
Seeking Inspiration: Examining the Validity and Reliability of a New Smartphone Respiratory Therapy Exergame App



Abstract
:1. Introduction
2. Inspiratory Air Flow and Sound Generation
2.1. Sound Detection and Modern Smartphones
2.2. Limited Respiratory Application Availability for Improving Health
2.3. Air Flows for Testing Respiratory Apps
3. Incentive Spirometry and Respiratory Therapy
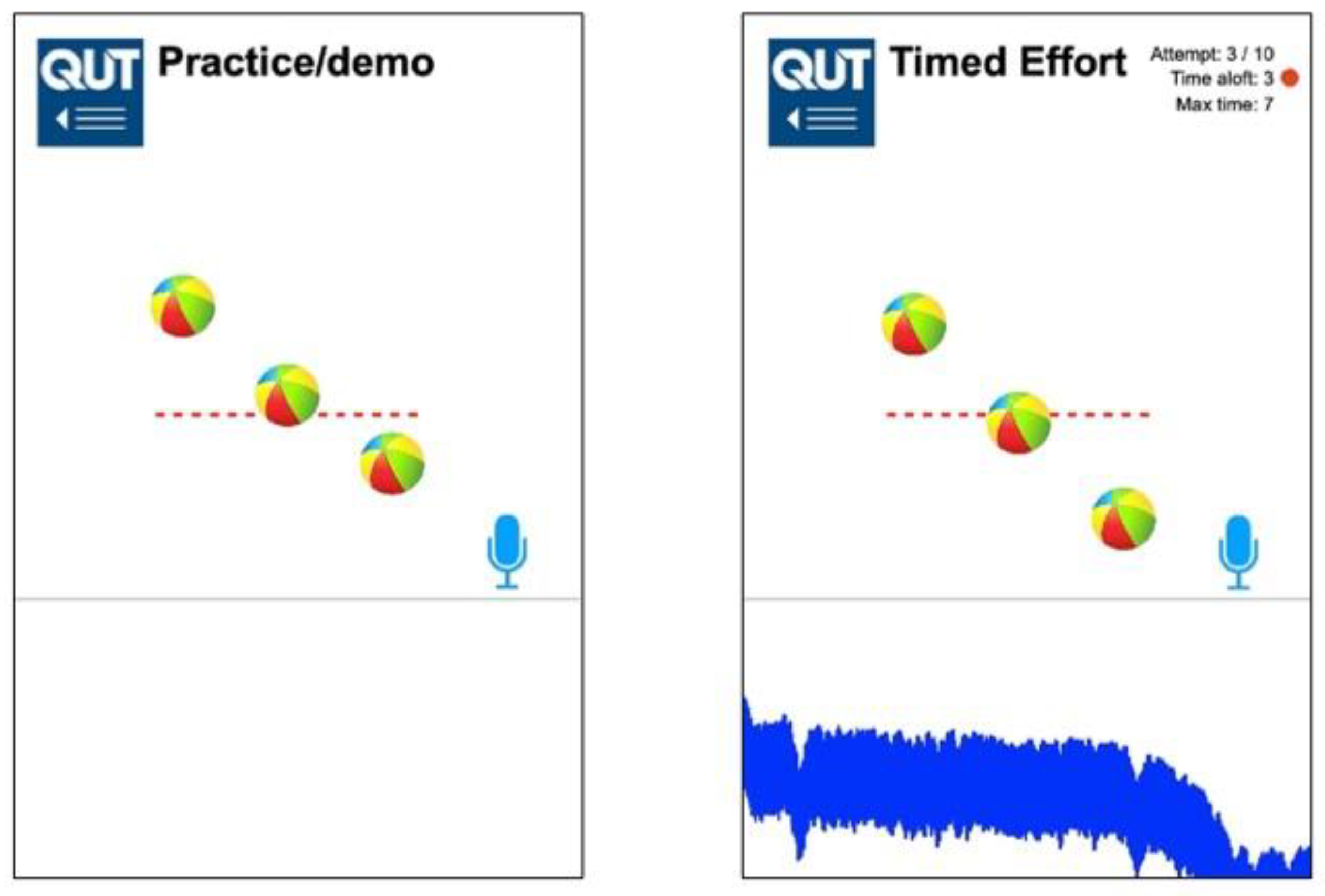
3.1. QUT Inspire—A Virtual Incentive Spirometer
3.2. Inspiratory Flow Rate (IFr)—Clinical Incentive Spirometer
3.3. Peak Inspiratory Flow Rate (PIFr)—Pneumotachograph
3.4. Sound Level of Syringe Inflows (dBA)—Digital Sound Meter
3.5. Acoustic Sampling for Smartphone Testing
3.6. QUT Inspire Smartphone Application Testing
3.7. Statistical Analysis
4. Results
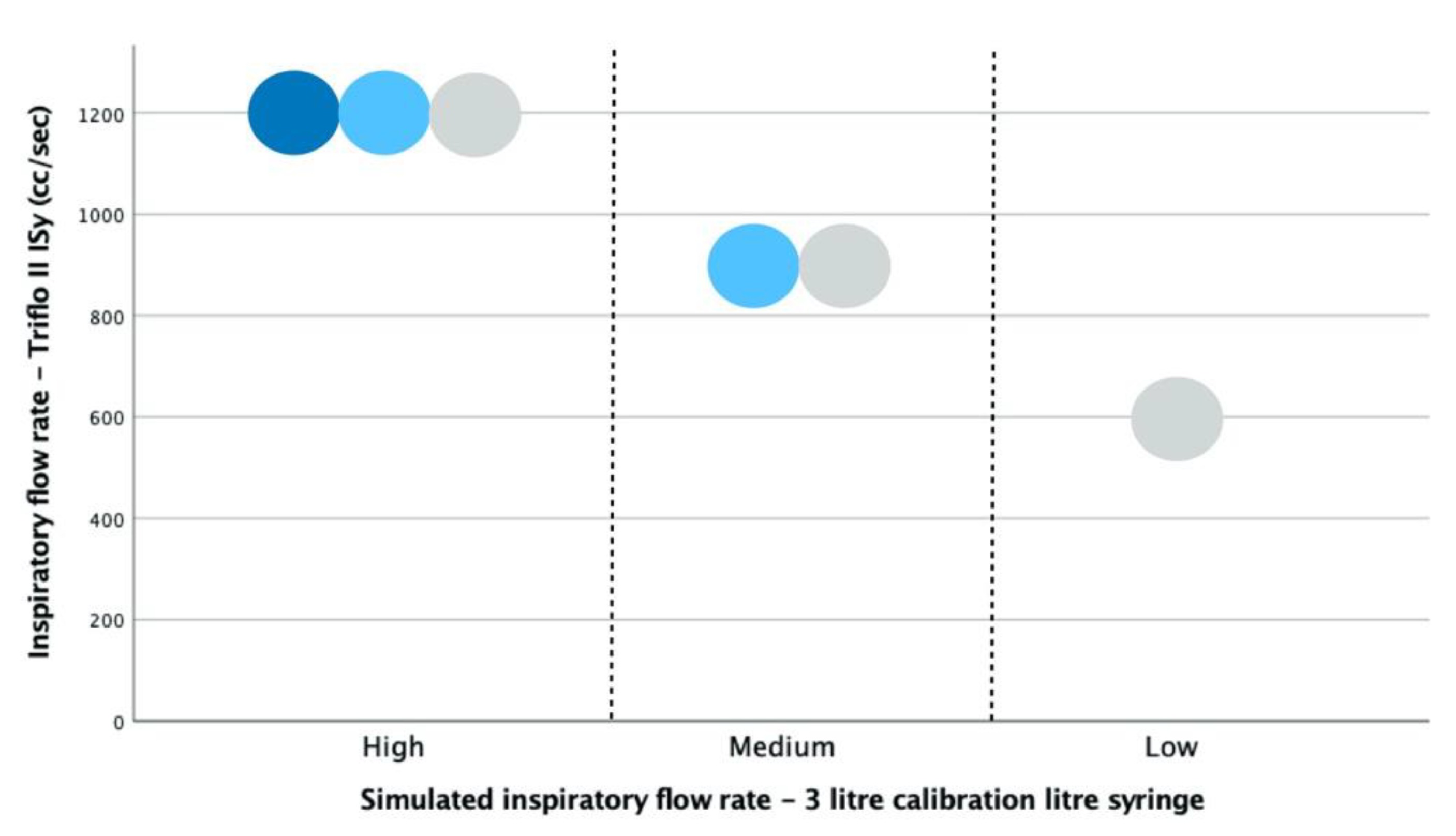
4.1. Syringe-Generated Inspirations by Flow Rate—Triflo II Clinical ISy Device
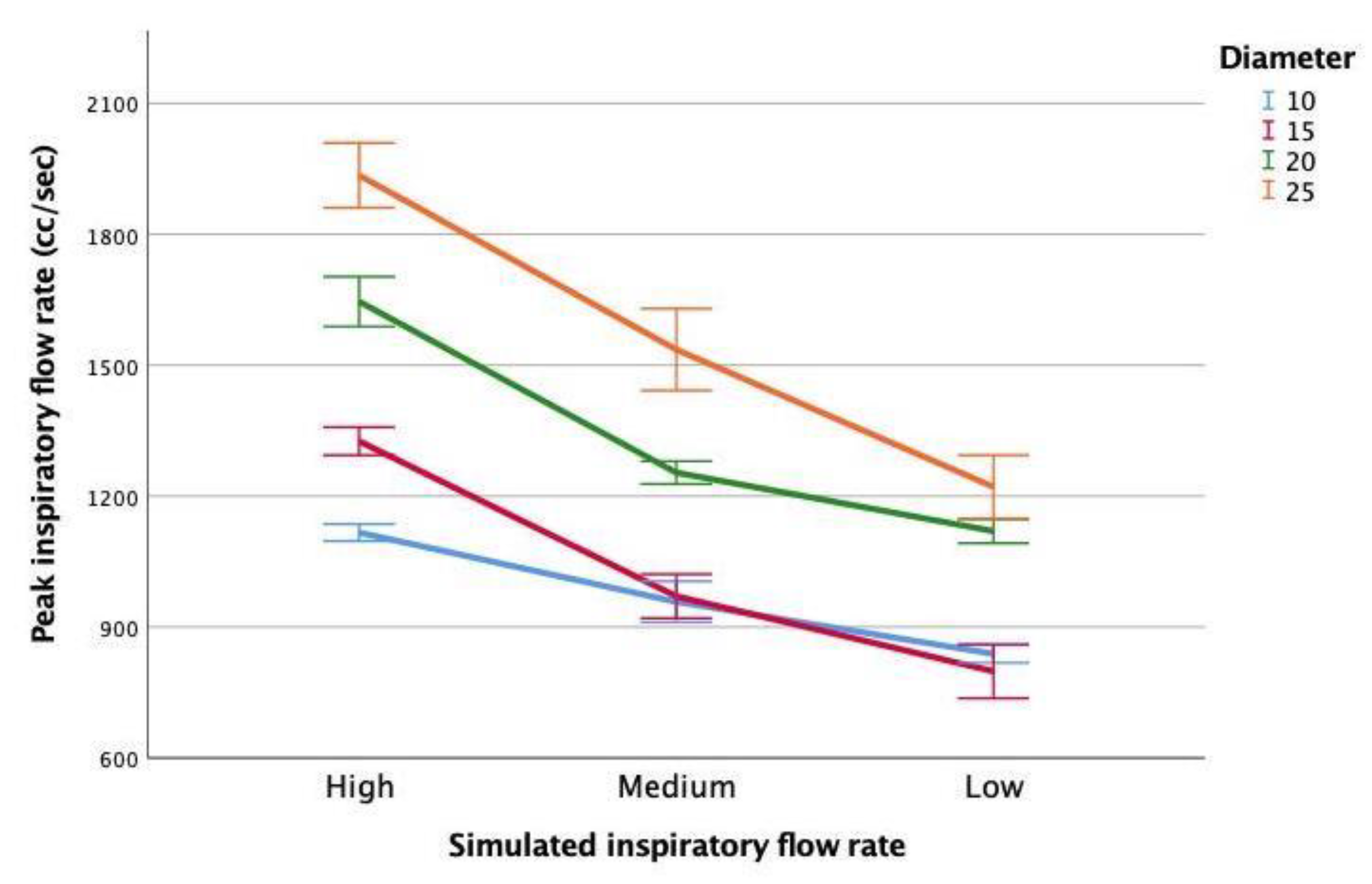
4.2. Peak Inspiratory Flow (PIFr) of Simulated Inspirations by Flow Rate and Mouth Diameter
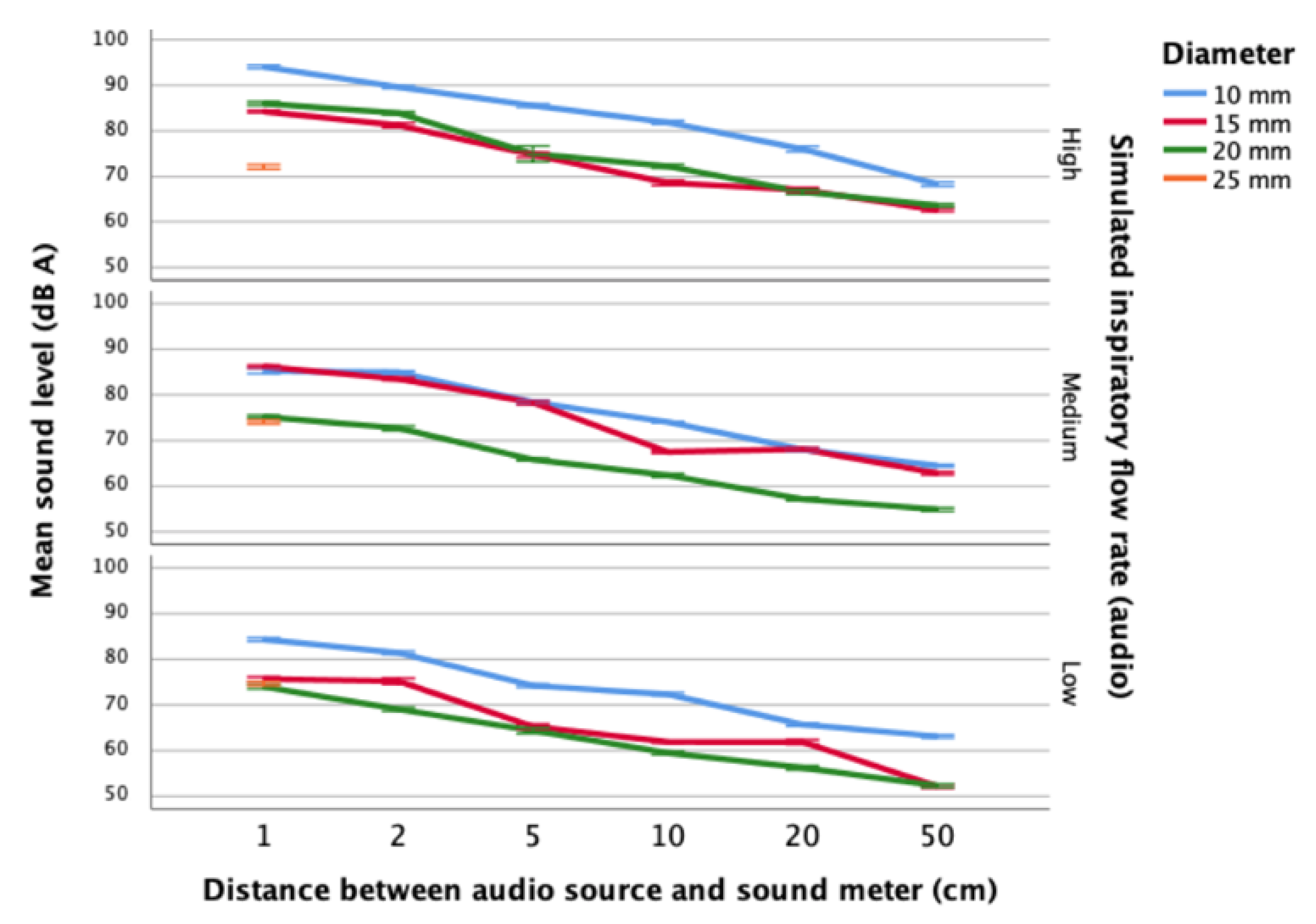
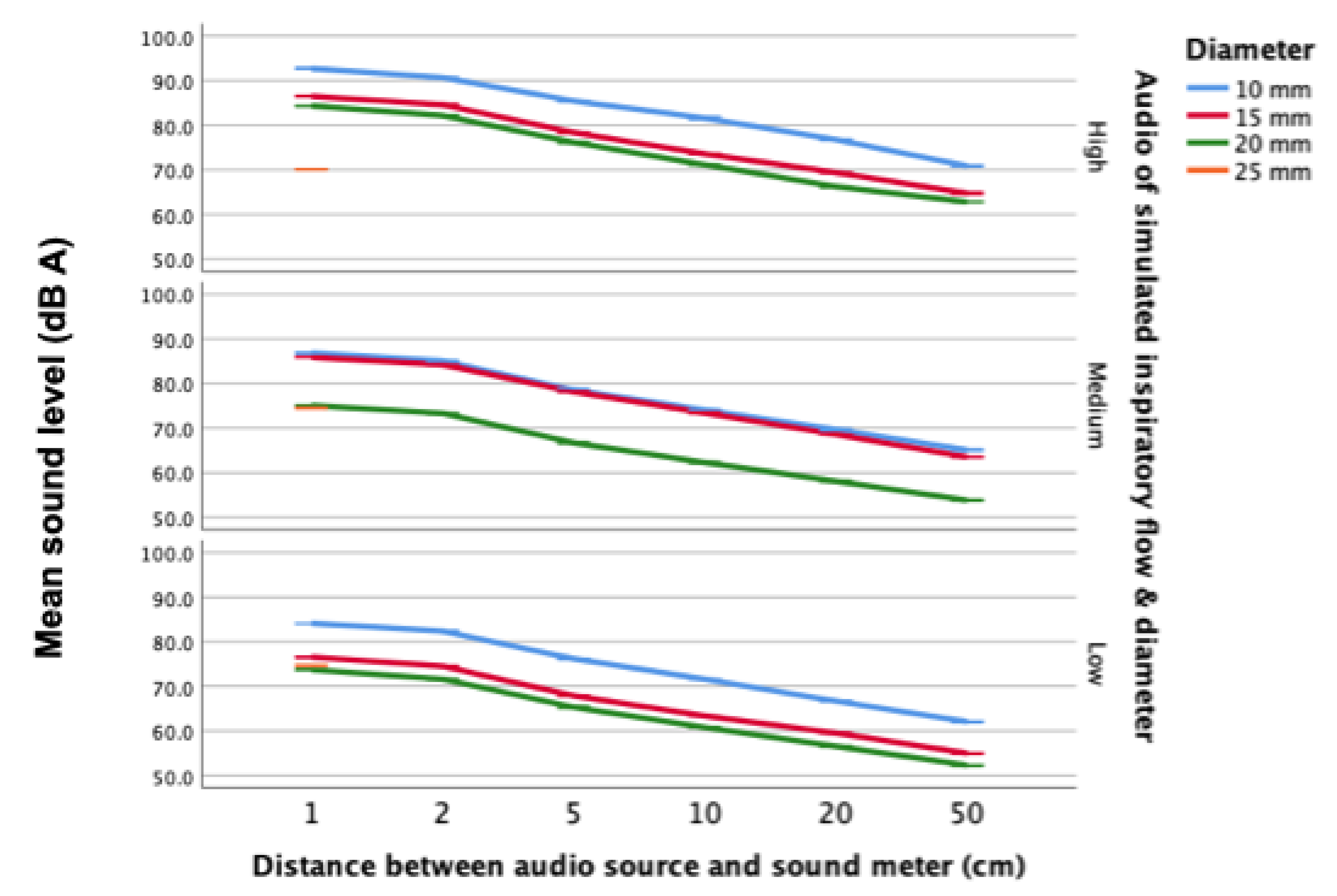
4.3. Sound Levels of Syringe-Simulated Inspirations by Distance, Flow Rate and Mouth Diameter
4.4. Sounds Level of Audio Samples of Syringe-Simulated Inspirations
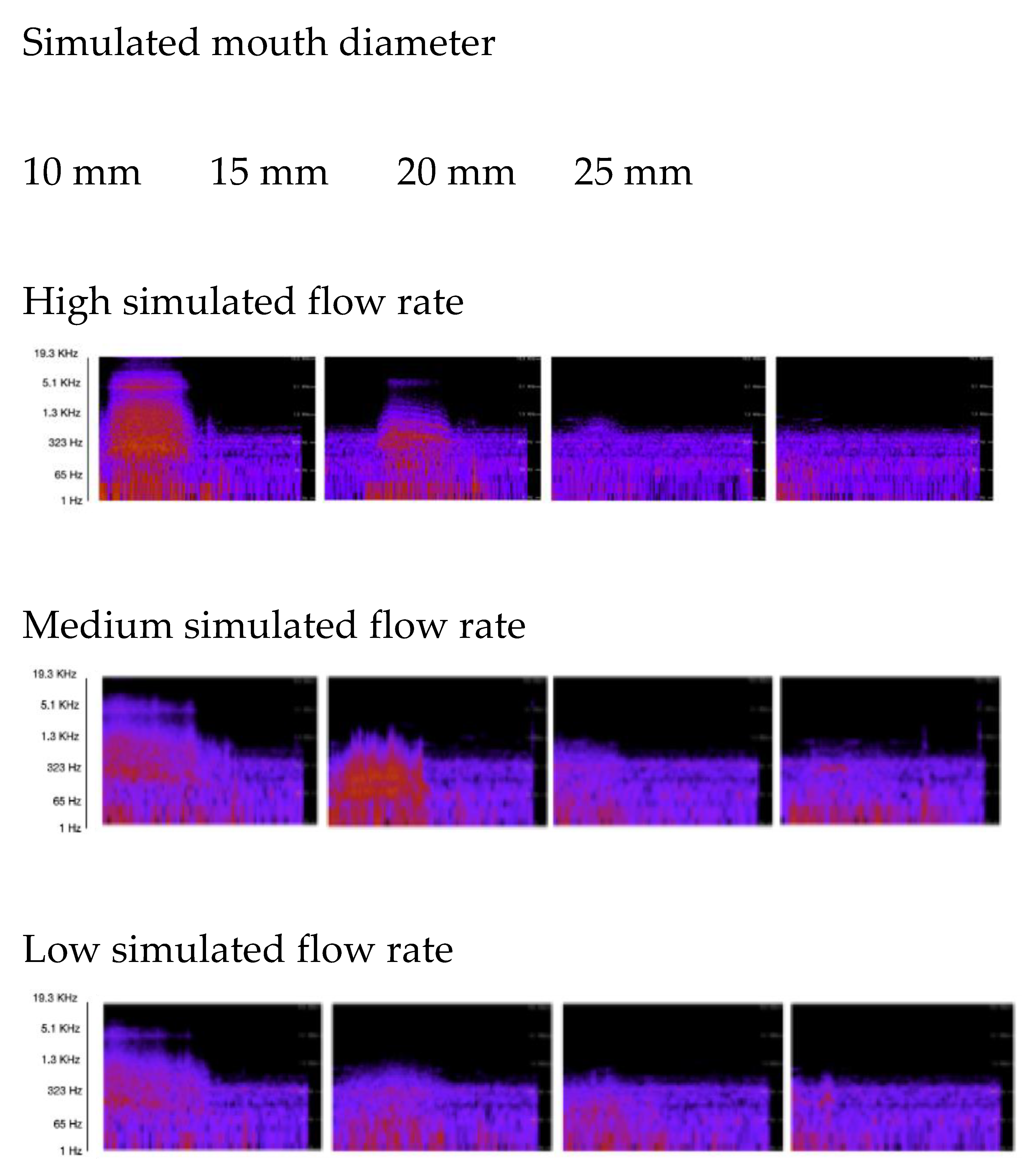
4.5. Audio Frequency Spectra for Simulated Inspirations
4.6. QUT Inspire Application Testing with Audio Samples
