
Increase of Circulating Endothelial Progenitor Cells and Released Angiogenic Factors in Children with Moyamoya Arteriopathy
 , , , , , , , , , ,
, , , , , , , , , ,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Recruitment of MMA Pediatric Patients and Unrelated Pediatric Subjects
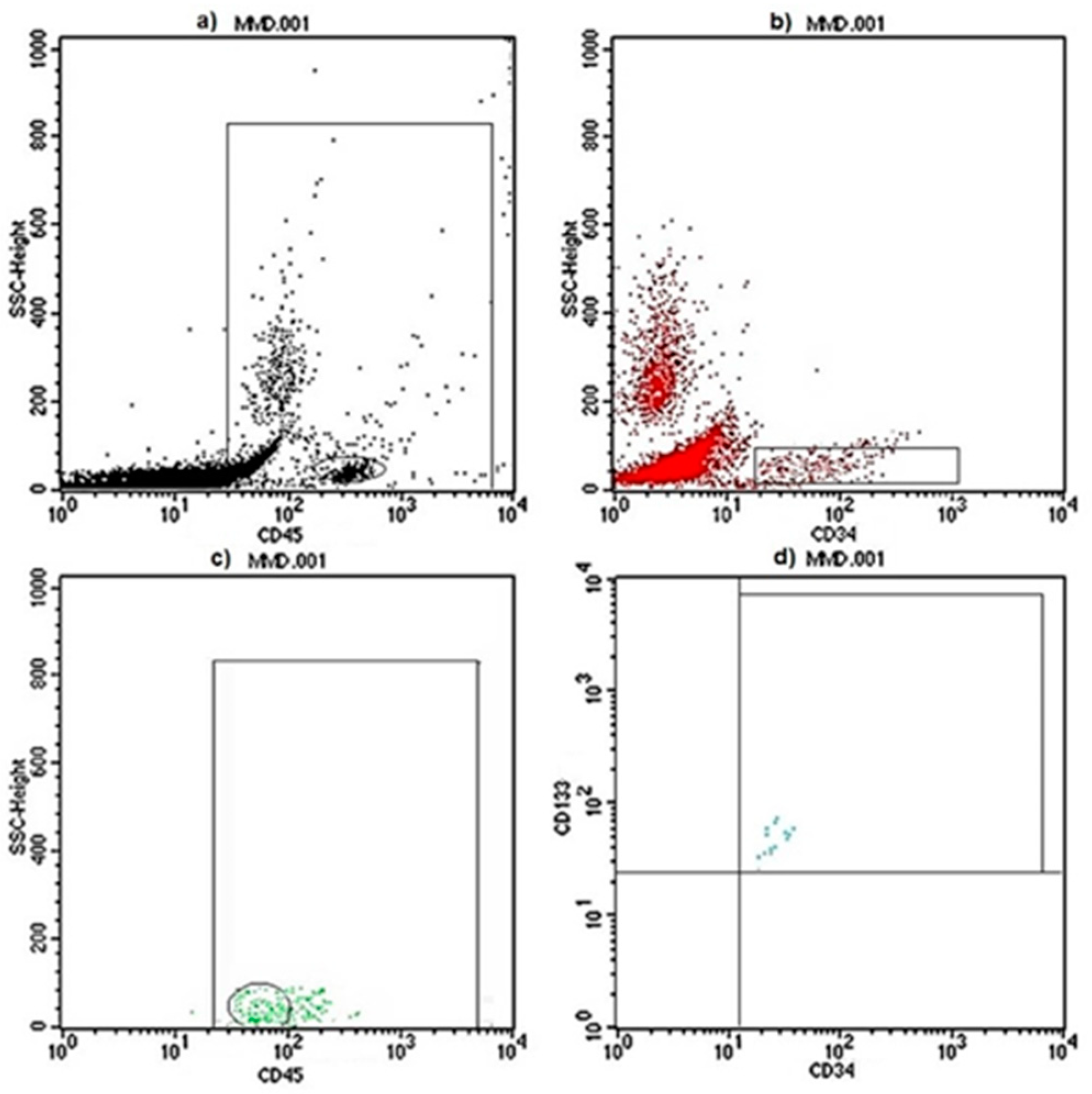
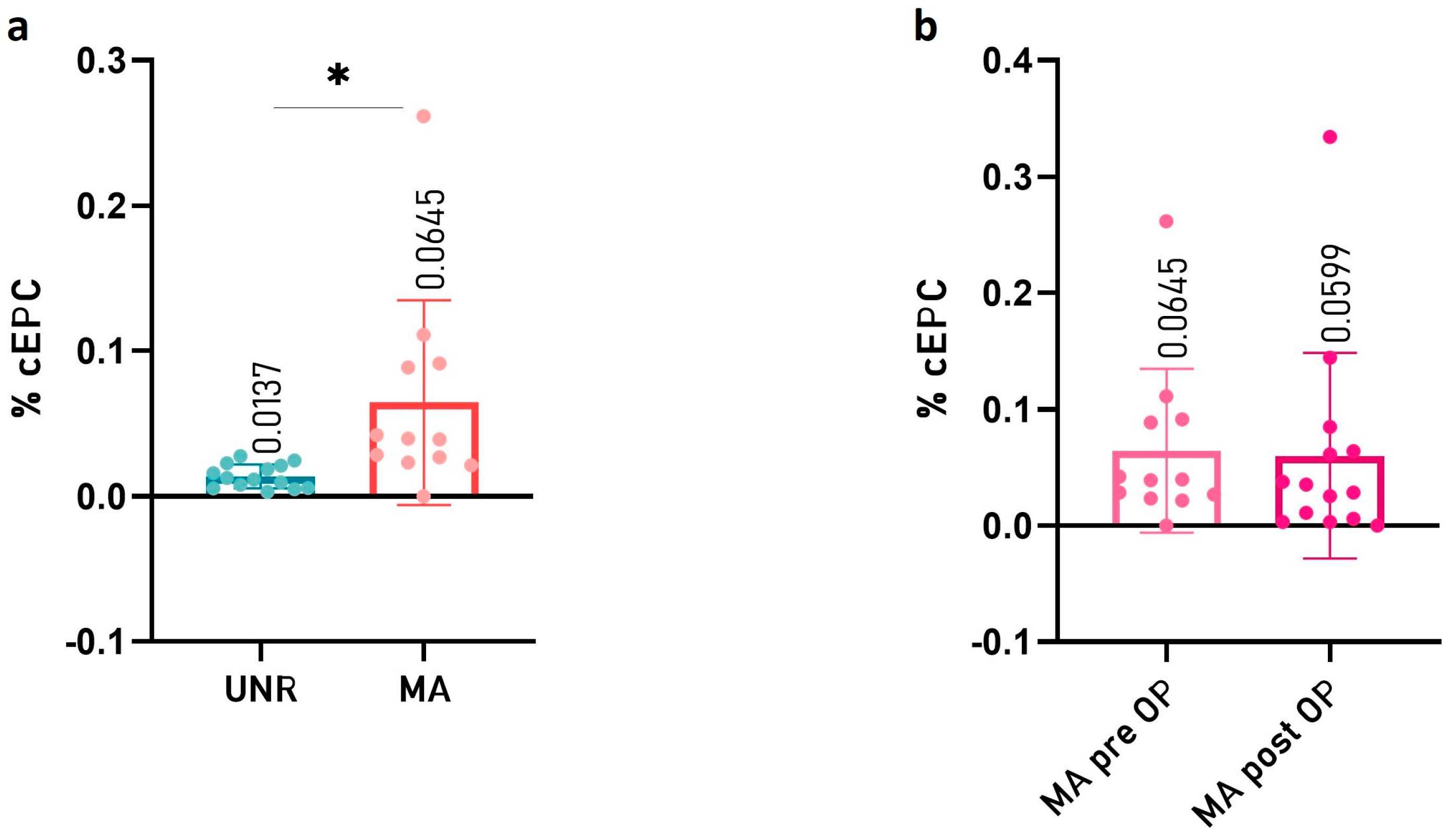
2.2. Circulating Endothelial Progenitor Cell (cEPC) Levels Are Increased in Peripheral Blood of Children with MMA
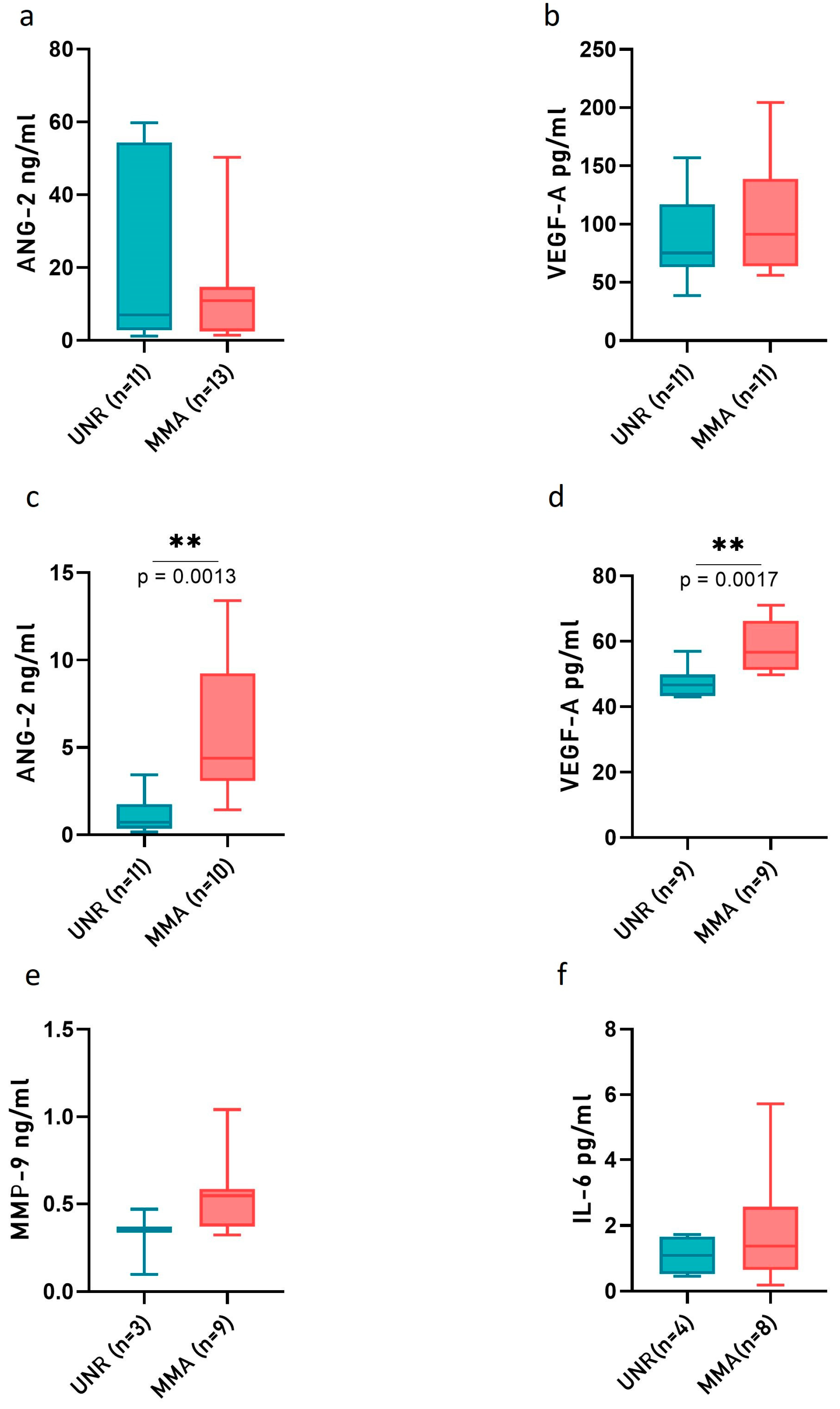
2.3. Angiopoietin-2 (ANG-2) and VEGF-A Level Are Increased in CSF of MMA Pediatric Patients
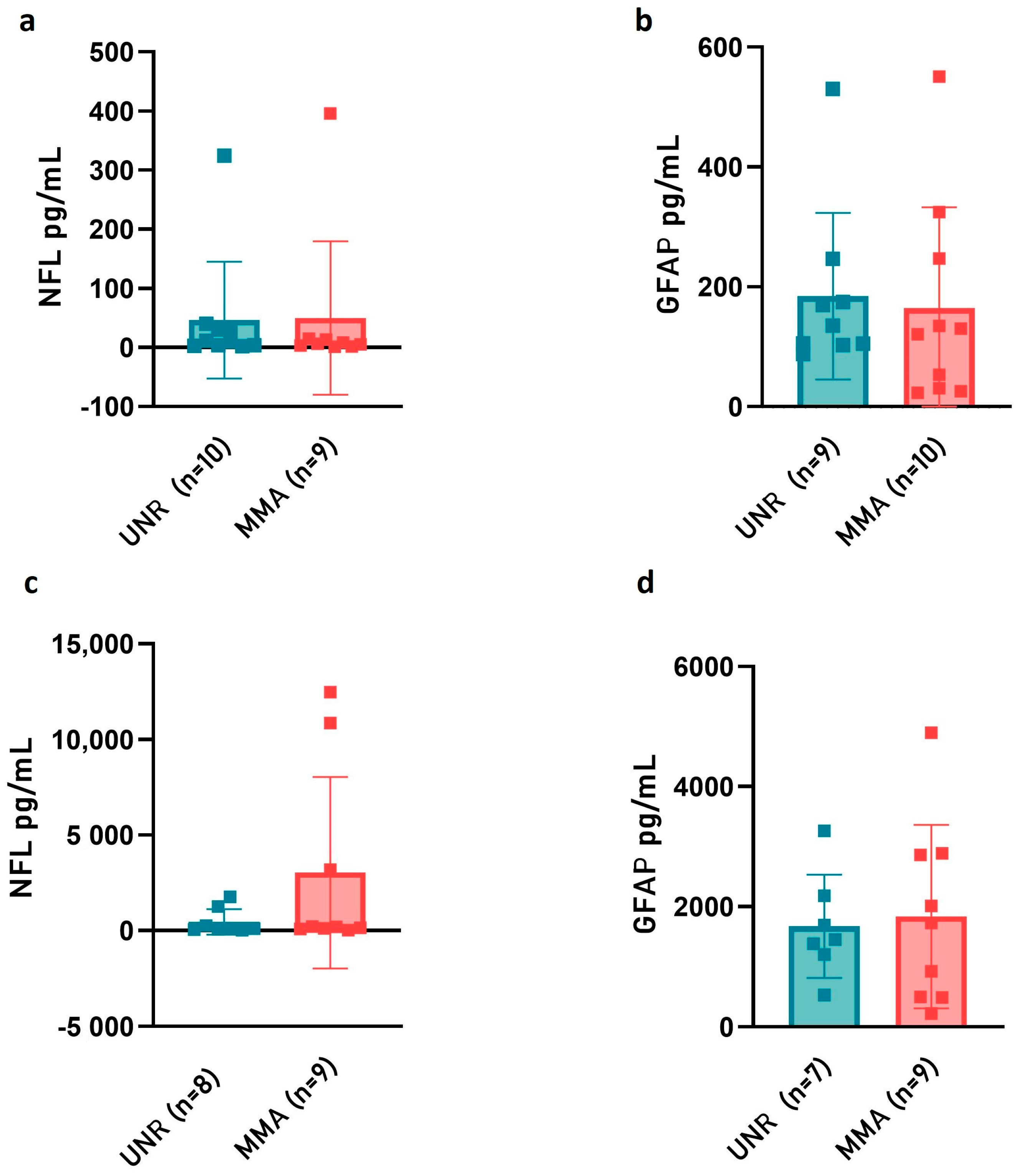
2.4. Neurofilament Light (NfL) and Glial Fibrillary Acidic Protein (GFAP) Release in Plasma and CSF of MMA Pediatric Patients
3. Discussion
4. Materials and Methods
4.1. Moyamoya Patients and Unrelated Controls: Inclusion Criteria
4.2. Ethical Issues
4.3. Peripheral Blood, Plasma and CSF Sample Collection
4.4. Clinical–Radiological Factors
4.5. Flow Cytometry Analysis
4.6. ELISA
4.7. SIMOA Ultra-Sensitive Digital Immunoassay for NF-Light and GFAP (Single Molecule Array SiMoA™)
4.8. Statistics and Data Visualization
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANG-2 | Angiopoietin-2 |
| cEPCs | Circulating endothelial progenitor cells |
| CSF | Cerebrospinal Fluid |
| CVD | Cerebrovascular disease |
| CV | Coefficient of variation |
| DEGs | Differentially expressed genes |
| F | Female |
| FACS | Fluorescence-activated cell sorting |
| GFAP | Glial Fibrillary acidic protein |
| ICAs | Internal carotid arteries |
| IL-6 | Interleukin 6 |
| LP | Lumbar Puncture |
| M | Male |
| MCA | Middle Cerebral Artery |
| MMA | Moyamoya arteriopathy |
| MMP-9 | Metalloproteinase-9 |
| NfL | Neurofilament light chain |
| RNAseq | RNA sequencing |
| RNF213 | Ring Finger Protein 213 |
| STA | Superficial temporal artery |
| SiMoA | Single molecule array |
| TIA | Transient ischemic attack |
| UNR | Unrelated controls |
| VEGF-A | Vascular endothelial growth factor-A |
| WBC | White blood cells |
References
- Fukui, M. Guidelines for the diagnosis and treatment of spontaneous occlusion of the circle of Willis (‘moyamoya’ disease). Research Committee on Spontaneous Occlusion of the Circle of Willis (Moyamoya Disease) of the Ministry of Health and Welfare, Japan. Clin. Neurol. Neurosurg. 1997, 99 (Suppl. 2), S238–S240. [Google Scholar] [CrossRef] [PubMed]
