
Brain-Derived Neurotrophic Factor Is Indispensable to Continence Recovery after a Dual Nerve and Muscle Childbirth Injury Model
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
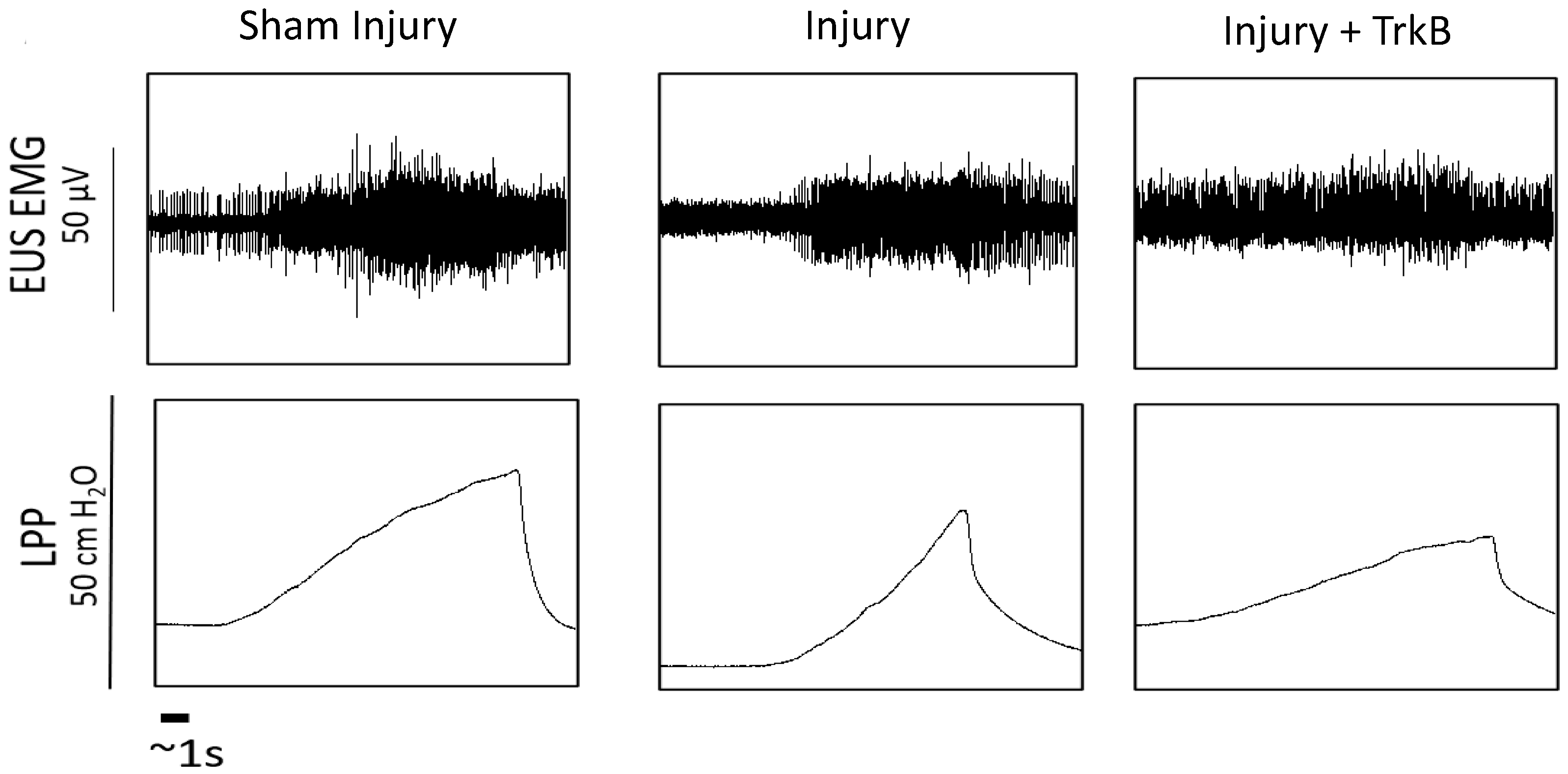
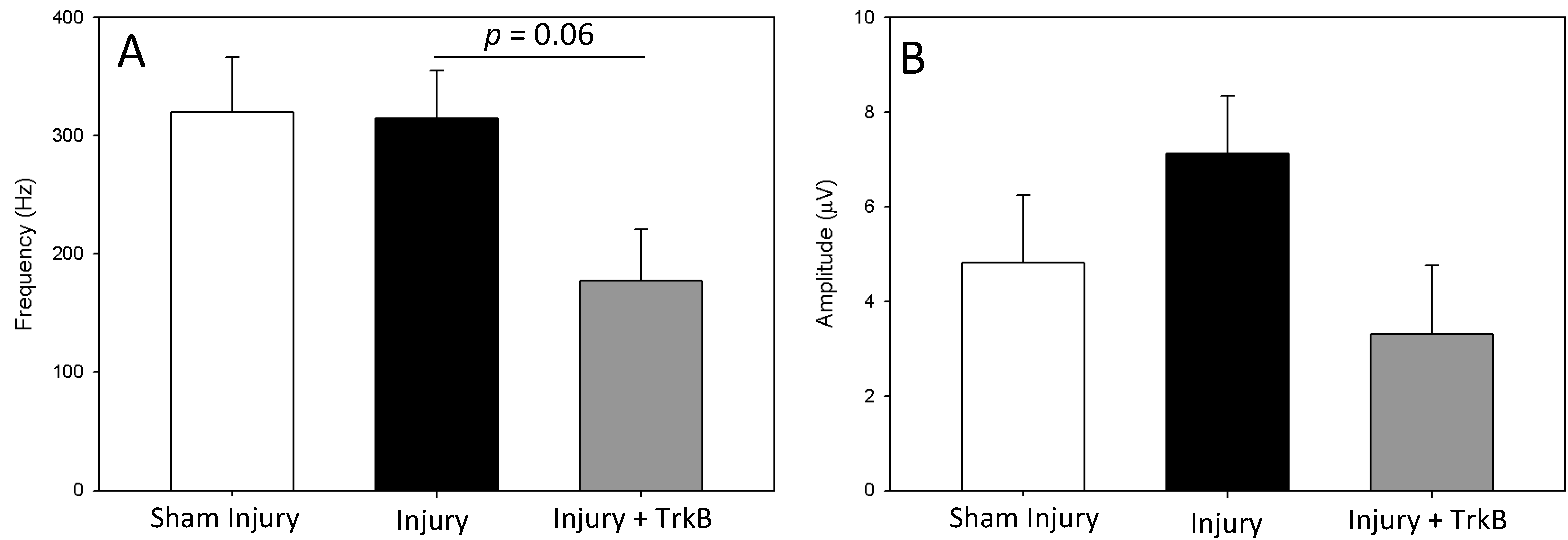
2.1. LPP and Electrophysiological Results
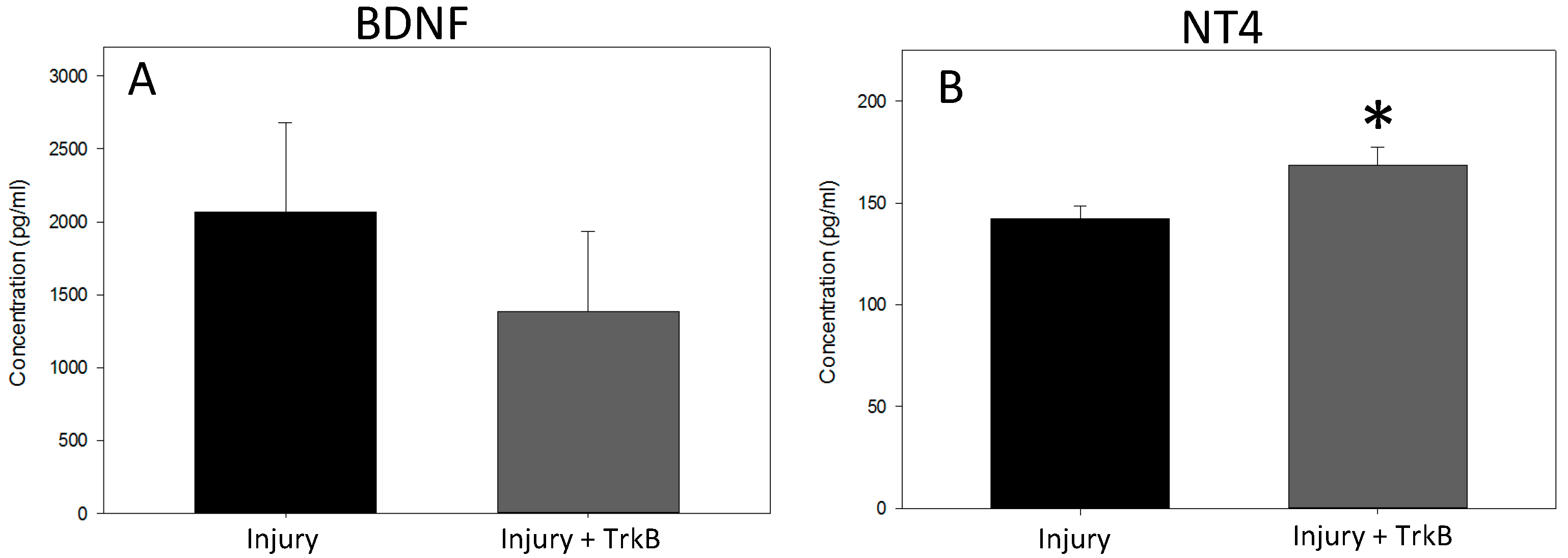
2.2. BDNF and NT4 Plasma Concentration
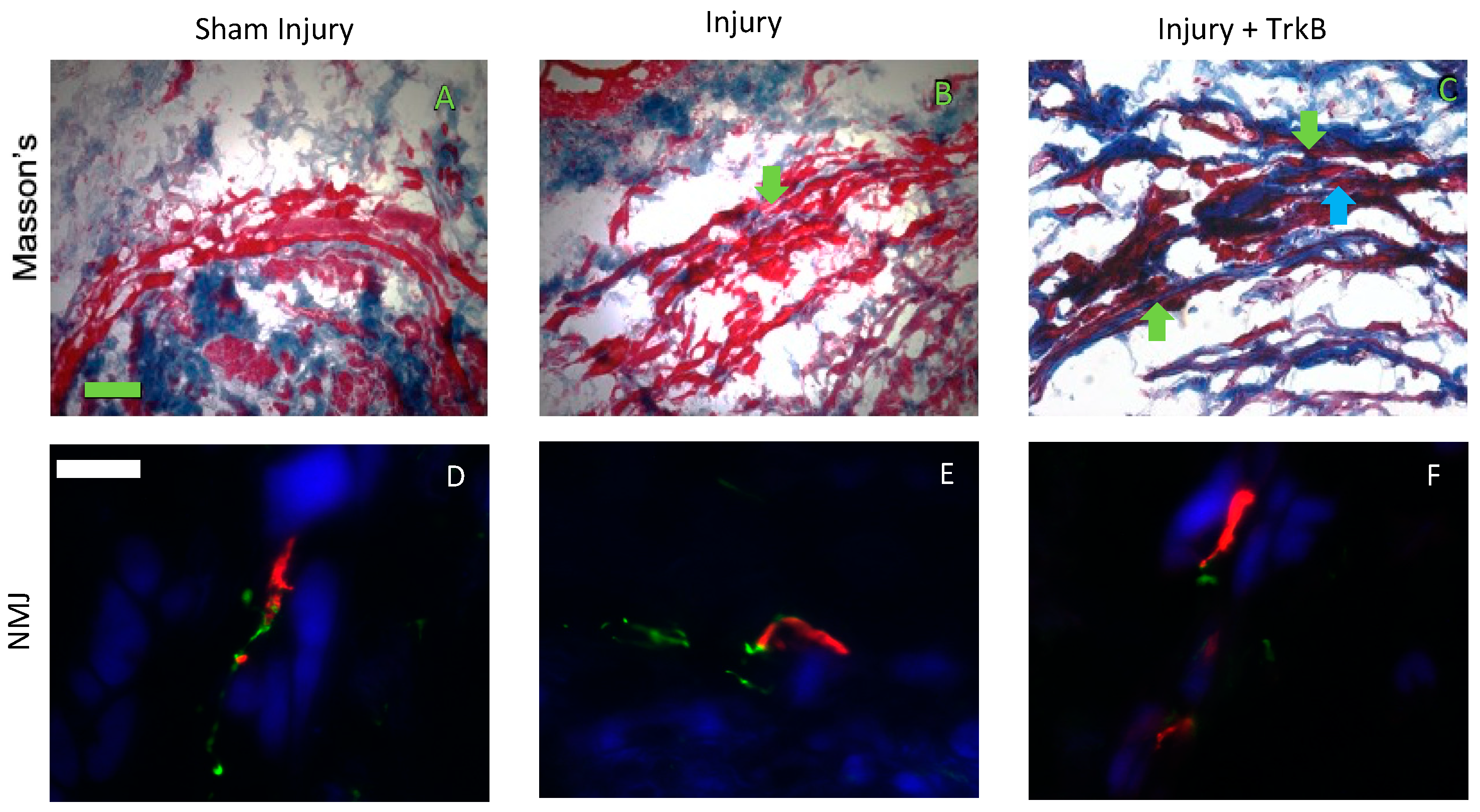
2.3. EUS Morphology and NMJs Staining
3. Discussion
4. Materials and Methods
4.1. Osmotic Pump Preparation
4.2. Injury model and Implantation of the Osmotic Pump
4.3. Suprapubic Bladder Catheter and Functional Testing
4.4. Plasma Collection
4.5. Histology and Immunofluorescence
4.6. ELISA
4.7. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van, K.P.; Victor, A.; Wein, A.; Van Kerrebroeck, P.; et al. The standardisation of terminology in lower urinary tract function: Report from the standardisation sub-committee of the International Continence Society. Urology 2003, 61, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Snooks, S.J.; Swash, M.; Mathers, S.E.; Henry, M.M. Effect of vaginal delivery on the pelvic floor: A 5-year follow-up. Br. J. Surg. 1990, 77, 1358–1360. [Google Scholar] [CrossRef] [PubMed]
- Rortveit, G.; Daltveit, A.K.; Hannestad, Y.S.; Hunskaar, S. Vaginal delivery parameters and urinary incontinence: The Norwegian EPINCONT study. Am. J. Obstet. Gynecol. 2003, 189, 1268–1274. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Gustilo-Ashby, A.M.; Salcedo, L.B.; Pan, H.Q.; Sypert, D.F.; Butler, R.S.; Damaser, M.S.; Gustillo-Ashby, M.A.; Gill, B.; Glaab, J.; et al. Dual simulated childbirth injuries result in slowed recovery of pudendal nerve and urethral function. Neurourol. Urodyn. 