
Advancing Spinal Cord Injury Treatment through Stem Cell Therapy: A Comprehensive Review of Cell Types, Challenges, and Emerging Technologies in Regenerative Medicine

Abstract
:1. Introduction
2. The Promise of Stem Cell Therapy for SCIs
2.1. Comparative Analysis of Stem Cell Transplantation and Other Cell-Based Therapies in SCIs
2.1.1. Advantages of Stem Cells
2.1.2. Disadvantages of Stem Cells
2.1.3. Advantages of Schwann Cells and Olfactory Ensheathing Glia Cells
2.1.4. Disadvantages of Schwann Cells and Olfactory Ensheathing Glia Cells
2.2. Biomaterials in 3D Stem Cell Constructs for SCI
2.2.1. Hydrogels
2.2.2. Poly(ethylene glycol)-Fibrinogen Hydrogels
2.2.3. Nanomaterials
2.2.4. Microgels
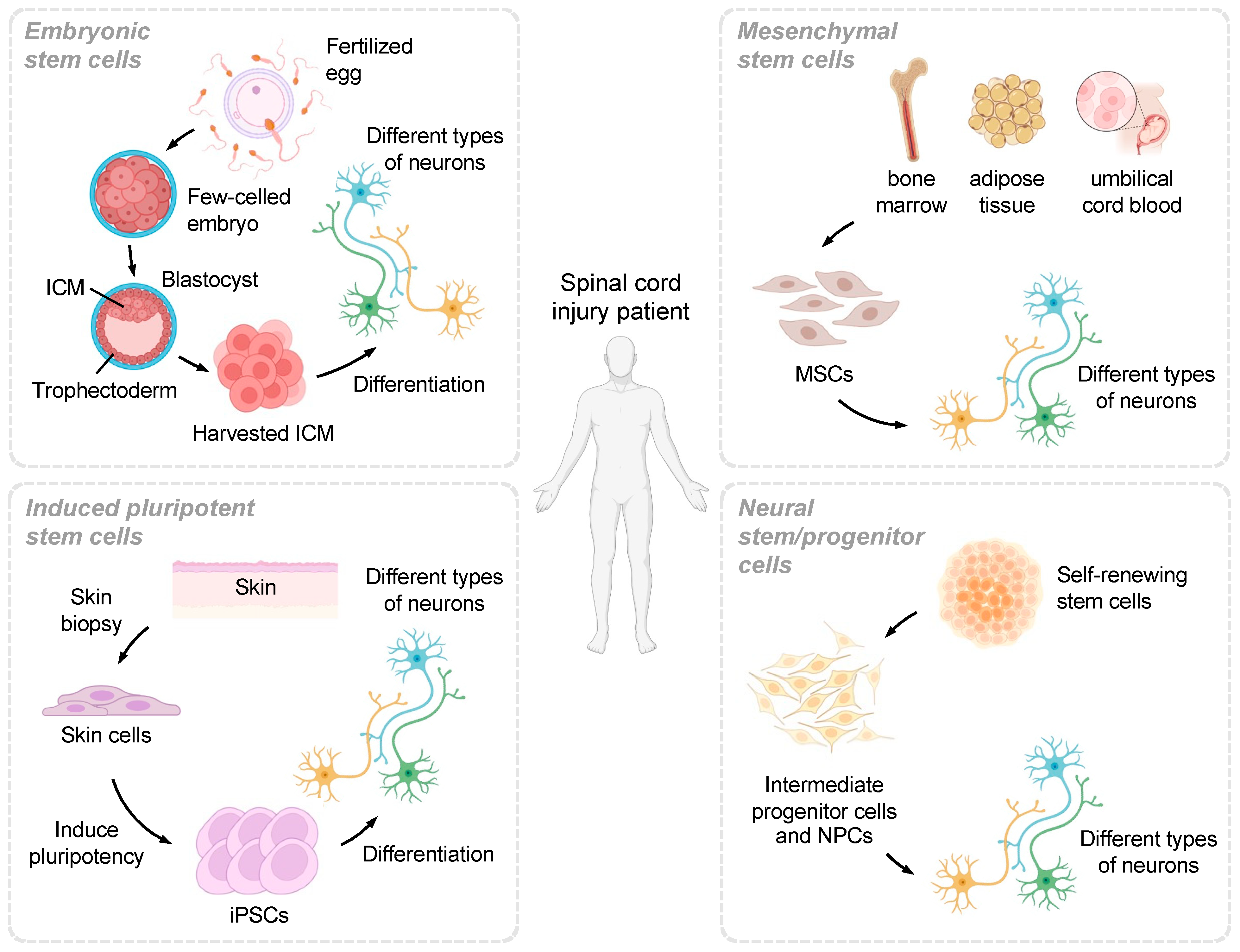
3. The Potential of Different Stem Cell Types
3.1. Embryonic Stem Cells
3.2. Induced Pluripotent Stem Cells
3.3. Mesenchymal Stem Cells
3.4. Neural Stem/Progenitor Cells
3.5. Clinical Outcomes and Adverse Events
3.5.1. Immune Rejection
3.5.2. Rate/Incidence of Improvement and Failure to Improve
3.5.3. Occurrence of Cancer or Other Adverse Events
3.5.4. Other Adverse Events
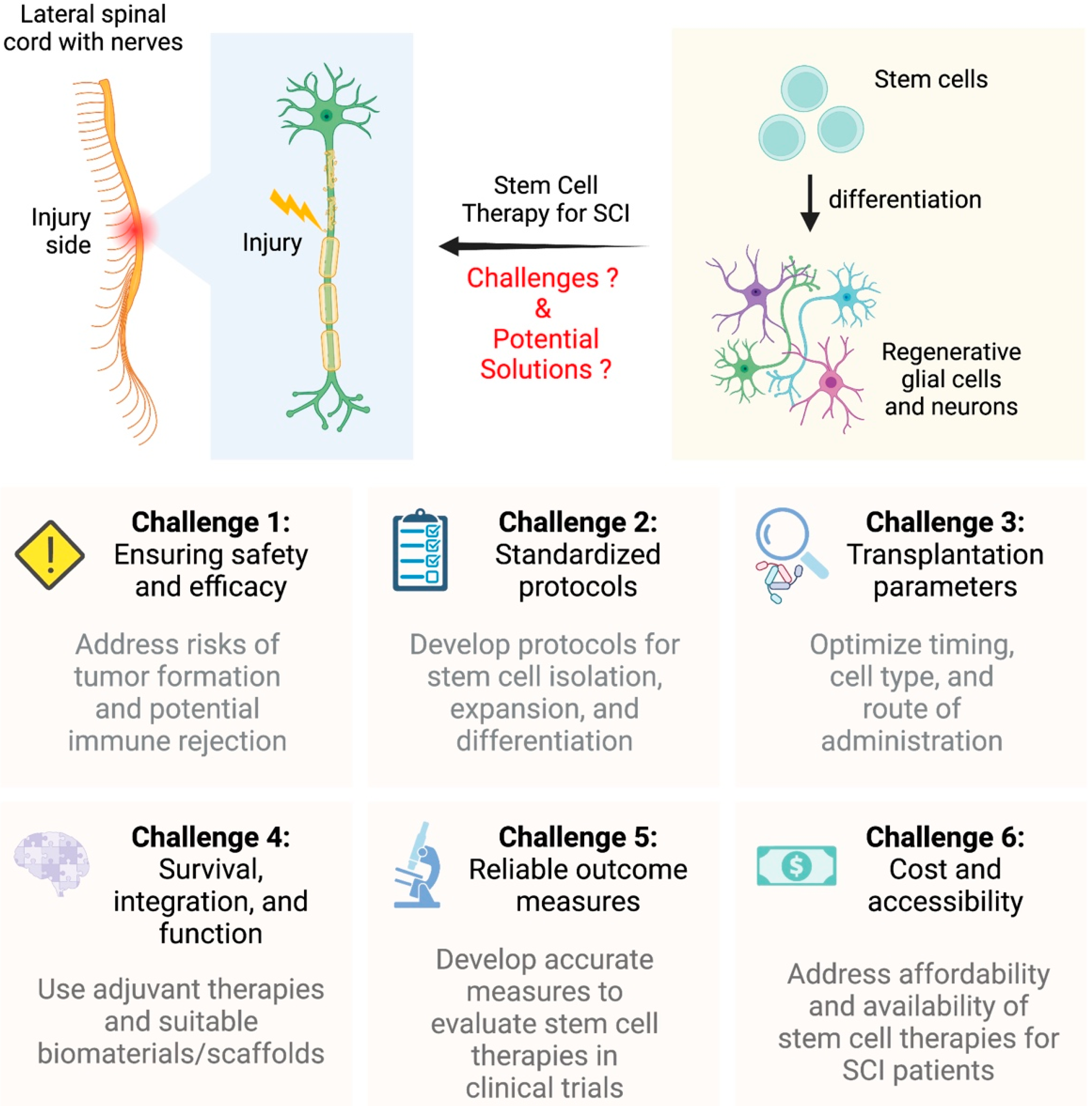
4. Challenges in Stem Cell Therapy for SCI
4.1. Secondary Injury and Stem Cell Transplantation
4.1.1. Prevention of Secondary Damage
4.1.2. Restriction of Tissue Damage
4.1.3. Optimal Timing
4.1.4. Microenvironment
5. Future Directions and Technological Advancements
5.1. Interdisciplinary Approaches to Advancing Stem Cell Therapies for SCIs
5.1.1. Biomaterials and Differentiation
5.1.2. Cell Engineering Techniques
5.1.3. Clinical Translations
5.1.4. Challenges and Solutions
5.1.5. Quality of Life Improvements in SCI Patients
5.2. Challenges and Problems in Non-Traumatic SCI
5.2.1. Safety and Feasibility
5.2.2. Optimal Timing
5.2.3. Microenvironment
5.2.4. Ethical Concerns
5.2.5. Efficacy
5.3. The Role of Biomaterials, Engineering, and Collaborative Research for SCI Therapies
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Badenhorst, M. Life after the Game: Consequences of Acute Spinal Cord Injuries in South African Rugby Union Players. Ph.D. Thesis, University of Cape Town, Cape Town, South Africa, 2019. [Google Scholar]
- Courtine, G.; Sofroniew, M.V. Spinal cord repair: Advances in biology and technology. Nat. Med. 2019, 25, 898–908. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Wu, Y.; Xu, Y.; Li, G.; Li, Z.; Liu, T. Mesenchymal stem cell-derived exosomes in cancer therapy resistance: Recent advances and therapeutic potential. Mol. Cancer 2022, 21, 179. [Google Scholar] [CrossRef] [PubMed]
- Chia, W.K.; Cheah, F.C.; Abdul Aziz, N.H.; Kampan, N.C.; Shuib, S.; Khong, T.Y.; Tan, G.C.; Wong, Y.P. A review of placenta and umbilical cord-derived stem cells and the immunomodulatory basis of their therapeutic potential in bronchopulmonary dysplasia. Front. Pediatr. 2021, 9, 615508. [Google Scholar] [CrossRef]
- Surkin, J.; Gilbert, B.J.C.; Harkey III, H.L.; Sniezek, J.; Currier, M. Spinal cord injury in Mississippi: Findings and evaluation, 1992–1994. Spine 2000, 25, 716–721. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.E.; Castellote, J.M.; Mahillo-Fernandez, I.; de Pedro-Cuesta, J. Incidence of nontraumatic spinal cord injury: A Spanish cohort study (1972–2008). Arch. Phys. Med. Rehabil. 2012, 93, 325–331. [Google Scholar] [CrossRef]
- Albert, T.; Ravaud, J.F. Rehabilitation of spinal cord injury in France: A nationwide multicentre study of incidence and regional disparities. Spinal Cord 2005, 43, 357–365. [Google Scholar] [CrossRef]
- Joseph, C.; Andersson, N.; Bjelak, S.; Giesecke, K.; Hultling, C. Incidence, aetiology and injury characteristics of traumatic spinal cord injury in Stockholm, Sweden: A prospective, population-based update. J. Rehabil. Med. 2017, 49, 431–436. [Google Scholar] [CrossRef]
- Fitzharris, M.; Cripps, R.A.; Lee, B.B. Estimating the global incidence of traumatic spinal cord injury. Spinal Cord 2014, 52, 117–122. [Google Scholar] [CrossRef]
- New, P.W.; Farry, A.; Baxter, D.; Noonan, V.K. Prevalence of non-traumatic spinal cord injury in Victoria, Australia. Spinal Cord 2013, 51, 99–102. [Google Scholar] [CrossRef]
- Hagen, E.M.; Eide, G.E.; Rekand, T.; Gilhus, N.E.; Gronning, M. A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord 2010, 48, 313–318. [Google Scholar] [CrossRef]
- Van den Berg, M.E.L.; Castellote, J.M.; Mahillo-Fernandez, I.; de Pedro-Cuesta, J. Incidence of spinal cord injury worldwide: A systematic review. Neuroepidemiology 2010, 34, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Ahoniemi, E.; Alaranta, H.; Hokkinen, E.M.; Valtonen, K.; Kautiainen, H. Incidence of traumatic spinal cord injuries in Finland over a 30-year period. Spinal Cord 2008, 46, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Hao, D.; He, B.; Yan, L.; Tang, Q.; Zhang, Z.; Wang, Y.; Li, H.; Cao, Y.; Jiang, C.Q.; et al. Epidemiological characteristics of traumatic spinal cord injury in Xi’an, China. Spinal Cord 2021, 59, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Ackery, A.; Tator, C.; Krassioukov, A. A global perspective on spinal cord injury epidemiology. J. Neurotrauma 2004, 21, 1355–1370. [Google Scholar] [CrossRef] [PubMed]