5. Discussion
6. Conclusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahlstrom, C.; Johansson, A.; Hult, P.; Ask, P. Chaotic dynamics of respiratory sounds. Chaos Solitons Fractals 2006, 29, 1054–1062. [Google Scholar] [CrossRef]
- Islam, M.S.; Paul, G.; Ong, H.X.; Young, P.M.; Gu, Y.T.; Saha, S.C. A review of respiratory anatomical development, air flow characterization and particle deposition. Int. J. Environ. Res. Public Health 2020, 17, 380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, R. Understanding Smart Sensors, 3rd ed.; Artech House: Boston, MA, USA, 2013; pp. 1–14. [Google Scholar]
- Gerhardt, U.; Breitschwerdt, R.; Thomas, O. mHealth Engineering: A Technology Review. J. Inf. Technol. Theory Appl. 2018, 19, 82–117. [Google Scholar]
- Ginsburg, A.S.; Lenahan, J.L.; Izadnegahdar, R.; Ansermino, J.M. A systematic review of tools to measure respiratory rate in order to identify childhood pneumonia. Am. J. Respir. Crit. Care Med. 2018, 197, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Abeyratne, U.R.; Swarnkar, V.; Setyati, A.; Triasih, R. Cough sound analysis can rapidly diagnose childhood pneumonia. Ann. Biomed. Eng. 2013, 41, 2448–2462. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, F.; Mostafa, S.S.; Ravelo-García, A.G.; Morgado-Dias, F.; Penzel, T. Devices for home detection of obstructive sleep apnea: A review. Sleep Med. Rev. 2018, 41, 149–160. [Google Scholar] [CrossRef]
