
Upper Limb Movement Measurement Systems for Cerebral Palsy: A Systematic Literature Review

 ,
,  ,
,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategies
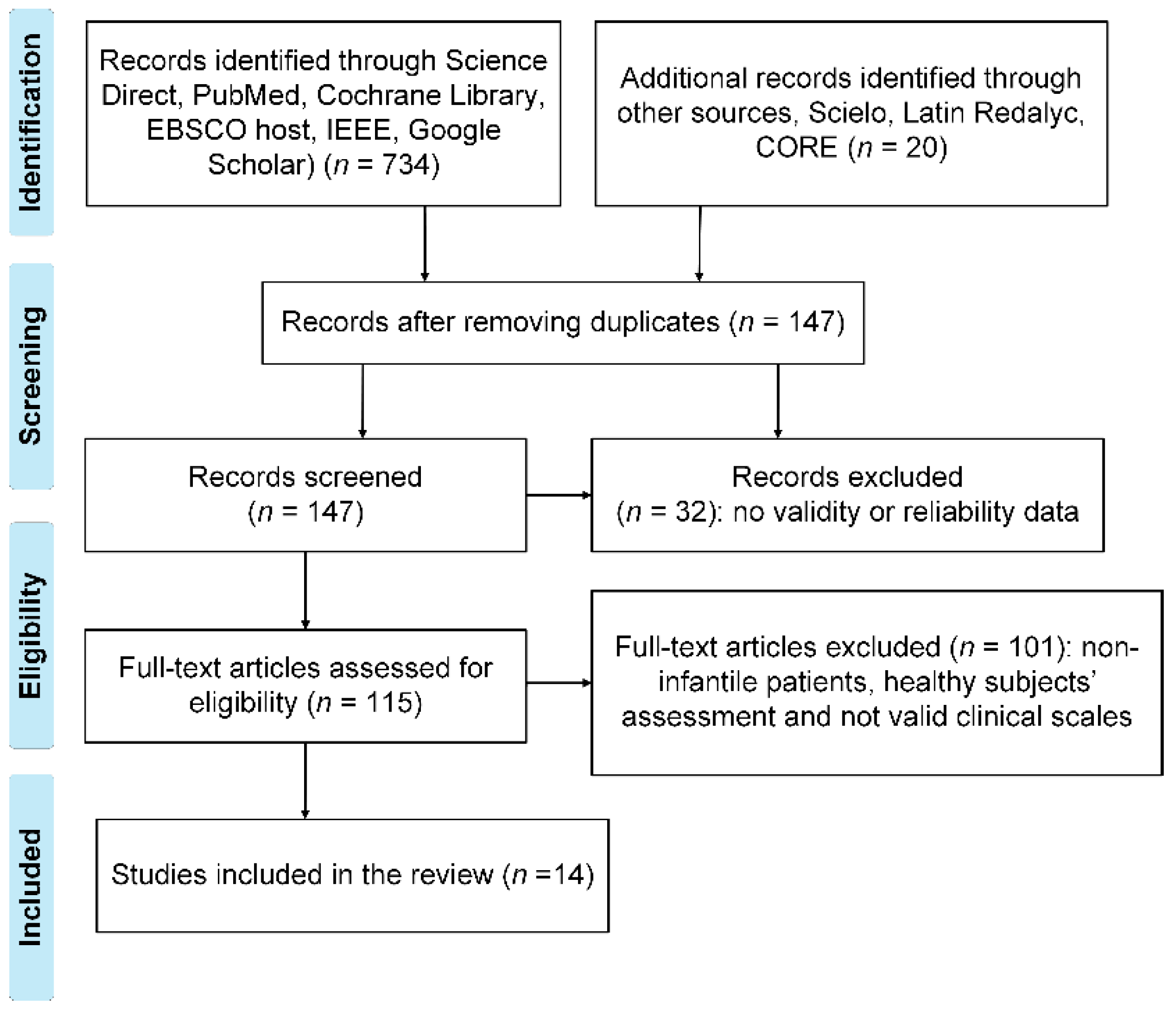
2.3. Study Selection
2.4. Data Extraction
3. Current Techniques for Objective Measurements
3.1. ROM Assessment
3.2. Kinematic Analysis
4. Discussion
4.1. Discussion of Assessment Methods
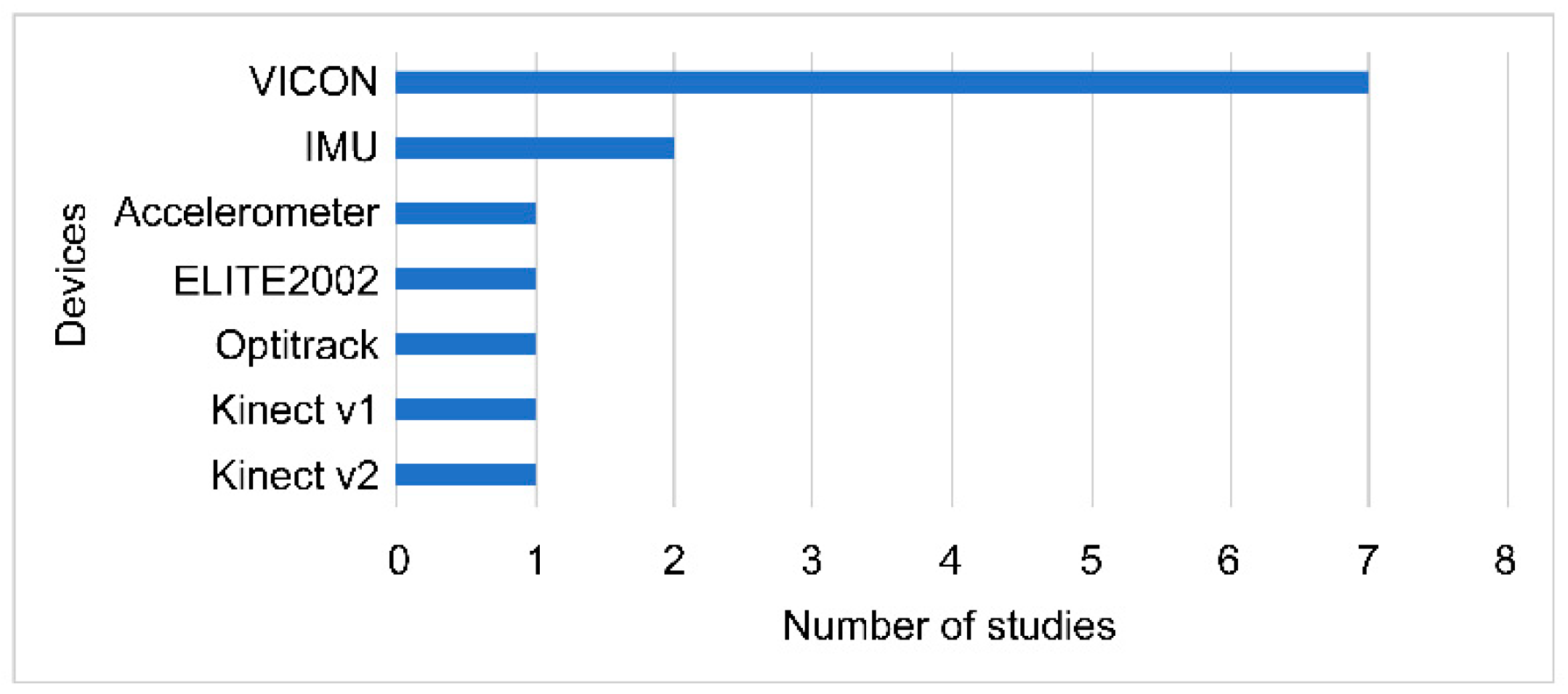
4.2. Discussion of Optoelectronic Devices
4.3. Discussion of Wearable Sensors
4.4. Discussion of the Low-Cost Sensor, Kinect
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 3D | Three-dimensional |
| AROM | Active range of motion |
| CP | Cerebral palsy |
| ISB | International Society of Biomechanics |
| VR | Virtual reality |
| LDJM | Log dimensionless jerk metric |
| MUUL | Melbourne Assessment of Unilateral Upper Limb Function |
| NUI | Natural user interface |
| PM | Peak metric |
| PROM | Passive range of motion |
| QUEST | Quality of Upper Extremity Skills Test |
| ROM | Range of motion |
| SALM | Spectral arc length metric |
| SHUEE | Shriners Hospital Upper Extremity Evaluation |
References
- Norkin, C.C.; White, D.J. Measurement of Joint Motion: A Guide to Goniometry, 5th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2016. [Google Scholar]
- Mesquita, I.A.; Fonseca, P.; Borgonovo-Santos, M.; Ribeiro, E.; Pinheiro, A.R.V.; Correia, M.V.; Silva, C. Comparison of upper limb kinematics in two activities of daily living with different handling requirements. Hum. Mov. Sci. 2020, 72, 102632. [Google Scholar] [CrossRef]
