Peculiarities of Platelet Metabolism in Patients with Acute Coronary Syndrome with Anxiety–Depressive Disorders and Informativity of Enzymes in the Forecast of Development of Cardiovascular Complications


Abstract
:1. Introduction
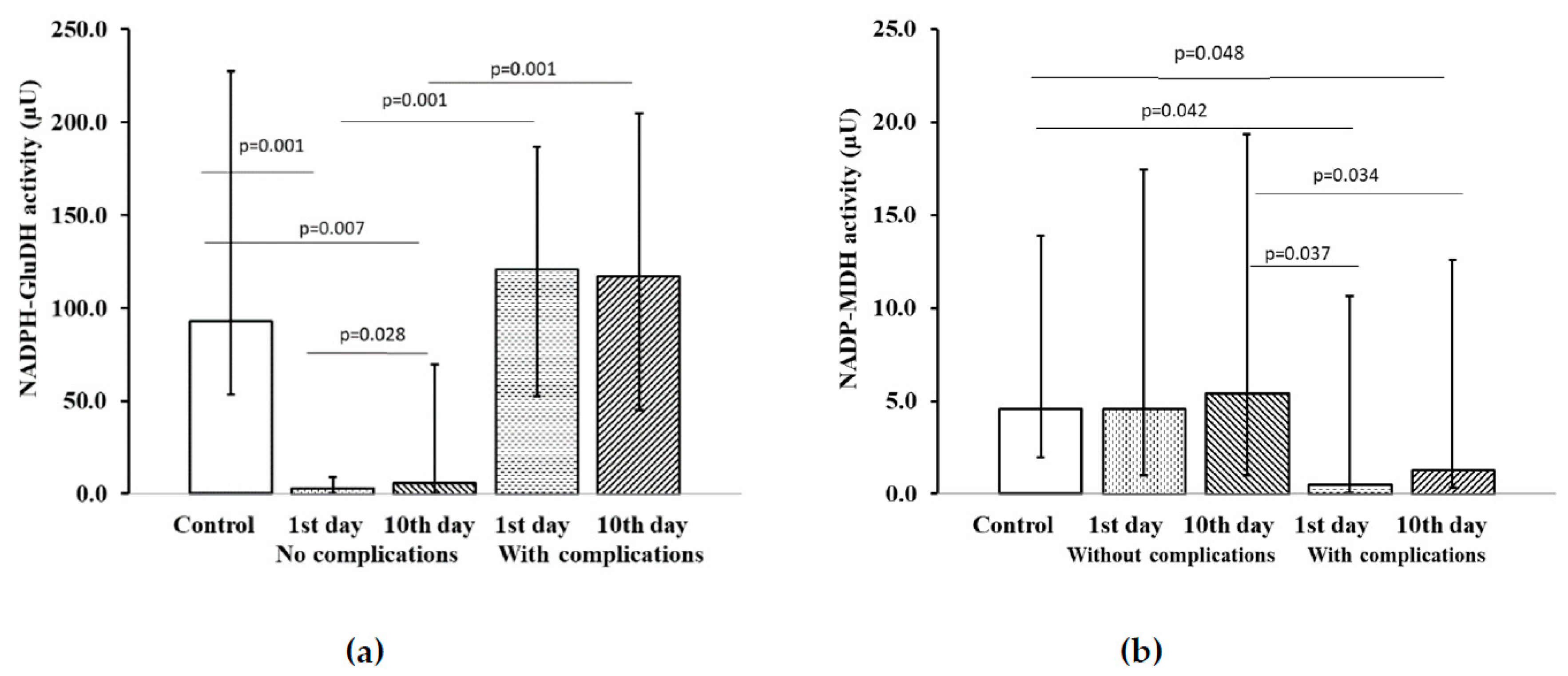