- Kikidis, D.; Konstantinos, V.; Tzovaras, D.; Usmani, O. The Digital Asthma Patient: The History and Future of Inhaler Based Health Monitoring Devices. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 219–232. [Google Scholar] [CrossRef]
- Larson, E.C.; Goel, M.; Boriello, G.; Heltshe, S.; Rosenfeld, M.; Patel, S.N. SpiroSmart: Using a microphone to measure lung function on a mobile phone. In Proceedings of the 2012 ACM Conference on Ubiquitous Computing—UbiComp’12, Pittsburgh, PA, USA, 5–8 September 2012; Association for Computing Machinery: New York, NY, USA, 2012; pp. 280–290. [Google Scholar]
- Mikalsen, I.B.; Nassehi, D.; Øymar, K. Vortex Whistle and Smart Phone Application for Peak Flow Recordings in Asthmatic Children: A Feasibility Study. Telemed. E-Health 2019, 25, 1077–1082. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, S.; Parks, A.; Leopard, P.; Albright, C.; Carlson, J.; Goel, M.; Nassehi, D.; Larson, E.C. Design and learnability of vortex whistles for managing chronic lung function via smartphones. In Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Heidelberg, Germany, 12–16 September 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 569–580. [Google Scholar]
- Bastawrous, A.; Armstrong, M. Mobile health use in low-and high-income countries: An overview of the peer-reviewed literature. J. R. Soc. Med. 2013, 106, 130–142. [Google Scholar] [CrossRef] [Green Version]