- Karakostas, T.; Watters, K.; King, E.C. Assessment of the Spastic Upper Limb with Computational Motion Analysis. Hand Clin. 2018, 34, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Lannin, N.A.; Borschmann, K.; English, C.; Ali, M.; Churilov, L.; Saposnik, G.; Winstein, C.; van Wegen, E.E.H.; Wolf, S.L.; et al. Standardized Measurement of Sensorimotor Recovery in Stroke Trials: Consensus-Based Core Recommendations from the Stroke Recovery and Rehabilitation Roundtable. Neurorehabil. Neural Repair 2017, 31, 784–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaspers, E.; Desloovere, K.; Bruyninckx, H.; Molenaers, G.; Klingels, K.; Feys, H. Review of quantitative measurements of upper limb movements in hemiplegic cerebral palsy. Gait Posture 2009, 30, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, C. Definition and classification of cerebral palsy: A historical perspective. Dev. Med. Child Neurol. Suppl. 2007, 109, 3–7. [Google Scholar] [CrossRef]
- World Health Organization. Disability and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/disability-and-health (accessed on 8 March 2021).
- Niedzwecki, C.M.; Thomas, S.P.; Schwabe, A.L. 47—Cerebral Palsy. In Braddom’s Physical Medicine and Rehabilitation, 6th ed.; Cifu, D.X., Ed.; Elsevier: Philadelphia, PA, USA, 2021; pp. 1006–1026.e2. [Google Scholar]
- APAMP. Cifras Sobre Parálisis Cerebral. Available online: http://www.apamp.org/cifras_paralisiscerebral.html (accessed on 8 March 2021).
