
Three-Dimensional Digital Superimposition of Orthodontic Bracket Position by Using a Computer-Aided Transfer Jig System: An Accuracy Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Procedure
2.2.1. Fabrication of Transfer Jigs
2.2.2. Indirect Bonding Procedures
2.3. Measurements
2.3.1. Linear Measurements
- Mesiodistal direction (M-D): a linear measurement (mm) of a discrepancy along the x-axis. The discrepancy in the mesial direction was recorded as a positive value, and the discrepancy in the distal direction was recorded as a negative value.
- Buccolingual direction (B-L): a linear measurement (mm) of a discrepancy along the y-axis. The discrepancy in the buccal direction was recorded as a positive value, and the discrepancy in the lingual direction was recorded as a negative value.
- Occlusogingival direction (O-G): a linear measurement (mm) of a discrepancy along the z-axis. The discrepancy in the occlusal direction was recorded as a positive value, and the discrepancy in the apical direction was recorded as a negative value.
2.3.2. Angular Measurements
- Torque (T): an angular measurement (°) of a discrepancy between the y-axis on the virtual model and the y-axis on the actual model, projected to the y–z plane of the virtual model. The torque discrepancy in the crown lingual direction was recorded as a positive value, and the torque discrepancy in the crown labial/buccal direction was recorded as a negative value.
- Angulation (A): an angular measurement (°) of a discrepancy between the x-axis on the virtual model and the x-axis on the actual model, projected to the x–z plane of the virtual model. The angulation discrepancy in the crown distal direction was recorded as a positive value, and the angulation discrepancy in the crown mesial direction was recorded as a negative value.
- Rotation (R): an angular measurement (°) of a discrepancy between the y-axis on the virtual model and the y-axis on the actual model, projected to the x–y plane of the virtual model. The rotation discrepancy in the distobuccal direction was recorded as a positive value, and the rotation discrepancy in the mesiobuccal direction was recorded as a negative value.
2.4. Statistical Analysis
3. Results
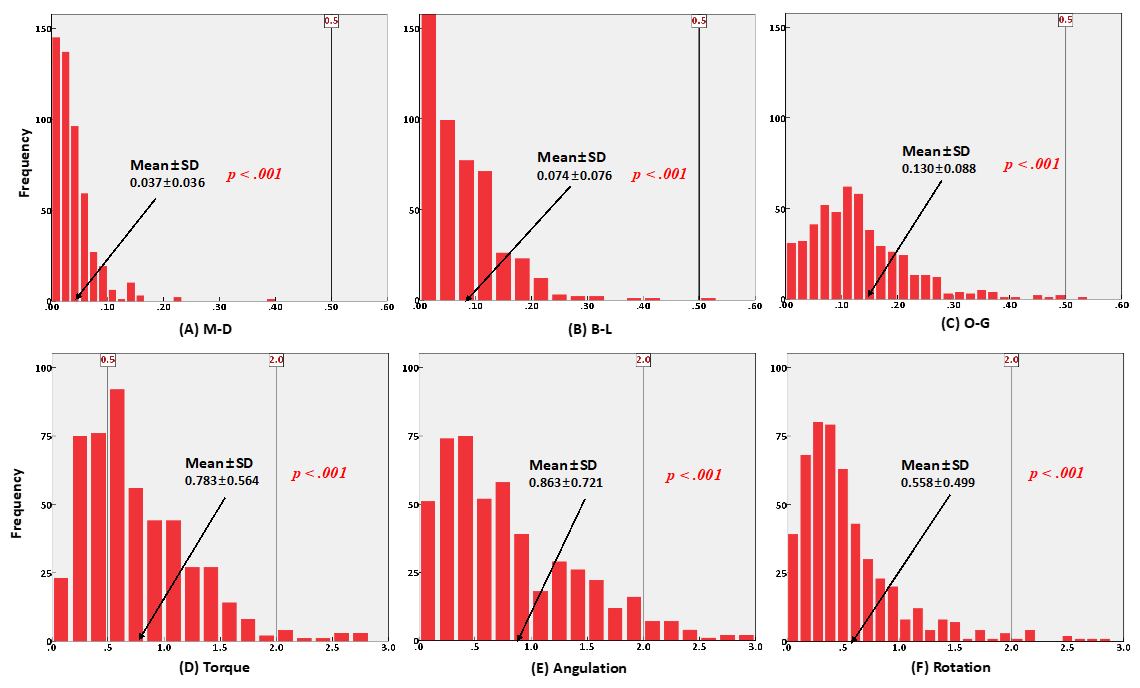
3.1. Overall Differences in Bracket Position
3.2. Differences in Bracket Position According to Tooth Type
3.3. Differences in Bracket Position According to the Presence/Absence of Resin Base
3.4. Interactions between Tooth Type and Resin Base
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Creekmore, T.D.; Kunik, R.L. Straight wire: The next generation. Am. J. Orthod. Dentofac. Orthop. 1993, 104, 8–20. [Google Scholar] [CrossRef]
- Andrews, L.F. The straight-wire appliance. Explained and compared. J. Clin. Orthod. 1976, 10, 174–195. [Google Scholar]
- Andrews, L.F. The straight-wire appliance. Br. J. Orthod. 1979, 6, 125–143. [Google Scholar] [CrossRef] [PubMed]