- Laamarti, F.; Eid, M.; El Saddik, A. An overview of serious games. Intern. J. Comput. Games Technol. 2014, 1–15. [Google Scholar] [CrossRef]
- Colombo, V.; Aliverti, A.; Sacco, M. Virtual reality for COPD rehabilitation: A technological perspective. Pulmonology 2020, in press. [Google Scholar] [CrossRef]
- Mazzoleni, S.; Montagnani, G.; Vagheggini, G.; Buono, L.; Moretti, F.; Dario, P.; Ambrosino, N. Interactive videogame as rehabilitation tool of patients with chronic respiratory diseases: Preliminary results of a feasibility study. Respir. Med. 2014, 108, 1516–1524. [Google Scholar] [CrossRef] [Green Version]
- Restrepo, R.D.; Wettstein, R.; Wittnebel, L.; Tracy, M. Incentive Spirometry: 2011. Respir. Care 2011, 56, 1600–1604. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Chau, B.; Lui, M.; Lam, G.T.; Lin, N.; Humbert, S. Physical medicine and rehabilitation and pulmonary rehabilitation for COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 769–774. [Google Scholar] [CrossRef]
- Marshall, J.; Mueller, F.F.; Benford, S.; Pijnappel, S. Expanding exertion gaming. Int. J. Hum. Comput. Stud. 2016, 90, 1–13. [Google Scholar] [CrossRef]
- Pirovano, M.; Surer, E.; Mainetti, R.; Lanzi, P.L.; Alberto Borghese, N. Exergaming and rehabilitation: A methodology for the design of effective and safe therapeutic exergames. Entertain. Comput. 2016, 14, 55–65. [Google Scholar] [CrossRef]
