
Epilepsy and Attention Deficit Hyperactivity Disorder: Connection, Chance, and Challenges

 , , ,
, , ,  and
and
Abstract
:1. Introduction
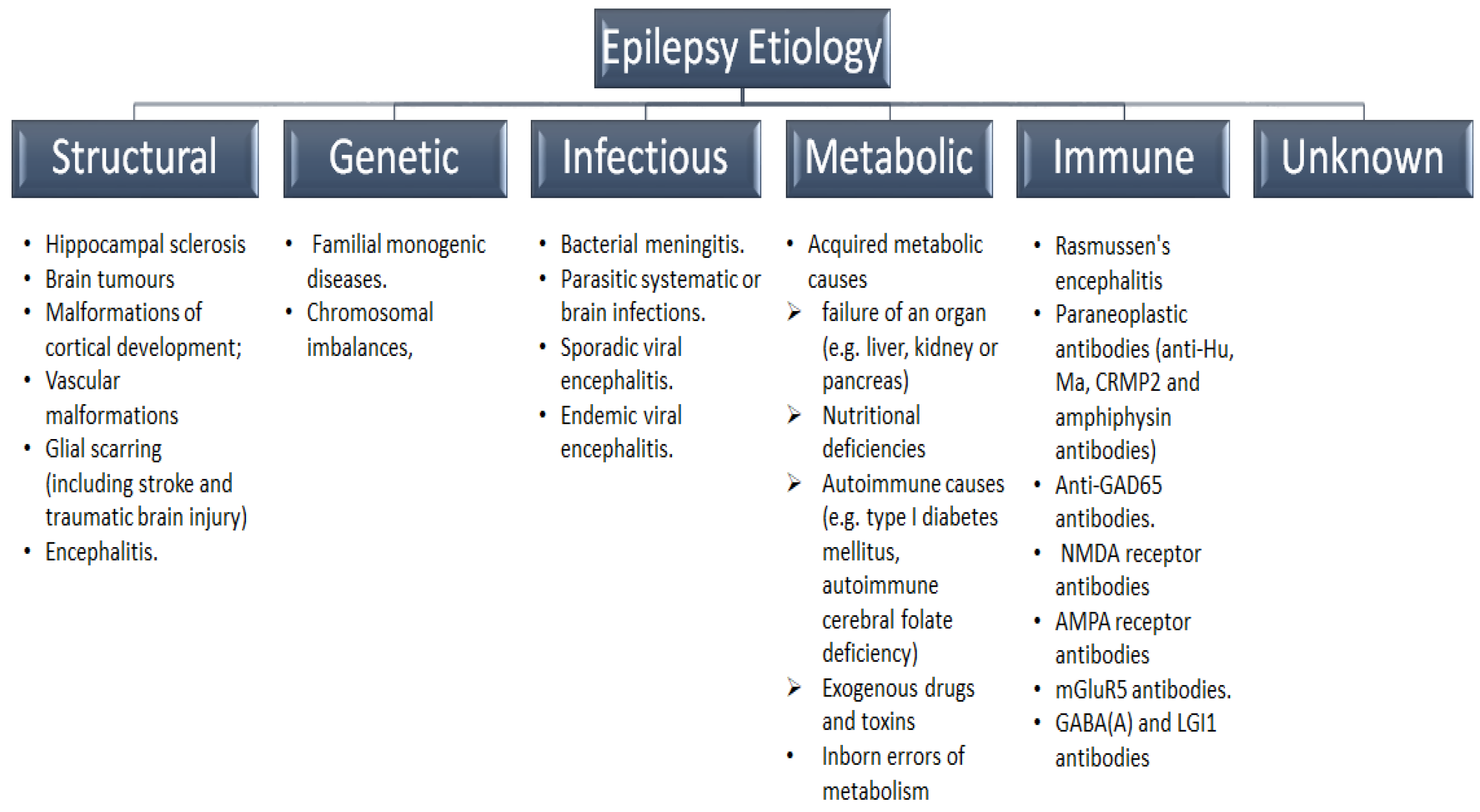
2. Evolving Concepts in Epilepsy Classification and Etiologies
3. The Burden of Psychiatric Comorbidities in Epilepsy
4. Evolving Concepts in ADHD
5. The Burden of ADHD in CWE
6. ADHD and Epilepsy: Mechanisms of Association
6.1. ADHD and Epilepsy: A Chance?
6.2. Causative Mechanisms
6.3. Resultants Mechanisms
6.4. Shared Genetics
6.5. Shared Risk Factors
6.6. Bidirectional Connection
7. ADHD in Different Types of Epilepsy
7.1. Generalized Epilepsy
7.2. Frontal Lobe Epilepsy (FLE)
7.3. Childhood Absence Epilepsy (CAE)
7.4. Benign Rolandic Epilepsy (BRE)
8. Do stimulants Increase the Risk of Epilepsy?
8.1. Stimulants Are Highly Efficacious in CWE with Comorbid ADHD
8.2. MPH in Pediatric Subjects and AMP in Adults Are the First-Line ADHD Therapy
8.3. Evaluating the Risk of Increasing Seizures in CWE and Comorbid ADHD Receiving Stimulants Is Crucial
8.4. The False Myth of Increased Risk of Seizures with Stimulants

{kind=link}
| Author | Year | Design | Patients | Stimulants/ADHD Improved the Rate | No. | Follow-Up | Main Findings |
|---|---|---|---|---|---|---|---|
| Liu [171] | 2018 | Retrospective | CWE | MPH or AMP/NA | 72,363 | 1 year | No risk increase |
| Wiggs [169] | 2017 | Retrospective | ADHD with and without epilepsy | ASC, d-MPH, DAS, LDX, MAH, MP, and MPHH/NA | 801,838 | 10 years | Reduced risk |
| Rheims [150] | 2016 | Prospective | Active or controlled CWE and comorbid ADHD | MPH/75% | 167 | 12–16 weeks | No risk increase |
| Radziuk [164] | 2015 | Open-label trial | Active CWE and comorbid ADHD | MPH/NA | 30 | 6 months | No risk increase |
| Gonzalez- Heydrich [156] | 2014 | Retrospective | Controlled CWE and comorbid ADHD | MPH/63% or AMP/24% | 36 | 49 months | No risk increased |
| Santos [153] | 2013 | Open-label trial | Active epilepsy and comorbid ADHD | MPH/73% | 22 | 4 weeks | No risk increased |
| Koneski [144] | 2011 | Open-label trial | Active epilepsy and comorbid ADHD | MPH/70.8% | 24 | 6 months | No risk increased |
| Gonzalez- Heydrich [149] | 2010 | Double-blind, controlled, trial | Active epilepsy and comorbid ADHD | OROS MPH/60–70% | 33 | 1–3 weeks | Increased risk |
| Yoo [170] | 2009 | Open-label trial | Controlled CWE and comorbid ADHD | OROS MPH/64% | 25 | 8 weeks | No risk increase in 92% of patients |
| Van der Feltz-Cornelis [168] | 2006 | Open-label trial | Active epilepsy and comorbid ADHD | MPH/100% | 6 | 6 weeks | No risk increase |
| Gucuyener [166] | 2003 | Open-label trial | Active CWE and comorbid ADHD | MPH/77% | 119 | 12 months | No risk increase |
| Hemmer [167] | 2001 | Retrospective | ADHD | MPH, DAS, or ASC/NA | 234 | 6 years | No risk increase |
| Gross-Tsur [162] | 1997 | Open-label trial | Controlled CWE and comorbid ADHD | MPH/70% | 30 | 8 weeks | Increased risk in active patients |
| Wroblewski [165] | 1992 | Retrospective | children and adults with active post-traumatic seizures | MPH/NA | 30 | 3 months | Risk reduction |
| Feldman [148] | 1989 | Double-blind, controlled, trial | Controlled CWE and comorbid ADHD | MPH/70% | 10 | 8 weeks | No risk increase |
9. ADHD and Epilepsy: Challenges and Opportunities
9.1. ADHD Is A Spectrum Disorder
9.2. Challenges in the Early Diagnosis of ADHD in CWE
9.3. Treatment Strategy for ADHD in Epilepsy
9.3.1. Pharmacological management
Choosing Proper ASMs
Pharmacological Management for ADHD in Epilepsy
Stimulants
Non-Stimulants
Non-Pharmacological Management: Behavioral Therapies
9.3.2. Drug Interactions
9.4. Novel ASMs against Both Epilepsy and ADHD
9.5. ASMs in CWE and Comorbid ADHD
9.6. Recent Medications Development for ADHD
9.6.1. Lisdexamfetamine (LDX)
9.6.2. Viloxazine
9.6.3. Serdexmethylphenidate (SDX)
9.6.4. Mazindol
9.6.5. Centanafadine
9.6.6. Dasotraline
9.6.7. Vortioxetine (VTX)
9.6.8. Droxidopa
9.6.9. Baicalin
9.7. Impact of Comorbid ADHD on Developmental Outcomes
9.8. Potential Role of Precision Medicine
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADHD | attention deficit hyperactivity disorder |
| AMP | amphetamine |
| ASC | amphetamine salt combination |
| ASMs | antiseizure medications |
| BECTS | benign epilepsy with centrotemporal spikes |
| BRE | benign rolandic epilepsy |
| CAE | childhood absence epilepsy |
| CWE | children with epilepsy |
| DAS | dextroamphetamine sulfate |
| DAT | dopamine transporters |
| D-MPH | dexmethylphenidate hydrochloride |
| DNRI | dopamine and norepinephrine reuptake inhibitor |
| DSM | Diagnostic and Statistical Manual of Mental Disorders |
| EEG | electroencephalogram |
| FDA | Food and Drug Administration |
| FLE | frontal lobe epilepsy |
| GABA | γ-aminobutyric acid |
| GWAS | genome-wide association studies |
| ILAE | International League Against Epilepsy |
| IQ | intelligence quotient |
| LDX | lisdexamfetamine dimesylate |
| MAH | methamphetamine hydrochloride |
| MECP2 | methyl-CpG binding protein 2 |
| MEF2C | myocyte enhancer factor 2 |
| MPH | methylphenidate |
| MPHH | methylphenidate hydrochloride |
| NET | norepineph- rine transporter |
| SBG | Scutellaria baicalensis Georgi |
| SDX | Serdexmethylphenidate |
| SEEG | stereo electroencephalogram |
| SERT | serotonin transporter |
| SNP | single nucleotide polymorphism |
| VMAT2 | vesicular monoamine transporter 2 |
| VTX | Vortioxetine |
References
- Ngugi, A.K.; Bottomley, C.; Kleinschmidt, I.; Sander, J.W.; Newton, C.R. Estimation of the burden of active and life-time epilepsy: A meta-analytic approach. Epilepsia 2010, 51, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Fiest, K.M.; Sauro, K.M.; Wiebe, S.; Patten, S.B.; Kwon, C.S.; Dykeman, J.; Pringsheim, T.; Lorenzetti, D.L.; Jette, N. Prevalence and incidence of epilepsy: A systematic review and meta-analysis of international studies. Neurology 2017, 88, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Panteliadis, C.P.; Vassilyadi, P.; Fehlert, J.; Hagel, C. Historical documents on epilepsy: From antiquity through the 20th century. Brain Dev. 2017, 39, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.V.; Reynolds, E.H. Texts and documents. Translation and analysis of a cuneiform text forming part of a Babylonian treatise on epilepsy. Med. Hist. 1990, 34, 185–198. [Google Scholar] [CrossRef] [Green Version]
- Wolf, P. History of epilepsy: Nosological concepts and classification. Epileptic Disord. 2014, 16, 261–269. [Google Scholar] [CrossRef]
- Aaberg, K.M.; Gunnes, N.; Bakken, I.J.; Lund Soraas, C.; Berntsen, A.; Magnus, P.; Lossius, M.I.; Stoltenberg, C.; Chin, R.; Suren, P. Incidence and Prevalence of Childhood Epilepsy: A Nationwide Cohort Study. Pediatrics 2017, 139, e20163908. [Google Scholar] [CrossRef] [Green Version]
- Kanner, A.M.; Bicchi, M.M. Review of Antiseizure Medications for Adults with Epilepsy-Reply. JAMA 2022, 328, 681. [Google Scholar] [CrossRef]
- Picot, M.C.; Baldy-Moulinier, M.; Daures, J.P.; Dujols, P.; Crespel, A. The prevalence of epilepsy and pharmacoresistant epilepsy in adults: A population-based study in a Western European country. Epilepsia 2008, 49, 1230–1238. [Google Scholar] [CrossRef]
- Trinka, E.; Kwan, P.; Lee, B.; Dash, A. Epilepsy in Asia: Disease burden, management barriers, and challenges. Epilepsia 2019, 60 (Suppl 1), 7–21. [Google Scholar] [CrossRef] [Green Version]
- Hamer, H.M.; Spottke, A.; Aletsee, C.; Knake, S.; Reis, J.; Strzelczyk, A.; Oertel, W.H.; Rosenow, F.; Dodel, R. Direct and indirect costs of refractory epilepsy in a tertiary epilepsy center in Germany. Epilepsia 2006, 47, 2165–2172. [Google Scholar] [CrossRef]
- Keezer, M.R.; Sisodiya, S.M.; Sander, J.W. Comorbidities of epilepsy: Current concepts and future perspectives. Lancet Neurol. 2016, 15, 106–115. [Google Scholar] [CrossRef]
- Magnus, W.; Nazir, S.; Anilkumar, A.C.; Shaban, K. Attention Deficit Hyperactivity Disorder; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Dunn, D.W.; Austin, J.K.; Harezlak, J.; Ambrosius, W.T. ADHD and epilepsy in childhood. Dev. Med. Child Neurol. 2003, 45, 50–54. [Google Scholar] [CrossRef]
- Davis, S.M.; Katusic, S.K.; Barbaresi, W.J.; Killian, J.; Weaver, A.L.; Ottman, R.; Wirrell, E.C. Epilepsy in children with attention-deficit/hyperactivity disorder. Pediatr. Neurol. 2010, 42, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, L.; Hamer, H.M.; Kostev, K. Adherence to antiepileptic drugs in children and adolescents: A retrospective study in primary care settings in Germany. Epilepsy Behav. 2017, 75, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Reilly, C.J. Attention deficit hyperactivity disorder (ADHD) in childhood epilepsy. Res. Dev. Disabil. 2011, 32, 883–893. [Google Scholar] [CrossRef]
- Collaborators, G.B.D.E. Global, regional, and national burden of epilepsy, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 357–375. [Google Scholar] [CrossRef] [Green Version]
