
Tumor Infiltration with CD20+CD73+ B Cells Correlates with Better Outcome in Colorectal Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
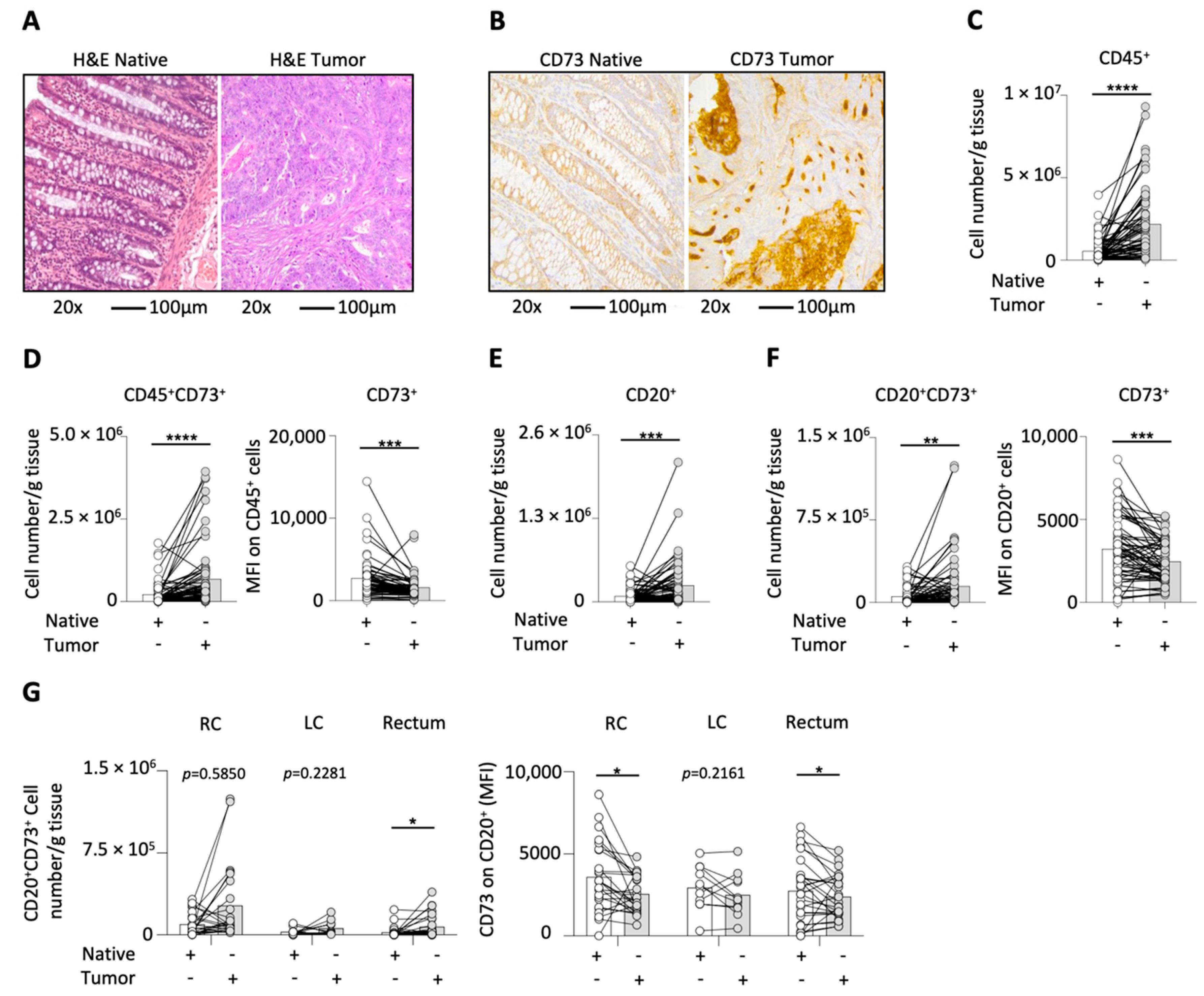
2.1. CD73 on Different Cell Types in CRC
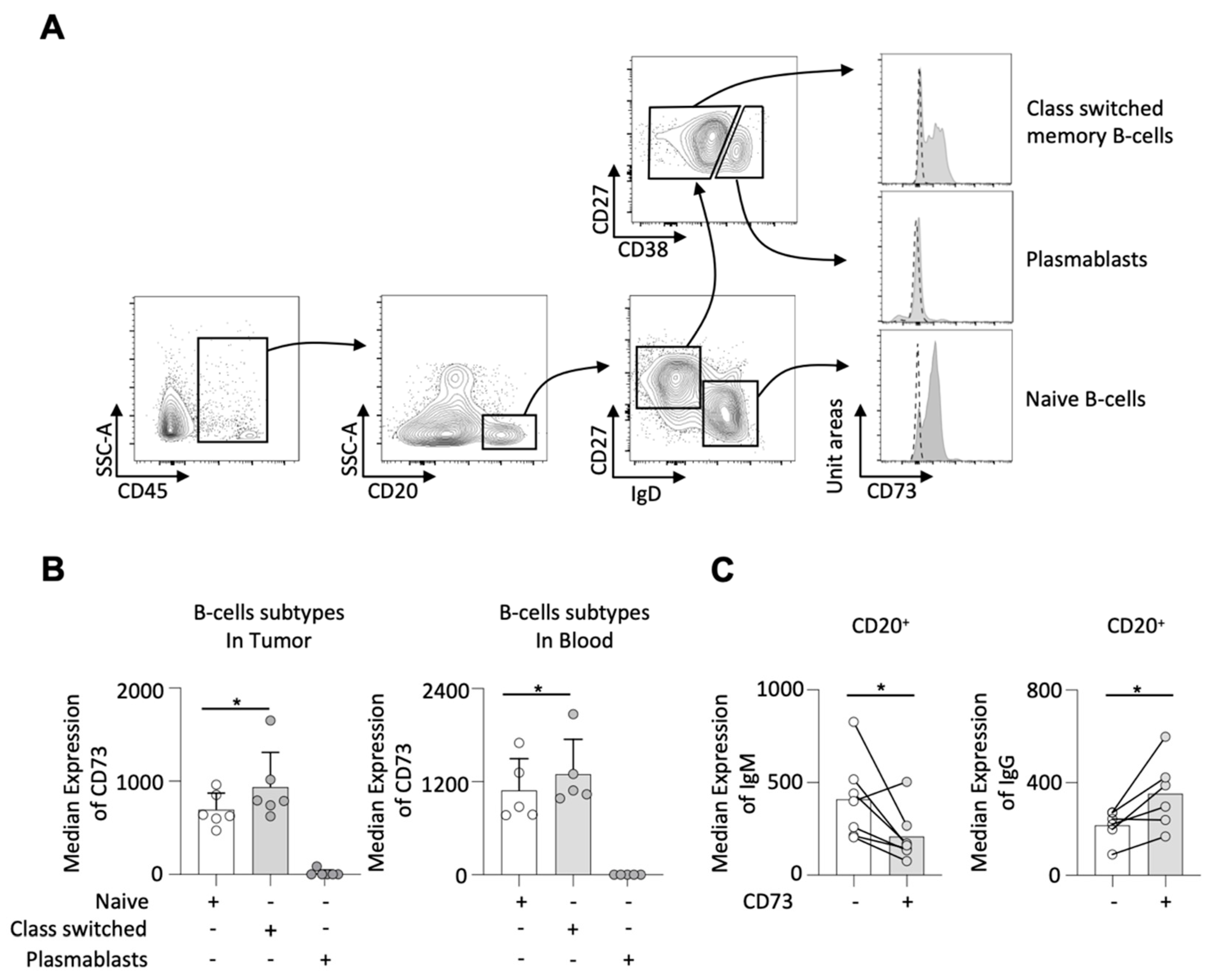
2.2. CD73 on Different B-Cell Subtypes
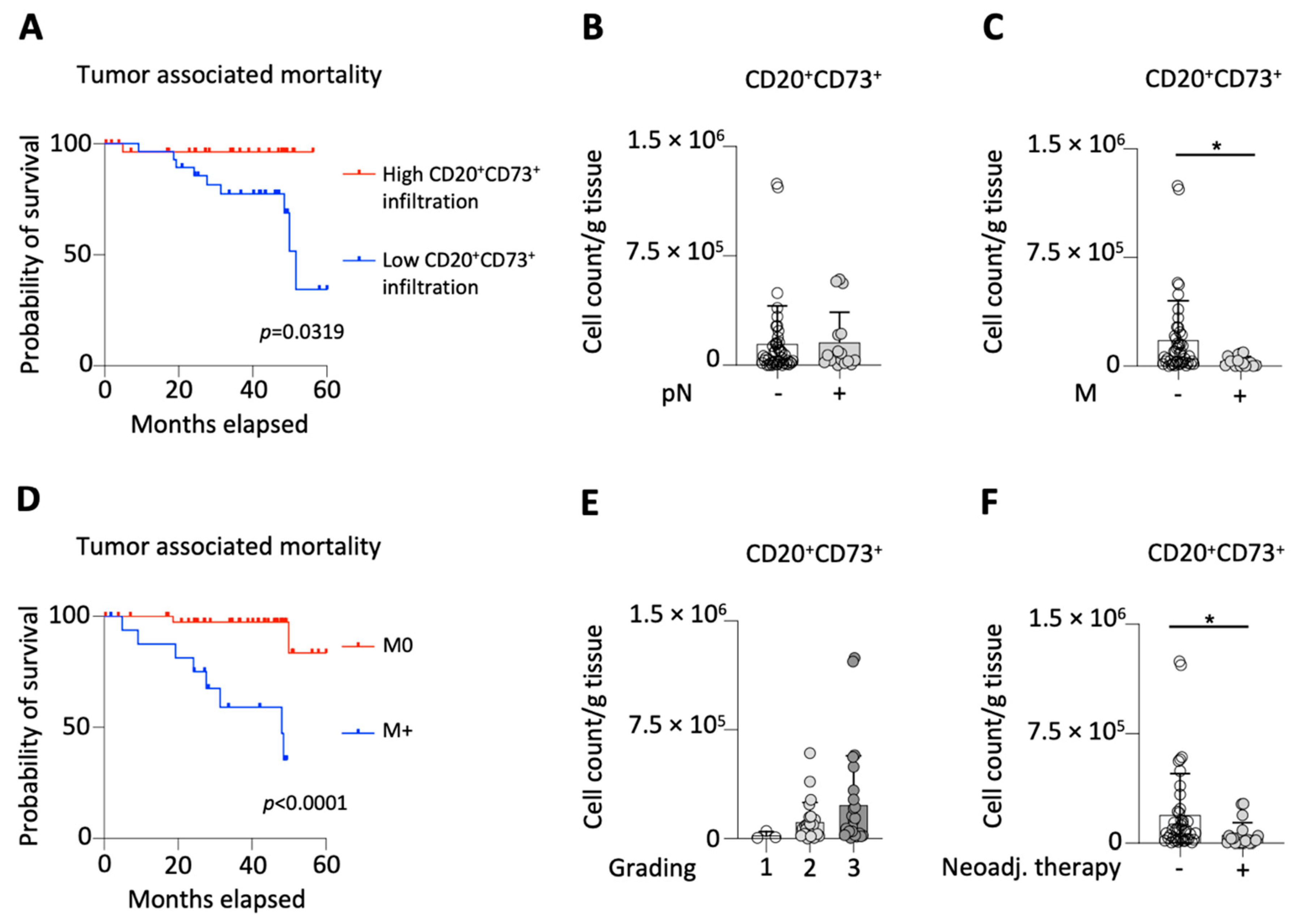
2.3. CD73 on B-Cells and Clinicopathological Characteristics
3. Discussion
4. Materials and Methods
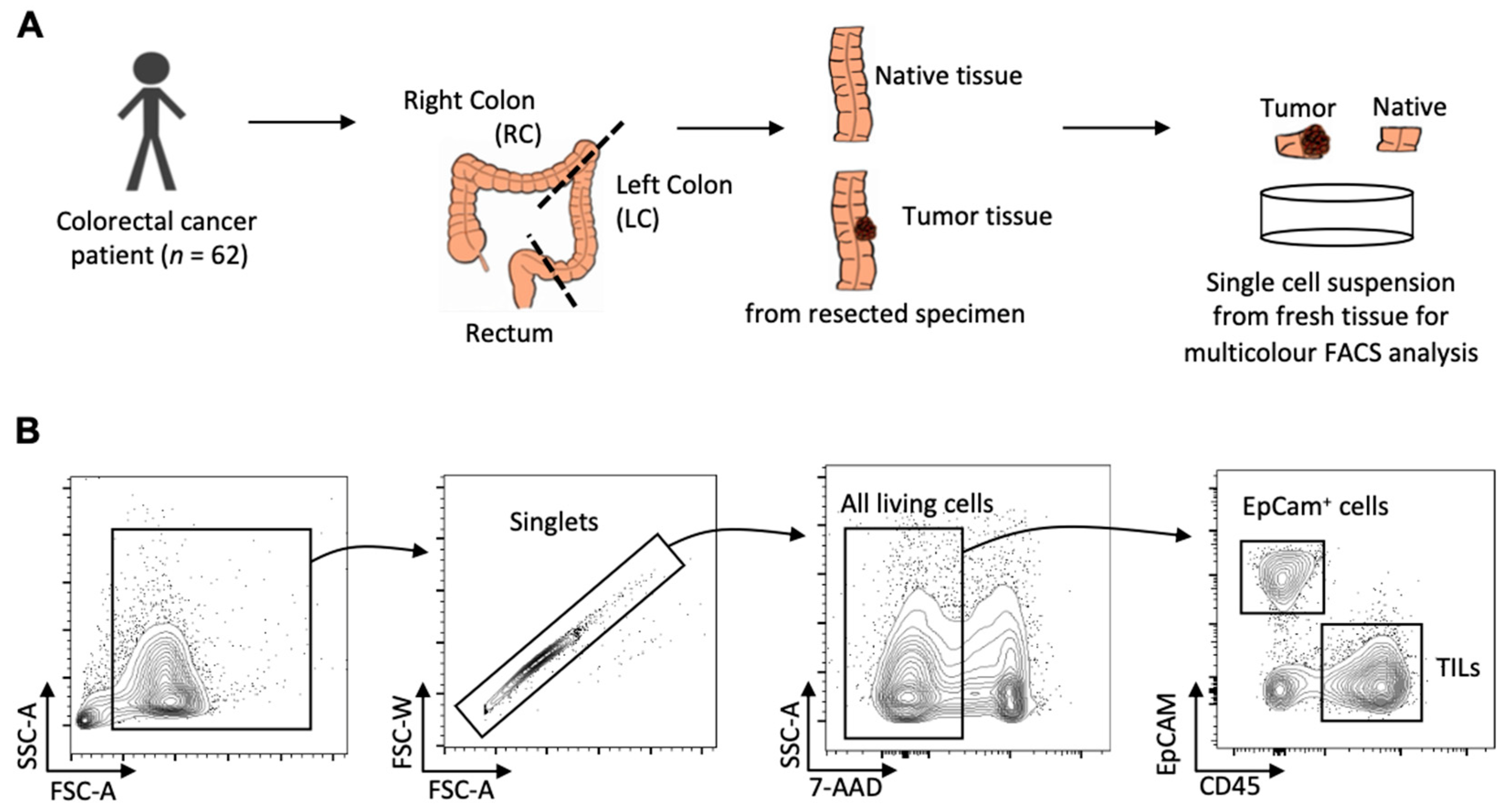
4.1. Patient Samples
4.2. Sample Preparation
4.3. Flow Cytometry
4.4. Histology
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRC | colorectal cancer |
| RC | right colon |
| LC | left colon |
| TILs | tumor-infiltrating lymphocytes |
| CEA | carcinoembryonic antigen |
| pN | lymph node invasion |
| M | metastatic spread |
| UICC | The Union of International Cancer Control |
| EpCam | epithelial cell adhesion molecule |
| TME | tumor microenvironment |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dekker, E.; Tanis, P.J.; Vleugels, J.L.A.; Kasi, P.M.; Wallace, M.B. Colorectal cancer. Lancet 2019, 394, 1467–1480. [Google Scholar] [CrossRef]
- Ganesh, K.; Stadler, Z.K.; Cercek, A.; Mendelsohn, R.B.; Shia, J.; Segal, N.H.; Diaz, L.A., Jr. Immunotherapy in colorectal cancer: Rationale, challenges and potential. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, J. Functions of Immune Checkpoint Molecules Beyond Immune Evasion. Adv. Exp. Med. Biol. 2020, 1248, 201–226. [Google Scholar] [PubMed]