- Madl, C.M.; Heilshorn, S.C.; Blau, H.M. Bioengineering strategies to accelerate stem cell therapeutics. Nature 2018, 557, 335–342. [Google Scholar] [CrossRef]
- Rajabzadeh, N.; Fathi, E.; Farahzadi, R. Stem cell-based regenerative medicine. Stem Cell Investig. 2019, 6, 19. [Google Scholar] [CrossRef]
- Fischer, I.; Dulin, J.N.; Lane, M.A. Transplanting neural progenitor cells to restore connectivity after spinal cord injury. Nat. Rev. Neurosci. 2020, 21, 366–383. [Google Scholar] [CrossRef]
- Pajer, K.; Bellák, T.; Nógrádi, A. Stem Cell secretome for spinal cord repair: Is it more than just a random baseline set of factors? Cells 2021, 10, 3214. [Google Scholar] [CrossRef]
- Myatich, A.; Haque, A.; Sole, C.; Banik, N.L. Clemastine in remyelination and protection of neurons and skeletal muscle after spinal cord injury. Neural Regen. Res. 2023, 18, 940–946. [Google Scholar]
- Rahman, M.M.; Islam, M.R.; Islam, M.T.; Harun-Or-Rashid, M.; Islam, M.; Abdullah, S.; Uddin, M.B.; Das, S.; Rahaman, M.S.; Ahmed, M.; et al. Stem cell transplantation therapy and neurological disorders: Current status and future perspectives. Biology 2022, 11, 147. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, F.; Song, M. The cell repair research of spinal cord injury: A review of cell transplantation to treat spinal cord injury. J. Neurorestoratology 2019, 7, 55–62. [Google Scholar] [CrossRef]
- Chen, X.; Wang, Y.; Zhou, G.; Hu, X.; Han, S.; Gao, J. The combination of nanoscaffolds and stem cell transplantation: Paving a promising road for spinal cord injury regeneration. Biomed. Pharmacother. 2021, 143, 112233. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Zhou, J.; Wang, Y.; Fan, F.; Liu, S.; Wang, Y. Neural Stem/Progenitor Cell Transplantation in Parkinson’s Rodent Animals: A Meta-Analysis and Systematic Review. Stem Cells Transl. Med. 2022, 11, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.W. Multipotent Mesenchymal Stem Cell-Based Therapies for Spinal Cord Injury: Current Progress and Future Prospects. Biology 2023, 12, 653. [Google Scholar] [CrossRef] [PubMed]
- Simonson, O.E.; Domogatskaya, A.; Volchkov, P.; Rodin, S. The safety of human pluripotent stem cells in clinical treatment. Ann. Med. 2015, 47, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Zhang, Y.; Xie, Y.; Zhang, L.; Tang, P. Cell transplantation for spinal cord injury: Tumorigenicity of induced pluripotent stem cell-derived neural stem/progenitor cells. Stem Cells Int. 2018, 2018, 5653787. [Google Scholar] [CrossRef]
- Liu, G.; David, B.T.; Trawczynski, M.; Fessler, R.G. Advances in pluripotent stem cells: History, mechanisms, technologies, and applications. Stem Cell Rev. Rep. 2020, 16, 3–32. [Google Scholar] [CrossRef]
- Cao, C.; Tarlé, S.; Kaigler, D. Characterization of the immunomodulatory properties of alveolar bone-derived mesenchymal stem cells. Stem Cell Res. Ther. 2020, 11, 102. [Google Scholar] [CrossRef]
- Ni, W.; Ramalingam, M.; Li, Y.; Park, J.H.; Dashnyam, K.; Lee, J.H.; Bloise, N.; Fassina, L.; Visai, L.; De Angelis, M.G.C.; et al. Immunomodulatory and Anti-inflammatory effect of Neural Stem/Progenitor Cells in the Central Nervous System. Stem Cell Rev. Rep. 2023, 19, 866–885. [Google Scholar] [CrossRef]
- Chen, F.M.; Sun, H.H.; Lu, H.; Yu, Q. Stem cell-delivery therapeutics for periodontal tissue regeneration. Biomaterials 2012, 33, 6320–6344. [Google Scholar] [CrossRef]
- Chen, Y.; Pal, S.; Hu, Q. Recent advances in biomaterial-assisted cell therapy. J. Mater. Chem. B 2022, 10, 7222–7238. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Li, Z.; Li, L.; Liu, S.; Wu, P.; Zhou, M.; Li, C.; Li, X.; Luo, G.; Zhang, J. Stem Cell-Niche Engineering via Multifunctional Hydrogel Potentiates Stem Cell Therapies for Inflammatory Bone Loss. Adv. Funct. Mater. 2023, 33, 2209466. [Google Scholar] [CrossRef]
- Charitos, I.A.; Ballini, A.; Cantore, S.; Boccellino, M.; Di Domenico, M.; Borsani, E.; Nocini, R.; Di Cosola, M.; Santacroce, L.; Bottalico, L. Stem cells: A historical review about biological, religious, and ethical issues. Stem Cells Int. 2021, 2021, 9978837. [Google Scholar] [CrossRef] [PubMed]
- Zarzeczny, A.; Atkins, H.; Illes, J.; Kimmelman, J.; Master, Z.; Robillard, J.M.; Snyder, J.; Turner, L.; Zettler, P.J.; Caulfield, T. The stem cell market and policy options: A call for clarity. J. Law Biosci. 2018, 5, 743–758. [Google Scholar] [CrossRef] [PubMed]
- Shao, A.; Tu, S.; Lu, J.; Zhang, J. Crosstalk between stem cell and spinal cord injury: Pathophysiology and treatment strategies. Stem Cell Res. Ther. 2019, 10, 238. [Google Scholar] [CrossRef] [PubMed]
- Duncan, G.J.; Manesh, S.B.; Hilton, B.J.; Assinck, P.; Plemel, J.R.; Tetzlaff, W. The fate and function of oligodendrocyte progenitor cells after traumatic spinal cord injury. Glia 2020, 68, 227–245. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Xu, J. Immune modulation by mesenchymal stem cells. Cell Prolif. 2020, 53, e12712. [Google Scholar] [CrossRef]
- Miyajima, H.; Itokazu, T.; Tanabe, S.; Yamashita, T. Interleukin-17A regulates ependymal cell proliferation and functional recovery after spinal cord injury in mice. Cell Death Dis. 2021, 12, 766. [Google Scholar] [CrossRef]