- Bersano, A.; Guey, S.; Bedini, G.; Nava, S.; Hervé, D.; Vajkoczy, P.; Tatlisumak, T.; Sareela, M.; van der Zwan, A.; Klijn, C.J.; et al. European Moyamoya Disease Initiative (2016). Research Progresses in Understanding the Pathophysiology of Moyamoya Disease. Cerebrovasc. Dis. 2016, 41, 105–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kossorotoff, M.; Tournier-Lasserve, E.; Herve, D.; Guey, S. Moyamoya disease and syndromes: From genetics to clinical management. Appl. Clin. Genet. 2015, 8, 49–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, E.; Saeki, N.; Oishi, H.; Hirai, S.; Yamaura, A. Long-term natural history of hemorrhagic type moyamoya disease in 42 patients. J. Neurosurg. 2000, 93, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, M.; Heienbrok, W.; Berlit, P. Moyamoya Disease in Europeans. Stroke 2008, 39, 3193–3200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acker, G.; Goerdes, S.; Schneider, U.C.; Schmiedek, P.; Czabanka, M.; Vajkoczy, P. Distinct clinical and radiographic characteristics of moyamoya disease amongst European Caucasians. Eur. J. Neurol. 2015, 22, 1012–1017. [Google Scholar] [CrossRef] [PubMed]
- Feghali, J.; Xu, R.; Yang, W.; Liew, J.; Tamargo, R.J.; Marsh, E.B.; Huang, J. Racial phenotypes in moyamoya disease: A comparative analysis of clinical presentation and natural history in a single multiethnic cohort of 250 hemispheres. J. Neurosurg. 2019, 1–7. [Google Scholar] [CrossRef]
- Wakai, K.; Tamakoshi, A.; Ikezaki, K.; Fukui, M.; Kawamura, T.; Aoki, R.; Kojima, M.; Lin, Y.; Ohno, Y. Epidemiological features of moyamoya disease in Japan: Findings from a nationwide survey. Clin. Neurol. Neurosurg. 1997, 99 (Suppl. 2), S1–S5. [Google Scholar] [CrossRef]
- Baba, T.; Houkin, K.; Kuroda, S. Novel epidemiological features of moyamoya disease. J. Neurol. Neurosurg. Psychiatry 2008, 79, 900–904. [Google Scholar] [CrossRef]
- Houkin, K.; Ito, M.; Sugiyama, T.; Shichinohe, H.; Nakayama, N.; Kazumata, K.; Kuroda, S. Review of past research and current concepts on the etiology of moyamoya disease. Neurol. Med. Chir. 2012, 52, 267–277. [Google Scholar] [CrossRef]
- Bedini, G.; Blecharz, K.; Nava, S.; Vajkoczy, P.; Alessandri, G.; Ranieri, M.; Acerbi, F.; Ferroli, P.; Riva, D.; Esposito, S.; et al. Vasculogenic and Angiogenic Pathways in Moyamoya Disease. Curr. Med. Chem. 2016, 23, 315–345. [Google Scholar] [CrossRef] [PubMed]
- Kamada, F.; Aoki, Y.; Narisawa, A.; Abe, Y.; Komatsuzaki, S.; Kikuchi, A.; Kanno, J.; Niihori, T.; Ono, M.; Ishii, N.; et al. A genome-wide association study identifies RNF213 as the first Moyamoya disease gene. J. Hum. Genet. 2011, 56, 34–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guey, S.; Kraemer, M.; Herve, D.; Ludwig, T.E.; Kossorotoff, M.; Bergametti, F.; Schwitalla, J.C.; Choi, S.; Broseus, L.; Callebaut, I.; et al. Rare RNF213 variants in the C-terminal region encompassing the RING-finger domain are associated with moyamoya angiopathy in Caucasians. Eur. J. Hum. Genet. 