- Yegutkin, G.G. Nucleotide- and nucleoside-converting ectoenzymes: Important modulators of purinergic signalling cascade. Biochim. Biophys. Acta 2008, 1783, 673–694. [Google Scholar] [CrossRef] [Green Version]
- Ohta, A.; Sitkovsky, M. Role of G-protein-coupled adenosine receptors in downregulation of inflammation and protection from tissue damage. Nature 2001, 414, 916–920. [Google Scholar] [CrossRef] [Green Version]
- Blay, J.; White, T.D.; Hoskin, D.W. The extracellular fluid of solid carcinomas contains immunosuppressive concentrations of adenosine. Cancer Res. 1997, 57, 2602–2605. [Google Scholar]
- Hu, S.; Meng, F.; Yin, X.; Cao, C.; Zhang, G. NT5E is associated with unfavorable prognosis and regulates cell proliferation and motility in gastric cancer. Biosci. Rep. 2019, 39, BSR20190101. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.L.; Shen, M.N.; Hu, B.; Wang, B.L.; Yang, W.J.; Lv, L.H.; Wang, H.; Zhou, Y.; Jin, A.L.; Sun, Y.F.; et al. CD73 promotes hepatocellular carcinoma progression and metastasis via activating PI3K/AKT signaling by inducing Rap1-mediated membrane localization of P110beta and predicts poor prognosis. J. Hematol. Oncol. 2019, 12, 37. [Google Scholar] [CrossRef]
- Zhou, L.; Jia, S.; Chen, Y.; Wang, W.; Wu, Z.; Yu, W.; Zhang, M.; Ding, G.; Cao, L. The distinct role of CD73 in the progression of pancreatic cancer. J. Mol. Med. 2019, 97, 803–815. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.R.; He, X.S.; Chen, Y.F.; Yuan, R.X.; Zeng, Y.; Lian, L.; Zou, Y.F.; Lan, N.; Wu, X.J.; Lan, P. High expression of CD73 as a poor prognostic biomarker in human colorectal cancer. J. Surg. Oncol. 