- Herron, J. Bad Apps: mHealth Apps Doubling as Medical Devices. J. Electron. Res. Med. Libr. 2016, 13, 177–181. [Google Scholar] [CrossRef]
- Cheng, Q.; Juen, J.; Bellam, S.; Fulara, N.; Close, D.; Silverstein, J.C.; Schatz, B. Predicting Pulmonary Function from Phone Sensors. Telemed. E-Health 2017, 23, 913–919. [Google Scholar] [CrossRef] [Green Version]
- Forgacs, P.; Nathoo, A.; Richardson, H. Breath sounds. Thorax 1971, 26, 288–295. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.; Marques, A. Respiratory sounds in healthy people: A systematic review. Respir. Med. 2014, 108, 550–570. [Google Scholar] [CrossRef] [Green Version]
- Shykoff, B.E.; Ploysongsang, Y.; Chang, H.K. Airflow and Normal Lung Sounds. Am. Rev. Respir. Dis. 1988, 137, 872–876. [Google Scholar] [CrossRef]
- Soufflet, G.; Charbonneau, G.; Polit, M.; Attal, P.; Denjean, A.; Escourrou, P.; Gaultier, C. Interaction Between Tracheal Sound and Flow Rate: A Comparison of Some Different Flow Evaluations from Lung Sounds. IEEE Trans. Biomed. Eng. 1990, 37, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Que, C.; Kolmaga, C.; Durand, L.; Kelly, S.M.; Macklem, P.T.; Phono-, P.T.M. Ventilation: Methodology and Preliminary Results. J. Appl. Physiol. 2002, 93, 1515–1526. [Google Scholar] [CrossRef] [Green Version]