- Orr, M.B.; Gensel, J.C. Spinal cord injury scarring and inflammation: Therapies targeting glial and inflammatory responses. Neurotherapeutics 2018, 15, 541–553. [Google Scholar] [CrossRef]
- Yang, B.; Zhang, F.; Cheng, F.; Ying, L.; Wang, C.; Shi, K.; Wang, J.; Xia, K.; Gong, Z.; Huang, X.; et al. Strategies and prospects of effective neural circuits reconstruction after spinal cord injury. Cell Death Dis. 2020, 11, 439. [Google Scholar] [CrossRef]
- Ding, Y.; Chen, Q. mTOR pathway: A potential therapeutic target for spinal cord injury. Biomed. Pharmacother. 2022, 145, 112430. [Google Scholar] [CrossRef] [PubMed]
- Pang, Q.M.; Chen, S.Y.; Fu, S.P.; Zhou, H.; Zhang, Q.; Ao, J.; Luo, X.P.; Zhang, T. Regulatory role of mesenchymal stem cells on secondary inflammation in spinal cord injury. J. Inflamm. Res. 2022, 15, 573–593. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.D.; Pickard, M.R.; Johnson, W.E. The comparative effects of mesenchymal stem cell transplantation therapy for spinal cord injury in humans and animal models: A systematic review and meta-analysis. Biology 2021, 10, 230. [Google Scholar] [CrossRef]
- Jin, M.C.; Medress, Z.A.; Azad, T.D.; Doulames, V.M.; Veeravagu, A. Stem cell therapies for acute spinal cord injury in humans: A review. Neurosurg. Focus 2019, 46, E10. [Google Scholar] [CrossRef] [PubMed]
- Bedir, T.; Ulag, S.; Ustundag, C.B.; Gunduz, O. 3D bioprinting applications in neural tissue engineering for spinal cord injury repair. Mater. Sci. Eng. C 2020, 110, 110741. [Google Scholar] [CrossRef]
- Szymoniuk, M.; Mazurek, M.; Dryla, A.; Kamieniak, P. The application of 3D-bioprinted scaffolds for neuronal regeneration after traumatic spinal cord injury–A systematic review of preclinical in vivo studies. Exp. Neurol. 2023, 363, 114366. [Google Scholar] [CrossRef]
- Xu, Z.X.; Zhang, L.Q.; Zhou, Y.N.; Chen, X.M.; Xu, W.H. Histological and functional outcomes in a rat model of hemisected spinal cord with sustained VEGF/NT-3 release from tissue-engineered grafts. Artif. Cells Nanomed. Biotechnol. 2020, 48, 362–376. [Google Scholar] [CrossRef]
- Stower, H. Cell therapy for spinal cord injury. Nat. Med. 2018, 24, 1088. [Google Scholar] [CrossRef]
- Oraee-Yazdani, S.; Hafizi, M.; Atashi, A.; Ashrafi, F.; Seddighi, A.S.; Hashemi, S.M.; Seddighi, A.; Soleimani, M.; Zali, A. Co-transplantation of autologous bone marrow mesenchymal stem cells and Schwann cells through cerebral spinal fluid for the treatment of patients with chronic spinal cord injury: Safety and possible outcome. Spinal Cord 2016, 54, 102–109. [Google Scholar] [CrossRef]
- Moviglia, G.A.; Fernandez Vina, R.; Brizuela, J.A.; Saslavsky, J.; Vrsalovic, F.; Varela, G.; Bastos, F.; Farina, P.; Etchegaray, G.; Barbieri, M.; et al. Combined protocol of cell therapy for chronic spinal cord injury. Report on the electrical and functional recovery of two patients. Cytotherapy 2006, 8, 202–209. [Google Scholar] [CrossRef]
- Chhabra, H.S.; Sarda, K.; Arora, M.; Sharawat, R.; Singh, V.; Nanda, A.; Sangodimath, G.M.; Tandon, V. Autologous bone marrow cell transplantation in acute spinal cord injury—An Indian pilot study. Spinal Cord 2016, 54, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.W. Macrophage–Neuroglia Interactions in Promoting Neuronal Regeneration in Zebrafish. Int. J. Mol. Sci. 2023, 24, 6483. [Google Scholar] [CrossRef] [PubMed]
- Koffler, J.; Zhu, W.; Qu, X.; Platoshyn, O.; Dulin, J.N.; Brock, J.; Graham, L.; Lu, P.; Sakamoto, J.; Marsala, M.; et al. Biomimetic 3D-printed scaffolds for spinal cord injury repair. Nat. Med. 2019, 25, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.W. Unraveling the Critical Mechanisms and Functions of Neuroglia in Spinal Cord Injuries. Neuroglia 2023, 4, 188–190. [Google Scholar] [CrossRef]
- Vijayavenkataraman, S. Nerve guide conduits for peripheral nerve injury repair: A review on design, materials and fabrication methods. Acta Biomater. 2020, 106, 54–69. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Kudva, A.K.; Saxena, N.S.; Roy, K. Engineering articular cartilage with spatially-varying matrix composition and mechanical properties from a single stem cell population using a multi-layered hydrogel. Biomaterials 2011, 32, 6946–6952. [Google Scholar] [CrossRef]
- Wei, K.; Chen, X.; Li, R.; Feng, Q.; Bian, L. Multivalent host–guest hydrogels as fatigue-resistant 3D matrix for excessive mechanical stimulation of encapsulated cells. Chem. Mater. 2017, 29, 8604–8610. [Google Scholar] [CrossRef]
- Kerscher, P.; Turnbull, I.C.; Hodge, A.J.; Kim, J.; Seliktar, D.; Easley, C.J.; Costa, K.D.; Lipke, E.A. Direct hydrogel encapsulation of pluripotent stem cells enables ontomimetic differentiation and growth of engineered human heart tissues. Biomaterials 2016, 83, 383–395. [Google Scholar] [CrossRef]
- Zhao, C.; Tan, A.; Pastorin, G.; Ho, H.K. Nanomaterial scaffolds for stem cell proliferation and differentiation in tissue engineering. Biotechnol. Adv. 2013, 31, 654–668. [Google Scholar] [CrossRef]
- Salehi, S.S.; Shamloo, A.; Hannani, S.K. Microfluidic technologies to engineer mesenchymal stem cell aggregates—Applications and benefits. Biophys. Rev. 2020, 12, 123–133. [Google Scholar] [CrossRef]