2012, 106, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Song, B.; Wang, X.; Chang, X.S.; Pang, T.; Zhang, X.; Yin, K.; Fang, G.E. The expression and clinical significance of CD73 molecule in human rectal adenocarcinoma. Tumour Biol. J. Int. Soc. Oncodevelopmental Biol. Med. 2015, 36, 5459–5466. [Google Scholar] [CrossRef] [PubMed]
- Berntsson, J.; Nodin, B.; Eberhard, J.; Micke, P.; Jirström, K. Prognostic impact of tumour-infiltrating B cells and plasma cells in colorectal cancer. Int. J. Cancer 2016, 139, 1129–1139. [Google Scholar] [CrossRef] [PubMed]
- Saze, Z.; Schuler, P.J.; Hong, C.S.; Cheng, D.; Jackson, E.K.; Whiteside, T.L. Adenosine production by human B cells and B cell-mediated suppression of activated T cells. Blood 2013, 122, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Thomson, L.F.; Ruedi, J.M.; Glass, A.; Moldenhauer, G.; Moller, P.; Low, M.G.; Klemens, M.R.; Massaia, M.; Lucas, A.H. Production and characterization of monoclonal antibodies to the glycosyl phosphatidylinositol-anchored lymphocyte differentiation antigen ecto-5′-nucleotidase (CD73). Tissue Antigens 1990, 35, 9–19. [Google Scholar] [CrossRef]
- Jin, D.; Fan, J.; Wang, L.; Thompson, L.F.; Liu, A.; Daniel, B.J.; Shin, T.; Curiel, T.J.; Zhang, B. CD73 on Tumor Cells Impairs Antitumor T-Cell Responses: A Novel Mechanism of Tumor-Induced Immune Suppression. Cancer Res. 2010, 70, 2245–2255. [Google Scholar] [CrossRef] [Green Version]
- Stagg, J.; Divisekera, U.; Duret, H.; Sparwasser, T.; Teng, M.W.L.; Darcy, P.K.; Smyth, M.J. CD73-Deficient Mice Have Increased Antitumor Immunity and Are Resistant to Experimental Metastasis. Cancer Res. 2011, 71, 2892–2900. [Google Scholar] [CrossRef] [Green Version]