2017, 25, 995–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raso, A.; Biassoni, R.; Mascelli, S.; Nozza, P.; Ugolotti, E.; Di Marco, E.; De Marco, P.; Merello, E.; Cama, A.; Pavanello, M.; et al. Moyamoya vasculopathy shows a genetic mutational gradient decreasing from East to West. J. Neurosurg. Sci. 2020, 64, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Fallen, S.; Zhou, Y.; Baxter, D.; Scherler, K.; Kuo, M.F.; Wang, K. The impact of moyamoya disease and RNF213 Mutations on the spectrum of plasma protein and microRNA. J. Clin. Med. 2019, 8, 1648. [Google Scholar] [CrossRef] [Green Version]
- Takeda, M.; Tezuka, T.; Kim, M.; Choi, J.; Oichi, Y.; Kobayashi, H.; Harada, K.H.; Mizushima, T.; Taketani, S.; Koizumi, A.; et al. Moyamoya disease patient mutations in the RING domain of RNF213 reduce its ubiquitin ligase activity and enhance NFκB activation and apoptosis in an AAA+ domain-dependent manner. Biochem. Biophys. Res. Commun. 2020, 525, 668–674. [Google Scholar] [CrossRef]
- Mertens, R.; Graupera, M.; Gerhardt, H.; Bersano, A.; Tournier-Lasserve, E.; Mensah, M.A.; Mundlos, S.; Vajkoczy, P. The Genetic Basis of Moyamoya Disease. Transl. Stroke Res. 2021, 13, 25–45. [Google Scholar] [CrossRef]
- Piccolis, M.; Bond, L.M.; Kampmann, M.; Pulimeno, P.; Chitraju, C.; Jayson, C.B.K.; Vaites, L.P.; Boland, S.; Lai, Z.W.; Gabriel, K.R.; et al. Probing the Global Cellular Responses to Lipotoxicity Caused by Saturated Fatty Acids. Mol. Cell. 2019, 74, 32–44. [Google Scholar] [CrossRef] [Green Version]
- Mineharu, Y.; Miyamoto, S. RNF213 and GUCY1A3 in Moyamoya Disease: Key Regulators of Metabolism, Inflammation, and Vascular Stability. Front. Neurol. 2021, 12, 687088. [Google Scholar] [CrossRef]
- Banh, R.S.; Iorio, C.; Marcotte, R.; Xu, Y.; Cojocari, D.; Rahman, A.A.; Pawling, J.; Zhang, W.; Sinha, A.; Rose, C.M.; et al. PTP1B controls non-mitochondrial oxygen consumption by regulating RNF213 to promote tumour survival during hypoxia. Nat. Cell Biol. 2016, 18, 803–813. [Google Scholar] [CrossRef]
- Pollaci, G.; Gorla, G.; Potenza, A.; Carrozzini, T.; Canavero, I.; Bersano, A.; Gatti, L. Novel Multifaceted Roles for RNF213 Protein. Int. J. Mol. Sci. 2022, 23, 4492. [Google Scholar] [CrossRef] [PubMed]
- Fox, B.M.; Dorschel, K.B.; Lawton, M.T.; Wanebo, J.E. Pathophysiology of Vascular Stenosis and Remodeling in Moyamoya Disease. Front. Neurol. 2021, 12, 661578. [Google Scholar] [CrossRef]