- Giussani, G.; Cricelli, C.; Mazzoleni, F.; Cricelli, I.; Pasqua, A.; Pecchioli, S.; Lapi, F.; Beghi, E. Prevalence and incidence of epilepsy in Italy based on a nationwide database. Neuroepidemiology 2014, 43, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Lv, R.J.; Wang, Q.; Cui, T.; Zhu, F.; Shao, X.Q. Status epilepticus-related etiology, incidence and mortality: A meta-analysis. Epilepsy Res. 2017, 136, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Thurman, D.J.; Durgin, T.; Faught, E.; Helmers, S. Estimating Epilepsy Incidence and Prevalence in the US Pediatric Population Using Nationwide Health Insurance Claims Data. J. Child Neurol. 2016, 31, 743–749. [Google Scholar] [CrossRef]
- Forsgren, L.; Beghi, E.; Oun, A.; Sillanpaa, M. The epidemiology of epilepsy in Europe—A systematic review. Eur. J. Neurol. 2005, 12, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Cross, J.H. Epilepsy (generalised seizures). BMJ Clin. Evid. 2015, 2015, 1201. [Google Scholar] [PubMed]
- Chiang, K.L.; Cheng, C.Y. Prevalence and neuro-psychiatric comorbidities of pediatric epilepsy in Taiwan: A national population-based study. Epilepsy Res. 2014, 108, 1451–1460. [Google Scholar] [CrossRef]
- Camfield, P.; Camfield, C. Incidence, prevalence and aetiology of seizures and epilepsy in children. Epileptic Disord. 2015, 17, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Fine, A.; Wirrell, E.C. Seizures in Children. Pediatr. Neurol. 2020, 41, 321–347. [Google Scholar] [CrossRef]
- Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981, 22, 489–501. [Google Scholar] [CrossRef]
- Berg, A.T.; Berkovic, S.F.; Brodie, M.J.; Buchhalter, J.; Cross, J.H.; van Emde Boas, W.; Engel, J.; French, J.; Glauser, T.A.; Mathern, G.W.; et al. Revised terminology and concepts for organization of seizures and epilepsies: Report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia 2010, 51, 676–685. [Google Scholar] [CrossRef]
- Patel, P.; Moshe, S.L. The evolution of the concepts of seizures and epilepsy: What’s in a name? Epilepsia Open 2020, 5, 22–35. [Google Scholar] [CrossRef] [Green Version]
- Turek, G.; Skjei, K. Seizure semiology, localization, and the 2017 ILAE seizure classification. Epilepsy Behav. 2022, 126, 108455. [Google Scholar] [CrossRef]
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshe, S.L.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [Green Version]
- Fisher, R.S.; Cross, J.H.; French, J.A.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshe, S.L.; Peltola, J.; Roulet Perez, E.; et al. Operational classification of seizure types by the International League against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 522–530. [Google Scholar] [CrossRef] [Green Version]
- Adelow, C.; Andell, E.; Amark, P.; Andersson, T.; Hellebro, E.; Ahlbom, A.; Tomson, T. Newly diagnosed single unprovoked seizures and epilepsy in Stockholm, Sweden: First report from the Stockholm Incidence Registry of Epilepsy (SIRE). Epilepsia 2009, 50, 1094–1101. [Google Scholar] [CrossRef]
- O’Callaghan, F.J.; Edwards, S.W.; Alber, F.D.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Likeman, M.; Lux, A.L.; Mackay, M.; Mallick, A.A.; et al. Safety and effectiveness of hormonal treatment versus hormonal treatment with vigabatrin for infantile spasms (ICISS): A randomised, multicentre, open-label trial. Lancet Neurol. 2017, 16, 33–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brigo, F.; Jones, K.; Eltze, C.; Matricardi, S. Anti-seizure medications for Lennox-Gastaut syndrome. Cochrane Database Syst. Rev. 2021, 4, CD003277. [Google Scholar] [CrossRef]
- Thomas, R.H.; Berkovic, S.F. The hidden genetics of epilepsy—A clinically important new paradigm. Nat. Rev. Neurol. 2014, 10, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Corey, L.A.; Pellock, J.M.; Kjeldsen, M.J.; Nakken, K.O. Importance of genetic factors in the occurrence of epilepsy syndrome type: A twin study. Epilepsy Res. 2011, 97, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheffer, I.E.; French, J.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshe, S.L.; Perucca, E.; Tomson, T.; Wiebe, S.; Zhang, Y.H.; et al. Classification of the epilepsies: New concepts for discussion and debate-Special report of the ILAE Classification Task Force of the Commission for Classification and Terminology. Epilepsia Open 2016, 1, 37–44. [Google Scholar] [CrossRef]
- Patel, R.S.; Elmaadawi, A.; Mansuri, Z.; Kaur, M.; Shah, K.; Nasr, S. Psychiatric Comorbidities and Outcomes in Epilepsy Patients: An Insight from a Nationwide Inpatient Analysis in the United States. Cureus 2017, 9, e1686. [Google Scholar] [CrossRef] [Green Version]
- Muhigwa, A.; Preux, P.M.; Gerard, D.; Marin, B.; Boumediene, F.; Ntamwira, C.; Tsai, C.H. Comorbidities of epilepsy in low and middle-income countries: Systematic review and meta-analysis. Sci. Rep. 2020, 10, 9015. [Google Scholar] [CrossRef]
- Forsgren, L. Prevalence of epilepsy in adults in northern Sweden. Epilepsia 1992, 33, 450–458. [Google Scholar] [CrossRef]
- Jennum, P.; Pickering, L.; Christensen, J.; Ibsen, R.; Kjellberg, J. Morbidity and mortality of childhood- and adolescent-onset epilepsy: A controlled national study. Epilepsy Behav. 2017, 66, 80–85. [Google Scholar] [CrossRef]
- Aaberg, K.M.; Bakken, I.J.; Lossius, M.I.; Lund Soraas, C.; Haberg, S.E.; Stoltenberg, C.; Suren, P.; Chin, R. Comorbidity and Childhood Epilepsy: A Nationwide Registry Study. Pediatrics 2016, 138, e20160921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weatherburn, C.J.; Heath, C.A.; Mercer, S.W.; Guthrie, B. Physical and mental health comorbidities of epilepsy: Population-based cross-sectional analysis of 1.5 million people in Scotland. Seizure 2017, 45, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Andell Jason, E. Neurodevelopmental and psychiatric comorbidities negatively affect outcome in children with unprovoked seizures—A non-systematic review. Acta Paediatr. 2021, 110, 2944–2950. [Google Scholar] [CrossRef] [PubMed]
- Pastor, P.N.; Reuben, C.A.; Kobau, R.; Helmers, S.L.; Lukacs, S. Functional difficulties and school limitations of children with epilepsy: Findings from the 2009–2010 National Survey of Children with Special Health Care Needs. Disabil. Health J. 2015, 8, 231–239. [Google Scholar] [CrossRef]
- Hermann, B.P.; Seidenberg, M.; Bell, B. Psychiatric comorbidity in chronic epilepsy: Identification, consequences, and treatment of major depression. Epilepsia 2000, 41 (Suppl. 2), S31–S41. [Google Scholar] [CrossRef] [Green Version]
- Oh, A.; Thurman, D.J.; Kim, H. Comorbidities and risk factors associated with newly diagnosed epilepsy in the U.S. pediatric population. Epilepsy Behav. 2017, 75, 230–236. [Google Scholar] [CrossRef]
- Jacoby, A.; Baker, G.A.; Steen, N.; Potts, P.; Chadwick, D.W. The clinical course of epilepsy and its psychosocial correlates: Findings from a U.K. Community study. Epilepsia 1996, 37, 148–161. [Google Scholar] [CrossRef]
- Alfstad, K.A.; Clench-Aas, J.; Van Roy, B.; Mowinckel, P.; Gjerstad, L.; Lossius, M.I. Psychiatric symptoms in Norwegian children with epilepsy aged 8–13 years: Effects of age and gender? Epilepsia 2011, 52, 1231–1238. [Google Scholar] [CrossRef]
- Dharmadhikari, A.S.; Sinha, V.K. Psychiatric Comorbidity in Children with Epilepsy: A Cross-sectional 5 Years Rural Prevalence Study. J. Neurosci. Rural. Pract. 2017, 8, 179–184. [Google Scholar] [CrossRef]
- Jason, E.A.; Tomson, T.; Carlsson, S.; Tedroff, K.; Amark, P. Neurodevelopmental comorbidities and seizure control 24 months after a first unprovoked seizure in children. Epilepsy Res. 2018, 143, 33–40. [Google Scholar] [CrossRef]
- Russ, S.A.; Larson, K.; Halfon, N. A national profile of childhood epilepsy and seizure disorder. Pediatrics 2012, 129, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics 2015, 135, e994–e1001. [Google Scholar] [CrossRef] [Green Version]
- Rydell, M.; Lundstrom, S.; Gillberg, C.; Lichtenstein, P.; Larsson, H. Has the attention deficit hyperactivity disorder phenotype become more common in children between 2004 and 2014? Trends over 10 years from a Swedish general population sample. J. Child Psychol. Psychiatry 2018, 59, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Del Campo, N.; Chamberlain, S.R.; Sahakian, B.J.; Robbins, T.W. The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biol. Psychiatry 2011, 69, e145–e157. [Google Scholar] [CrossRef]
- Spalletta, G.; Pasini, A.; Pau, F.; Guido, G.; Menghini, L.; Caltagirone, C. Prefrontal blood flow dysregulation in drug naive ADHD children without structural abnormalities. J. Neural Transm. Vienna 2001, 108, 1203–1216. [Google Scholar] [CrossRef]
- Valera, E.M.; Faraone, S.V.; Murray, K.E.; Seidman, L.J. Meta-analysis of structural imaging findings in attention-deficit/hyperactivity disorder. Biol. Psychiatry 2007, 61, 1361–1369. [Google Scholar] [CrossRef]
- Frodl, T.; Skokauskas, N. Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects. Acta Psychiatr. Scand. 2012, 125, 114–126. [Google Scholar] [CrossRef]
- Cortese, S.; Kelly, C.; Chabernaud, C.; Proal, E.; Di Martino, A.; Milham, M.P.; Castellanos, F.X. Toward systems neuroscience of ADHD: A meta-analysis of 55 fMRI studies. Am. J. Psychiatry 2012, 169, 1038–1055. [Google Scholar] [CrossRef] [Green Version]