- Stagg, J.; Beavis, P.A.; Divisekera, U.; Liu, M.C.P.; Möller, A.; Darcy, P.K.; Smyth, M.J. CD73-Deficient Mice Are Resistant to Carcinogenesis. Cancer Res. 2012, 72, 2190–2196. [Google Scholar] [CrossRef] [Green Version]
- Yegutkin, G.G.; Marttila-Ichihara, F.; Karikoski, M.; Niemelä, J.; Laurila, J.P.; Elima, K.; Jalkanen, S.; Salmi, M. Altered purinergic signaling in CD73-deficient mice inhibits tumor progression. Eur. J. Immunol. 2011, 41, 1231–1241. [Google Scholar] [CrossRef]
- Kwak, K.; Akkaya, M.; Pierce, S.K. B cell signaling in context. Nat. Immunol. 2019, 20, 963–969. [Google Scholar] [CrossRef]
- Burger, J.A.; Wiestner, A. Targeting B cell receptor signalling in cancer: Preclinical and clinical advances. Nat. Rev. Cancer 2018, 18, 148–167. [Google Scholar] [CrossRef] [PubMed]
- DiLillo, D.J.; Yanaba, K.; Tedder, T.F. B Cells Are Required for Optimal CD4+ and CD8+ T Cell Tumor Immunity: Therapeutic B Cell Depletion Enhances B16 Melanoma Growth in Mice. J. Immunol. 2010, 184, 4006–4016. [Google Scholar] [CrossRef] [Green Version]
- Shimabukuro-Vornhagen, A.; Schlosser, H.A.; Gryschok, L.; Malcher, J.; Wennhold, K.; Garcia-Marquez, M.; Herbold, T.; Neuhaus, L.S.; Becker, H.J.; Fiedler, A.; et al. Characterization of tumor-associated B-cell subsets in patients with colorectal cancer. Oncotarget 2014, 5, 4651–4664. [Google Scholar] [CrossRef] [Green Version]