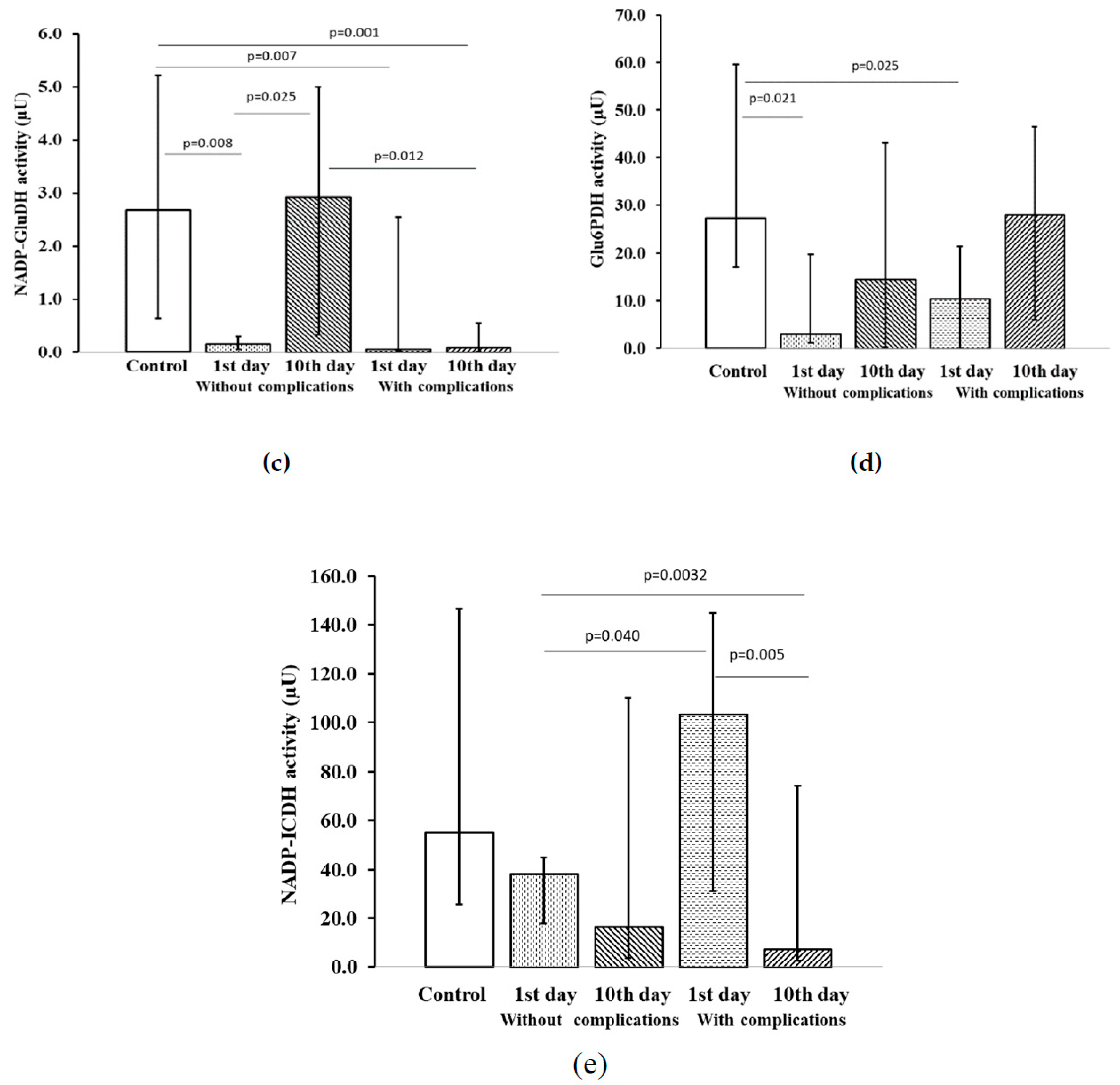
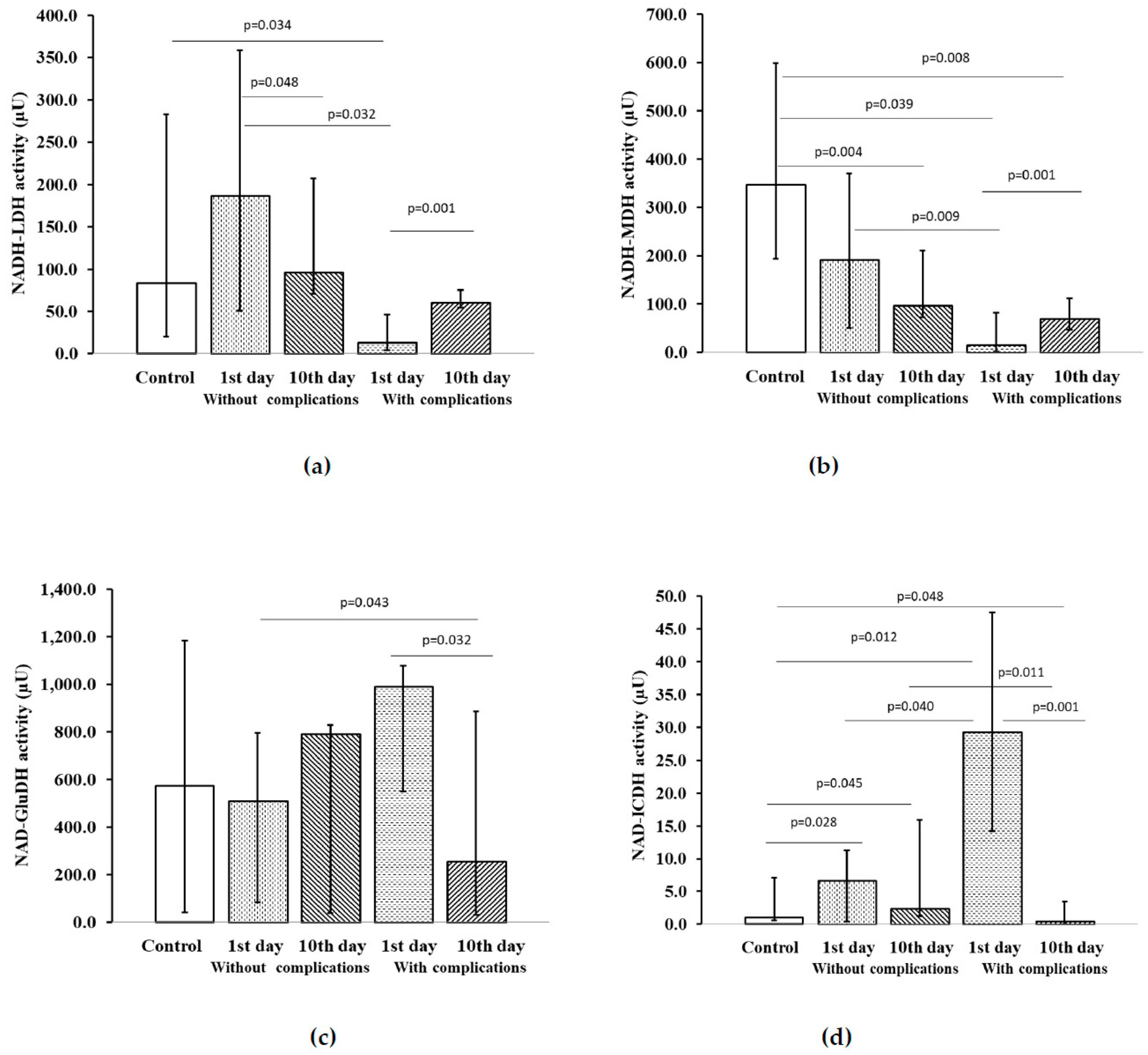
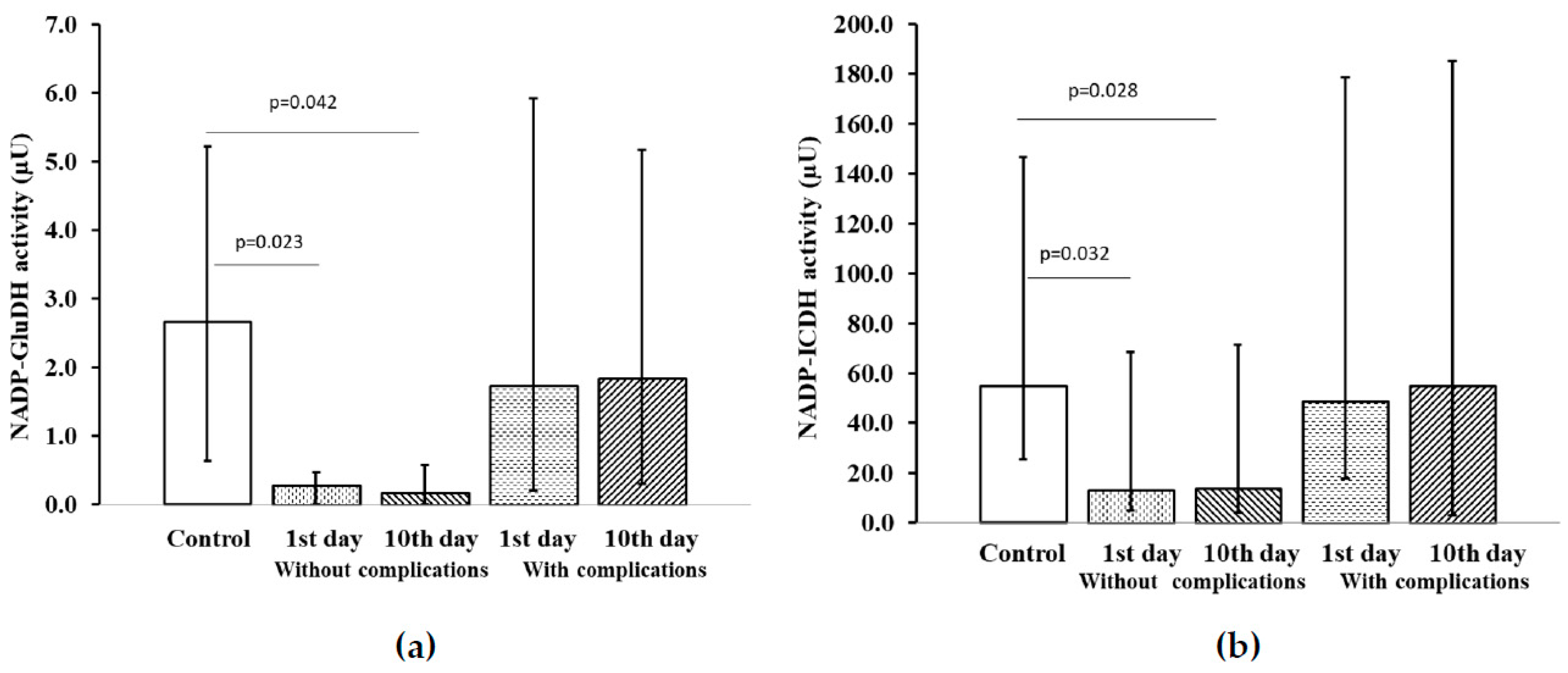