- Umayahara, Y.; Soh, Z.; Sekikawa, K.; Kawae, T.; Otsuka, A.; Tsuji, T. Estimation of cough peak flow using cough sounds. Sensors 2018, 18, 2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celestina, M.; Hrovat, J.; Kardous, C.A. Smartphone-based sound level measurement apps: Evaluation of compliance with international sound level meter standards. Appl. Acoust. 2018, 139, 119–128. [Google Scholar] [CrossRef]
- Murphy, E.; King, E.A. Testing the accuracy of smartphones and sound level meter applications for measuring environmental noise. Appl. Acoust. 2016, 106, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Kardous, C.A.; Shaw, P.B. So How Good are These Smartphone Sound Measurement Apps? Update Counc. Accredit. Occup Hear. Conserv. 2013, 25, 1–2. [Google Scholar]
- Brown, R.; Evans, L. Acoustics and the smartphone. Acoustics 2011, 106, 106–111. [Google Scholar]
- Danaher, B.G.; Brendryen, H.; Seeley, J.R.; Tyler, M.S.; Woolley, T. From black box to toolbox: Outlining device functionality, engagement activities, and the pervasive information architecture of mHealth interventions. Internet Interv. 2015, 2, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Faezipour, M.; Faezipour, M. Sustainable smartphone-based healthcare systems: A systems engineering approach to assess the efficacy of respiratory monitoring apps. Sustainability 2020, 12, 5061. [Google Scholar] [CrossRef]
- Majumder, S.; Deen, M.J. Smartphone sensors for health monitoring and diagnosis. Sensors 2019, 19, 2164. [Google Scholar] [CrossRef] [Green Version]