2009, 215, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Pan, H.Q.; Lin, D.L.; Strauch, C.; Butler, R.S.; Monnier, V.M.; Daneshgari, F.; Damaser, M.S. Pudendal nerve injury reduces urethral outlet resistance in diabetic rats. Am. J. Physiol.-Ren. Physiol. 2010, 299, F1443–F1450. [Google Scholar] [CrossRef] [Green Version]
- Gill, B.C.; Balog, B.M.; Dissaranan, C.; Jiang, H.H.; Steward, J.B.; Lin, D.L.; Damaser, M.S. Neurotrophin therapy improves recovery of the neuromuscular continence mechanism following simulated birth injury in rats. Neurourol. Urodyn. 2013, 32, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Yuan, X.; Balog, B.M.; Lin, D.L.; Hanzlicek, B.; Kuang, M.; Yan, H.; Majerus, S.J.A.; Damaser, M.S. Brain-Derived Neurotrophic Factor Is an Important Therapeutic Factor in Mesenchymal Stem Cell Secretions for Treatment of Traumatic Peripheral Pelvic Injuries. Front. Cell. Neurosci. 2022, 16, 866094. [Google Scholar] [CrossRef]
- Jones, K.R.; Farinas, I.; Backus, C.; Reichardt, L.F. Targeted disruption of the BDNF gene perturbs brain and sensory neuron development but not motor neuron development. Cell 1994, 76, 989–999. [Google Scholar] [CrossRef] [Green Version]
- El Hassan, R.; Galante, A.; Kavran, M.; Ganocy, S.; Khalifa, A.O.; Hijaz, A. The vaginal distention model in mice is not a reliable model of simulated birth trauma-induced stress urinary incontinence. Neurourol. Urodyn. 2019, 38, 599–606. [Google Scholar] [CrossRef]
- Li, X.; Wu, Q.; Xie, C.; Wang, C.; Wang, Q.; Dong, C.; Fang, L.; Ding, J.; Wang, T. Blocking of BDNF-TrkB signaling inhibits the promotion effect of neurological function recovery after treadmill training in rats with spinal cord injury. Spinal Cord 2019, 57, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Mantilla, C.B.; Gransee, H.M.; Sieck, G.C. Motoneuron BDNF/TrkB Signaling Enhances Functional recovery after Cerival Spinal Cord INjury. Exp. Neurol. 2013, 247, 101–109. [Google Scholar] [CrossRef] [Green Version]