- Edin, S.; Kaprio, T.; Hagström, J.; Larsson, P.; Mustonen, H.; Böckelman, C.; Strigård, K.; Gunnarsson, U.; Haglund, C.; Palmqvist, R. The Prognostic Importance of CD20(+) B lymphocytes in Colorectal Cancer and the Relation to Other Immune Cell subsets. Sci. Rep. 2019, 9, 19997. [Google Scholar] [CrossRef] [PubMed]
- Fremd, C.; Schuetz, F.; Sohn, C.; Beckhove, P.; Domschke, C. B cell-regulated immune responses in tumor models and cancer patients. OncoImmunology 2013, 2, e25443. [Google Scholar] [CrossRef] [PubMed]
- Kaku, H.; Cheng, K.F.; Al-Abed, Y.; Rothstein, T.L. A Novel Mechanism of B Cell–Mediated Immune Suppression through CD73 Expression and Adenosine Production. J. Immunol. 2014, 193, 5904–5913. [Google Scholar] [CrossRef] [Green Version]
- Forte, G.; Sorrentino, R.; Montinaro, A.; Luciano, A.; Adcock, I.M.; Maiolino, P.; Arra, C.; Cicala, C.; Pinto, A.; Morello, S. Inhibition of CD73 improves B cell-mediated anti-tumor immunity in a mouse model of melanoma. J. Immunol. 2012, 189, 2226–2233. [Google Scholar] [CrossRef]
- Allard, B.; Longhi, M.S.; Robson, S.C.; Stagg, J. The ectonucleotidases CD39 and CD73: Novel checkpoint inhibitor targets. Immunol. Rev. 2017, 276, 121–144. [Google Scholar] [CrossRef] [Green Version]
- Conter, L.J.; Song, E.; Shlomchik, M.J.; Tomayko, M.M. CD73 expression is dynamically regulated in the germinal center and bone marrow plasma cells are diminished in its absence. PLoS ONE 2014, 9, e92009. [Google Scholar]
- Thompson, L.F.; Eltzschig, H.K.; Ibla, J.C.; Van De Wiele, C.J.; Resta, R.; Morote-Garcia, J.C.; Colgan, S.P. Crucial Role for Ecto-5′-Nucleotidase (CD73) in Vascular Leakage during Hypoxia. J. Exp. Med. 2004, 200, 1395–1405. [Google Scholar] [CrossRef]