- Kuriyama, S.; Kusaka, Y.; Fujimura, M.; Wakai, K.; Tamakoshi, A.; Hashimoto, S.; Tsuji, I.; Inaba, Y.; Yoshimoto, T. Prevalence and clinic-epidemiological features of Moyamoya disease in Japan: Findings from a nationwide epidemiological survey. Stroke 2008, 39, 42–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amlie-Lefond, C.; Bernard, T.J.; Sébire, G.; Friedman, N.R.; Heyer, G.L.; Lerner, N.B.; DeVeber, G.; Fullerton, H.J. International Pediatric Stroke Study Group Predictors of cerebral arteriopathy in children with arterial ischemic stroke: Results of the International Pediatric Stroke Study. Circulation 2009, 119, 1417–1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, R.M.; Smith, J.L.; Robertson, R.L.; Madsen, J.R.; Soriano, S.G.; Rockoff, M.A. Long-term outcome in children with moyamoya syndrome after cranial revascularization by pial synangiosis. J. Neurosurg. 2004, 100, 142–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Sharydah, A.M.; Al-Arfaj, H.K.; Al-Suhibani, S.S.; Al-Safran, F.S.; Al-Abdulwahhab, A.H.; Al-Jubran, S.A.; AlSaflan, A.A. Pediatric Stroke from Bench to Bedside: A Single-Center Experience in Saudi Arabia. Vasc. Health Risk Manag. 2022, 18, 529–540. [Google Scholar] [CrossRef]
- Hackenberg, A.; Battilana, B.; Hebeisen, M.; Steinfeld, R.; Khan, N. Preoperative clinical symptomatology and stroke burden in pediatric moyamoya angiopathy: Defining associated risk variables. Eur. J. Paediatr. Neurol. 2021, 35, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Rivkin, M.J.; Kirton, A.; de Veber, G.; Elbers, J.; International Pediatric Stroke Study. Moyamoya Disease in Children: Results from the International Pediatric Stroke Study. J. Child Neurol. 2017, 32, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Kong, H.; Wang, Y.; Jin, P.; Ding, J.; Li, H.; Wang, H.; Zhuo, Z. A Retrospective Study on Clinical Features of Childhood Moyamoya Disease. Pediatr. Neurol. 2022, 138, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Yu, L.B.; Dai, K.F.; Zhang, Y.; Wang, R.; Zhang, D. Clinical Features, Surgical Treatment, and Long-Term Outcome of a Multicenter Cohort of Pediatric Moyamoya. Front. Neurol. 2019, 10, 14. [Google Scholar] [CrossRef]
- Maruwaka, M.; Yoshikawa, K.; Okamoto, S.; Araki, Y.; Sumitomo, M.; Kawamura, A.; Yokoyama, K.; Wakabayashi, T. Biomarker research for moyamoya disease in cerebrospinal fluid using surface-enhanced laser desorption/ionization time-of-flight mass spectrometry. J. Stroke Cerebrovasc. Dis. 2015, 24, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Sesen, J.; Driscoll, J.; Moses-Gardner, A.; Orbach, D.B.; Zurakowski, D.; Smith, E.R. Non-invasive Urinary Biomarkers in Moyamoya Disease. Front. Neurol. 2021, 12, 661952. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Moon, Y.J.; Lee, H.O.; Park, A.K.; Choi, S.A.; Wang, K.C.; Han, J.W.; Joung, J.G.; Kang, H.S.; Kim, J.E.; et al. Deregulation of Retinaldehyde Dehydrogenase 2 Leads to Defective Angiogenic Function of Endothelial Colony-Forming Cells in Pediatric Moyamoya Disease. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1670–1677. [Google Scholar] [CrossRef] [Green Version]