- Hart, H.; Radua, J.; Nakao, T.; Mataix-Cols, D.; Rubia, K. Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: Exploring task-specific, stimulant medication, and age effects. JAMA Psychiatry 2013, 70, 185–198. [Google Scholar] [CrossRef] [Green Version]
- Norman, L.J.; Carlisi, C.; Lukito, S.; Hart, H.; Mataix-Cols, D.; Radua, J.; Rubia, K. Structural and Functional Brain Abnormalities in Attention-Deficit/Hyperactivity Disorder and Obsessive-Compulsive Disorder: A Comparative Meta-analysis. JAMA Psychiatry 2016, 73, 815–825. [Google Scholar] [CrossRef] [Green Version]
- Soheilipour, F.; Shiri, S.; Ahmadkhaniha, H.R.; Abdollahi, E.; Hosseini-Baharanchi, F.S. Risk factors for attention-deficit/hyperactivity disorder: A case-control study in 5 to 12 years old children. Med. Pharm. Rep. 2020, 93, 175–180. [Google Scholar] [CrossRef]
- Linnet, K.M.; Dalsgaard, S.; Obel, C.; Wisborg, K.; Henriksen, T.B.; Rodriguez, A.; Kotimaa, A.; Moilanen, I.; Thomsen, P.H.; Olsen, J.; et al. Maternal lifestyle factors in pregnancy risk of attention deficit hyperactivity disorder and associated behaviors: Review of the current evidence. Am. J. Psychiatry 2003, 160, 1028–1040. [Google Scholar] [CrossRef]
- Knopik, V.S.; Heath, A.C.; Jacob, T.; Slutske, W.S.; Bucholz, K.K.; Madden, P.A.; Waldron, M.; Martin, N.G. Maternal alcohol use disorder and offspring ADHD: Disentangling genetic and environmental effects using a children-of-twins design. Psychol. Med. 2006, 36, 1461–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nigg, J.T.; Nikolas, M.; Mark Knottnerus, G.; Cavanagh, K.; Friderici, K. Confirmation and extension of association of blood lead with attention-deficit/hyperactivity disorder (ADHD) and ADHD symptom domains at population-typical exposure levels. J. Child Psychol. Psychiatry 2010, 51, 58–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caspersen, I.H.; Aase, H.; Biele, G.; Brantsaeter, A.L.; Haugen, M.; Kvalem, H.E.; Skogan, A.H.; Zeiner, P.; Alexander, J.; Meltzer, H.M.; et al. The influence of maternal dietary exposure to dioxins and PCBs during pregnancy on ADHD symptoms and cognitive functions in Norwegian preschool children. Environ. Int. 2016, 94, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Millichap, J.G. Etiologic classification of attention-deficit/hyperactivity disorder. Pediatrics 2008, 121, e358–e365. [Google Scholar] [CrossRef]
- Robberecht, H.; Verlaet, A.A.J.; Breynaert, A.; De Bruyne, T.; Hermans, N. Magnesium, Iron, Zinc, Copper and Selenium Status in Attention-Deficit/Hyperactivity Disorder (ADHD). Molecules 2020, 25, 4440. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.C.; Chen, C.M.; Tsai, J.D.; Chiang, K.L.; Tsai, S.C.; Huang, C.Y.; Lin, C.L.; Hsu, C.Y.; Chang, K.H. Association between Exposure to Particulate Matter Air Pollution during Early Childhood and Risk of Attention-Deficit/Hyperactivity Disorder in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 16138. [Google Scholar] [CrossRef]
- Nikolas, M.A.; Burt, S.A. Genetic and environmental influences on ADHD symptom dimensions of inattention and hyperactivity: A meta-analysis. J. Abnorm. Psychol. 2010, 119, 1–17. [Google Scholar] [CrossRef]
- Taylor, M.J.; Martin, J.; Lu, Y.; Brikell, I.; Lundstrom, S.; Larsson, H.; Lichtenstein, P. Association of Genetic Risk Factors for Psychiatric Disorders and Traits of These Disorders in a Swedish Population Twin Sample. JAMA Psychiatry 2019, 76, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Demontis, D.; Walters, R.K.; Martin, J.; Mattheisen, M.; Als, T.D.; Agerbo, E.; Baldursson, G.; Belliveau, R.; Bybjerg-Grauholm, J.; Baekvad-Hansen, M.; et al. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat. Genet. 2019, 51, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Middeldorp, C.M.; Hammerschlag, A.R.; Ouwens, K.G.; Groen-Blokhuis, M.M.; Pourcain, B.S.; Greven, C.U.; Pappa, I.; Tiesler, C.M.T.; Ang, W.; Nolte, I.M.; et al. A Genome-Wide Association Meta-Analysis of Attention-Deficit/Hyperactivity Disorder Symptoms in Population-Based Pediatric Cohorts. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 896–905. [Google Scholar] [CrossRef] [Green Version]
- Lange, K.W.; Reichl, S.; Lange, K.M.; Tucha, L.; Tucha, O. The history of attention deficit hyperactivity disorder. Atten. Deficit Hyperact. Disord. 2010, 2, 241–255. [Google Scholar] [CrossRef] [Green Version]
- Wolraich, M.L.; Chan, E.; Froehlich, T.; Lynch, R.L.; Bax, A.; Redwine, S.T.; Ihyembe, D.; Hagan, J.F., Jr. ADHD Diagnosis and Treatment Guidelines: A Historical Perspective. Pediatrics 2019, 144, e20191682. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychological Association: Washington, DC, USA, 2013. [Google Scholar]
- Agnew-Blais, J.C.; Polanczyk, G.V.; Danese, A.; Wertz, J.; Moffitt, T.E.; Arseneault, L. Evaluation of the Persistence, Remission, and Emergence of Attention-Deficit/Hyperactivity Disorder in Young Adulthood. JAMA Psychiatry 2016, 73, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Reilly, C.; Atkinson, P.; Das, K.B.; Chin, R.F.; Aylett, S.E.; Burch, V.; Gillberg, C.; Scott, R.C.; Neville, B.G. Neurobehavioral comorbidities in children with active epilepsy: A population-based study. Pediatrics 2014, 133, e1586–e1593. [Google Scholar] [CrossRef] [Green Version]
- Bennett-Back, O.; Keren, A.; Zelnik, N. Attention-deficit hyperactivity disorder in children with benign epilepsy and their siblings. Pediatr. Neurol. 2011, 44, 187–192. [Google Scholar] [CrossRef]
- Davies, S.; Heyman, I.; Goodman, R. A population survey of mental health problems in children with epilepsy. Dev. Med. Child Neurol. 2003, 45, 292–295. [Google Scholar] [CrossRef]
- Han, Y.; Qin, J.; Jiang, Y.W.; Chen, J.; Ji, X.N.; Lin, Q. Co-morbidity of attention deficit hyperactivity disorder in children with epilepsy. Zhongguo Dang Dai Er Ke Za Zhi 2012, 14, 89–92. [Google Scholar]
- Koneski, J.A.; Casella, E.B. Attention deficit and hyperactivity disorder in people with epilepsy: Diagnosis and implications to the treatment. Arq. Neuropsiquiatr. 2010, 68, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Shamsaei, F.; Cheraghi, F.; Zamani, G. Comparing Mental Health of School-Age Children with and without Epilepsy. Iran. J. Child Neurol. 2016, 10, 35–41. [Google Scholar] [PubMed]
- Zhao, Q.; Wang, M.; Kang, H.; Zhu, S. Behavior problems in children with epilepsy and attention-deficit hyperactivity disorder in Central China. Epilepsy Behav. 2018, 89, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Hermann, B.; Jones, J.; Dabbs, K.; Allen, C.A.; Sheth, R.; Fine, J.; McMillan, A.; Seidenberg, M. The frequency, complications and aetiology of ADHD in new onset paediatric epilepsy. Brain 2007, 130, 3135–3148. [Google Scholar] [CrossRef] [Green Version]
- Bechtel, N.; Weber, P. Attention problems in children with epilepsy. How is the long-term outcome? Eur. J. Paediatr. Neurol. 2015, 19, 383–385. [Google Scholar] [CrossRef]
- Gonzalez-Heydrich, J.; Dodds, A.; Whitney, J.; MacMillan, C.; Waber, D.; Faraone, S.V.; Boyer, K.; Mrakotsky, C.; DeMaso, D.; Bourgeois, B.; et al. Psychiatric disorders and behavioral characteristics of pediatric patients with both epilepsy and attention-deficit hyperactivity disorder. Epilepsy Behav. 2007, 10, 384–388. [Google Scholar] [CrossRef] [Green Version]
- Hesdorffer, D.C.; Ludvigsson, P.; Olafsson, E.; Gudmundsson, G.; Kjartansson, O.; Hauser, W.A. ADHD as a risk factor for incident unprovoked seizures and epilepsy in children. Arch. Gen. Psychiatry 2004, 61, 731–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danhofer, P.; Pejcochova, J.; Dusek, L.; Rektor, I.; Oslejskova, H. The influence of EEG-detected nocturnal centrotemporal discharges on the expression of core symptoms of ADHD in children with benign childhood epilepsy with centrotemporal spikes (BCECTS): A prospective study in a tertiary referral center. Epilepsy Behav. 2018, 79, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Kral, M.C.; Lally, M.D.; Boan, A.D. Identification of ADHD in youth with epilepsy. J. Pediatr. Rehabil. Med. 2016, 9, 223–229. [Google Scholar] [CrossRef] [Green Version]
- Auvin, S.; Wirrell, E.; Donald, K.A.; Berl, M.; Hartmann, H.; Valente, K.D.; Van Bogaert, P.; Cross, J.H.; Osawa, M.; Kanemura, H.; et al. Systematic review of the screening, diagnosis, and management of ADHD in children with epilepsy. Consensus paper of the Task Force on Comorbidities of the ILAE Pediatric Commission. Epilepsia 2018, 59, 1867–1880. [Google Scholar] [CrossRef] [Green Version]
- Gascoigne, M.B.; Smith, M.L.; Barton, B.; Webster, R.; Gill, D.; Lah, S. Attention deficits in children with epilepsy: Preliminary findings. Epilepsy Behav. 2017, 67, 7–12. [Google Scholar] [CrossRef]
- Kernan, C.L.; Asarnow, R.; Siddarth, P.; Gurbani, S.; Lanphier, E.K.; Sankar, R.; Caplan, R. Neurocognitive profiles in children with epilepsy. Epilepsia 2012, 53, 2156–2163. [Google Scholar] [CrossRef] [PubMed]
- Fastenau, P.S.; Johnson, C.S.; Perkins, S.M.; Byars, A.W.; deGrauw, T.J.; Austin, J.K.; Dunn, D.W. Neuropsychological status at seizure onset in children: Risk factors for early cognitive deficits. Neurology 2009, 73, 526–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metz-Lutz, M.N.; Kleitz, C.; de Saint Martin, A.; Massa, R.; Hirsch, E.; Marescaux, C. Cognitive development in benign focal epilepsies of childhood. Dev. Neurosci. 1999, 21, 182–190. [Google Scholar] [CrossRef]