- Gan, S.K.-E.; Koshy, C.; Nguyen, P.-V.; Haw, Y.-X. An overview of clinically and healthcare related apps in Google and Apple app stores: Connecting patients, drugs, and clinicians. Sci. Phone Apps Mob. Devices 2016, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Baxter, C.; Carroll, J.-A.; Keogh, B.; Vandelanotte, C. Assessment of Mobile Health Apps Using Built-In Smartphone Sensors for Diagnosis and Treatment: Systematic Survey of Apps Listed in International Curated Health App Libraries. JMIR Mhealth Uhealth 2020, 8, e16741. [Google Scholar] [CrossRef]
- Paglialonga, A.; Lugo, A.; Santoro, E. An overview on the emerging area of identification, characterization, and assessment of health apps. J. Biomed. Inform. 2018, 83, 97–102. [Google Scholar] [CrossRef]
- Lupton, D. The digitally engaged patient: Self-monitoring and self-care in the digital health era. Soc. Theory Health 2013, 11, 256–270. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile App Rating Scale: A New Tool for Assessing the Quality of Health Mobile Apps. JMIR Mhealth Uhealth 2015, 3, e27. [Google Scholar] [CrossRef] [Green Version]
- Wicks, P.; Chiauzzi, E. “Trust but verify”—Five approaches to ensure safe medical apps. BMC Med. 2015, 13, 1–5. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Recommendations on Digital Interventions for Health System Strengthening. WHO Guideline. 2019. Available online: https://www.who.int/publications/i/item/9789241550505 (accessed on 16 September 2021).