- Chin, E.M.; Gwynn, H.E.; Robinson, S.; Hoon, A.H., Jr. Principles of Medical and Surgical Treatment of Cerebral Palsy. Neurol. Clin. 2020, 38, 397–416. [Google Scholar] [CrossRef]
- Koman, L.A.; Smith, B.P.; Shilt, J.S. Cerebral palsy. Lancet 2004, 363, 1619–1631. [Google Scholar] [CrossRef]
- Bard, R.; Chaléat-Valayer, E.; Combey, A.; Bleu, P.E.; Perretant, I.; Bernard, J.C. Upper limb assessment in children with cerebral palsy: Translation and reliability of the French version for the Melbourne unilateral upper limb assessment (test de Melbourne). Ann. Phys. Rehabil. Med. 2009, 52, 297–310. [Google Scholar] [CrossRef] [Green Version]
- de los Reyes-Guzmán, A.; Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; Monasterio-Huelin, F.; Torricelli, D.; Gil-Agudo, A. Quantitative assessment based on kinematic measures of functional impairments during upper extremity movements: A review. Clin. Biomech. 2014, 29, 719–727. [Google Scholar] [CrossRef] [Green Version]
- Pérez-de la Cruz, S.; de León, Ó.A.; Mallada, N.P.; Rodríguez, A.V. Validity and intra-examiner reliability of the Hawk goniometer versus the universal goniometer for the measurement of range of motion of the glenohumeral joint. Med. Engl. Phys. 2021, 89, 7–11. [Google Scholar] [CrossRef]
- Fard, M.K.; Fallah, A.; Maleki, A. The compensation of biomechanical errors in electrogoniometric measurements of the upper extremity kinematics. Sens. Actuators A Phys. 2020, 315, 112170. [Google Scholar] [CrossRef]
- Mohammed, H.E.; Wael, O.A.A.E.-k. Validity and intra-rater reliability of laser goniometer versus electro-goniometer in measuring shoulder range of motion. Int. J. Physiother. 2019, 6, 169–176. [Google Scholar]
- Tozzo, M.C.; Ansanello, W.; Martins, J.; Zatiti, S.C.A.; de Oliveira, A.S. Inclinometer Reliability for Shoulder Ranges of Motion in Individuals With Subacromial Impingement Syndrome. J. Manip. Physiol. Ther. 2021, 44, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Martín-San Agustín, R.; García-Vidal, J.A.; Cánovas-Ambit, G.; Arenas-Della Vecchia, A.; López-Nicolás, M.; Medina-Mirapeix, F. Validity and Reliability of a New Optoelectronic System for Measuring Active Range of Motion of Upper Limb Joints in Asymptomatic and Symptomatic Subjects. J. Clin. Med. 2019, 8, 1851. [Google Scholar] [CrossRef] [Green Version]
- Topley, M.; Richards, J.G. A comparison of currently available optoelectronic motion capture systems. J. Biomech. 2020, 106, 109820. [Google Scholar] [CrossRef] [PubMed]
- Raghu, S.L.; Kang, C.K.; Whitehead, P.; Takeyama, A.; Conners, R. Static accuracy analysis of Vicon T40s motion capture cameras arranged externally for motion capture in constrained aquatic environments. J. Biomech. 2019, 89, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, E.; Feys, H.; Bruyninckx, H.; Cutti, A.; Harlaar, J.; Molenaers, G.; Desloovere, K. The reliability of upper limb kinematics in children with hemiplegic cerebral palsy. Gait Posture 2011, 33, 568–575. [Google Scholar] [CrossRef]
- Mourcou, Q.; Fleury, A.; Diot, B.; Franco, C.; Vuillerme, N. Mobile Phone-Based Joint Angle Measurement for Functional Assessment and Rehabilitation of Proprioception. BioMed Res. Int. 2015, 2015, 328142. [Google Scholar] [CrossRef] [Green Version]
- Werner, B.C.; Holzgrefe, R.E.; Griffin, J.W.; Lyons, M.L.; Cosgrove, C.T.; Hart, J.M.; Brockmeier, S.F. Validation of an innovative method of shoulder range-of-motion measurement using a smartphone clinometer application. J. Shoulder Elbow Surg. 2014, 23, e275–e282. [Google Scholar] [CrossRef]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.-S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [Green Version]
- Rigoni, M.; Gill, S.; Babazadeh, S.; Elsewaisy, O.; Gillies, H.; Nguyen, N.; Pathirana, P.N.; Page, R. Assessment of Shoulder Range of Motion Using a Wireless Inertial Motion Capture Device-A Validation Study. Sensors 2019, 19, 1781. [Google Scholar] [CrossRef] [Green Version]