- Berl, M.M.; Terwilliger, V.; Scheller, A.; Sepeta, L.; Walkowiak, J.; Gaillard, W.D. Speed and complexity characterize attention problems in children with localization-related epilepsy. Epilepsia 2015, 56, 833–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCusker, C.G.; Kennedy, P.J.; Anderson, J.; Hicks, E.M.; Hanrahan, D. Adjustment in children with intractable epilepsy: Importance of seizure duration and family factors. Dev. Med. Child Neurol. 2002, 44, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.E.; Giust, J.M.; Kronenberger, W.G.; Dunn, D.W. Epilepsy and attention-deficit hyperactivity disorder: Links, risks, and challenges. Neuropsychiatr. Dis. Treat. 2016, 12, 287–296. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Heydrich, J.; Hamoda, H.M.; Luna, L.; Rao, S.; McClendon, J.; Rotella, P.; Waber, D.; Boyer, K.; Faraone, S.V.; Whitney, J.; et al. Elevated rates of ADHD in mothers of children with comorbid ADHD and epilepsy. Neuropsychiatry 2012, 2, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Kwong, K.L.; Lam, D.; Tsui, S.; Ngan, M.; Tsang, B.; Lai, T.S.; Lam, S.M. Self-esteem in adolescents with epilepsy: Psychosocial and seizure-related correlates. Epilepsy Behav. 2016, 63, 118–122. [Google Scholar] [CrossRef]
- Kaufmann, R.; Goldberg-Stern, H.; Shuper, A. Attention-deficit disorders and epilepsy in childhood: Incidence, causative relations and treatment possibilities. J. Child Neurol. 2009, 24, 727–733. [Google Scholar] [CrossRef]
- Chou, I.C.; Chang, Y.T.; Chin, Z.N.; Muo, C.H.; Sung, F.C.; Kuo, H.T.; Tsai, C.H.; Kao, C.H. Correlation between epilepsy and attention deficit hyperactivity disorder: A population-based cohort study. PLoS ONE 2013, 8, e57926. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.H.; Choi, Y.S.; Yoon, H.S.; Bahn, G.H. Clinical Impact of Epileptiform Discharge in Children with Attention-Deficit/Hyperactivity Disorder (ADHD). J. Child Neurol. 2016, 31, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, S.; Farello, G.; Operto, F.F.; Coppola, G.; Verrotti, A. What are the challenges with the pharmacological management of epilepsy in patients with Attention Deficit Hyperactivity Disorder (ADHD)? Expert Opin. Pharmacother. 2020, 21, 737–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, G.K.; Abdalla, A.A.; Mohamed, A.M.; Mohamed, L.A.; Shamaa, H.A. Relationship between time spent playing internet gaming apps and behavioral problems, sleep problems, alexithymia, and emotion dysregulations in children: A multicentre study. Child Adolesc. Psychiatry Ment. Health 2022, 16, 67. [Google Scholar] [CrossRef] [PubMed]
- Hernan, A.E.; Alexander, A.; Jenks, K.R.; Barry, J.; Lenck-Santini, P.P.; Isaeva, E.; Holmes, G.L.; Scott, R.C. Focal epileptiform activity in the prefrontal cortex is associated with long-term attention and sociability deficits. Neurobiol. Dis. 2014, 63, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Pineda, E.; Jentsch, J.D.; Shin, D.; Griesbach, G.; Sankar, R.; Mazarati, A. Behavioral impairments in rats with chronic epilepsy suggest comorbidity between epilepsy and attention deficit/hyperactivity disorder. Epilepsy Behav. 2014, 31, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Shimojima, K.; Okumura, A.; Mori, H.; Abe, S.; Ikeno, M.; Shimizu, T.; Yamamoto, T. De novo microdeletion of 5q14.3 excluding MEF2C in a patient with infantile spasms, microcephaly, and agenesis of the corpus callosum. Am. J. Med. Genet. A 2012, 158A, 2272–2276. [Google Scholar] [CrossRef]
- Liu, S.; Rao, S.; Xu, Y.; Li, J.; Huang, H.; Zhang, X.; Fu, H.; Wang, Q.; Cao, H.; Baranova, A.; et al. Identifying common genome-wide risk genes for major psychiatric traits. Hum. Genet. 2020, 139, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Morimoto, Y.; Yamamoto, N.; Tayama, T.; Ozawa, H.; Imamura, A. Overlap between Epilepsy and Neurodevelopmental Disorders: Insights from Clinical and Genetic Studies. In Epilepsy; Czuczwar, S.J., Ed.; Exon Publications: Brisbane, Australia, 2022. [Google Scholar]
- Halmoy, A.; Klungsoyr, K.; Skjaerven, R.; Haavik, J. Pre- and perinatal risk factors in adults with attention-deficit/hyperactivity disorder. Biol. Psychiatry 2012, 71, 474–481. [Google Scholar] [CrossRef]
- Brikell, I.; Ghirardi, L.; D’Onofrio, B.M.; Dunn, D.W.; Almqvist, C.; Dalsgaard, S.; Kuja-Halkola, R.; Larsson, H. Familial Liability to Epilepsy and Attention-Deficit/Hyperactivity Disorder: A Nationwide Cohort Study. Biol. Psychiatry 2018, 83, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, P.; Carlstrom, E.; Rastam, M.; Gillberg, C.; Anckarsater, H. The genetics of autism spectrum disorders and related neuropsychiatric disorders in childhood. Am. J. Psychiatry 2010, 167, 1357–1363. [Google Scholar] [CrossRef] [Green Version]
- Moreno-De-Luca, A.; Myers, S.M.; Challman, T.D.; Moreno-De-Luca, D.; Evans, D.W.; Ledbetter, D.H. Developmental brain dysfunction: Revival and expansion of old concepts based on new genetic evidence. Lancet Neurol. 2013, 12, 406–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, H.; Hao, N.; Liu, S.; Zhou, D. Seizure frequency and obstetric complications at advanced maternal age: A preliminary observational study in women with epilepsy. Acta Epileptol. 2021, 3, 17. [Google Scholar] [CrossRef]
- Heaney, D.C.; MacDonald, B.K.; Everitt, A.; Stevenson, S.; Leonardi, G.S.; Wilkinson, P.; Sander, J.W. Socioeconomic variation in incidence of epilepsy: Prospective community based study in south east England. BMJ 2002, 325, 1013–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jett, D.A. Chemical toxins that cause seizures. Neurotoxicology 2012, 33, 1473–1475. [Google Scholar] [CrossRef]
- Morgan, C.L.; Ahmed, Z.; Kerr, M.P. Social deprivation and prevalence of epilepsy and associated health usage. J. Neurol. Neurosurg. Psychiatry 2000, 69, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Vestergaard, M.; Pedersen, C.B.; Christensen, J.; Basso, O.; Olsen, J. Gestational age, birth weight, intrauterine growth, and the risk of epilepsy. Am. J. Epidemiol. 2008, 167, 262–270. [Google Scholar] [CrossRef] [Green Version]
- England, M.J.; Liverman, C.T.; Schultz, A.M.; Strawbridge, L.M. Epilepsy across the spectrum: Promoting health and understanding. A summary of the Institute of Medicine report. Epilepsy Behav. 2012, 25, 266–276. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.T.; Tsai, F.J.; Lee, W.T.; Lee, C.M.; Fan, P.C.; Lin, W.S.; Chiu, Y.N.; Gau, S.S. Attentional processes and ADHD-related symptoms in pediatric patients with epilepsy. Epilepsy Res. 2011, 93, 53–65. [Google Scholar] [CrossRef]
- Bhise, V.V.; Burack, G.D.; Mandelbaum, D.E. Baseline cognition, behavior, and motor skills in children with new-onset, idiopathic epilepsy. Dev. Med. Child Neurol. 2010, 52, 22–26. [Google Scholar] [CrossRef]
- Jeong, M.H.; Yum, M.S.; Ko, T.S.; You, S.J.; Lee, E.H.; Yoo, H.K. Neuropsychological status of children with newly diagnosed idiopathic childhood epilepsy. Brain Dev. 2011, 33, 666–671. [Google Scholar] [CrossRef]
- MacAllister, W.S.; Schaffer, S.G. Neuropsychological deficits in childhood epilepsy syndromes. Neuropsychol. Rev. 2007, 17, 427–444. [Google Scholar] [CrossRef] [PubMed]
- You, S.J. Cognitive function of idiopathic childhood epilepsy. Korean J. Pediatr. 2012, 55, 159–163. [Google Scholar] [CrossRef]
- McWilliam, M.; Al Khalili, Y. Idiopathic (Genetic) Generalized Epilepsy; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Jawaid, W.; Nisa, Q.; Umer, S.R.; Barry, S.J.; Qureshi, A.; Shahbaz, N.N. Etiology and Types of Seizures in Patients Presenting to a Tertiary Care Hospital in Karachi: A Cross-Sectional Study. Cureus 2020, 12, e9194. [Google Scholar] [CrossRef]
- Hermann, B.P.; Jones, J.E.; Sheth, R.; Koehn, M.; Becker, T.; Fine, J.; Allen, C.A.; Seidenberg, M. Growing up with epilepsy: A two-year investigation of cognitive development in children with new onset epilepsy. Epilepsia 2008, 49, 1847–1858. [Google Scholar] [CrossRef] [PubMed]
- Schubert, R. Attention deficit disorder and epilepsy. Pediatr. Neurol. 2005, 32, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Manford, M.; Hart, Y.M.; Sander, J.W.; Shorvon, S.D. National General Practice Study of Epilepsy (NGPSE): Partial seizure patterns in a general population. Neurology 1992, 42, 1911–1917. [Google Scholar] [CrossRef]
- Chayer, C.; Freedman, M. Frontal lobe functions. Curr. Neurol. Neurosci. Rep. 2001, 1, 547–552. [Google Scholar] [CrossRef]
- Gold, J.A.; Sher, Y.; Maldonado, J.R. Frontal Lobe Epilepsy: A Primer for Psychiatrists and a Systematic Review of Psychiatric Manifestations. Psychosomatics 2016, 57, 445–464. [Google Scholar] [CrossRef]
- Holmes, G.L.; Lenck-Santini, P.P. Role of interictal epileptiform abnormalities in cognitive impairment. Epilepsy Behav. 2006, 8, 504–515. [Google Scholar] [CrossRef]