- Synnestvedt, K.; Furuta, G.T.; Comerford, K.M.; Louis, N.; Karhausen, J.; Eltzschig, H.K.; Hansen, K.R.; Thompson, L.F.; Colgan, S.P. Ecto-5′-nucleotidase (CD73) regulation by hypoxia-inducible factor-1 mediates permeability changes in intestinal epithelia. J. Clin. Investig. 2002, 110, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Bowser, J.L.; Blackburn, M.R.; Shipley, G.L.; Molina, J.G.; Dunner, K., Jr.; Broaddus, R.R. Loss of CD73-mediated actin polymerization promotes endometrial tumor progression. J. Clin. Investig. 2016, 126, 220–238. [Google Scholar] [CrossRef] [Green Version]
- Loi, S.; Pommey, S.; Haibe-Kains, B.; Beavis, P.A.; Darcy, P.K.; Smyth, M.J.; Stagg, J. CD73 promotes anthracycline resistance and poor prognosis in triple negative breast cancer. Proc. Natl. Acad. Sci. USA 2013, 110, 11091–11096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsukui, H.; Horie, H.; Koinuma, K.; Ohzawa, H.; Sakuma, Y.; Hosoya, Y.; Yamaguchi, H.; Yoshimura, K.; Lefor, A.K.; Sata, N.; et al. CD73 blockade enhances the local and abscopal effects of radiotherapy in a murine rectal cancer model. BMC Cancer 2020, 20, 411. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infiltration of CD20+CD73+ | Low | High | p-Value | |
|---|---|---|---|---|
| Number | 31 | 31 | ||
| Mean Age (in years (range)) | 66 (30–90) | 70 (38–82) | 0.2713 | |
| Sex | Female | 11 | 12 | 0.79 |
| Male | 20 | 19 | ||
| Localization of the tumor | Right Colon | 5 | 19 | <0.01 |
| Left Colon | 7 | 4 | ||
| Rectum | 19 | 8 | ||
| Mean Tumor size (in cm (range)) | 3.7 (0–7.2) | 4.4 (0–14.0) | 0.3839 | |