- Corti, S.; Nizzardo, M.; Nardini, M.; Donadoni, C.; Salani, S.; Ronchi, D.; Simone, C.; Falcone, M.; Papadimitriou, D.; Locatelli, F.; et al. Embryonic stem cell-derived neural stem cells improve spinal muscular atrophy phenotype in mice. Brain 2010, 133, 465–481. [Google Scholar] [CrossRef] [PubMed]
- Jones, I.; Novikova, L.N.; Wiberg, M.; Carlsson, L.; Novikov, L.N. Human embryonic stem cell–derived neural crest cells promote sprouting and motor recovery following spinal cord injury in adult rats. Cell Transplant. 2021, 30, 0963689720988245. [Google Scholar] [CrossRef] [PubMed]
- Nori, S.; Tsuji, O.; Okada, Y.; Toyama, Y.; Okano, H.; Nakamura, M. Therapeutic potential of induced pluripotent stem cells for spinal cord injury. Brain Nerve = Shinkei Kenkyu No Shinpo 2012, 64, 17–27. [Google Scholar] [PubMed]
- Li, Y.; Shen, P.P.; Wang, B. Induced pluripotent stem cell technology for spinal cord injury: A promising alternative therapy. Neural Regen. Res. 2021, 16, 1500. [Google Scholar]
- Zhang, D.; He, X. A meta-analysis of the motion function through the therapy of spinal cord injury with intravenous transplantation of bone marrow mesenchymal stem cells in rats. PLoS ONE 2014, 9, e93487. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, W.; Liu, W.; Zhou, Y.; Jia, J.; Yang, L. Transplantation of placenta-derived mesenchymal stem cell-induced neural stem cells to treat spinal cord injury. Neural Regen. Res. 2014, 9, 2197. [Google Scholar]
- McMahon, S.S.; Albermann, S.; Rooney, G.E.; Shaw, G.; Garcia, Y.; Sweeney, E.; Hynes, J.; Dockery, P.; O’Brien, T.; Windebank, A.J.; et al. Engraftment, migration and differentiation of neural stem cells in the rat spinal cord following contusion injury. Cytotherapy 2010, 12, 313–325. [Google Scholar] [CrossRef]
- Tang, Y.; Cui, Y.C.; Wang, X.J.; Wu, A.L.; Hu, G.F.; Luo, F.L.; Sun, J.; Sun, J.; Wu, L. Neural progenitor cells derived from adult bone marrow mesenchymal stem cells promote neuronal regeneration. Life Sci. 2012, 91, 951–958. [Google Scholar] [CrossRef]
- Cusimano, M.; Biziato, D.; Brambilla, E.; Donega, M.; Alfaro-Cervello, C.; Snider, S.; Salani, G.; Pucci, F.; Comi, G.; Garcia-Verdugo, J.M.; et al. Transplanted neural stem/precursor cells instruct phagocytes and reduce secondary tissue damage in the injured spinal cord. Brain 2012, 135, 447–460. [Google Scholar] [CrossRef]
- Guo, S.; Wang, L.; Xie, Y.; Luo, X.; Zhang, S.; Xiong, L.; Ai, H.; Yuan, Z.; Wang, J. Bibliometric and visualized analysis of stem cells therapy for spinal cord injury based on Web of Science and CiteSpace in the last 20 years. World Neurosurg. 2019, 132, e246–e258. [Google Scholar] [CrossRef]
- Coutts, M.; Keirstead, H.S. Stem cells for the treatment of spinal cord injury. Exp. Neurol. 2008, 209, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Soto, D.A.; Navarro, M.; Zheng, C.; Halstead, M.M.; Zhou, C.; Guiltinan, C.; Wu, J.; Ross, P.J. Simplification of culture conditions and feeder-free expansion of bovine embryonic stem cells. Sci. Rep. 2021, 11, 11045. [Google Scholar] [CrossRef] [PubMed]
- Barbuti, P.A.; Barker, R.A.; Brundin, P.; Przedborski, S.; Papa, S.M.; Kalia, L.V.; Mochizuki, H. Recent advances in the development of stem-cell-derived dopaminergic neuronal transplant therapies for Parkinson’s disease. Mov. Disord. 2021, 36, 1772–1780. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, T.; Abasi, M.; Seifar, F.; Eyvazi, S.; Hejazi, M.S.; Tarhriz, V.; Montazersaheb, S. Transplantation of stem cells as a potential therapeutic strategy in neurodegenerative disorders. Curr. Stem Cell Res. Ther. 2021, 16, 133–144. [Google Scholar] [CrossRef]
- Kossow, S. Creating a united front: Harmonizing the united states regulatory policies surrounding human embryonic stem cell research. SMU Sci. Technol. Law Rev. 2022, 25, 295. [Google Scholar] [CrossRef]
- Otsuka, R.; Wada, H.; Murata, T.; Seino, K.I. Immune reaction and regulation in transplantation based on pluripotent stem cell technology. Inflamm. Regen. 2020, 40, 12. [Google Scholar] [CrossRef]
- Haworth, R.; Sharpe, M. Accept or reject: The role of immune tolerance in the development of stem cell therapies and possible future approaches. Toxicol. Pathol. 2021, 49, 1308–1316. [Google Scholar] [CrossRef]
- Gong, Z.; Xia, K.; Xu, A.; Yu, C.; Wang, C.; Zhu, J.; Huang, X.; Chen, Q.; Li, F.; Liang, C.; et al. Stem cell transplantation: A promising therapy for spinal cord injury. Curr. Stem Cell Res. Ther. 2020, 15, 321–331. [Google Scholar] [CrossRef]
- Chang, E.A.; Jin, S.W.; Nam, M.H.; Kim, S.D. Human induced pluripotent stem cells: Clinical significance and applications in neurologic diseases. J. Korean Neurosurg. Soc. 2019, 62, 493–501. [Google Scholar] [CrossRef]