- Ben-Ari, Y.; Holmes, G.L. Effects of seizures on developmental processes in the immature brain. Lancet Neurol. 2006, 5, 1055–1063. [Google Scholar] [CrossRef]
- Ryvlin, P.; Rheims, S.; Risse, G. Nocturnal frontal lobe epilepsy. Epilepsia 2006, 47 (Suppl. 2), 83–86. [Google Scholar] [CrossRef] [PubMed]
- D’Agati, E.; Moavero, R.; Cerminara, C.; Curatolo, P. Attention-deficit hyperactivity disorder (ADHD) and tuberous sclerosis complex. J. Child Neurol. 2009, 24, 1282–1287. [Google Scholar] [CrossRef]
- Loiseau, P.; Duche, B.; Pedespan, J.M. Absence epilepsies. Epilepsia 1995, 36, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Sadleir, L.G.; Farrell, K.; Smith, S.; Connolly, M.B.; Scheffer, I.E. Electroclinical features of absence seizures in childhood absence epilepsy. Neurology 2006, 67, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Caplan, R.; Siddarth, P.; Stahl, L.; Lanphier, E.; Vona, P.; Gurbani, S.; Koh, S.; Sankar, R.; Shields, W.D. Childhood absence epilepsy: Behavioral, cognitive, and linguistic comorbidities. Epilepsia 2008, 49, 1838–1846. [Google Scholar] [CrossRef]
- Loiseau, P.; Duche, B. Benign rolandic epilepsy. Adv. Neurol. 1992, 57, 411–417. [Google Scholar]
- Guerrini, R.; Pellacani, S. Benign childhood focal epilepsies. Epilepsia 2012, 53 (Suppl. 4), 9–18. [Google Scholar] [CrossRef]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. Lancet Psychiatry 2018, 5, 727–738. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Attention Deficit Hyperactivity Disorder: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/ng87/resources/attention-deficit-hyperactivity-disorder-diagnosis-and-management-pdf-1837699732933 (accessed on 2 March 2023).
- Koneski, J.A.; Casella, E.B.; Agertt, F.; Ferreira, M.G. Efficacy and safety of methylphenidate in treating ADHD symptoms in children and adolescents with uncontrolled seizures: A Brazilian sample study and literature review. Epilepsy Behav. 2011, 21, 228–232. [Google Scholar] [CrossRef]
- Park, J.; Choi, H.W.; Yum, M.S.; Ko, T.S.; Shon, S.H.; Kim, H.W. Relationship between Aggravation of Seizures and Methylphenidate Treatment in Subjects with Attention-Deficit/Hyperactivity Disorder and Epilepsy. J. Child Adolesc. Psychopharmacol. 2018, 28, 537–546. [Google Scholar] [CrossRef]
- Faraone, S.V. The pharmacology of amphetamine and methylphenidate: Relevance to the neurobiology of attention-deficit/hyperactivity disorder and other psychiatric comorbidities. Neurosci. Biobehav. Rev. 2018, 87, 255–270. [Google Scholar] [CrossRef]
- Mohammadi, M.R.; Akhondzadeh, S. Pharmacotherapy of attention-deficit/hyperactivity disorder: Nonstimulant medication approaches. Expert Rev. Neurother. 2007, 7, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.; Crumrine, P.; Handen, B.L.; Alvin, R.; Teodori, J. Methylphenidate in children with seizures and attention-deficit disorder. Am. J. Dis. Child 1989, 143, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Heydrich, J.; Whitney, J.; Waber, D.; Forbes, P.; Hsin, O.; Faraone, S.V.; Dodds, A.; Rao, S.; Mrakotsky, C.; Macmillan, C.; et al. Adaptive phase I study of OROS methylphenidate treatment of attention deficit hyperactivity disorder with epilepsy. Epilepsy Behav. 2010, 18, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Rheims, S.; Herbillon, V.; Villeneuve, N.; Auvin, S.; Napuri, S.; Cances, C.; Berquin, P.; Castelneau, P.; Nguyen The Tich, S.; Villega, F.; et al. ADHD in childhood epilepsy: Clinical determinants of severity and of the response to methylphenidate. Epilepsia 2016, 57, 1069–1077. [Google Scholar] [CrossRef]
- Heidbreder, R. ADHD symptomatology is best conceptualized as a spectrum: A dimensional versus unitary approach to diagnosis. Atten. Deficit Hyperact. Disord. 2015, 7, 249–269. [Google Scholar] [CrossRef] [PubMed]
- Fosi, T.; Lax-Pericall, M.T.; Scott, R.C.; Neville, B.G.; Aylett, S.E. Methylphenidate treatment of attention deficit hyperactivity disorder in young people with learning disability and difficult-to-treat epilepsy: Evidence of clinical benefit. Epilepsia 2013, 54, 2071–2081. [Google Scholar] [CrossRef] [Green Version]
- Santos, K.; Palmini, A.; Radziuk, A.L.; Rotert, R.; Bastos, F.; Booij, L.; Fernandes, B.S. The impact of methylphenidate on seizure frequency and severity in children with attention-deficit-hyperactivity disorder and difficult-to-treat epilepsies. Dev. Med. Child Neurol. 2013, 55, 654–660. [Google Scholar] [CrossRef]
- Paterson, R.; Douglas, C.; Hallmayer, J.; Hagan, M.; Krupenia, Z. A randomised, double-blind, placebo-controlled trial of dexamphetamine in adults with attention deficit hyperactivity disorder. Aust. N. Z. J. Psychiatry 1999, 33, 494–502. [Google Scholar] [CrossRef]
- Taylor, F.B. Comparing guanfacine and dextroamphetamine for adult ADHD: Efficacy and implications. In Proceedings of the 153rd Annual Meeting of the American Psychiatric Association, Chicago, IL, USA, 13–18 May 2000; p. NR 658. [Google Scholar]
- Gonzalez-Heydrich, J.; Hsin, O.; Gumlak, S.; Kimball, K.; Rober, A.; Azeem, M.W.; Hickory, M.; Mrakotsky, C.; Torres, A.; Mezzacappa, E.; et al. Comparing stimulant effects in youth with ADHD symptoms and epilepsy. Epilepsy Behav. 2014, 36, 102–107. [Google Scholar] [CrossRef] [Green Version]
- Chamberlain, R.W. Letter: Convulsions and ritalin? Pediatrics 1974, 54, 658–659. [Google Scholar] [CrossRef] [PubMed]
- Feeney, D.J.; Klykylo, W.M. Medication-induced seizures. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 1018–1019. [Google Scholar] [CrossRef]
- Tavakoli, S.A.; Gleason, O.C. Seizures associated with venlafaxine, methylphenidate, and zolpidem. Psychosomatics 2003, 44, 262–264. [Google Scholar] [CrossRef]
- Klein-Schwartz, W. Abuse and toxicity of methylphenidate. Curr. Opin. Pediatr. 2002, 14, 219–223. [Google Scholar] [CrossRef]
- Gray, S.D.; Fatovich, D.M.; McCoubrie, D.L.; Daly, F.F. Amphetamine-related presentations to an inner-city tertiary emergency department: A prospective evaluation. Med. J. Aust. 2007, 186, 336–339. [Google Scholar] [CrossRef]
- Gross-Tsur, V.; Manor, O.; van der Meere, J.; Joseph, A.; Shalev, R.S. Epilepsy and attention deficit hyperactivity disorder: Is methylphenidate safe and effective? J. Pediatr. 1997, 130, 40–44. [Google Scholar] [CrossRef]
- Torres, A.R.; Whitney, J.; Gonzalez-Heydrich, J. Attention-deficit/hyperactivity disorder in pediatric patients with epilepsy: Review of pharmacological treatment. Epilepsy Behav. 2008, 12, 217–233. [Google Scholar] [CrossRef]
- Radziuk, A.L.; Kieling, R.R.; Santos, K.; Rotert, R.; Bastos, F.; Palmini, A.L. Methylphenidate improves the quality of life of children and adolescents with ADHD and difficult-to-treat epilepsies. Epilepsy Behav. 2015, 46, 215–220. [Google Scholar] [CrossRef]
- Wroblewski, B.A.; Leary, J.M.; Phelan, A.M.; Whyte, J.; Manning, K. Methylphenidate and seizure frequency in brain injured patients with seizure disorders. J. Clin. Psychiatry 1992, 53, 86–89. [Google Scholar]
- Gucuyener, K.; Erdemoglu, A.K.; Senol, S.; Serdaroglu, A.; Soysal, S.; Kockar, A.I. Use of methylphenidate for attention-deficit hyperactivity disorder in patients with epilepsy or electroencephalographic abnormalities. J. Child Neurol. 2003, 18, 109–112. [Google Scholar] [CrossRef]
- Hemmer, S.A.; Pasternak, J.F.; Zecker, S.G.; Trommer, B.L. Stimulant therapy and seizure risk in children with ADHD. Pediatr. Neurol. 2001, 24, 99–102. [Google Scholar] [CrossRef]
- van der Feltz-Cornelis, C.M.; Aldenkamp, A.P. Effectiveness and safety of methylphenidate in adult attention deficit hyperactivity disorder in patients with epilepsy: An open treatment trial. Epilepsy Behav. 2006, 8, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Wiggs, K.K.; Chang, Z.; Quinn, P.D.; Hur, K.; Gibbons, R.; Dunn, D.; Brikell, I.; Larsson, H.; D’Onofrio, B.M. Attention-deficit/hyperactivity disorder medication and seizures. Neurology 2018, 90, e1104–e1110. [Google Scholar] [CrossRef] [Green Version]
- Yoo, H.K.; Park, S.; Wang, H.R.; Lee, J.S.; Kim, K.; Paik, K.W.; Yum, M.S.; Ko, T.S. Effect of methylphenidate on the quality of life in children with epilepsy and attention deficit hyperactivity disorder: And open-label study using an osmotic-controlled release oral delivery system. Epileptic. Disord. 2009, 11, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Carney, P.R.; Bussing, R.; Segal, R.; Cottler, L.B.; Winterstein, A.G. Stimulants Do Not Increase the Risk of Seizure-Related Hospitalizations in Children with Epilepsy. J. Child Adolesc. Psychopharmacol. 2018, 28, 111–116. [Google Scholar] [CrossRef]
- Ravi, M.; Ickowicz, A. Epilepsy, Attention-Deficit/Hyperactivity Disorder and Methylphenidate: Critical Examination of Guiding Evidence. J. Can. Acad. Child Adolesc. Psychiatry 2016, 25, 50–58. [Google Scholar]