| Grading | G1 | 2 | 1 | 0.08 |
| G2 | 9 | 16 | ||
| G3 | 13 | 13 | ||
| Unknown | 7 | 1 | ||
| pN-category | pN0 | 22 | 23 | 0.78 |
| pN+ | 9 | 8 | ||
| Distant Metastasis | No | 19 | 26 | 0.05 |
| Yes | 12 | 5 | ||
| UICC stage | I | 4 | 10 | 0.12 |
| II | 10 | 12 | ||
| III | 5 | 4 | ||
| IV | 12 | 5 | ||
| Neoadjuvant treatment | Yes | 16 | 4 | 0.041 |
| No | 15 | 27 | ||
| CEA | <5 µg/L | 16 | 11 | 0.41 |
| ≥5 µg/L | 5 | 8 | ||
| Unknown | 10 | 12 |
| Neoadjuvant Treatment | − | + | p-Value | |
|---|---|---|---|---|
| Number | 42 | 20 | ||
| Mean cell count of CD20+CD73+ (in per gram tissue) | 191,753 | 55,206 | 0.0411 | |
| Mean MFI of CD73 on CD20+ | 2707 | 2008 | 0.0363 | |
| Mean Age (in years (range)) | 68 (30–87) | 67 (52–90) | 0.7117 | |
| Sex | Female | 15 | 8 | 0.74 |
| Male | 27 | 12 | ||
| Localization of the tumor | Right Colon | 23 | 1 | <0.01 |
| Left Colon | 11 | 0 | ||
| Rectum | 8 | 19 | ||
| Mean Tumor size (in cm (range)) | 4.1 (0.15–11.3) | 3.6 (0–7.0) | 0.4052 | |
| Grading | G1 | 3 | 0 | <0.01 |
| G2 | 17 | 8 | ||
| G3 | 22 | 4 | ||
| Unknown | 0 | 8 | ||
| pN-category | pN0 | 29 | 16 | 0.37 |
| pN+ | 13 | 4 | ||
| Distant Metastasis | No | 35 | 10 | <0.01 |
| Yes | 7 | 10 | ||
| UICC stage | I | 9 | 5 | <0.01 |
| II | 17 | 5 | ||
| III | 9 | 0 | ||
| IV | 7 | 10 | ||
| CEA | <5 µg/L | 16 | 11 | 0.40 |
| ≥5 µg/L | 9 | 4 | ||
| Unknown | 17 | 5 |
| CRC Patients | |
|---|---|
| Number | 62 |
| Age (median) | 71 (38–90) |
| Sex (Male:Female) | 39:23 |
| Neoadjuvant therapy | |
| Radiochemotherapy | 19 |