- Tinelli, F.; Nava, S.; Arioli, F.; Bedini, G.; Scelzo, E.; Lisini, D.; Faragò, G.; Gioppo, A.; Ciceri, E.F.; Acerbi, F.; et al. Vascular Remodeling in Moyamoya Angiopathy: From Peripheral Blood Mononuclear Cells to Endothelial Cells. Int. J. Mol. Sci. 2020, 21, 5763. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.A.; Chong, S.; Kwak, P.A.; Moon, Y.J.; Jangra, A.; Phi, J.H.; Lee, J.Y.; Park, S.H.; Kim, S.K. Impaired functional recovery of endothelial colony-forming cells from moyamoya disease in a chronic cerebral hypoperfusion rat model. J. Neurosurg. Pediatr. 2018, 23, 204–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Jung, J.H.; Phi, J.H.; Kang, H.S.; Kim, J.E.; Chae, J.H.; Kim, S.J.; Kim, Y.H.; Kim, Y.Y.; Cho, B.K.; et al. Decreased level and defective function of circulating endothelial progenitor cells in children with moyamoya disease. J. Neurosci. Res. 2010, 88, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Shibuya, M. Vascular endothelial growth factor and its receptor system: Physiological functions in angiogenesis and pathological roles in various diseases. J. Biochem. 2013, 153, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Scholz, A.; Plate, K.H.; Reiss, Y. Angiopoietin-2: A multifaceted cytokine that functions in both angiogenesis and inflammation. Ann. N. Y. Acad. Sci. 2015, 1347, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Coelho, A.L.; Gomes, M.P.; Catarino, R.J.; Rolfo, C.; Lopes, A.M.; Medeiros, R.M.; Araújo, A.M. Angiogenesis in NSCLC: Is vessel co-option the trunk that sustains the branches? Oncotarget 2017, 8, 39795–39804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blecharz, K.G.; Frey, D.; Schenkel, T.; Prinz, V.; Bedini, G.; Krug, S.M.; Czabanka, M.; Wagner, J.; Fromm, M.; Bersano, A.; et al. Autocrine release of angiopoietin-2 mediates cerebrovascular disintegration in Moyamoya disease. J. Cereb. Blood Flow Metab. 2017, 37, 1527–1539. [Google Scholar] [CrossRef]
- Yu, J.; Huang, K.; Pan, J.; Shen, J.; Zhan, R. Significance of Serum Angiopoietin-2 in Patients with Hemorrhage in Adult-Onset Moyamoya Disease. BioMed Res. Int. 2020, 2020, 8209313. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, M.; Watanabe, M.; Narisawa, A.; Shimizu, H.; Tominaga, T. Increased expression of serum Matrix Metalloproteinase-9 in patients with moyamoya disease. Surg. Neurol. 