- Basso, D.M.; Beattie, M.S.; Bresnahan, J.C. A sensitive and reliable locomotor rating scale for open field testing in rats. J. Neurotrauma 1995, 12, 1–21. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Tator, C.H. The relationships among the severity of spinal cord injury, residual neurological function, axon counts, and counts of retrogradely labeled neurons after experimental spinal cord injury. Exp. Neurol. 1995, 132, 220–228. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.W.; Sadowsky, C. Spinal-cord injury. Lancet 2002, 359, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Tetzlaff, W.; Okon, E.B.; Karimi-Abdolrezaee, S.; Hill, C.E.; Sparling, J.S.; Plemel, J.R.; Plunet, W.T.; Tsai, E.C.; Baptiste, D.C.; Smithson, L.J.; et al. A systematic review of cellular transplantation therapies for spinal cord injury. J. Neurotrauma 2011, 28, 1611–1682. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.L.; Margolis, R.U.; Tuszynski, M.H. The chondroitin sulfate proteoglycans neurocana, brevican, phosphacan, and versican are differentially regulated following spinal cord injury. Exp. Neurol. 2003, 182, 399–411. [Google Scholar] [CrossRef]
- Assinck, P.; Duncan, G.J.; Hilton, B.J.; Plemel, J.R.; Tetzlaff, W. Cell transplantation therapy for spinal cord injury. Nat. Neurosci. 2017, 20, 637–647. [Google Scholar] [CrossRef]
- Gao, L.; Peng, Y.; Xu, W.; He, P.; Li, T.; Lu, X.; Chen, G. Progress in stem cell therapy for spinal cord injury. Stem Cells Int. 2020, 2020, 2853650. [Google Scholar] [CrossRef]
- Oliveri, R.S.; Bello, S.; Biering-Sørensen, F. Mesenchymal stem cells improve locomotor recovery in traumatic spinal cord injury: Systematic review with meta-analyses of rat models. Neurobiol. Dis. 2014, 62, 338–353. [Google Scholar] [CrossRef]
- Yang, C.; Li, X.; Sun, L.; Guo, W.; Tian, W. Potential of human dental stem cells in repairing the complete transection of rat spinal cord. J. Neural Eng. 2017, 14, 026005. [Google Scholar] [CrossRef]
- Nagoshi, N.; Tsuji, O.; Nakamura, M.; Okano, H. Cell therapy for spinal cord injury using induced pluripotent stem cells. Regen. Ther. 2019, 11, 75–80. [Google Scholar] [CrossRef]
- Dwivedi, S.; Choudhary, P.; Gupta, A.; Singh, S. Therapeutical growth in oligodendroglial fate induction via transdifferentiation of stem cells for neuroregenerative therapy. Biochimie 2023, 211, 35–56. [Google Scholar] [CrossRef]
- Yu, L.; Liu, S.; Wang, C.; Zhang, C.; Wen, Y.; Zhang, K.; Shang, C.; Hu, H.; Liu, Y.; Wu, L.; et al. Embryonic stem cell-derived extracellular vesicles promote the recovery of kidney injury. Stem Cell Res. Ther. 2021, 12, 379. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.X.; Xia, T.; She, L.P.; Lin, S.; Luo, X.M. Stem cell therapies for human infertility: Advantages and challenges. Cell Transplant. 2022, 31, 09636897221083252. [Google Scholar] [CrossRef] [PubMed]
- Belviso, I.; Romano, V.; Nurzynska, D.; Castaldo, C.; Di Meglio, F. Non-integrating methods to produce induced pluripotent stem cells for regenerative medicine: An overview. In Biomechanics and Functional Tissue Engineering; IntechOpen: London, UK, 2020. [Google Scholar]
- Gorecka, J.; Kostiuk, V.; Fereydooni, A.; Gonzalez, L.; Luo, J.; Dash, B.; Isaji, T.; Ono, S.; Liu, S.; Lee, S.R.; et al. The potential and limitations of induced pluripotent stem cells to achieve wound healing. Stem Cell Res. Ther. 2019, 10, 87. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.P.; Hsiao, Y.J.; Chang, K.J.; Foustine, S.; Ko, Y.L.; Tsai, Y.C.; Tai, H.Y.; Ko, Y.C.; Chiou, S.H.; Lin, T.C.; et al. Pluripotent stem cells in clinical cell transplantation: Focusing on induced pluripotent stem cell-derived RPE cell therapy in age-related macular degeneration. Int. J. Mol. Sci. 2022, 23, 13794. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Okada, Y.; Itakura, G.; Iwai, H.; Nishimura, S.; Yasuda, A.; Nori, S.; Hikishima, K.; Konomi, T.; Fujiyoshi, K.; et al. Pre-evaluated safe human iPSC-derived neural stem cells promote functional recovery after spinal cord injury in common marmoset without tumorigenicity. PLoS ONE 2012, 7, e52787. [Google Scholar] [CrossRef]
- Shen, H.; Fan, C.; You, Z.; Xiao, Z.; Zhao, Y.; Dai, J. Advances in biomaterial-based spinal cord injury repair. Adv. Funct. Mater. 2022, 32, 2110628. [Google Scholar] [CrossRef]
- Lee, A.S.; Tang, C.; Rao, M.S.; Weissman, I.L.; Wu, J.C. Tumorigenicity as a clinical hurdle for pluripotent stem cell therapies. Nat. Med. 2013, 19, 998–1004. [Google Scholar] [CrossRef]
- Shamsian, A.; Sahebnasagh, R.; Norouzy, A.; Hussein, S.H.; Ghahremani, M.H.; Azizi, Z. Cancer cells as a new source of induced pluripotent stem cells. Stem Cell Res. Ther. 2022, 13, 459. [Google Scholar] [CrossRef]
- Paolini Sguazzi, G.; Muto, V.; Tartaglia, M.; Bertini, E.; Compagnucci, C. Induced pluripotent stem cells (iPSCs) and gene therapy: A new era for the treatment of neurological diseases. Int. J. Mol. Sci. 2021, 22, 13674. [Google Scholar] [CrossRef]
- Haridhasapavalan, K.K.; Borgohain, M.P.; Dey, C.; Saha, B.; Narayan, G.; Kumar, S.; Thummer, R.P. An insight into non-integrative gene delivery approaches to generate transgene-free induced pluripotent stem cells. Gene 2019, 686, 146–159. [Google Scholar] [CrossRef]
- Huang, Z.; Powell, R.; Phillips, J.B.; Haastert-Talini, K. Perspective on schwann cells derived from induced pluripotent stem cells in peripheral nerve tissue engineering. Cells 2020, 9, 2497. [Google Scholar] [CrossRef] [PubMed]
- Scesa, G.; Adami, R.; Bottai, D. iPSC preparation and epigenetic memory: Does the tissue origin matter? Cells 2021, 10, 1470. [Google Scholar] [CrossRef] [PubMed]