- Nawrocka, A.; Lukomska-Szymanska, M. The Indirect Bonding Technique in Orthodontics—A Narrative Literature Review. Materials 2020, 13, 986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deahl, S.T.; Salome, N.; Hatch, J.P.; Rugh, J.D. Practice-based comparison of direct and indirect bonding. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 738–742. [Google Scholar] [CrossRef]
- Zachrisson, B.U.; Brobakken, B.O. Clinical comparison of direct versus indirect bonding with different bracket types and adhesives. Am. J. Orthod. 1978, 74, 62–78. [Google Scholar] [CrossRef]
- Aguirre, M.J.; King, G.J.; Waldron, J.M. Assessment of bracket placement and bond strength when comparing direct bonding to indirect bonding techniques. Am. J. Orthod. 1982, 82, 269–276. [Google Scholar] [CrossRef]
- Koo, B.C.; Chung, C.H.; Vanarsdall, R.L. Comparison of the accuracy of bracket placement between direct and indirect bonding techniques. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 346–351. [Google Scholar] [CrossRef]
- Hodge, T.M.; Dhopatkar, A.A.; Rock, W.P.; Spary, D.J. A randomized clinical trial comparing the accuracy of direct versus indirect bracket placement. J. Orthod. 2004, 31, 132–137. [Google Scholar] [CrossRef]
- Shpack, N.; Geron, S.; Floris, I.; Davidovitch, M.; Brosh, T.; Vardimon, A.D. Bracket placement in lingual vs. labial systems and direct vs. indirect bonding. Angle Orthod. 2007, 77, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Bozelli, J.V.; Bigliazzi, R.; Barbosa, H.A.; Ortolani, C.L.; Bertoz, F.A.; Faltin, K., Jr. Comparative study on direct and indirect bracket bonding techniques regarding time length and bracket detachment. Dent. Press J. Orthod. 2013, 18, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Silverman, E.; Cohen, M.; Gianelly, A.A.; Dietz, V.S. A universal direct bonding system for both metal and plastic brackets. Am. J. Orthod. 1972, 62, 236–244. [Google Scholar] [CrossRef]
- Kalange, J.T. Indirect bonding: A comprehensive review of the advantages. World J. Orthod. 2004, 5, 301–307. [Google Scholar]
- Thomas, R.G. Indirect bonding: Simplicity in action. J. Clin. Orthod. 1979, 13, 93–106. [Google Scholar]
- Layman, B. Digital Bracket Placement for Indirect Bonding. J. Clin. Orthod. 2019, 53, 387–396. [Google Scholar]
- Möhlhenrich, S.C.; Alexandridis, C.; Peters, F.; Kniha, K.; Modabber, A.; Danesh, G.; Fritz, U. Three-dimensional evaluation of bracket placement accuracy and excess bonding adhesive depending on indirect bonding technique and bracket geometry: An in-vitro study. Head Face Med. 2020, 16, 17. [Google Scholar] [CrossRef]
- Castilla, A.E.; Crowe, J.J.; Moses, J.R.; Wang, M.; Ferracane, J.L.; Covell, D.A., Jr. Measurement and comparison of bracket transfer accuracy of five indirect bonding techniques. Angle Orthod. 2014, 84, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Seo, H. Accuracy of Indirect Bracket Bonding Via Virtual Setup and 3D Printing. Master’s Thesis, Yonsei University, Seoul, Korea, 2016. [Google Scholar]