- Curatolo, P.; D’Agati, E.; Moavero, R. The neurobiological basis of ADHD. Ital. J. Pediatr. 2010, 36, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamond, A. Attention-deficit disorder (attention-deficit/hyperactivity disorder without hyperactivity): A neurobiologically and behaviorally distinct disorder from attention-deficit/hyperactivity disorder (with hyperactivity). Dev. Psychopathol. 2005, 17, 807–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Hakoda, Y. Executive and Non-Executive Functions in Attention Deficit Hyperactivity Disorder of the Inattentive Type (ADHD-I): A Cognitive Profile. J. Behav. Brain Sci. 2014, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sonuga-Barke, E.J.; Koerting, J.; Smith, E.; McCann, D.C.; Thompson, M. Early detection and intervention for attention-deficit/hyperactivity disorder. Expert Rev. Neurother. 2011, 11, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Pliszka, S.; Issues, A.W.G.o.Q. Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 894–921. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, M.; Brown, L.; Brown, R.T.; DuPaul, G.; Earls, M.; Feldman, H.M.; Ganiats, T.G.; Kaplanek, B.; Subcommittee on Attention-Deficit/Hyperactivity Disorder; Steering Committee on Quality Improvement and Management; et al. ADHD: Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 2011, 128, 1007–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flowers, A.; McDougle, L. In search of an ADHD screening tool for African American children. J. Natl. Med. Assoc. 2010, 102, 372–374. [Google Scholar] [CrossRef] [PubMed]
- Freeman, N.C.; Gray, K.M.; Taffe, J.R.; Cornish, K.M. Development of a New Attention Rating Scale for Children with Intellectual Disability: The Scale of Attention in Intellectual Disability (SAID). Am. J. Intellect. Dev. Disabil. 2015, 120, 91–109. [Google Scholar] [CrossRef]
- Masur, D.; Shinnar, S.; Cnaan, A.; Shinnar, R.C.; Clark, P.; Wang, J.; Weiss, E.F.; Hirtz, D.G.; Glauser, T.A.; Childhood Absence Epilepsy Study, G. Pretreatment cognitive deficits and treatment effects on attention in childhood absence epilepsy. Neurology 2013, 81, 1572–1580. [Google Scholar] [CrossRef] [Green Version]
- Meador, K.J. Newer anticonvulsants: Dosing strategies and cognition in treating patients with mood disorders and epilepsy. J. Clin. Psychiatry 2003, 64 (Suppl. 8), 30–34. [Google Scholar]
- Ekinci, O.; Isik, U.; Gunes, S.; Ekinci, N. Understanding sleep problems in children with epilepsy: Associations with quality of life, Attention-Deficit Hyperactivity Disorder and maternal emotional symptoms. Seizure 2016, 40, 108–113. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, W.G.; Chavez, J.M.; Lee, H.; Guzman, B.L. Academic underachievement in children with epilepsy. J. Child Neurol. 1991, 6, 65–72. [Google Scholar] [CrossRef]
- Pellock, J.M. Defining the problem: Psychiatric and behavioral comorbidity in children and adolescents with epilepsy. Epilepsy Behav. 2004, 5 (Suppl. 3), S3–S9. [Google Scholar] [CrossRef]
- Pellock, J.M. Understanding co-morbidities affecting children with epilepsy. Neurology 2004, 62, S17–S23. [Google Scholar] [CrossRef]
- Salpekar, J.A.; Mishra, G. Key issues in addressing the comorbidity of attention deficit hyperactivity disorder and pediatric epilepsy. Epilepsy Behav. 2014, 37, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Gomer, B.; Wagner, K.; Frings, L.; Saar, J.; Carius, A.; Harle, M.; Steinhoff, B.J.; Schulze-Bonhage, A. The influence of antiepileptic drugs on cognition: A comparison of levetiracetam with topiramate. Epilepsy Behav. 2007, 10, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Bush, G.; Spencer, T.J.; Holmes, J.; Shin, L.M.; Valera, E.M.; Seidman, L.J.; Makris, N.; Surman, C.; Aleardi, M.; Mick, E.; et al. Functional magnetic resonance imaging of methylphenidate and placebo in attention-deficit/hyperactivity disorder during the multi-source interference task. Arch. Gen. Psychiatry 2008, 65, 102–114. [Google Scholar] [CrossRef] [Green Version]
- Pliszka, S.R. The neuropsychopharmacology of attention-deficit/hyperactivity disorder. Biol. Psychiatry 2005, 57, 1385–1390. [Google Scholar] [CrossRef]
- Wernicke, J.F.; Holdridge, K.C.; Jin, L.; Edison, T.; Zhang, S.; Bangs, M.E.; Allen, A.J.; Ball, S.; Dunn, D. Seizure risk in patients with attention-deficit-hyperactivity disorder treated with atomoxetine. Dev. Med. Child Neurol. 2007, 49, 498–502. [Google Scholar] [CrossRef]
- Parisi, P.; Moavero, R.; Verrotti, A.; Curatolo, P. Attention deficit hyperactivity disorder in children with epilepsy. Brain Dev. 2010, 32, 10–16. [Google Scholar] [CrossRef]
- Kolar, D.; Keller, A.; Golfinopoulos, M.; Cumyn, L.; Syer, C.; Hechtman, L. Treatment of adults with attention-deficit/hyperactivity disorder. Neuropsychiatr. Dis. Treat. 2008, 4, 107–121. [Google Scholar] [CrossRef] [Green Version]
- Bymaster, F.P.; Golembiowska, K.; Kowalska, M.; Choi, Y.K.; Tarazi, F.I. Pharmacological characterization of the norepinephrine and dopamine reuptake inhibitor EB-1020: Implications for treatment of attention-deficit hyperactivity disorder. Synapse 2012, 66, 522–532. [Google Scholar] [CrossRef]
- Adler, L.A.; Clemow, D.B.; Williams, D.W.; Durell, T.M. Atomoxetine effects on executive function as measured by the BRIEF-a in young adults with ADHD: A randomized, double-blind, placebo-controlled study. PLoS ONE 2014, 9, e104175. [Google Scholar] [CrossRef]
- Clemow, D.B.; Bushe, C.J. Atomoxetine in patients with ADHD: A clinical and pharmacological review of the onset, trajectory, duration of response and implications for patients. J. Psychopharmacol. 2015, 29, 1221–1230. [Google Scholar] [CrossRef]
- Michelson, D.; Adler, L.; Spencer, T.; Reimherr, F.W.; West, S.A.; Allen, A.J.; Kelsey, D.; Wernicke, J.; Dietrich, A.; Milton, D. Atomoxetine in adults with ADHD: Two randomized, placebo-controlled studies. Biol. Psychiatry 2003, 53, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Young, J.L.; Sarkis, E.; Qiao, M.; Wietecha, L. Once-daily treatment with atomoxetine in adults with attention-deficit/hyperactivity disorder: A 24-week, randomized, double-blind, placebo-controlled trial. Clin. Neuropharmacol. 2011, 34, 51–60. [Google Scholar] [CrossRef]
- Palumbo, D.R.; Sallee, F.R.; Pelham, W.E., Jr.; Bukstein, O.G.; Daviss, W.B.; Mc, D.M.; Cat Study, T. Clonidine for attention-deficit/hyperactivity disorder: I. Efficacy and tolerability outcomes. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 180–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strange, B.C. Once-daily treatment of ADHD with guanfacine: Patient implications. Neuropsychiatr. Dis. Treat. 2008, 4, 499–506. [Google Scholar] [CrossRef] [Green Version]
- Cruz, M.P. Guanfacine Extended-Release Tablets (Intuniv), a Nonstimulant Selective Alpha(2A)-Adrenergic Receptor Agonist for Attention-Deficit/Hyperactivity Disorder. P T 2010, 35, 448–451. [Google Scholar]
- Tourette’s Syndrome Study, G. Treatment of ADHD in children with tics: A randomized controlled trial. Neurology 2002, 58, 527–536. [Google Scholar] [CrossRef]
- Ming, X.; Mulvey, M.; Mohanty, S.; Patel, V. Safety and efficacy of clonidine and clonidine extended-release in the treatment of children and adolescents with attention deficit and hyperactivity disorders. Adolesc. Health Med. Ther. 2011, 2, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Connor, D.F.; Fletcher, K.E.; Swanson, J.M. A meta-analysis of clonidine for symptoms of attention-deficit hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1551–1559. [Google Scholar] [CrossRef]
- Hazell, P.L.; Stuart, J.E. A randomized controlled trial of clonidine added to psychostimulant medication for hyperactive and aggressive children. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 886–894. [Google Scholar] [CrossRef]
- Sallee, F.R. The role of alpha2-adrenergic agonists in attention-deficit/hyperactivity disorder. Postgrad. Med. 2010, 122, 78–87. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.; Brandeis, D.; Cortese, S.; Daley, D.; Ferrin, M.; Holtmann, M.; Stevenson, J.; Danckaerts, M.; van der Oord, S.; Dopfner, M.; et al. Nonpharmacological interventions for ADHD: Systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am. J. Psychiatry 2013, 170, 275–289. [Google Scholar] [CrossRef] [PubMed]
- Catala-Lopez, F.; Hutton, B.; Nunez-Beltran, A.; Page, M.J.; Ridao, M.; Macias Saint-Gerons, D.; Catala, M.A.; Tabares-Seisdedos, R.; Moher, D. The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: A systematic review with network meta-analyses of randomised trials. PLoS ONE 2017, 12, e0180355. [Google Scholar] [CrossRef] [Green Version]
- Kanner, A.M.; Gidal, B.E. Pharmacodynamic and pharmacokinetic interactions of psychotropic drugs with antiepileptic drugs. Int. Rev. Neurobiol. 2008, 83, 397–416. [Google Scholar] [CrossRef]
- Markowitz, J.S.; Morrison, S.D.; DeVane, C.L. Drug interactions with psychostimulants. Int. Clin. Psychopharmacol. 1999, 14, 1–18. [Google Scholar] [CrossRef]
- Fan, H.C.; Lee, H.S.; Chang, K.P.; Lee, Y.Y.; Lai, H.C.; Hung, P.L.; Lee, H.F.; Chi, C.S. The Impact of Anti-Epileptic Drugs on Growth and Bone Metabolism. Int. J. Mol. Sci. 2016, 17, 1242. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Clinical Excellence Epilepsies: 5 Treating Epileptic Seizures in Children, Young People and Adults. Available online: https://www.nice.org.uk/guidance/ng217/chapter/5-Treating-epileptic-seizures-in-children-young-people-and-adults#generalised-tonic-clonic-seizures (accessed on 2 March 2023).