2009, 72, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Wang, J.; Lin, Z.; Shi, G.; Wang, R.; Zhao, Y.; Zhao, Y.; Zhao, J. MMP-9 as a Biomarker for Predicting Hemorrhagic Strokes in Moyamoya Disease. Front. Neurol. 2021, 12, 721118. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Wei, W.; Zhang, F.; Chen, T.; Dong, L.; Shi, J.; Wu, X.; Zhang, T.; Li, Z.; Zhang, J.; et al. Transcriptomic Profiling of Intracranial Arteries in Adult Patients With Moyamoya Disease Reveals Novel Insights Into Its Pathogenesis. Front. Mol. Neurosci. 2022, 15, 881954. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Zhang, Z.; Ye, D.; Xing, P.; Zou, Z.; Lei, H.; Duan, L. Gene dysregulation in peripheral blood of moyamoya disease and comparison with other vascular disorders. PLoS ONE 2019, 14, e0221811. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Nishimoto, N.; Yoshizaki, K.; Tagoh, H.; Monden, M.; Kishimoto, S.; Hirano, T.; Kishimoto, T. Elevation of serum interleukin 6 prior to acute phase proteins on the inflammation by surgical operation. Clin. Immunol. Immunopathol. 1989, 50, 399–401. [Google Scholar] [CrossRef]
- Zhao, L.; Li, T.; Xue, B.; Liang, H.; Zhang, S.; Wu, R.; Guo, G.; Gao, T.; Liu, Y.; Sun, Y.; et al. Influence of Autologous Bone Marrow Stem Cell Therapy on the Levels of Inflammatory Factors and Conexin43 of Patients with Moyamoya Disease. Comput. Intell. Neurosci. 2022, 2022, 7620287. [Google Scholar] [CrossRef]
- Han, W.; Qiao, Y.; Zhang, H.; Geng, C.; Zhu, X.; Liao, D.; Guo, Y.; Yang, M.; Chen, D.; Jiang, P. Circulating sortilin levels are associated with inflammation in patients with moyamoya disease. Metab. Brain Dis. 2021, 36, 103–109. [Google Scholar] [CrossRef]
- Bersano, A.; Bedini, G.; Nava, S.; Acerbi, F.; Sebastiano, D.R.; Binelli, S.; Franceschetti, S.; Faragò, G.; Grisoli, M.; Gioppo, A.; et al. GEN-O-MA study group. GEN-O-MA project: An Italian network studying clinical course and pathogenic pathways of moyamoya disease-study protocol and preliminary results. Neurol. Sci. 2019, 40, 561–570. [Google Scholar] [CrossRef]
- Dei Cas, M.; Carrozzini, T.; Pollaci, G.; Potenza, A.; Nava, S.; Canavero, I.; Tinelli, F.; Gorla, G.; Vetrano, I.G.; Acerbi, F.; et al. Plasma Lipid Profiling Contributes to Untangle the Complexity of Moyamoya Arteriopathy. Int. J. Mol. Sci. 2021, 22, 13410. [Google Scholar] [CrossRef]
- Kang, H.S.; Moon, Y.J.; Kim, Y.Y.; Park, W.Y.; Park, A.K.; Wang, K.C.; Kim, J.E.; Phi, J.H.; Lee, J.Y.; Kim, S.K. Smooth-muscle progenitor cells isolated from patients with moyamoya disease: Novel experimental cell model. J. Neurosurg. 2014, 120, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; Wang, K.C.; Kim, S.K. Circulating Vascular Progenitor Cells in Moyamoya Disease. J. Korean Neurosurg. Soc. 2015, 57, 428–431. [Google Scholar] [CrossRef]