- Pottier, T.; Brient, A.; Turpin, Y.L.; Chauvel, B.; Meuric, V.; Sorel, O.; Brezulier, D. Accuracy evaluation of bracket repositioning by indirect bonding: Hard acrylic CAD/CAM versus soft one-layer silicone trays, an in vitro study. Clin. Oral Investig. 2020, 24, 3889–3897. [Google Scholar] [CrossRef]
- Xue, C.; Xu, H.; Guo, Y.; Xu, L.; Dhami, Y.; Wang, H.; Liu, Z.; Ma, J.; Bai, D. Accurate bracket placement using a computer-aided design and computer-aided manufacturing-guided bonding device: An in vivo study. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 269–277. [Google Scholar] [CrossRef] [Green Version]
- Fillion, D. Clinical advantages of the Orapix-straight wire lingual technique. Int. Orthod. 2010, 8, 125–151. [Google Scholar] [CrossRef]
- Fillion, D. Lingual straightwire treatment with the Orapix system. J. Clin. Orthod. 2011, 45, 488–497. [Google Scholar]
- Klocke, A.; Tadic, D.; Vaziri, F.; Kahl-Nieke, B. Custom base preaging in indirect bonding. Angle Orthod. 2004, 74, 106–111. [Google Scholar] [CrossRef]
- Muguruma, T.; Yasuda, Y.; Iijima, M.; Kohda, N.; Mizoguchi, I. Force and amount of resin composite paste used in direct and indirect bonding. Angle Orthod. 2010, 80, 1089–1094. [Google Scholar] [CrossRef]
- Park, J.H.; Choi, J.Y.; Kim, S.H.; Kim, S.J.; Lee, K.J.; Nelson, G. Three-dimensional evaluation of the transfer accuracy of a bracket jig fabricated using computer-aided design and manufacturing to the anterior dentition: An in vitro study. Korean J. Orthod. 2021, in press. [Google Scholar]
- Park, K.H.; Choi, J.Y.; Kim, K.A.; Kim, S.J.; Chung, K.R.; Kim, S.H. Critical issues concerning biocreative strategy in contemporary temporary skeletal anchorage device orthodontics: A narrative review. Orthod. Craniofac. Res. 2021, 24 (Suppl. S1), 39–47. [Google Scholar] [CrossRef]
- Ludwig, B.; Alexander, J.C.; Cacciafesta, V.; Fillion, D.; Gilbert, A.; Moles, R.C.; Paz, M.E.; Silli, S.M.; Takemoto, K. JCO roundtable. Lingual orthodontics. Part 1. J. Clin. Orthod. 2012, 46, 203–217. [Google Scholar]
- Spanou, A.; Koletsi, D.; Fleming, P.S.; Polychronopoulou, A.; Pandis, N. Statistical analysis in orthodontic journals: Are we ignoring confounding? Eur. J. Orthod. 2016, 38, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goracci, C.; Özcan, M.; Franchi, L.; Di Bello, G.; Louca, C.; Vichi, A. Bracket bonding to polymethylmethacrylate-based materials for computer-aided design/manufacture of temporary restorations: Influence of mechanical treatment and chemical treatment with universal adhesives. Korean J. Orthod. 2019, 49, 404–412. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.Y.; Ha, S.W.; Cho, I.S.; Yang, I.H.; Baek, S.H. In-vitro investigation of the mechanical friction properties of a computer-aided design and computer-aided manufacturing lingual bracket system under diverse tooth displacement condition. Korean J. Orthod. 2019, 49, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Czolgosz, I.; Cattaneo, P.M.; Cornelis, M.A. Computer-aided indirect bonding versus traditional direct bonding of orthodontic brackets: Bonding time, immediate bonding failures, and cost-minimization. A randomized controlled trial. Eur. J. Orthod. 2021, 43, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Schmid, J.; Brenner, D.; Recheis, W.; Hofer-Picout, P.; Brenner, M.; Crismani, A.G. Transfer accuracy of two indirect bonding techniques—An in vitro study with 3D scanned models. Eur. J. Orthod. 2018, 40, 549–555. [Google Scholar] [CrossRef]