- Picerno, P.; Viero, V.; Donati, M.; Triossi, T.; Tancredi, V.; Melchiorri, G. Ambulatory assessment of shoulder abduction strength curve using a single wearable inertial sensor. J. Rehabil. Res. Dev. 2015, 52, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Morrow, M.M.B.; Lowndes, B.; Fortune, E.; Kaufman, K.R.; Hallbeck, M.S. Validation of Inertial Measurement Units for Upper Body Kinematics. J. Appl. Biomech. 2017, 33, 227–232. [Google Scholar] [CrossRef]
- Bai, L.; Pepper, M.G.; Yana, Y.; Spurgeon, S.K.; Sakel, M. Application of low cost inertial sensors to human motion analysis. In Proceedings of the 2012 IEEE International Instrumentation and Measurement Technology Conference Proceedings, Graz, Austria, 13–16 May 2012; pp. 1280–1285. [Google Scholar]
- Çubukçu, B.; Yüzgeç, U.; Zileli, R.; Zileli, A. Reliability and validity analyzes of Kinect V2 based measurement system for shoulder motions. Med. Engl. Phys. 2020, 76, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha Neto, J.S.; Rebouças Filho, P.P.; Da Silva, G.P.F.; Da Cunha Olegario, N.B.; Duarte, J.B.F.; De Albuquerque, V.H.C. Dynamic evaluation and treatment of the movement amplitude using Kinect sensor. IEEE Access 2018, 6, 17292–17305. [Google Scholar] [CrossRef]
- Franco-García, J.M.; Rodal, M.; Gutiérrez-Horrillo, R.; Carlos-Vivas, J.; Pérez-Gómez, J.; Nobari, H.; Ardigò, L.P.; Gianikellis, K. Shoulder Kinematics and Symmetry at Different Load Intensities during Bench Press Exercise. Symmetry 2021, 13, 1859. [Google Scholar] [CrossRef]
- Uhlár, Á.; Ambrus, M.; Kékesi, M.; Fodor, E.; Grand, L.; Szathmáry, G.; Rácz, K.; Lacza, Z. Kinect Azure–Based Accurate Measurement of Dynamic Valgus Position of the Knee—A Corrigible Predisposing Factor of Osteoarthritis. Appl. Sci. 2021, 11, 5536. [Google Scholar] [CrossRef]
- de Oliveira, J.M.; Munoz, R.; Ribeiro, S.; Wu, W.; de Albuquerque, V.H.C. REHAB FUN: An assistive technology in neurological motor disorders rehabilitation of children with cerebral palsy. Neural Comput. Appl. 2020, 32, 10957–10970. [Google Scholar] [CrossRef]
- Gutiérrez Zúñiga, R.; Alonso de Leciñana, M.; Díez, A.; Torres Iglesias, G.; Pascual, A.; Higashi, A.; Rodríguez Pardo, J.; Hernández Herrero, D.; Fuentes, B.; Díez Tejedor, E. A New Software for Quantifying Motor Deficit After Stroke: A Case-Control Feasibility Pilot Study. Front. Neurol. 2021, 12, 603619. [Google Scholar] [CrossRef]
- Kohout, J.; Verešpejová, L.; Kříž, P.; Červená, L.; Štícha, K.; Crha, J.; Trnková, K.; Chovanec, M.; Mareš, J. Advanced Statistical Analysis of 3D Kinect Data: Mimetic Muscle Rehabilitation Following Head and Neck Surgeries Causing Facial Paresis. Sensors 2020, 21, 103. [Google Scholar] [CrossRef]
- Quan, L.; Li, H.; Li, H.; Jiang, W.; Lou, Z.; Chen, L. Two-Stream Dense Feature Fusion Network Based on RGB-D Data for the Real-Time Prediction of Weed Aboveground Fresh Weight in a Field Environment. Remote Sens. 2021, 13, 2288. [Google Scholar] [CrossRef]
- Sempere-Tortosa, M.; Fernández-Carrasco, F.; Mora-Lizán, F.; Rizo-Maestre, C. Objective Analysis of Movement in Subjects with ADHD. Multidisciplinary Control Tool for Students in the Classroom. Int. J. Environ. Res. Public Health 2020, 17, 5620. [Google Scholar] [CrossRef]
- Pavão, S.L.; Arnoni, J.L.; de Oliveira, A.K.; Rocha, N.A. Impact of a virtual reality-based intervention on motor performance and balance of a child with cerebral palsy: A case study. Rev. Paul. Pediatr. 2014, 32, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, R.; Molina, A.; Gómez, I.; García-Heras, J. Kinect as an access device for people with cerebral palsy: A preliminary study. Int. J. Hum. Comput. Stud. 2017, 108, 62–69. [Google Scholar] [CrossRef]