- Balog, B.M.; Askew, T.; Lin, D.L.; Kuang, M.; Hanzlicek, B.; Damaser, M.S. The pudendal nerve motor branch regenerates via a brain derived neurotrophic factor mediated mechanism. Exp. Neurol. 2020, 334, 113438. [Google Scholar] [CrossRef]
- Viktrup, L.; Lose, G.; Rolff, M.; Barfoed, K. The symptom of stress incontinence caused by pregnancy or delivery in primiparas. Obstet. Gynecol. 1992, 79, 945–949. [Google Scholar]
- Viktrup, L. The risk of lower urinary tract symptoms five years after the first delivery. Neurourol. Urodyn. 2002, 21, 2–29. [Google Scholar] [CrossRef]
- Fritel, X.; Fauconnier, A.; Levet, C.; Benifla, J.L. Stress urinary incontinence 4 years after the first delivery: A retrospective cohort survey. Acta Obstet. Gynecol. Scand. 2004, 83, 941–945. [Google Scholar] [CrossRef]
- Gill, B.C.; Damaser, M.S.; Vasavada, S.P.; Goldman, H.B. Stress incontinence in the era of regenerative medicine: Reviewing the importance of the pudendal nerve. J. Urol. 2013, 190, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Song, Q.X.; Chermansky, C.J.; Birder, L.A.; Li, L.; Damaser, M.S. Brain-derived neurotrophic factor in urinary continence and incontinence. Nat. Rev. Urol. 2014, 11, 579–588. [Google Scholar] [CrossRef]
- Pan, H.Q.; Kerns, J.M.; Lin, D.L.; Sypert, D.; Steward, J.; Hoover, C.R.V.; Zaszczurynski, P.; Butler, R.S.; Damaser, M.S. Dual simulated childbirth injury delays anatomic recovery. Am. J. Physiol. Physiol. 2009, 296, F277–F283. [Google Scholar] [CrossRef]