- Duarte, M.E.A.; Gribel, B.F.; Spitz, A.; Artese, F.; Miguel, J.A.M. Reproducibility of digital indirect bonding technique using three-dimensional (3D) models and 3D-printed transfer trays. Angle Orthod. 2020, 90, 92–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackers, N.; Maes, N.; Lambert, F.; Albert, A.; Charavet, C. Standard vs computer-aided design/computer-aided manufacturing customized self-ligating systems using indirect bonding with both. Angle Orthod. 2021, 91, 74–80. [Google Scholar] [CrossRef]
- Niu, Y.; Zeng, Y.; Zhang, Z.; Xu, W.; Xiao, L. Comparison of the transfer accuracy of two digital indirect bonding trays for labial bracket bonding. Angle Orthod. 2021, 91, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Wan Hassan, W.N.; Yusoff, Y.; Mardi, N.A. Comparison of reconstructed rapid prototyping models produced by 3-dimensional printing and conventional stone models with different degrees of crowding. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazeveld, A.; Huddleston Slater, J.J.; Ren, Y. Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 108–115. [Google Scholar] [CrossRef]
- Gyllenhaal, K.A. Accuracy of Two Indirect Bonding Transfer Methods—A Three-Dimensional, In-Vivo Analysis. Master’s Thesis, University of Minnesota, Minneapolis, MN, USA, 2015. [Google Scholar]
- Koch, P.J. Measuring the accuracy of a computer-aided design and computer-aided manufacturing-based indirect bonding tray. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 315. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Tooth Type (n) | Mesiodistal (mm) | Buccolingual (mm) | Occlusogingival (mm) | Torque (°) | Angulation (°) | Rotation (°) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p | Mean ± SD | p | Mean ± SD | p | Mean ± SD | p | Mean ± SD | p | Mean ± SD | p | ||
| A | 1 (226) | 0.050 ±0.042 | <0.001 †† | 0.097 ±0.081 | <0.001 †† | 0.142 ±0.099 | <0.001 †† | 0.982 ±0.708 | <0.001 †† | 1.169 ±0.824 | <0.001 †† | 0.692 ±0.616 | <0.001 †† |
| 2 (122) | 0.022 ±0.026 | <0.001 †† | 0.053 ±0.070 | <0.001 †† | 0.100 ±0.055 | <0.001 †† | 0.551 ±0.299 | <0.001 †† | 0.545 ±0.442 | <0.001 †† | 0.467 ±0.396 | <0.001 †† | |
| 3 (158) | 0.030 ±0.027 | <0.001 †† | 0.057 ±0.062 | <0.001 †† | 0.131 ±0.084 | <0.001 †† | 0.679 ±0.358 | <0.001 †† | 0.671 ±0.545 | <0.001 †† | 0.435 ±0.300 | <0.001 †† | |
| B | 1 (226) | 0.039 ±0.033 | <0.001 †† | 0.081 ±0.057 | <0.001 †† | 0.203 ±0.139 | <0.001 †† | 0.895 ±0.527 | <0.001 †† | 1.035 ±0.576 | <0.001 †† | 0.676 ±0.485 | <0.001 †† |
| 2 (122) | 0.034 ±0.030 | <0.001 †† | 0.060 ±0.071 | <0.001 †† | 0.092 ±0.085 | <0.001 †† | 0.598 ±0.414 | <0.001 †† | 0.639 ±0.488 | <0.001 †† | 0.459 ±0.342 | <0.001 †† | |