- Marson, A.G.; Al-Kharusi, A.M.; Alwaidh, M.; Appleton, R.; Baker, G.A.; Chadwick, D.W.; Cramp, C.; Cockerell, O.C.; Cooper, P.N.; Doughty, J.; et al. The SANAD study of effectiveness of carbamazepine, gabapentin, lamotrigine, oxcarbazepine, or topiramate for treatment of partial epilepsy: An unblinded randomised controlled trial. Lancet 2007, 369, 1000–1015. [Google Scholar] [CrossRef] [Green Version]
- Marson, A.G.; Al-Kharusi, A.M.; Alwaidh, M.; Appleton, R.; Baker, G.A.; Chadwick, D.W.; Cramp, C.; Cockerell, O.C.; Cooper, P.N.; Doughty, J.; et al. The SANAD study of effectiveness of valproate, lamotrigine, or topiramate for generalised and unclassifiable epilepsy: An unblinded randomised controlled trial. Lancet 2007, 369, 1016–1026. [Google Scholar] [CrossRef] [Green Version]
- Marson, A.G.; Burnside, G.; Appleton, R.; Smith, D.; Leach, J.P.; Sills, G.; Tudur-Smith, C.; Plumpton, C.O.; Hughes, D.A.; Williamson, P.R.; et al. Lamotrigine versus levetiracetam or zonisamide for focal epilepsy and valproate versus levetiracetam for generalised and unclassified epilepsy: Two SANAD II non-inferiority RCTs. Health Technol. Assess. 2021, 25, 1–134. [Google Scholar] [CrossRef]
- Steinhoff, B.J.; Ueberall, M.A.; Siemes, H.; Kurlemann, G.; Schmitz, B.; Bergmann, L.; Group, L.-S.S. The LAM-SAFE Study: Lamotrigine versus carbamazepine or valproic acid in newly diagnosed focal and generalised epilepsies in adolescents and adults. Seizure 2005, 14, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Guo, C.Y.; Ronen, G.M.; Atkinson, S.A. Long-term valproate and lamotrigine treatment may be a marker for reduced growth and bone mass in children with epilepsy. Epilepsia 2001, 42, 1141–1147. [Google Scholar] [CrossRef] [Green Version]
- Mitra-Ghosh, T.; Callisto, S.P.; Lamba, J.K.; Remmel, R.P.; Birnbaum, A.K.; Barbarino, J.M.; Klein, T.E.; Altman, R.B. PharmGKB summary: Lamotrigine pathway, pharmacokinetics and pharmacodynamics. Pharm. Genom. 2020, 30, 81–90. [Google Scholar] [CrossRef]
- Zamponi, G.W. Targeting voltage-gated calcium channels in neurological and psychiatric diseases. Nat. Rev. Drug Discov. 2016, 15, 19–34. [Google Scholar] [CrossRef]
- Han, J.H.; Oh, J.E.; Kim, S.J. Clinical efficacy and safety of lamotrigine monotherapy in newly diagnosed pediatric patients with epilepsy. Korean J. Pediatr. 2010, 53, 565–570. [Google Scholar] [CrossRef]
- Han, S.A.; Yang, E.J.; Song, M.K.; Kim, S.J. Effects of lamotrigine on attention-deficit hyperactivity disorder in pediatric epilepsy patients. Korean J. Pediatr. 2017, 60, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Oncu, B.; Er, O.; Colak, B.; Nutt, D.J. Lamotrigine for attention deficit-hyperactivity disorder comorbid with mood disorders: A case series. J. Psychopharmacol. 2014, 28, 282–283. [Google Scholar] [CrossRef]
- Uvebrant, P.; Bauziene, R. Intractable epilepsy in children. The efficacy of lamotrigine treatment, including non-seizure-related benefits. Neuropediatrics 1994, 25, 284–289. [Google Scholar] [CrossRef]
- Ross, D.C.; Fischhoff, J.; Davenport, B. Treatment of ADHD when tolerance to methylphenidate develops. Psychiatr. Serv. 2002, 53, 102. [Google Scholar] [CrossRef]
- Pennick, M. Absorption of lisdexamfetamine dimesylate and its enzymatic conversion to d-amphetamine. Neuropsychiatr. Dis. Treat. 2010, 6, 317–327. [Google Scholar] [CrossRef] [Green Version]
- Ichikawa, H.; Miyajima, T.; Yamashita, Y.; Fujiwara, M.; Fukushi, A.; Saito, K. Long-term study of lisdexamfetamine dimesylate in Japanese children and adolescents with attention-deficit/hyperactivity disorder. Neuropsychopharmacol. Rep. 2020, 40, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Dittmann, R.W.; Cardo, E.; Nagy, P.; Anderson, C.S.; Bloomfield, R.; Caballero, B.; Higgins, N.; Hodgkins, P.; Lyne, A.; Civil, R.; et al. Efficacy and safety of lisdexamfetamine dimesylate and atomoxetine in the treatment of attention-deficit/hyperactivity disorder: A head-to-head, randomized, double-blind, phase IIIb study. CNS Drugs 2013, 27, 1081–1092. [Google Scholar] [CrossRef] [Green Version]
- Coghill, D.; Banaschewski, T.; Lecendreux, M.; Soutullo, C.; Johnson, M.; Zuddas, A.; Anderson, C.; Civil, R.; Higgins, N.; Lyne, A.; et al. European, randomized, phase 3 study of lisdexamfetamine dimesylate in children and adolescents with attention-deficit/hyperactivity disorder. Eur. Neuropsychopharmacol. 2013, 23, 1208–1218. [Google Scholar] [CrossRef] [Green Version]
- Biederman, J.; Krishnan, S.; Zhang, Y.; McGough, J.J.; Findling, R.L. Efficacy and tolerability of lisdexamfetamine dimesylate (NRP-104) in children with attention-deficit/hyperactivity disorder: A phase III, multicenter, randomized, double-blind, forced-dose, parallel-group study. Clin. Ther. 2007, 29, 450–463. [Google Scholar] [CrossRef]
- Babcock, T.; Dirks, B.; Adeyi, B.; Scheckner, B. Efficacy of lisdexamfetamine dimesylate in adults with attention-deficit/hyperactivity disorder previously treated with amphetamines: Analyses from a randomized, double-blind, multicenter, placebo-controlled titration study. BMC Pharmacol. Toxicol. 2012, 13, 18. [Google Scholar] [CrossRef] [Green Version]
- Adler, L.A.; Goodman, D.W.; Kollins, S.H.; Weisler, R.H.; Krishnan, S.; Zhang, Y.; Biederman, J.; Study, G. Double-blind, placebo-controlled study of the efficacy and safety of lisdexamfetamine dimesylate in adults with attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2008, 69, 1364–1373. [Google Scholar] [CrossRef] [Green Version]
- Madaan, V.; Kolli, V.; Bestha, D.P.; Shah, M.J. Update on optimal use of lisdexamfetamine in the treatment of ADHD. Neuropsychiatr. Dis. Treat. 2013, 9, 977–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edinoff, A.N.; Akuly, H.A.; Wagner, J.H.; Boudreaux, M.A.; Kaplan, L.A.; Yusuf, S.; Neuchat, E.E.; Cornett, E.M.; Boyer, A.G.; Kaye, A.M.; et al. Viloxazine in the Treatment of Attention Deficit Hyperactivity Disorder. Front. Psychiatry 2021, 12, 789982. [Google Scholar] [CrossRef]
- Lamb, Y.N. Viloxazine: Pediatric First Approval. Paediatr. Drugs 2021, 23, 403–409. [Google Scholar] [CrossRef]
- Yu, C.; Garcia-Olivares, J.; Candler, S.; Schwabe, S.; Maletic, V. New Insights into the Mechanism of Action of Viloxazine: Serotonin and Norepinephrine Modulating Properties. J. Exp. Pharmacol. 2020, 12, 285–300. [Google Scholar] [CrossRef]
- Faison, S.L.; Fry, N.; Adewole, T.; Odebo, O.; Wang, Z.; Maletic, V.; Nasser, A. Pharmacokinetics of Coadministered Viloxazine Extended-Release (SPN-812) and Lisdexamfetamine in Healthy Adults. J. Clin. Psychopharmacol. 2021, 41, 155–162. [Google Scholar] [CrossRef]
- Braeckman, R.; Guenther, S.; Mickle, T.C.; Barrett, A.C.; Smith, A.; Oh, C. Dose Proportionality and Steady-State Pharmacokinetics of Serdexmethylphenidate/Dexmethylphenidate, a Novel Prodrug Combination to Treat Attention-Deficit/Hyperactivity Disorder. J. Child Adolesc. Psychopharmacol. 2022, 32, 288–295. [Google Scholar] [CrossRef]
- Kollins, S.H.; Braeckman, R.; Guenther, S.; Barrett, A.C.; Mickle, T.C.; Oh, C.; Marraffino, A.; Cutler, A.J.; Brams, M.N. A Randomized, Controlled Laboratory Classroom Study of Serdexmethylphenidate and d-Methylphenidate Capsules in Children with Attention-Deficit/Hyperactivity Disorder. J. Child Adolesc. Psychopharmacol. 2021, 31, 597–609. [Google Scholar] [CrossRef]
- Zhou, J. Norepinephrine transporter inhibitors and their therapeutic potential. Drugs Future 2004, 29, 1235–1244. [Google Scholar] [CrossRef]
- Wigal, T.L.; Newcorn, J.H.; Handal, N.; Wigal, S.B.; Mulligan, I.; Schmith, V.; Konofal, E. A Double-Blind, Placebo-Controlled, Phase II Study to Determine the Efficacy, Safety, Tolerability and Pharmacokinetics of a Controlled Release (CR) Formulation of Mazindol in Adults with DSM-5 Attention-Deficit/Hyperactivity Disorder (ADHD). CNS Drugs 2018, 32, 289–301. [Google Scholar] [CrossRef] [Green Version]
- Sakayori, T.; Tateno, A.; Arakawa, R.; Ikeda, Y.; Suzuki, H.; Okubo, Y. Effect of mazindol on extracellular dopamine concentration in human brain measured by PET. Psychopharmacology 2014, 231, 2321–2325. [Google Scholar] [CrossRef]
- Konofal, E.; Zhao, W.; Laouenan, C.; Lecendreux, M.; Kaguelidou, F.; Benadjaoud, L.; Mentre, F.; Jacqz-Aigrain, E. Pilot Phase II study of mazindol in children with attention deficit/hyperactivity disorder. Drug Des. Devel. Ther. 2014, 8, 2321–2332. [Google Scholar] [CrossRef] [Green Version]
