Google Scholar] [CrossRef]
- Klein, S.; Staring, M.; Murphy, K.; Viergever, M.A.; Pluim, J.P.W. elastix: A Toolbox for Intensity-Based Medical Image Registration. IEEE Trans. Med. Imaging 2010, 29, 196–205. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical. Computing, Vienna, Austria URL. 2014. Available online: http://wwwR-projectorg/ (accessed on 15 February 2022).
- RStudio Team. RStudio: Integrated Development for R. RStudio, PBC, Boston, MA URL. 2020. Available online: http://wwwrstudiocom/ (accessed on 15 February 2022).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Participants | No OA | OA | p Value *** |
|---|---|---|---|---|
| Number of participants | 16 | 9 | 7 | |
| Age (years) * | 57 ± 13 | 48 ± 16 | 65 ± 8 | 0.01 |
| Sex ** | ||||
| M | 15 (93.7) | 9 (100) | 6 (85.7) | |
| F | 1 (0.06) | 0 (0) | 1 (14.2) | |
| KOOS * | ||||
| KOOS pain | 60 ± 19 | 79 ± 21 | 36 ± 19 | <0.001 |
| KOOS symptoms | 41 ± 20 | 77 ± 18 | 41 ± 20 | <0.001 |
| KOOS ADL | 46 ± 24 | 78 ± 19 | 46 ± 24 | <0.001 |
| KOOS sports/rec | 24 ± 25 | 66 ± 29 | 24 ± 25 | <0.001 |
| KOOS QOL | 19 ± 15 | 72 ± 28 | 19 ± 15 | <0.001 |
| KOOS PF | 50 ± 34 | 67 ± 17 | 27 ± 23 | <0.001 |
| VAPS | 4 ± 3 | 0.9 ± 0.8 | 6.8 ± 1.8 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardi, A.F.; Ma, Y.; Jang, H.; Jerban, S.; Tang, Q.; Searleman, A.C.; Meyer, R.S.; Du, J.; Chang, E.Y. AcidoCEST-UTE MRI Reveals an Acidic Microenvironment in Knee Osteoarthritis. Int. J. Mol. Sci. 2022, 23, 4466. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23084466
Lombardi AF, Ma Y, Jang H, Jerban S, Tang Q, Searleman AC, Meyer RS, Du J, Chang EY. AcidoCEST-UTE MRI Reveals an Acidic Microenvironment in Knee Osteoarthritis. International Journal of Molecular Sciences. 2022; 23(8):4466. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23084466
Chicago/Turabian StyleLombardi, Alecio F., Yajun Ma, Hyungseok Jang, Saeed Jerban, Qingbo Tang, Adam C. Searleman, Robert Scott Meyer, Jiang Du, and Eric Y. Chang. 2022. "AcidoCEST-UTE MRI Reveals an Acidic Microenvironment in Knee Osteoarthritis" International Journal of Molecular Sciences 23, no. 8: 4466. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23084466