- Camara Machado, F.R.; Antunes, P.P.; Souza, J.M.; Santos, A.C.D.; Levandowski, D.C.; Oliveira, A.A. Motor Improvement Using Motion Sensing Game Devices for Cerebral Palsy Rehabilitation. J. Mot. Behav. 2017, 49, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Cheung, J.; Maron, M.; Tatla, S.; Jarus, T. Virtual reality as balance rehabilitation for children with brain injury: A case study. Technol. Disabil. 2013, 25, 207–219. [Google Scholar] [CrossRef]
- Zhenli, L.; Xuanlin, S.; Jun, L.; Guodong, Z.; Chenbin, G. Design of a cerebral palsy rehabilitation training system based on Kinect motion interactive mode. High Technol. Commun. 2016, 26, 1014–1021. [Google Scholar]
- Luna-Oliva, L.; Ortiz-Gutiérrez, R.M.; Cano-de la Cuerda, R.; Piédrola, R.M.; Alguacil-Diego, I.M.; Sánchez-Camarero, C.; Martínez Culebras Mdel, C. Kinect Xbox 360 as a therapeutic modality for children with cerebral palsy in a school environment: A preliminary study. NeuroRehabilitation 2013, 33, 513–521. [Google Scholar] [CrossRef]
- Monge Pereira, E.; Molina Rueda, F.; Alguacil Diego, I.M.; Cano de la Cuerda, R.; de Mauro, A.; Miangolarra Page, J.C. Use of virtual reality systems as proprioception method in cerebral palsy: Clinical practice guideline. Neurologia 2014, 29, 550–559. [Google Scholar] [CrossRef]
- Pourazar, M.; Mirakhori, F.; Hemayattalab, R.; Bagherzadeh, F. Use of virtual reality intervention to improve reaction time in children with cerebral palsy: A randomized controlled trial. Dev. Neurorehabil. 2018, 21, 515–520. [Google Scholar] [CrossRef]
- Rathinam, C.; Mohan, V.; Peirson, J.; Skinner, J.; Nethaji, K.S.; Kuhn, I. Effectiveness of virtual reality in the treatment of hand function in children with cerebral palsy: A systematic review. J. Hand Ther. 2019, 32, 426–434.e421. [Google Scholar] [CrossRef] [PubMed]
- Arnoni, J.L.B.; Pavão, S.L.; Dos Santos Silva, F.P.; Rocha, N. Effects of virtual reality in body oscillation and motor performance of children with cerebral palsy: A preliminary randomized controlled clinical trial. Complement. Ther. Clin. Pract. 2019, 35, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Clutterbuck, G.; Auld, M.; Johnston, L. Active exercise interventions improve gross motor function of ambulant/semi-ambulant children with cerebral palsy: A systematic review. Disabil. Rehabil. 2019, 41, 1131–1151. [Google Scholar] [CrossRef]
- Deutsch, J.E.; Westcott McCoy, S. Virtual Reality and Serious Games in Neurorehabilitation of Children and Adults: Prevention, Plasticity, and Participation. Pediatr. Phys. Ther. 2017, 29 (Suppl. 3), S23–S36. [Google Scholar] [CrossRef] [PubMed]
- Lachat, E.; Macher, H.; Landes, T.; Grussenmeyer, P. Assessment and calibration of a RGB-D camera (Kinect v2 sensor) towards a potential use for close-range 3D modeling. Remote Sens. 2015, 7, 13070–13097. [Google Scholar] [CrossRef] [Green Version]
- Gaillard, F.; Cacioppo, M.; Bouvier, B.; Bouzille, G.; Newman, C.J.; Pasquet, T.; Cretual, A.; Rauscent, H.; Bonan, I. Assessment of bimanual performance in 3-D movement analysis: Validation of a new clinical protocol in children with unilateral cerebral palsy. Ann. Phys. Rehabil. Med. 2019, 63, 408–415. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, M.; Bani Mohammad, E.; Anshasi, H.A. Virtual Reality Technology for Pain and Anxiety Management among Patients with Cancer: A Systematic Review. Pain Manag. Nurs. 2020, 21, 601–607. [Google Scholar] [CrossRef]
- Fitoussi, F.; Diop, A.; Maurel, N.; El Mostefa, L.; Ilharreborde, B.; Penneçot, G.F. Upper limb motion analysis in children with hemiplegic cerebral palsy: Proximal kinematic changes after distal botulinum toxin or surgical treatments. J. Child. Orthop. 2011, 5, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Jaspers, E.; Desloovere, K.; Bruyninckx, H.; Klingels, K.; Molenaers, G.; Aertbeliën, E.; Van Gestel, L.; Feys, H. Three-dimensional upper limb movement characteristics in children with hemiplegic cerebral palsy and typically developing children. Res. Dev. Disabil. 2011, 32, 2283–2294. [Google Scholar] [CrossRef]