| 3 (158) | 0.065 ±0.080 | <0.001 †† | 0.097 ±0.054 | <0.001 †† | 0.111 ±0.103 | <0.001 †† | 0.726 ±0.436 | <0.001 †† | 0.633 ±0.531 | <0.001 †† | 0.447 ±0.344 | <0.001 †† | |
| Group | Tooth Type (n) | Mesiodistal (mm) | Buccolingual (mm) | Occlusogingival (mm) | Torque (°) | Angulation (°) | Rotation (°) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mesial | Distal | Buccal | Lingual | Occlusal | Gingival | BCT | LCT | MRT | DRT | m-b | m-l | ||
| A | 1 (226) | 188 | 38 | 119 | 107 | 208 | 18 | 141 | 85 | 104 | 122 | 107 | 119 |
| 2 (122) | 62 | 60 | 61 | 61 | 107 | 15 | 70 | 52 | 62 | 60 | 63 | 59 | |
| 3 (158) | 71 | 87 | 82 | 76 | 145 | 13 | 108 | 50 | 66 | 91 | 83 | 75 | |
| B | 1 (226) | 140 | 86 | 130 | 96 | 214 | 12 | 151 | 75 | 96 | 130 | 121 | 105 |
| 2 (122) | 81 | 41 | 62 | 60 | 105 | 17 | 84 | 38 | 72 | 50 | 54 | 68 | |
| 3 (158) | 86 | 72 | 88 | 70 | 140 | 18 | 87 | 71 | 75 | 83 | 73 | 85 | |
| Group | Mesiodistal (mm) | Buccolingual (mm) | Occlusogingival (mm) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (226) | 2 (122) | 3 (158) | p | 1 (226) | 2 (122) | 3 (158) | p | 1 (226) | 2 (122) | 3 (158) | p | |
| A | 0.050 ±0.042 | 0.022 ±0.026 | 0.030 ±0.027 | <0.001 †† | 0.097 ±0.081 | 0.053 ±0.070 | 0.057 ±0.062 | <0.001 †† | 0.142 ±0.099 | 0.100 ±0.055 | 0.131 ±0.084 | <0.001 †† |
| B | 0.039 ±0.033 | 0.034 ±0.030 | 0.065 ±0.080 | <0.001 †† | 0.081 ±0.057 | 0.060 ±0.071 | 0.067 ±0.054 | 0.004 † | 0.203 ±0.139 | 0.092 ±0.085 | 0.111 ±0.103 | <0.001 †† |
| Group | Torque (°) | Angulation (°) | Rotation (°) | |||||||||
| 1 (226) | 2 (122) | 3 (158) | p | 1 (226) | 2 (122) | 3 (158) | p | 1 (226) | 2 (122) | 3 (158) | p | |
| A | 0.982 ±0.708 | 0.551 ±0.299 | 0.679 ±0.358 | <0.001 †† | 1.169 ±0.824 | 0.545 ±0.442 | 0.671 ±0.545 | <0.001 †† | 0.692 ±0.616 | 0.467 ±0.396 | 0.435 ±0.300 | <0.001 †† |
| B | 0.895 ±0.527 | 0.598 ±0.414 | 0.726 ±0.436 | <0.001 †† | 1.035 ±0.576 | 0.639 ±0.488 | 0.633 ±0.531 | <0.001 †† | 0.676 ±0.485 | 0.459 ±0.342 | 0.447 ±0.344 | <0.001 †† |
| Tooth Type (n) | Mesiodistal (mm) | Buccolingual (mm) | Occlusogingival (mm) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean Difference | SD | p | Mean Difference | SD | p | Mean Difference | SD | p | ||
| 1 (226) | 2 (122) | 0.028 | 0.003 | <0.001 †† | 0.043 | 0.008 | <0.001 †† | 0.042 | 0.009 | <0.001 †† |
| 3 (158) | 0.019 | 0.003 | <0.001 †† | 0.040 | 0.007 | <0.001 †† | 0.011 | 0.008 | 0.611 | |
| 2 (122) | 3 (158) | −0.008 | 0.004 | 0.107 | −0.003 | 0.008 | >0.999 | −0.031 | 0.010 | 0.008 † |
| Tooth Type (n) | Torque (°) | Angulation (°) | Rotation (°) | |||||||
| Mean Difference | SD | p | Mean Difference | SD | p | Mean Difference | SD | p | ||
| 1 (226) | 2 (122) | 0.430 | 0.060 | <0.001 †† | 0.624 | 0.074 | <0.001 †† | 0.224 | 0.054 | <0.001 †† |
| 3 (158) | 0.302 | 0.055 | <0.001 †† | 0.497 | 0.069 | <0.001 †† | 0.257 | 0.050 | <0.001 †† | |
| 2 (122) | 3 (158) | −0.127 | 0.064 | 0.146 | −0.121 | 0.080 | 0.351 | 0.032 | 0.058 | >0.999 |