- Yoshihara, T.; Taguchi, A.; Matsuyama, T.; Shimizu, Y.; Kikuchi-Taura, A.; Soma, T.; Stern, D.M.; Yoshikawa, H.; Kasahara, Y.; Moriwaki, H.; et al. Increase in circulating CD34-positive cells in patients with angiographic evidence of moyamoya-like vessels. J. Cereb. Blood Flow Metab. 2008, 28, 1086–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, G.; Liu, W.; Huang, X.; Zhu, S.; Yue, X.; Chen, Z.; Chen, M.; Liu, X.; Xu, G. Increased levels of circulating SDF-1α and CD34+ CXCR4+ cells in patients with moyamoya disease. Eur. J. Neurol. 2011, 18, 1304–1309. [Google Scholar] [CrossRef] [PubMed]
- Amlie-Lefond, C.; Ellenbogen, R.G. Factors associated with the presentation of moyamoya in childhood. J. Stroke Cerebrovasc. Dis. 2015, 24, 1204–1210. [Google Scholar] [CrossRef] [PubMed]
- Gatti, J.R.; Torriente, A.G.; Sun, L.R. Clinical Presentation and Stroke Incidence Differ by Moyamoya Etiology. J. Child Neurol. 2021, 36, 272–280. [Google Scholar] [CrossRef]
- Rissin, D.M.; Kan, C.W.; Song, L.; Rivnak, A.J.; Fishburn, M.W.; Shao, Q.; Piech, T.; Ferrell, E.P.; Meyer, R.E.; Campbell, T.G.; et al. Multiplexed single molecule immunoassays. Lab Chip 2013, 13, 2902–2911. [Google Scholar] [CrossRef]
- Duering, M.; Konieczny, M.J.; Tiedt, S.; Baykara, E.; Tuladhar, A.M.; Leijsen, E.V.; Lyrer, P.; Engelter, S.T.; Gesierich, B.; Achmüller, M.; et al. Serum Neurofilament Light Chain Levels Are Related to Small Vessel Disease Burden. J. Stroke 2018, 20, 228–238. [Google Scholar] [CrossRef]
- Kirschen, M.P.; Yehya, N.; Graham, K.; Kilbaugh, T.; Berg, R.A.; Topjian, A.; Diaz-Arrastia, R. Circulating Neurofilament Light Chain Is Associated With Survival After Pediatric Cardiac Arrest. Pediatr. Crit. Care Med. 2020, 21, 656–661. [Google Scholar] [CrossRef]
- Kristjánsdóttir, R.; Uvebrant, P.; Rosengren, L. Glial fibrillary acidic protein and neurofilament in children with cerebral white matter abnormalities. Neuropediatrics 2001, 32, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Research Committee on the Pathology and Treatment of Spontaneous Occlusion of the Circle of Willis; Health Labour Sciences Research Grant for Research on Measures for Infractable Diseases. Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis). Neurol. Med. Chir. 2012, 52, 245–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelborghs, S.; Niemantsverdriet, E.; Struyfs, H.; Blennow, K.; Brouns, R.; Comabella, M.; Dujmovic, I.; van der Flier, W.; Frölich, L.; Galimberti, D.; et al. Consensus guidelines for lumbar puncture in patients with neurological diseases. Alzheimers Dement. 2017, 8, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, J.; Takaku, A. Cerebrovascular “moyamoya” disease. Disease showing abnormal net-like vessels in base of brain. Arch. Neurol. 1969, 20, 288–299. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age (y) | Gender | CVD Type | NIHSS | U-B | Suzuki Grading | Pharmacological Therapy | Indirect R | Direct R | Genetic Syndromes |