- Howcroft, J.; Klejman, S.; Fehlings, D.; Wright, V.; Zabjek, K.; Andrysek, J.; Biddiss, E. Active video game play in children with cerebral palsy: Potential for physical activity promotion and rehabilitation therapies. Arch. Phys. Med. Rehabil. 2012, 93, 1448–1456. [Google Scholar] [CrossRef] [PubMed]
- Galli, M.; Cimolin, V.; Albertini, G.; Piccinini, L.; Turconi, A.C.; Romkes, J.; Brunner, R. Kinematic analysis of upper limb during walking in diplegic children with Cerebral Palsy. Eur. J. Paediatr. Neurol. 2014, 18, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Sarcher, A.; Raison, M.; Ballaz, L.; Lemay, M.; Leboeuf, F.; Trudel, K.; Mathieu, P.A. Impact of muscle activation on ranges of motion during active elbow movement in children with spastic hemiplegic cerebral palsy. Clin. Biomech. 2015, 30, 86–94. [Google Scholar] [CrossRef]
- Sevick, M.; Eklund, E.; Mensch, A.; Foreman, M.; Standeven, J.; Engsberg, J. Using Free Internet Videogames in Upper Extremity Motor Training for Children with Cerebral Palsy. Behav. Sci. 2016, 6, 10. [Google Scholar] [CrossRef]
- Anaya-Campos, L.; Quijano-González, Y.; Quiñones-Urióstegui, I.; Alessi-Montero, A.; Bueyes-Roiz, V.; Chong-Quero, J. Segmentación automática del movimiento en la valoración funcional del miembro superior en niños con parálisis cerebral. Rev. Mex. Ingeniería Biomed. 2017, 38, 343–356. [Google Scholar]
- Mailleux, L.; Jaspers, E.; Ortibus, E.; Simon-Martinez, C.; Desloovere, K.; Molenaers, G.; Klingels, K.; Feys, H. Clinical assessment and three-dimensional movement analysis: An integrated approach for upper limb evaluation in children with unilateral cerebral palsy. PLoS ONE 2017, 12, e0180196. [Google Scholar]
- Kim, D.H.; An, D.H.; Yoo, W.G. Measurement of upper limb movement acceleration and functions in children with cerebral palsy. Technol. Health Care 2018, 26, 429–435. [Google Scholar] [CrossRef]
- Cacioppo, M.; Marin, A.; Rauscent, H.; Le Pabic, E.; Gaillard, F.; Brochard, S.; Garlantezec, R.; Cretual, A.; Bonan, I. A new child-friendly 3D bimanual protocol to assess upper limb movement in children with unilateral cerebral palsy: Development and validation. J. Electromyogr. Kinesiol. 2020, 55, 102481. [Google Scholar] [CrossRef]
- Daoud, M.I.; Alhusseini, A.; Ali, M.Z.; Alazrai, R. A Game-Based Rehabilitation System for Upper-Limb Cerebral Palsy: A Feasibility Study. Sensors 2020, 20, 2416. [Google Scholar] [CrossRef]
- Shim, D.; Choi, J.Y.; Yi, S.H.; Park, E.S.; Kim, S.; Yoo, B.; Park, D.; Park, H.R.; Rha, D.W. Spatiotemporal parameters from instrumented motion analysis represent clinical measurement of upper limb function in children with cerebral palsy. Gait Posture 2020. [Google Scholar] [CrossRef]
- Povedano, E.; Gallardo-Calero, I.; Navarrete, M.; Adillon, C.; Knorr, J.; Soldado, F. Analysis of dynamic elbow flexion deformity in children with hemiplegic cerebral palsy. Clin. Biomech. 2021, 81, 105245. [Google Scholar] [CrossRef]
- Guzsvinecz, T.; Szucs, V.; Sik-Lanyi, C. Suitability of the Kinect Sensor and Leap Motion Controller—A Literature Review. Sensors 2019, 19, 1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, M.E.; Seitz, A.L.; Leeser, M.; Sternad, D. Validity and reliability of Kinect skeleton for measuring shoulder joint angles: A feasibility study. Physiotherapy 2015, 101, 389–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jariwala, A.C.; Kiran, M.; Hyndman, I.; Johnston, L.R.; Wang, W.; Abboud, R.J.; Wigderowitz, C.A. Kinematic 3-D motion analysis of shoulder resurfacing hemiarthroplasty—An objective assessment method. J. Biomech. 2021, 122, 110454. [Google Scholar] [CrossRef] [PubMed]
- Krasowicz, K.; Michoński, J.; Liberadzki, P.; Sitnik, R. Monitoring Improvement in Infantile Cerebral Palsy Patients Using the 4DBODY System-A Preliminary Study. Sensors 2020, 20, 3232. [Google Scholar] [CrossRef]
- Amazon.com. Sensor Kinect de Xbox One—Standard Edition. Available online: https://www.amazon.com.mx/dp/B00INAX3Q2/ref=cm_sw_em_r_mt_dp_XBQJDW2SS8A9NPMHQXWG (accessed on 17 November 2021).