- Wigal, S.B.; Wigal, T.; Hobart, M.; Madera, J.J.; Baker, R.A.; Kohegyi, E.; McKinney, A.; Wilens, T.E. Safety and Efficacy of Centanafadine Sustained-Release in Adults with Attention-Deficit Hyperactivity Disorder: Results of Phase 2 Studies. Neuropsychiatr. Dis. Treat. 2020, 16, 1411–1426. [Google Scholar] [CrossRef]
- DeLorenzo, C.; Lichenstein, S.; Schaefer, K.; Dunn, J.; Marshall, R.; Organisak, L.; Kharidia, J.; Robertson, B.; Mann, J.J.; Parsey, R.V. SEP-225289 serotonin and dopamine transporter occupancy: A PET study. J. Nucl. Med. 2011, 52, 1150–1155. [Google Scholar] [CrossRef] [Green Version]
- Hannestad, J.; Gallezot, J.D.; Planeta-Wilson, B.; Lin, S.F.; Williams, W.A.; van Dyck, C.H.; Malison, R.T.; Carson, R.E.; Ding, Y.S. Clinically relevant doses of methylphenidate significantly occupy norepinephrine transporters in humans in vivo. Biol. Psychiatry 2010, 68, 854–860. [Google Scholar] [CrossRef] [Green Version]
- Findling, R.L.; Adler, L.A.; Spencer, T.J.; Goldman, R.; Hopkins, S.C.; Koblan, K.S.; Kent, J.; Hsu, J.; Loebel, A. Dasotraline in Children with Attention-Deficit/Hyperactivity Disorder: A Six-Week, Placebo-Controlled, Fixed-Dose Trial. J. Child Adolesc. Psychopharmacol. 2019, 29, 80–89. [Google Scholar] [CrossRef]
- Koblan, K.S.; Hopkins, S.C.; Sarma, K.; Jin, F.; Goldman, R.; Kollins, S.H.; Loebel, A. Dasotraline for the Treatment of Attention-Deficit/Hyperactivity Disorder: A Randomized, Double-Blind, Placebo-Controlled, Proof-of-Concept Trial in Adults. Neuropsychopharmacology 2015, 40, 2745–2752. [Google Scholar] [CrossRef] [Green Version]
- Wigal, S.B.; Hopkins, S.C.; Koblan, K.S.; Childress, A.; Kent, J.M.; Tsai, J.; Hsu, J.; Loebel, A.; Goldman, R. Efficacy and Safety of Dasotraline in Children with ADHD: A Laboratory Classroom Study. J. Atten. Disord. 2020, 24, 192–204. [Google Scholar] [CrossRef]
- Bang-Andersen, B.; Ruhland, T.; Jorgensen, M.; Smith, G.; Frederiksen, K.; Jensen, K.G.; Zhong, H.; Nielsen, S.M.; Hogg, S.; Mork, A.; et al. Discovery of 1-[2-(2,4-dimethylphenylsulfanyl)phenyl]piperazine (Lu AA21004): A novel multimodal compound for the treatment of major depressive disorder. J. Med. Chem. 2011, 54, 3206–3221. [Google Scholar] [CrossRef]
- Mork, A.; Pehrson, A.; Brennum, L.T.; Nielsen, S.M.; Zhong, H.; Lassen, A.B.; Miller, S.; Westrich, L.; Boyle, N.J.; Sanchez, C.; et al. Pharmacological effects of Lu AA21004: A novel multimodal compound for the treatment of major depressive disorder. J. Pharmacol. Exp. Ther. 2012, 340, 666–675. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, C.; Asin, K.E.; Artigas, F. Vortioxetine, a novel antidepressant with multimodal activity: Review of preclinical and clinical data. Pharmacol. Ther. 2015, 145, 43–57. [Google Scholar] [CrossRef]
- Bortoletto, R.; Puttini, R.; Zoccante, L.; Colizzi, M. Vortioxetine add-on to methylphenidate for the treatment of symptoms of sickness behavior in attention-deficit hyperactivity disorder: Report of two cases. Reports 2021, 4, 30. [Google Scholar] [CrossRef]
- Biederman, J.; Lindsten, A.; Sluth, L.B.; Petersen, M.L.; Ettrup, A.; Eriksen, H.F.; Fava, M. Vortioxetine for attention deficit hyperactivity disorder in adults: A randomized, double-blind, placebo-controlled, proof-of-concept study. J. Psychopharmacol. 2019, 33, 511–521. [Google Scholar] [CrossRef]
- Goldstein, D.S. L-Dihydroxyphenylserine (L-DOPS): A norepinephrine prodrug. Cardiovasc Drug Rev. 2006, 24, 189–203. [Google Scholar] [CrossRef]
- Keating, G.M. Droxidopa: A review of its use in symptomatic neurogenic orthostatic hypotension. Drugs 2015, 75, 197–206. [Google Scholar] [CrossRef]
- Adler, L.A.; Gorny, S.W. Pilot Study of Droxidopa with Carbidopa in Adults with ADHD. J. Atten. Disord. 2019, 23, 189–198. [Google Scholar] [CrossRef]
- Zhou, R.; Han, X.; Wang, J.; Sun, J. Baicalin may have a therapeutic effect in attention deficit hyperactivity disorder. Med. Hypotheses 2015, 85, 761–764. [Google Scholar] [CrossRef]
- Gao, L.; Li, C.; Yang, R.Y.; Lian, W.W.; Fang, J.S.; Pang, X.C.; Qin, X.M.; Liu, A.L.; Du, G.H. Ameliorative effects of baicalein in MPTP-induced mouse model of Parkinson’s disease: A microarray study. Pharmacol. Biochem. Behav. 2015, 133, 155–163. [Google Scholar] [CrossRef]
- Hung, K.C.; Huang, H.J.; Wang, Y.T.; Lin, A.M. Baicalein attenuates alpha-synuclein aggregation, inflammasome activation and autophagy in the MPP(+)-treated nigrostriatal dopaminergic system in vivo. J. Ethnopharmacol. 2016, 194, 522–529. [Google Scholar] [CrossRef]
- Zhou, R.; Wang, J.; Han, X.; Ma, B.; Yuan, H.; Song, Y. Baicalin regulates the dopamine system to control the core symptoms of ADHD. Mol. Brain 2019, 12, 11. [Google Scholar] [CrossRef] [Green Version]
- Boutzoukas, E.M.; Crutcher, J.; Somoza, E.; Sepeta, L.N.; You, X.; Gaillard, W.D.; Wallace, G.L.; Berl, M.M. Cortical thickness in childhood left focal epilepsy: Thinning beyond the seizure focus. Epilepsy Behav. 2020, 102, 106825. [Google Scholar] [CrossRef]
- Genc, E.; Fraenz, C.; Schluter, C.; Friedrich, P.; Hossiep, R.; Voelkle, M.C.; Ling, J.M.; Gunturkun, O.; Jung, R.E. Diffusion markers of dendritic density and arborization in gray matter predict differences in intelligence. Nat. Commun. 2018, 9, 1905. [Google Scholar] [CrossRef] [Green Version]
- Shaw, P.; Lerch, J.; Greenstein, D.; Sharp, W.; Clasen, L.; Evans, A.; Giedd, J.; Castellanos, F.X.; Rapoport, J. Longitudinal mapping of cortical thickness and clinical outcome in children and adolescents with attention-deficit/hyperactivity disorder. Arch. Gen. Psychiatry 2006, 63, 540–549. [Google Scholar] [CrossRef] [Green Version]
- Varenhorst, C.; James, S.; Erlinge, D.; Brandt, J.T.; Braun, O.O.; Man, M.; Siegbahn, A.; Walker, J.; Wallentin, L.; Winters, K.J.; et al. Genetic variation of CYP2C19 affects both pharmacokinetic and pharmacodynamic responses to clopidogrel but not prasugrel in aspirin-treated patients with coronary artery disease. Eur. Heart J. 2009, 30, 1744–1752. [Google Scholar] [CrossRef] [Green Version]
- Harowitz, J.; Crandall, L.; McGuone, D.; Devinsky, O. Seizure-related deaths in children: The expanding spectrum. Epilepsia 2021, 62, 570–582. [Google Scholar] [CrossRef]

| Inattentive Symptoms | Hyperactivity/Impulsivity Symptoms |
|---|---|
| Pays no attention to details and makes reckless actions | ❖ Excessive fidgets. |
| Inability to maintain attention in school, exercise, and work | Failure to remain in the seat when required. |
| When addressed, he does not appear to listen. | Frequently runs around or climbs in inappropriate settings. |
| Inability to follow directions, failure to complete work | Often unable to quietly participate in play when needed. |
| Demonstrate a significant level of disorganization during the execution of tasks and activities | Always “on the move” and appears “powered by a motor.” |
| Tendency to avoid tasks that require attention, such as reading long papers. | Talks excessively. |
| Items required for tasks and activities are misplaced. | Answers impatiently before the inquiry is finished. |
| Extraneous stimuli such as irrelevant ideas cause distraction. | Frequently unable to await their turn. |
| Inattention to regular tasks such as paying bills and making appointments | Frequently interrupts or interferes with others |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, H.-C.; Chiang, K.-L.; Chang, K.-H.; Chen, C.-M.; Tsai, J.-D. Epilepsy and Attention Deficit Hyperactivity Disorder: Connection, Chance, and Challenges. Int. J. Mol. Sci. 2023, 24, 5270. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065270
Fan H-C, Chiang K-L, Chang K-H, Chen C-M, Tsai J-D. Epilepsy and Attention Deficit Hyperactivity Disorder: Connection, Chance, and Challenges. International Journal of Molecular Sciences. 2023; 24(6):5270. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065270
Chicago/Turabian StyleFan, Hueng-Chuen, Kuo-Liang Chiang, Kuang-Hsi Chang, Chuan-Mu Chen, and Jeng-Dau Tsai. 2023. "Epilepsy and Attention Deficit Hyperactivity Disorder: Connection, Chance, and Challenges" International Journal of Molecular Sciences 24, no. 6: 5270. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065270