- Jiang, H.; Gustilo-Ashby, A.M.; Salcedo, L.B.; Pan, H.Q.; Sypert, D.F.; Butler, R.S.; Damaser, M.S. Electrophysiological function during voiding after simulated childbirth injuries. Exp. Neurol. 2009, 215, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Skoner, M.M.; Thompson, W.D.; Caron, V.A. Factors associated with risk of stress urinary incontinence in women. Nurs. Res. 1994, 43, 301–306. [Google Scholar] [CrossRef]
- Swash, M. The neurogenic hypothesis of stress incontinence. Ciba Found. Symp. 1990, 151, 155–156. [Google Scholar]
- Jiang, H.; Salcedo, L.B.; Damaser, M.S. Quantification of neurological and other contributors to continence in female rats. Brain Res. 2011, 1382, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Dissaranan, C.; Cruz, M.A.; Kiedrowski, M.J.; Balog, B.M.; Gill, B.C.; Penn, M.S.; Goldman, H.B.; Damaser, M.S. Rat mesenchymal stem cell secretome promotes elastogenesis and facilitates recovery from simulated childbirth injury. Cell Transpl. 2011, 23, 1395–1406. [Google Scholar] [CrossRef] [Green Version]
- Byrne, P.J.; Stuart, R.M.; Fakhry, C.; Lehar, M.; Flint, P.W. An electrophysiologic model for functional assessment of effects of neurotrophic factors on facial nerve reinnervation. Arch. Facial Plast. Surg. 2005, 7, 114–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, K.; Lin, D.L.; Hanzlicek, B.; Deng, K.; Balog, B.M.; van der Vaart, C.H.; Damaser, M.S. Multiple doses of stem cells maintain urethral function in a model of neuromuscular injury resulting in stress urinary incontinence. Am. J. Physiol.-Ren. Physiol. Physiol. 2019, 317, F1047–F1057. [Google Scholar] [CrossRef]
- Sharma, N.; Moeller, C.W.; Marzo, S.J.; Jones, K.J.; Foecking, E.M. Combinatorial Treatments Enhance Recovery Following Facial Nerve Crush. Laryngoscope 2010, 120, 1523–1530. [Google Scholar] [CrossRef]