- Agostinelli, T.; Generosi, A.; Ceccacci, S.; Khamaisi, R.K.; Peruzzini, M.; Mengoni, M. Preliminary Validation of a Low-Cost Motion Analysis System Based on RGB Cameras to Support the Evaluation of Postural Risk Assessment. Appl. Sci. 2021, 11, 10645. [Google Scholar] [CrossRef]
- Scano, A.; Mira, R.M.; Cerveri, P.; Molinari Tosatti, L.; Sacco, M. Analysis of Upper-Limb and Trunk Kinematic Variability: Accuracy and Reliability of an RGB-D Sensor. Multimodal Technol. Interact. 2020, 4, 14. [Google Scholar] [CrossRef]
- Moreira, R.; Teles, A.; Fialho, R.; Baluz, R.; Santos, T.C.; Goulart-Filho, R.; Rocha, L.; Silva, F.J.; Gupta, N.; Bastos, V.H.; et al. Mobile Applications for Assessing Human Posture: A Systematic Literature Review. Electronics 2020, 9, 1196. [Google Scholar] [CrossRef]
- Wasenmüller, O.; Stricker, D. Comparison of kinect v1 and v2 depth images in terms of accuracy and precision. In Computer Vision—ACCV 2016 Workshops; Springer: Cham, Switzerland, 2017; pp. 34–45. [Google Scholar]
- Glonek, G.; Wojciechowski, A. Hybrid Orientation Based Human Limbs Motion Tracking Method. Sensors 2017, 17, 2857. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author | Downs and Black (n = 27) | Population (n) | Protocol | Clinical Scale |
|---|---|---|---|---|
| Gaillard et al. [51] | 22 | 20 | Carry out four bimanual tasks during three consecutive evaluations | AHA and ABILHAND-Kids |
| Fitoussi et al. [55] | 25 | 27 | Two daily tasks named “to drink” and “to move an object” | Ashworth Scale |
| Jaspers et al. [56] | 20 | 20 | Three reach tasks (forward, upward, and sideways) for two sessions | MACS |
| Howcroft et al. [57] | 22 | 17 | Play four games for 8 min with a 5 min rest interval in between | Physical Activity Enjoyment Scale (PACES) |
| Galli et al. [58] | 23 | 16 | 3D video recording and gait analysis along a 10 m walkway | ROM |
| Sarcher et al. [59] | 22 | 15 | Perform eight different tasks for four cycles with a 2 min break between each task | Modified MACS and Ashworth Scale (MAS) |
| Sevick et al. [60] | 19 | 4 | Playing four different games in an hour three times a week over twelve weeks | GMFCS, MACS, and BOT-2 Bruininks–Oseretsy Motor Behavior Test Scale |
| Anaya Campos et al. [61] | 19 | 16 | Insert pieces into a board three times on each side and then return them to their original places | MAS, Tardieu, MACS, and BFMF |
| Mailleux et al. [62] | 24 | 50 | Eight movement repetitions per task | MACS, AHA, and Melbourne Assessment 2 |
| Kim et al. [63] | 20 | 15 | Perform a scoping task three times with a 10 s break between each assessment | Jebsen Taylor Hand Function Test (JTHFT), QUEST, Box and Blocks Test (BBT), and ABILHAND-Kids |
| Cacioppo et al. [64] | 23 | 20 | Perform five bimanual tasks during a complete cycle | MACS |
| Daoud et al. [65] | 20 | 6 | 180 game-playing over 12 to 16 recording periods | Motion-Pose Geometric Descriptor (MPGD) |
| Shim et al. [66] | 21 | 40 | Motion capture in four phases (T1–T4) during a reach and grasp task | Melbourne Assessment 2 |
| Povedano et al. [67] | 23 | 16 | Eight activities per day with four repetitions per task in a 90 min session | GMFCS, MACS, and SHUEE |
| Author | Type of Devices | Manufacturer Device | Parameters | Method | N° 3D Markers | N° of Cameras | Frequency Sampling | Kinematic Model | Algorithm | ISB |
|---|---|---|---|---|---|---|---|---|---|---|
| Gaillard et al. [51] | OptiTrack optoelectronic system | Motion Analysis, Corvallis, OR, USA | AROM, kinematic analysis | Retroreflective markers | 26 | 12 | 100 Hz | X Euler angles | * | |
| Fitoussi et al. [55] | Vicon optoelectronic system | Oxford Metrics Group, UK | AROM and PROM, kinematic analysis | Retroreflective markers | 6 | 4 segments | X | |||
| Jaspers et al. [56] | Vicon optoelectronic system | Oxford Metrics Group, UK | Kinematic analysis | Retroreflective markers | 17 | 12–15 | 100 Hz | 5 segments | X BodyMech http://www.bodymech.nl (accessed on 30 August 2021) | * |
| Howcroft et al. [57] | Vicon optoelectronic system | Oxford Metrics Group, UK | Kinematic analysis | Retroreflective markers | 16 | 7 | 60 Hz | 10 segments | X | |
| Galli et al. [58] | ELITE2002 optoelectronic system | BTS, Milan, Italy | Kinematic analysis | Retroreflective markers | 26 | 100 Hz | X Euler angles | |||
| Sarcher et al. [59] | Vicon optoelectronic system | Oxford Metrics Group, UK | AROM, kinematic analysis | Retroreflective markers | 29 | 12 | 100 Hz | X | * | |
| Sevick et al. [60] | Kinect v1 | Microsoft, Redmond, WA, USA | AROM | NUI | 2 | 30 Hz | Flexible Action and Articulated Skeleton Toolkit (FAAST) software (Institute for Creative Technologies, CA) | |||