| Tooth Type (n) | Mesiodistal (mm) | Buccolingual (mm) | Occlusogingival (mm) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean Difference | SD | p | Mean Difference | SD | p | Mean Difference | SD | p | ||
| 1 (226) | 2 (122) | 0.005 | 0.058 | >0.999 | 0.021 | 0.006 | 0.006 † | 0.111 | 0.013 | <0.001 †† |
| 3 (158) | −0.025 | 0.005 | <0.001 †† | 0.014 | 0.006 | 0.076 | 0.092 | 0.012 | <0.001 †† | |
| 2 (122) | 3 (158) | −0.031 | 0.006 | <0.001 †† | −0.007 | 0.007 | >0.999 | −0.018 | 0.014 | 0.566 |
| Tooth Type (n) | Torque (°) | Angulation (°) | Rotation (°) | |||||||
| Mean Difference | SD | p | Mean Difference | SD | p | Mean Difference | SD | p | ||
| 1 (226) | 2 (122) | 0.296 | 0.053 | <0.001 †† | 0.396 | 0.060 | <0.001 †† | 0.216 | 0.046 | <0.001 †† |
| 3 (158) | 0.168 | 0.049 | 0.002 † | 0.402 | 0.056 | <0.001 †† | 0.229 | 0.042 | <0.001 †† | |
| 2 (122) | 3 (158) | −0.127 | 0.057 | 0.077 | 0.005 | 0.065 | >0.999 | 0.012 | 0.049 | >0.999 |
| Tooth Type (n) | Mesiodistal (mm) | Buccolingual (mm) | Occlusogingival (mm) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| A | B | p | A | B | p | A | B | p | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||||
| 1 (226) | 0.050 ±0.042 | 0.039 ±0.033 | 0.003 † | 0.097 ±0.081 | 0.081 ±0.057 | 0.018 * | 0.142 ±0.099 | 0.203 ±0.139 | <0.001 †† |
| 2 (122) | 0.022 ±0.026 | 0.034 ±0.030 | 0.001 † | 0.053 ±0.070 | 0.060 ±0.071 | 0.459 | 0.100 ±0.055 | 0.092 ±0.085 | 0.390 |
| 3 (158) | 0.030 ±0.027 | 0.065 ±0.080 | <0.001 †† | 0.057 ±0.062 | 0.067 ±0.054 | 0.119 | 0.131 ±0.084 | 0.111 ±0.103 | 0.053 |
| Tooth Type (n) | Torque (°) | Angulation (°) | Rotation (°) | ||||||
| A | B | p | A | B | p | A | B | p | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||||
| 1 (226) | 0.982 ±0.708 | 0.895 ±0.527 | 0.141 | 1.169 ±0.824 | 1.035 ±0.576 | 0.046 * | 0.692 ±0.616 | 0.676 ±0.485 | 0.757 |
| 2 (122) | 0.551 ±0.299 | 0.598 ±0.414 | 0.311 | 0.545 ±0.442 | 0.639 ±0.488 | 0.117 | 0.467 ±0.396 | 0.459 ±0.342 | 0.863 |
| 3 (158) | 0.679 ±0.358 | 0.726 ±0.436 | 0.290 | 0.671 ±0.545 | 0.633 ±0.531 | 0.531 | 0.435 ±0.300 | 0.447 ±0.344 | 0.750 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-H.; Choi, J.-Y.; Oh, S.H.; Kim, S.-H. Three-Dimensional Digital Superimposition of Orthodontic Bracket Position by Using a Computer-Aided Transfer Jig System: An Accuracy Analysis. Sensors 2021, 21, 5911. https://0-doi-org.brum.beds.ac.uk/10.3390/s21175911
Park J-H, Choi J-Y, Oh SH, Kim S-H. Three-Dimensional Digital Superimposition of Orthodontic Bracket Position by Using a Computer-Aided Transfer Jig System: An Accuracy Analysis. Sensors. 2021; 21(17):5911. https://0-doi-org.brum.beds.ac.uk/10.3390/s21175911
Chicago/Turabian StylePark, Jae-Hyun, Jin-Young Choi, Song Hee Oh, and Seong-Hun Kim. 2021. "Three-Dimensional Digital Superimposition of Orthodontic Bracket Position by Using a Computer-Aided Transfer Jig System: An Accuracy Analysis" Sensors 21, no. 17: 5911. https://0-doi-org.brum.beds.ac.uk/10.3390/s21175911