- Heo, J.S.; Choi, Y.; Kim, H.S.; Kim, H.O. Comparison of molecular profiles of human mesenchymal stem cells derived from bone marrow, umbilical cord blood, placenta and adipose tissue. Int. J. Mol. Med. 2016, 37, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Jiang, C.M.; An, S.; Cheng, Q.; Huang, Y.F.; Wang, Y.T.; Gou, Y.C.; Xiao, L.; Yu, W.J.; Wang, J.; et al. Immunomodulatory properties of dental tissue-derived mesenchymal stem cells. Oral Dis. 2014, 20, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Kandoi, S.; Misra, R.; Vijayalakshmi, S.; Rajagopal, K.; Verma, R.S. The mesenchymal stem cell secretome: A new paradigm towards cell-free therapeutic mode in regenerative medicine. Cytokine Growth Factor Rev. 2019, 46, 1–9. [Google Scholar]
- Shang, L.; Shao, J.; Ge, S. Immunomodulatory functions of oral mesenchymal stem cells: Novel force for tissue regeneration and disease therapy. J. Leukoc. Biol. 2021, 110, 539–552. [Google Scholar] [CrossRef]
- Lv, B.; Zhang, X.; Yuan, J.; Chen, Y.; Ding, H.; Cao, X.; Huang, A. Biomaterial-supported MSC transplantation enhances cell–cell communication for spinal cord injury. Stem Cell Res. Ther. 2021, 12, 36. [Google Scholar] [CrossRef]
- Zhang, Y.; Dong, N.; Hong, H.; Qi, J.; Zhang, S.; Wang, J. Mesenchymal stem cells: Therapeutic mechanisms for stroke. Int. J. Mol. Sci. 2022, 23, 2550. [Google Scholar] [CrossRef]
- Fan, L.; Liu, C.; Chen, X.; Zheng, L.; Zou, Y.; Wen, H.; Guan, P.; Lu, F.; Luo, Y.; Tan, G.; et al. Exosomes-Loaded Electroconductive Hydrogel Synergistically Promotes Tissue Repair after Spinal Cord Injury via Immunoregulation and Enhancement of Myelinated Axon Growth. Adv. Sci. 2022, 9, 2105586. [Google Scholar] [CrossRef]
- Pang, Q.M.; Deng, K.Q.; Zhang, M.; Wu, X.C.; Yang, R.L.; Fu, S.P.; Lin, F.Q.; Zhang, Q.; Ao, J.; Zhang, T. Multiple strategies enhance the efficacy of MSCs transplantation for spinal cord injury. Biomed. Pharmacother. 2023, 157, 114011. [Google Scholar] [CrossRef]
- Zheng, Q.; Zhang, S.; Guo, W.Z.; Li, X.K. The unique immunomodulatory properties of MSC-derived exosomes in organ transplantation. Front. Immunol. 2021, 12, 659621. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tang, Z.; Gu, P. Stem/progenitor cell-based transplantation for retinal degeneration: A review of clinical trials. Cell Death Dis. 2020, 11, 793. [Google Scholar] [CrossRef]
- Hu, C.; Li, L. Preconditioning influences mesenchymal stem cell properties in vitro and in vivo. J. Cell. Mol. Med. 2018, 22, 1428–1442. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, M.; Jung, Y.; Kim, S.H. Insight on stem cell preconditioning and instructive biomaterials to enhance cell adhesion, retention, and engraftment for tissue repair. Biomaterials 2016, 90, 85–115. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Chen, L.; Zeng, C.; Wang, W.E. Functionally improved mesenchymal stem cells to better treat myocardial infarction. Stem Cells Int. 2018, 2018, 7045245. [Google Scholar] [CrossRef]
- García-Sánchez, D.; Fernández, D.; Rodríguez-Rey, J.C.; Pérez-Campo, F.M. Enhancing survival, engraftment, and osteogenic potential of mesenchymal stem cells. World J. Stem Cells 2019, 11, 748. [Google Scholar] [CrossRef]
- Xu, B.; Yin, M.; Yang, Y.; Zou, Y.; Liu, W.; Qiao, L.; Zhang, J.; Wang, Z.; Wu, Y.; Shen, H.; et al. Transplantation of neural stem progenitor cells from different sources for severe spinal cord injury repair in rat. Bioact. Mater. 2023, 23, 300–313. [Google Scholar] [CrossRef]
- Finkel, Z.; Esteban, F.; Rodriguez, B.; Fu, T.; Ai, X.; Cai, L. Diversity of adult neural stem and progenitor cells in physiology and disease. Cells 2021, 10, 2045. [Google Scholar] [CrossRef]
- Pieczonka, K.; Fehlings, M.G. Incorporating combinatorial approaches to encourage targeted neural stem/progenitor cell integration following transplantation in spinal cord injury. Stem Cells Transl. Med. 2023, 12, 207–214. [Google Scholar] [CrossRef]
- Jeong, S.K.; Choi, I.; Jeon, S.R. Current status and future strategies to treat spinal cord injury with adult stem cells. J. Korean Neurosurg. Soc. 2020, 63, 153–162. [Google Scholar] [CrossRef]
- Yavarpour-Bali, H.; Nakhaei-Nejad, M.; Yazdi, A.; Ghasemi-Kasman, M. Direct conversion of somatic cells towards oligodendroglial lineage cells: A novel strategy for enhancement of myelin repair. J. Cell. Physiol. 2020, 235, 2023–2036. [Google Scholar] [CrossRef] [PubMed]
- Mothe, A.J.; Tator, C.H. Review of transplantation of neural stem/progenitor cells for spinal cord injury. Int. J. Dev. Neurosci. 2013, 31, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Pereira, I.M.; Marote, A.; Salgado, A.J.; Silva, N.A. Filling the gap: Neural stem cells as a promising therapy for spinal cord injury. Pharmaceuticals 2019, 12, 65. [Google Scholar] [CrossRef]
- Yuan, T.; Liu, Q.; Kang, J.; Gao, H.; Gui, S. High-dose neural stem/progenitor cell transplantation increases engraftment and neuronal distribution and promotes functional recovery in rats after acutely severe spinal cord injury. Stem Cells Int. 2019, 2019, 9807978. [Google Scholar] [CrossRef]
- Wang, X.; Rivera-Bolanos, N.; Jiang, B.; Ameer, G.A. Advanced functional biomaterials for stem cell delivery in regenerative engineering and medicine. Adv. Funct. Mater. 2019, 29, 1809009. [Google Scholar] [CrossRef]