|---|---|---|---|---|---|---|---|---|---|---|
| MMA8 | 16 | F | none | 0 | B | III | AG, ASA | yes | yes | no |
| MMA12 | 16 | F | IS | 1 | B | III | / | no | yes | no |
| MMA14 | 15 | F | TIA | 4 | B | IV | AG, ASA | yes | yes | no |
| MMA16 | 11 | M | IS | 6 | U | III | AG, ASA, AE | no | no | no |
| MMA18 | 9 | M | TIA | 0 | B | IV | AG, ASA, AE | no | no | no |
| MMA22 | 5 | M | IS | 2 | B | III | AG, ASA, AE | yes | yes | no |
| MMA44 | 9 | M | TIA | 0 | B | IV | AG, ASA | yes | yes | no |
| MMA46 | 6 | F | TIA | 0 | B | IV | ASA | yes | yes | u/i |
| MMA57 | 11 | M | none | 0 | U | III | AG, ASA | yes | yes | NF-1 |
| MMA60 | 9 | M | IS | 2 | B | IV | / | yes | yes | no |
| MMA62 | 7 | F | TIA | 0 | B | IV | AG, ASA | yes | yes | no |
| MMA64 | 3 | M | IS | 0 | B | III | AG, ASA, AE | yes | yes | NF-1 |
| MMA65 | 7 | F | IS | 1 | B | IV | AG, ASA | yes | yes | no |
| MMA67 | 6 | M | IS | 1 | B | IV | AG, ASA | yes | yes | no |
| MMA73 | 9 | F | none | 0 | B | III | AG, ASA | no | no | DS |
| MMA77 | 8 | F | none | 0 | B | IV | AG, ASA, AE | no | no | DT4q |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorla, G.; Carrozzini, T.; Pollaci, G.; Potenza, A.; Nava, S.; Acerbi, F.; Ferroli, P.; Esposito, S.; Saletti, V.; Ciusani, E.; et al. Increase of Circulating Endothelial Progenitor Cells and Released Angiogenic Factors in Children with Moyamoya Arteriopathy. Int. J. Mol. Sci. 2023, 24, 1233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24021233
Gorla G, Carrozzini T, Pollaci G, Potenza A, Nava S, Acerbi F, Ferroli P, Esposito S, Saletti V, Ciusani E, et al. Increase of Circulating Endothelial Progenitor Cells and Released Angiogenic Factors in Children with Moyamoya Arteriopathy. International Journal of Molecular Sciences. 2023; 24(2):1233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24021233
Chicago/Turabian StyleGorla, Gemma, Tatiana Carrozzini, Giuliana Pollaci, Antonella Potenza, Sara Nava, Francesco Acerbi, Paolo Ferroli, Silvia Esposito, Veronica Saletti, Emilio Ciusani, and et al. 2023. "Increase of Circulating Endothelial Progenitor Cells and Released Angiogenic Factors in Children with Moyamoya Arteriopathy" International Journal of Molecular Sciences 24, no. 2: 1233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24021233