| Anaya Campos et al. [61] | IMU (Shimmer 3®) | Shimmer Research, Cambridge, MA, USA | Kinematic analysis, smoothness of movement metrics | Direct via inertial sensor | Spectral Arc Length Metric (SALM), Peaks Metric (PM), Log Dimensionless Jerk Metric (LDJM) | |||||
| Mailleux et al. [62] | Vicon optoelectronic system | Oxford Metrics Group, UK | Kinematic analysis | Retroreflective markers | 17 | 12–15 | 100 Hz | 5 segments | Upper Limb Evaluation in Motion Analysis (ULEMA) https://github.com/u0078867/ulema-ul-analyzer (accessed on 30 August 2021) | * |
| Kim et al. [63] | Accelerometer (Fitmeter) | Fitmeter, Fit.Life Inc., Suwon, Korea | Kinematic analysis | Direct via inertial sensor | 128 Hz | Peak acceleration curve, Fitmeter Manager 2 software (Fit.Life Inc., Suwon, Korea) | ||||
| Cacioppo et al. [64] | Vicon optoelectronic system | Oxford Metrics Group, UK | AROM, smoothness of movement metrics | Retroreflective markers | 26 | 10 | 100 Hz | X Arm Profile Score, Spectral arc length (SPARC), Index of curvature | * | |
| Daoud et al. [65] | Kinect v2 | Microsoft, Redmond, WA, USA | AROM | NUI | 2 | 30 Hz | X Extended Motion-Pose Geometric Descriptor | |||
| Shim et al. [66] | Vicon optoelectronic system | Oxford Metrics Group, UK | Kinematic analysis | Retroreflective markers | 100 Hz | X NEXUS software (Oxford Metrics Group, UK) | ||||
| Povedano et al. [67] | Tech-IMU V4 | Technaid, Madrid, Spain | Kinematic analysis | Direct via inertial sensor | 50 Hz | Tech-MCS V3 System (Technaid, Madrid, Spain) |
| Device | Movement | ROM (°) | Accuracy | Angular Velocity (°/s) | Acceleration (°/s2) | Peak Acceleration (m/s2) | PM (%) | SALM (%) | LDJM (%) | SPARC | Timing of Maximal Velocity % | Durations (s) | References |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vicon | Shoulder flexion (+) Extension (−) | −0.22–9.04 | −0.39 | 4.37 | [57] | ||||||||
| IMU | Hand and wrist | 43.74 | 64.76 | 33.33 | [61] | ||||||||
| Vicon | Elbow flexion/extension | 54.6–69.3 | 0.47 + | −0.63 + | [62] | ||||||||
| Accelerometer | Elbow flexion/extension | 0.80 ± 0.13 | [63] | ||||||||||
| Vicon | Shoulder rotation | 52.43 | 1.67 ± 0.22 | [64] | |||||||||
| Vicon | Elbow flexion/extension | −0.32 * | −0.25 * | [66] |
| References | Instrument/ Device | Manufacturer | ROM | Accuracy | Reliability (ICC) | Advantages | Disadvantages |
|---|---|---|---|---|---|---|---|
| Universal instrument | |||||||
| [14] | Goniometer | Passive | 5–10° | Intra-rater ± 9.6° Inter-rater ± 8.4° | Inexpensive, transportable, easy to use | Accuracy, its correct use depends mainly on the experience of the evaluator | |
| Optoelectronic device | |||||||
| [20,21,56] | Vicon | Oxford Metrics Group, UK | Active | <1 mm | Intra-rater: 0.54–0.91 Inter-rater: 0.70–0.96 | Accuracy in dynamic and static environments | Retroreflective body markers, expensive |
| Wearable sensors | |||||||
| [24,26,27] | IMU | Opal, APDM, Inc., Portland, OR USA | Active | 6.8 ± 2.7° | 0.930–0.979 | Small, portable, wireless, lightweight | Overestimates small joint angles and underestimates large joint angles |
| Low-cost sensors | |||||||
| [69] | Kinect v1 | Microsoft, Redmond, WA, USA | Active | ±5° | 0.76–0.98 | NUI, low-cost, markerless | Inaccurate measurements in the sagittal plane, |
| [29,30] | Kinect v2 | Microsoft, Redmond, WA, USA | Active | ±5° | 0.85–0.99 flexion 0.86–0.98 shoulder abduction | inaccurate measurements of ulnar and radial deviations of the upper limbs | |
| Other devices | |||||||
| [23] | Smartphone applications | Plaincode Software Solutions, Gunzenhausen, Germany | Passive | ±3.6° | 0.63–0.68 | Small, easy to use, affordable | Its correct use depends mainly on the experience of the evaluator |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francisco-Martínez, C.; Prado-Olivarez, J.; Padilla-Medina, J.A.; Díaz-Carmona, J.; Pérez-Pinal, F.J.; Barranco-Gutiérrez, A.I.; Martínez-Nolasco, J.J. Upper Limb Movement Measurement Systems for Cerebral Palsy: A Systematic Literature Review. Sensors 2021, 21, 7884. https://0-doi-org.brum.beds.ac.uk/10.3390/s21237884
Francisco-Martínez C, Prado-Olivarez J, Padilla-Medina JA, Díaz-Carmona J, Pérez-Pinal FJ, Barranco-Gutiérrez AI, Martínez-Nolasco JJ. Upper Limb Movement Measurement Systems for Cerebral Palsy: A Systematic Literature Review. Sensors. 2021; 21(23):7884. https://0-doi-org.brum.beds.ac.uk/10.3390/s21237884
Chicago/Turabian StyleFrancisco-Martínez, Celia, Juan Prado-Olivarez, José A. Padilla-Medina, Javier Díaz-Carmona, Francisco J. Pérez-Pinal, Alejandro I. Barranco-Gutiérrez, and Juan J. Martínez-Nolasco. 2021. "Upper Limb Movement Measurement Systems for Cerebral Palsy: A Systematic Literature Review" Sensors 21, no. 23: 7884. https://0-doi-org.brum.beds.ac.uk/10.3390/s21237884