- Streiner, D.L.; Norman, G.R. “Precision” and “accuracy”: Two terms that are neither. J. Clin. Epidemiol. 2006, 59, 327–330. [Google Scholar] [CrossRef]
- Andrès, E.; Gass, R.; Charloux, A.; Brandt, C.; Hentzler, A. Respiratory sound analysis in the era of evidence-based medicine and the world of medicine 2.0. J. Med. Life 2018, 11, 89–106. [Google Scholar]
- Dirksen, A.; Madsen, F.; Pedersen, O.F.; Vedel, A.M.; Kok-Jensen, A. Long term performance of a hand held spirometer. Thorax 1996, 51, 973–976. [Google Scholar] [CrossRef] [Green Version]
- Hobbes, A.F.T. A comparison of methods of calibrating the pneumotachograph. Br. J. Anaesth. 1967, 39, 899–907. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Nam, Y.; Reyes, B.A.; Member, S.; Chon, K.H.; Member, S. Estimation of Respiratory Rates Using the Built-in Microphone of a Smartphone or Headset. IEEE J. Biomed. Health Inform. 2016, 20, 1493–1501. [Google Scholar] [CrossRef]
- Larson, E.C.; Goel, M.; Redfield, M.; Boriello, G.; Rosenfeld, M.; Patel, S.N. Tracking Lung Function on any Phone. In Proceedings of the DEV ’13 Annual Symposium on Computing for Development, Bangalore, India, 11–12 January 2013; Thies, B., Nanavati, A., Eds.; Association for Computing Machinery: New York, NY, USA, 2013; Volume 4, pp. 1–2. [Google Scholar]
- Goel, M.; Saba, E.; Stiber, M.; Whitmire, E.; Fromm, J.; Larson, E.C.; Borriello, G.; Patel, S.N. SpiroCall: Measuring lung function over a phone call. In Proceedings of the 2016 Conference on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 5675–5685. [Google Scholar]
- Trupti, A.; Pravin, A.; Subin, S. Effect of Incentive Spirometry on Cardiac Autonomic Functions in Normal Healthy Subjects. Indian J. Physiother. Occup. Therapy 2016, 7, 264–270. [Google Scholar]
- Craven, J.L.; Evans, G.A.; Davenport, P.J.; Williams, R.H.P. The evaluation of the incentive spirometer in the management of postoperative pulmonary complications. Br. J. Surg. 1974, 61, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A. Peak inspiratory flow rate: An emerging biomarker in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2019, 199, 1577–1579. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Pleasants, R.A.; Ohar, J.A.; Donohue, J.F.; Drummond, M.B. Prevalence and factors associated with suboptimal peak inspiratory flow rates in COPD. Int. J. COPD 2019, 14, 585–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, G.; Mahler, D.; Mayorga, V.; Deering, K.; Harshaw, Q.; Ganapathy, V. Prevalence of Low Peak Inspiratory Flow Rate at Discharge in Patients Hospitalized for COPD Exacerbation. J. COPD Found. 2017, 4, 217–224. [Google Scholar] [CrossRef]
- Kumar, A.S. Comparison of Flow and Volume Incentive Spirometry on Pulmonary Function and Exercise Tolerance in Open Abdominal Surgery: A Randomized Clinical Trial. J. Clin. Diagn. Res. 2016, 10, KC01–KC06. [Google Scholar] [CrossRef]
- Kirkwood, B.; Sterne, A. Regression modelling. In Essential Medical Statistics, 2nd ed.; Blackwell Publishers: Carlton, Australia, 2003; pp. 315–342. [Google Scholar]
- Ambrosino, P.; Fuschillo, S.; Papa, A.; DI Minno, M.N.D.; Maniscalco, M. Exergaming as a Supportive Tool for Home-Based Rehabilitation in the COVID-19 Pandemic Era. Games Health J. 2020, 9, 311–313. [Google Scholar] [CrossRef]
- Chang, A.T.; Hons, B.; Palmer, K.R.; Hons, B.; Mcnaught, J. Inspiratory flow rate, not type of incentive spirometry device, influences chest wall motion in healthy individuals. Physiother. Theory Pract. 2010, 26, 385–392. [Google Scholar] [CrossRef]
- Kortli, Y.; Jridi, M.; Al Falou, A.; Atri, M. Face recognition systems: A survey. Sensors 2020, 20, 342. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Flow Rate | Counting Sequence |
|---|---|
| High | One, two, three |
| Medium | One, one hundred, two, one hundred |
| Low | One, one hundred thousand, two, one hundred thousand |
| Distance Between Smartphone and Audio Source | ||||||
|---|---|---|---|---|---|---|
| 1 cm | 2 cm | 5 cm | 10 cm | 20 cm | 50 cm | |
| High flow audio | ||||||
| Apple iPhone XR |  |  |  |  |  |  |
| Samsung Galaxy S10 |  |  |  |  |  |  |
| Medium flow audio | ||||||
| Apple iPhone XR |  |  |  |  |  |  |
| Samsung Galaxy S10 |  |  |  |  |  |  |
| Low flow audio | ||||||
| Apple iPhone XR |  |  |  |  |  |  |
| Samsung Galaxy S10 |  |  |  |  |  |  |
 = 10 mm;
= 10 mm;  = 15 mm;
= 15 mm;  = 20 mm;
= 20 mm;  = 25 mm.
= 25 mm.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baxter, C.; Carroll, J.-A.; Keogh, B.; Vandelanotte, C. Seeking Inspiration: Examining the Validity and Reliability of a New Smartphone Respiratory Therapy Exergame App. Sensors 2021, 21, 6472. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196472
Baxter C, Carroll J-A, Keogh B, Vandelanotte C. Seeking Inspiration: Examining the Validity and Reliability of a New Smartphone Respiratory Therapy Exergame App. Sensors. 2021; 21(19):6472. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196472
Chicago/Turabian StyleBaxter, Clarence, Julie-Anne Carroll, Brendan Keogh, and Corneel Vandelanotte. 2021. "Seeking Inspiration: Examining the Validity and Reliability of a New Smartphone Respiratory Therapy Exergame App" Sensors 21, no. 19: 6472. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196472