- Moffat, B.A.; Chen, M.; Kariaapper, M.S.T.; Hamstra, D.A.; Hall, D.E.; Stojanovska, J.; Johnson, T.D.; Blaivas, M.; Kumar, M.; Chenevert, T.L.; et al. Inhibition of vascular endothelial growth factor (VEGF)-A causes a paradoxical increase in tumor blood flow and up-regulation of VEGF-D. Clin. Cancer Res. 2006, 12, 1525–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croll, S.D.; Chesnutt, C.R.; Rudge, J.S.; Acheson, A.; Ryan, T.E.; Siuciak, J.A.; DiStefano, P.S.; Wiegand, S.J.; Lindsay, R.M. Co-infusion with a TrkB-Fc receptor body carrier enhances BDNF distribution in the adult rat brain. Exp. Neurol. 1998, 152, 20–33. [Google Scholar] [CrossRef]
- Fu, S.Y.; Gordon, T. Contributing factors to poor functional recovery after delayed nerve repair: Prolonged denervation. J. Neurosci. 1995, 15, 3886–3895. [Google Scholar] [CrossRef]
- Gordon, T.; English, A.W. Strategies to promote peripheral nerve regeneration: Electrical stimulation and/or exercise. Eur. J. Neurosci. 2016, 43, 336–350. [Google Scholar] [CrossRef] [Green Version]
- Verdú, E.; Ceballos, D.; Vilches, J.J.; Navarro, X. Influence of aging on peripheral nerve function and regeneration. J. Peripher. Nerv. Syst. 2000, 5, 191–208. [Google Scholar] [CrossRef]
- Song, Q.X.; Balog, B.M.; Kerns, J.; Lin, D.L.; Sun, Y.; Damaser, M.S.; Jiang, H.H. Long-term effects of simulated childbirth injury on function and innervation of the urethra. Neurourol. Urodyn. 2015, 34, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Sangsawang, B.; Sangsawang, N. Stress urinary incontinence in pregnant women: A review of prevalence, pathophysiology, and treatment. Int. Urogynecol. J. 2013, 24, 901–912. [Google Scholar] [CrossRef] [Green Version]
- Deng, K.; Balog, B.M.; Lin, D.L.; Hanzlicek, B.; Song, Q.X.; Zhu, H.; Damaser, M.S. Daily bilateral pudendal nerve electrical stimulation improves recovery from stress urinary incontinence. Interface Focus 2019, 9, 20190020. [Google Scholar] [CrossRef] [Green Version]