- Liu, D.; Bobrovskaya, L.; Zhou, X.F. Cell therapy for neurological disorders: The perspective of promising cells. Biology 2021, 10, 1142. [Google Scholar] [CrossRef]
- Torres-Espín, A.; Hernández, J.; Navarro, X. Gene expression changes in the injured spinal cord following transplantation of mesenchymal stem cells or olfactory ensheathing cells. PLoS ONE 2013, 8, e76141. [Google Scholar] [CrossRef]
- Brennan, F.H.; Popovich, P.G. Emerging targets for reprograming the immune response to promote repair and recovery of function after spinal cord injury. Curr. Opin. Neurol. 2018, 31, 334–344. [Google Scholar] [CrossRef]
- Kang, E.S.; Ha, K.Y.; Kim, Y.H. Fate of transplanted bone marrow derived mesenchymal stem cells following spinal cord injury in rats by transplantation routes. J. Korean Med. Sci. 2012, 27, 586–593. [Google Scholar] [CrossRef]
- Allison, D.J.; Ditor, D.S. Immune dysfunction and chronic inflammation following spinal cord injury. Spinal Cord 2015, 53, 14–18. [Google Scholar] [CrossRef]
- Zhuang, X.; Hu, X.; Zhang, S.; Li, X.; Yuan, X.; Wu, Y. Mesenchymal stem cell–based therapy as a new approach for the treatment of systemic sclerosis. Clin. Rev. Allergy Immunol. 2022, 64, 284–320. [Google Scholar] [CrossRef] [PubMed]
- Hoang, D.M.; Pham, P.T.; Bach, T.Q.; Ngo, A.T.; Nguyen, Q.T.; Phan, T.T.; Nguyen, G.H.; Le, P.T.; Hoang, V.T.; Forsyth, N.R.; et al. Stem cell-based therapy for human diseases. Signal Transduct. Target. Ther. 2022, 7, 272. [Google Scholar] [CrossRef] [PubMed]
- Rheault-Henry, M.; White, I.; Grover, D.; Atoui, R. Stem cell therapy for heart failure: Medical breakthrough, or dead end? World J. Stem Cells 2021, 13, 236. [Google Scholar] [CrossRef]
- Attia, N.; Mashal, M.; Puras, G.; Pedraz, J.L. Mesenchymal stem cells as a gene delivery tool: Promise, problems, and prospects. Pharmaceutics 2021, 13, 843. [Google Scholar] [CrossRef]
- Kong, X.; Gao, J. Macrophage polarization: A key event in the secondary phase of acute spinal cord injury. J. Cell. Mol. Med. 2017, 21, 941–954. [Google Scholar] [CrossRef] [PubMed]
- Zipser, C.M.; Cragg, J.J.; Guest, J.D.; Fehlings, M.G.; Jutzeler, C.R.; Anderson, A.J.; Curt, A. Cell-based and stem-cell-based treatments for spinal cord injury: Evidence from clinical trials. Lancet Neurol. 2022, 21, 659–670. [Google Scholar] [CrossRef]
- Okano, H.; Ogawa, Y.; Nakamura, M.; Kaneko, S.; Iwanami, A.; Toyama, Y. Transplantation of neural stem cells into the spinal cord after injury. In Seminars in Cell Developmental Biology; Academic Press: Cambridge, MA, USA, 2003; Volume 14, Number 3, pp. 191–198. [Google Scholar]
- Syková, E.; Homola, A.; Mazanec, R.; Lachmann, H.; Konrádová, Š.L.; Kobylka, P.; Pádr, R.; Neuwirth, J.; Komrska, V.; Vávra, V.; et al. Autologous bone marrow transplantation in patients with subacute and chronic spinal cord injury. Cell Transplant. 2006, 15, 675–687. [Google Scholar] [CrossRef]
- Dai, G.; Liu, X.; Zhang, Z.; Wang, X.; Li, M.; Cheng, H.; Hua, R.; Shi, J.; Wang, R.; Qin, C.; et al. Comparative analysis of curative effect of CT-guided stem cell transplantation and open surgical transplantation for sequelae of spinal cord injury. J. Transl. Med. 2013, 11, 315. [Google Scholar] [CrossRef]
- Kharbikar, B.N.; Mohindra, P.; Desai, T.A. Biomaterials to enhance stem cell transplantation. Cell Stem Cell 2022, 29, 692–721. [Google Scholar] [CrossRef]
- Smith, L.J.; Silverman, L.; Sakai, D.; Le Maitre, C.L.; Mauck, R.L.; Malhotra, N.R.; Lotz, J.C.; Buckley, C.T. Advancing cell therapies for intervertebral disc regeneration from the lab to the clinic: Recommendations of the ORS spine section. JOR Spine 2018, 1, e1036. [Google Scholar] [CrossRef]
- Riha, S.M.; Maarof, M.; Fauzi, M.B. Synergistic effect of biomaterial and stem cell for skin tissue engineering in cutaneous wound healing: A concise review. Polymers 2021, 13, 1546. [Google Scholar] [CrossRef]
- Vonk, L.A.; De Windt, T.S.; Slaper-Cortenbach, I.C.; Saris, D.B. Autologous, allogeneic, induced pluripotent stem cell or a combination stem cell therapy? Where are we headed in cartilage repair and why: A concise review. Stem Cell Res. Ther. 2015, 6, 94. [Google Scholar] [CrossRef] [PubMed]
- Pajer, K.; Bellák, T.; Redl, H.; Nógrádi, A. Neuroectodermal stem cells grafted into the injured spinal cord induce both axonal regeneration and morphological restoration via multiple mechanisms. J. Neurotrauma 2019, 36, 2977–2990. [Google Scholar] [CrossRef] [PubMed]
- Stenudd, M.; Sabelström, H.; Frisén, J. Role of endogenous neural stem cells in spinal cord injury and repair. JAMA Neurol. 2015, 72, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; Moyo, B.; Lee, C.M.; Leong, K.; Bao, G. Engineered materials for in vivo delivery of genome-editing machinery. Nat. Rev. Mater. 2019, 4, 726–737. [Google Scholar] [CrossRef]
- Lee, J.; Bayarsaikhan, D.; Bayarsaikhan, G.; Kim, J.S.; Schwarzbach, E.; Lee, B. Recent advances in genome editing of stem cells for drug discovery and therapeutic application. Pharmacol. Ther. 2020, 209, 107501. [Google Scholar] [CrossRef]
- Ferrari, G.; Thrasher, A.J.; Aiuti, A. Gene therapy using haematopoietic stem and progenitor cells. Nat. Rev. Genet. 2021, 22, 216–234. [Google Scholar] [CrossRef]