| Chemotherapy | 1 |
| - | 42 |
| Localization of the tumor | |
| Right colon (RC) | 24 |
| Left colon (LC) | 11 |
| Rectum | 27 |
| Histological Grade | |
| G1 | 3 |
| G2 | 25 |
| G3 | 26 |
| Unknown | 8 |
| pN-category | |
| pN0 | 17 |
| pN+ | 45 |
| Distant Metastasis | |
| No | 45 |
| Yes | 17 |
| UICC stage | |
| I | 14 |
| II | 22 |
| III | 9 |
| IV | 17 |
| Preoperative CEA level | |
| Low (<5 µg/L) | 27 |
| High (≥5 µg/L) | 13 |
| Unknown | 22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, F.J.; Wu, Z.; David, P.; Mittelstädt, A.; Jacobsen, A.; Podolska, M.J.; Ubieta, K.; Brunner, M.; Kouhestani, D.; Swierzy, I.; et al. Tumor Infiltration with CD20+CD73+ B Cells Correlates with Better Outcome in Colorectal Cancer. Int. J. Mol. Sci. 2022, 23, 5163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23095163
Hansen FJ, Wu Z, David P, Mittelstädt A, Jacobsen A, Podolska MJ, Ubieta K, Brunner M, Kouhestani D, Swierzy I, et al. Tumor Infiltration with CD20+CD73+ B Cells Correlates with Better Outcome in Colorectal Cancer. International Journal of Molecular Sciences. 2022; 23(9):5163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23095163
Chicago/Turabian StyleHansen, Frederik J., Zhiyuan Wu, Paul David, Anke Mittelstädt, Anne Jacobsen, Malgorzata J. Podolska, Kenia Ubieta, Maximilian Brunner, Dina Kouhestani, Izabela Swierzy, and et al. 2022. "Tumor Infiltration with CD20+CD73+ B Cells Correlates with Better Outcome in Colorectal Cancer" International Journal of Molecular Sciences 23, no. 9: 5163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23095163