- Balog, B.M.; Deng, K.; Askew, T.; Kuang, M.; Hanzlicek, B.; Damaser, M.S. Brain derived neurotrophic factor mediates accelerated recovery of regenerative electrical stimulation in an animal model of stress urinary incontinence. Exp. Neurol. 2021, 343, 113781. [Google Scholar] [CrossRef]
- Deng, K.; Lin, D.L.L.; Hanzlicek, B.; Balog, B.M.; Penn, M.S.; Kiedrowski, M.J.; Hu, Z.; Ye, Z.; Zhu, H.; Damaser, M.S. Mesenchymal stem cells and their secretome partially restore nerve and urethral function in a dual muscle and nerve injury stress urinary incontinence model. Am. J. Physiol.-Ren. Physiol. Ren. Physiol. 2015, 308, F92–F100. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balog, B.M.; Deng, K.; Askew, T.; Hanzlicek, B.; Kuang, M.; Damaser, M.S. Brain-Derived Neurotrophic Factor Is Indispensable to Continence Recovery after a Dual Nerve and Muscle Childbirth Injury Model. Int. J. Mol. Sci. 2023, 24, 4998. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24054998
Balog BM, Deng K, Askew T, Hanzlicek B, Kuang M, Damaser MS. Brain-Derived Neurotrophic Factor Is Indispensable to Continence Recovery after a Dual Nerve and Muscle Childbirth Injury Model. International Journal of Molecular Sciences. 2023; 24(5):4998. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24054998
Chicago/Turabian StyleBalog, Brian M., Kangli Deng, Tessa Askew, Brett Hanzlicek, Mei Kuang, and Margot S. Damaser. 2023. "Brain-Derived Neurotrophic Factor Is Indispensable to Continence Recovery after a Dual Nerve and Muscle Childbirth Injury Model" International Journal of Molecular Sciences 24, no. 5: 4998. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24054998