- Hussey, G.S.; Dziki, J.L.; Badylak, S.F. Extracellular matrix-based materials for regenerative medicine. Nat. Rev. Mater. 2018, 3, 159–173. [Google Scholar] [CrossRef]
- Wang, J.; Kong, X.; Li, Q.; Li, C.; Yu, H.; Ning, G.; Xiang, Z.; Liu, Y.; Feng, S. The spatial arrangement of cells in a 3D-printed biomimetic spinal cord promotes directional differentiation and repairs the motor function after spinal cord injury. Biofabrication 2021, 13, 045016. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, X.; Janairo, R.R.R.; Kwong, G.; Tsou, A.D.; Chu, J.S.; Wang, A.; Yu, J.; Wang, D.; Li, S. Matrix stiffness modulates the differentiation of neural crest stem cells in vivo. J. Cell. Physiol. 2019, 234, 7569–7578. [Google Scholar] [CrossRef]
- Deng, W.S.; Ma, K.; Liang, B.; Liu, X.Y.; Xu, H.Y.; Zhang, J.; Shi, H.; Sun, H.; Chen, X.; Zhang, S. Collagen scaffold combined with human umbilical cord-mesenchymal stem cells transplantation for acute complete spinal cord injury. Neural Regen. Res. 2020, 15, 1686. [Google Scholar] [PubMed]
- Schira, J.; Gasis, M.; Estrada, V.; Hendricks, M.; Schmitz, C.; Trapp, T.; Kruse, F.; Kögler, G.; Wernet, P.; Hartung, H.; et al. Significant clinical, neuropathological and behavioural recovery from acute spinal cord trauma by transplantation of a well-defined somatic stem cell from human umbilical cord blood. Brain 2012, 135, 431–446. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, J.V.; Gillett, G.R. Ethics, stem cells and spinal cord repair. Med. J. Aust. 2004, 180, 637–639. [Google Scholar] [CrossRef]
- Hashimoto, S.; Nagoshi, N.; Shinozaki, M.; Nakanishi, K.; Suematsu, Y.; Shibata, T.; Kawai, M.; Kitagawa, T.; Ago, K.; Kamata, Y.; et al. Microenvironmental modulation in tandem with human stem cell transplantation enhances functional recovery after chronic complete spinal cord injury. Biomaterials 2023, 295, 122002. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Tashiro, S.; Shibata, S.; Shinozaki, M.; Shindo, T.; Hashimoto, S.; Kawai, M.; Kitagawa, T.; Ago, K.; Matsumoto, M.; et al. Rehabilitative training enhances therapeutic effect of human-iPSC-derived neural stem/progenitor cells transplantation in chronic spinal cord injury. Stem Cells Transl. Med. 2023, 12, 83–96. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Data | Country/Region | Age Group Most Affected | Primary Causes of Injury | Notable Trends | Year | Reference | |
|---|---|---|---|---|---|---|---|
| Incidence Rates | 32–50 per million requiring hospital admission | United States | N/A | N/A | N/A | 2000 | [5] |
| 11.4 per million | Spain | 60–69 years | Tumors | N/A | 2012 | [6] | |
| 19.4 per million inhabitants | France | N/A | N/A | N/A | 2005 | [7] | |
| Stable incidence rate, changes in injury etiology | Stockholm, Sweden | N/A | Falls, Transport-related | N/A | 2017 | [8] | |
| 23 cases per 1,000,000 persons | Global | N/A | N/A | N/A | 2007 | [9] | |
| Prevalence | Estimate provided, further refinements needed | Victoria, Australia | N/A | N/A | N/A | 2012 | [10] |
| Demographic Trends | Increased incidence due to falls and motor vehicle accidents | Global | N/A | Falls, Motor Accidents | Increasing | 2010 | [11] |
| Increased incidence in the elderly | Global | Elderly | Falls, Non-traumatic | Increasing | 2010 | [12] | |
| Mean age at injury increased | Finland | N/A | N/A | Increasing | 2008 | [13] | |
| Specific epidemiological characteristics | Xi’an, China | N/A | N/A | N/A | 2020 | [14] | |
| Global Trends | Significant variation in incidence worldwide | Global | N/A | N/A | Varies | 2010 | [11] |
| Variation in etiology, male-to-female ratios, age distributions, and complications | Global | N/A | N/A | Varies | 2004 | [15] |
| Stem Cell Type | Advantages | Challenges | References |
|---|---|---|---|
| Embryonic Stem Cells (ESCs) |
|
| [52,56,57,58] |
| Induced Pluripotent Stem Cells (iPSCs) |
|
| [66,67,68,69] |
| Mesenchymal Stem Cells (MSCs) |
|
| [70,71,72,73,74,75] |
| Neural Stem/Progenitor Cells (NSPCs) |
|
| [76,77,78,79,80] |
| Stem Cell Type | Advantages | Existing Challenges | Possible Solutions |
|---|---|---|---|
| Embryonic Stem Cells (ESCs) |
|
|
|
| Induced Pluripotent Stem Cells (iPSCs) |
|
|
|
| Mesenchymal Stem Cells (MSCs) |
|
|
|
| Neural Stem/Progenitor Cells (NSPCs) |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, C.-W. Advancing Spinal Cord Injury Treatment through Stem Cell Therapy: A Comprehensive Review of Cell Types, Challenges, and Emerging Technologies in Regenerative Medicine. Int. J. Mol. Sci. 2023, 24, 14349. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241814349
Zeng C-W. Advancing Spinal Cord Injury Treatment through Stem Cell Therapy: A Comprehensive Review of Cell Types, Challenges, and Emerging Technologies in Regenerative Medicine. International Journal of Molecular Sciences. 2023; 24(18):14349. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241814349
Chicago/Turabian StyleZeng, Chih-Wei. 2023. "Advancing Spinal Cord Injury Treatment through Stem Cell Therapy: A Comprehensive Review of Cell Types, Challenges, and Emerging Technologies in Regenerative Medicine" International Journal of Molecular Sciences 24, no. 18: 14349. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241814349