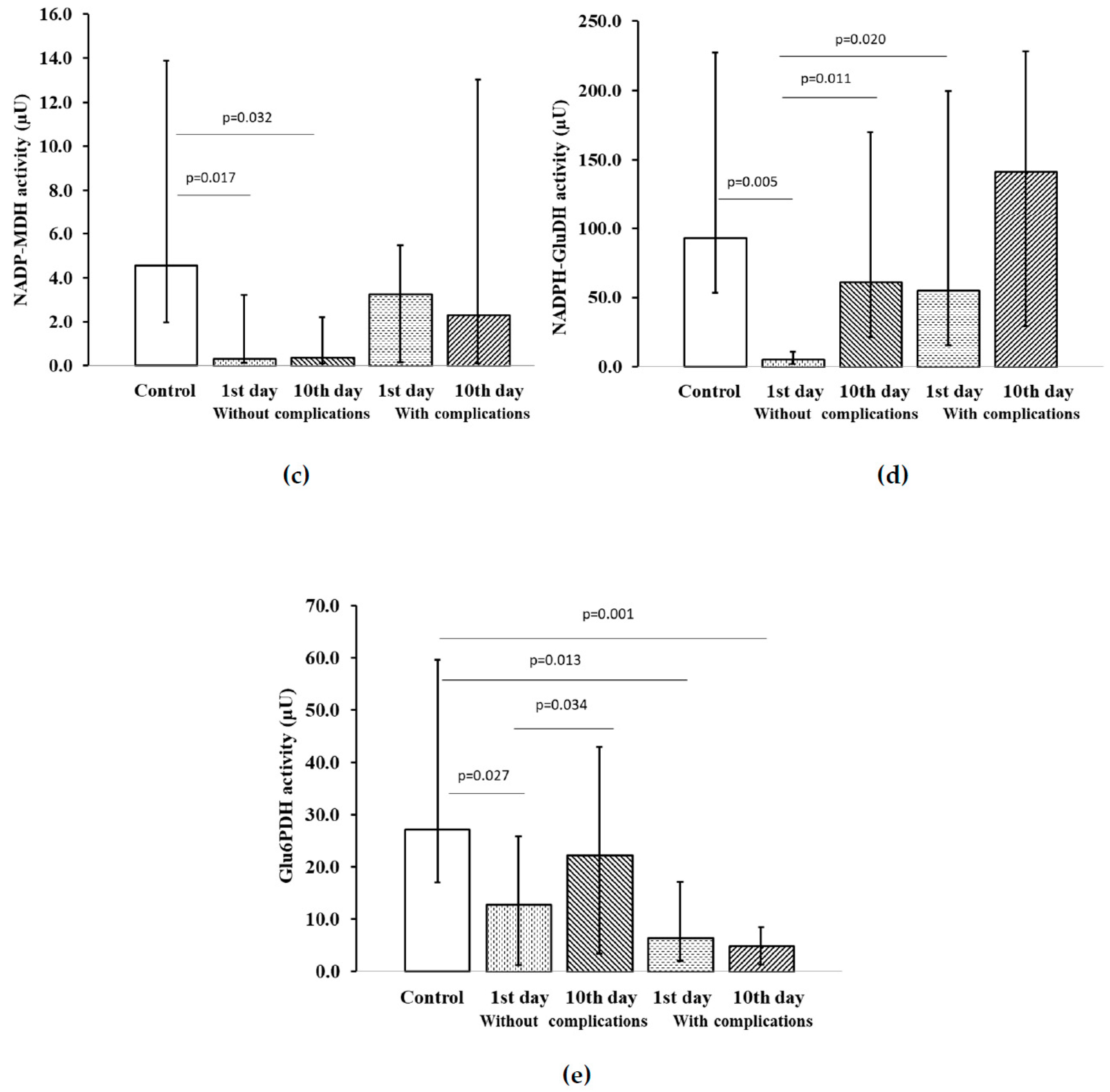
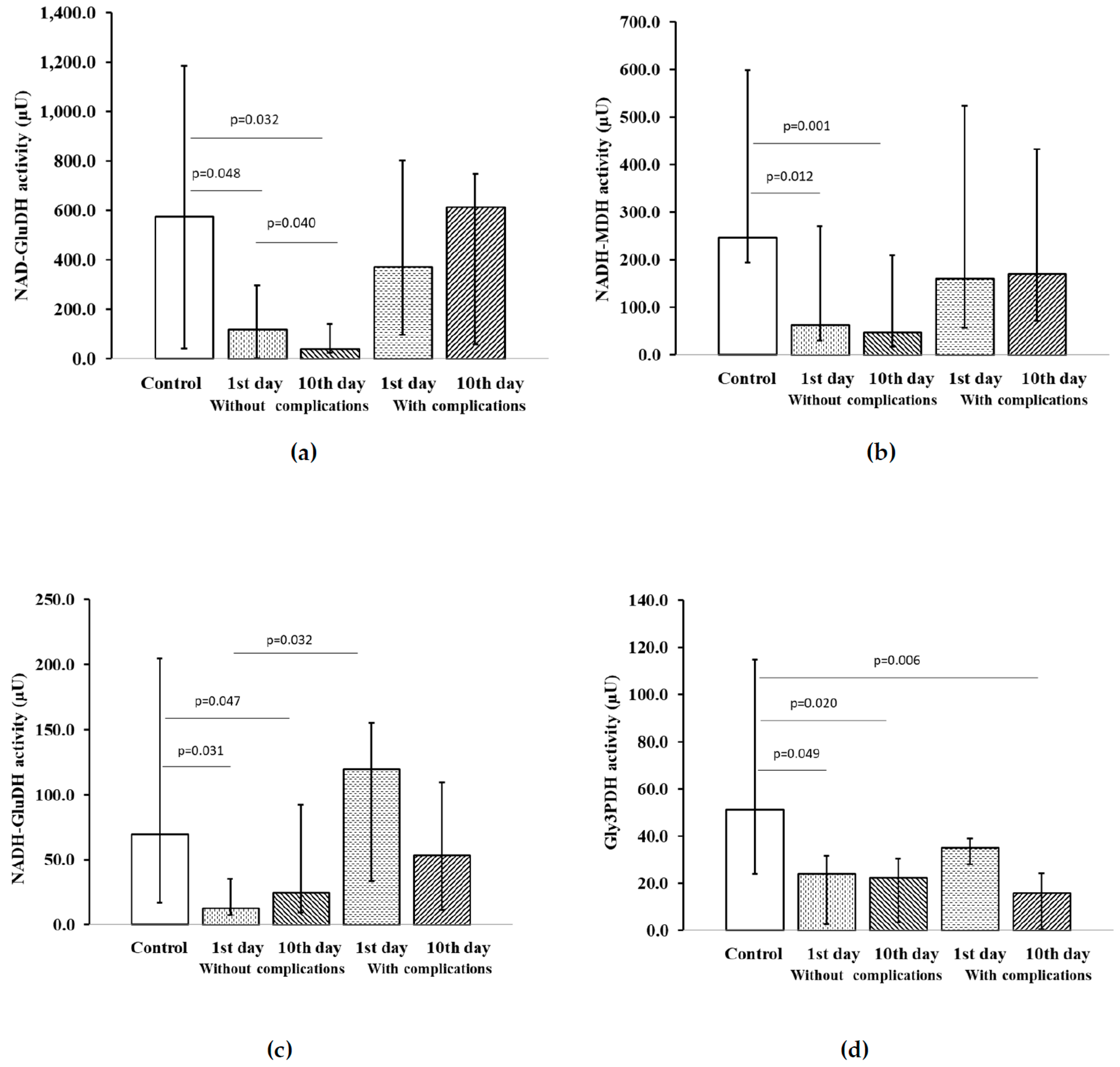
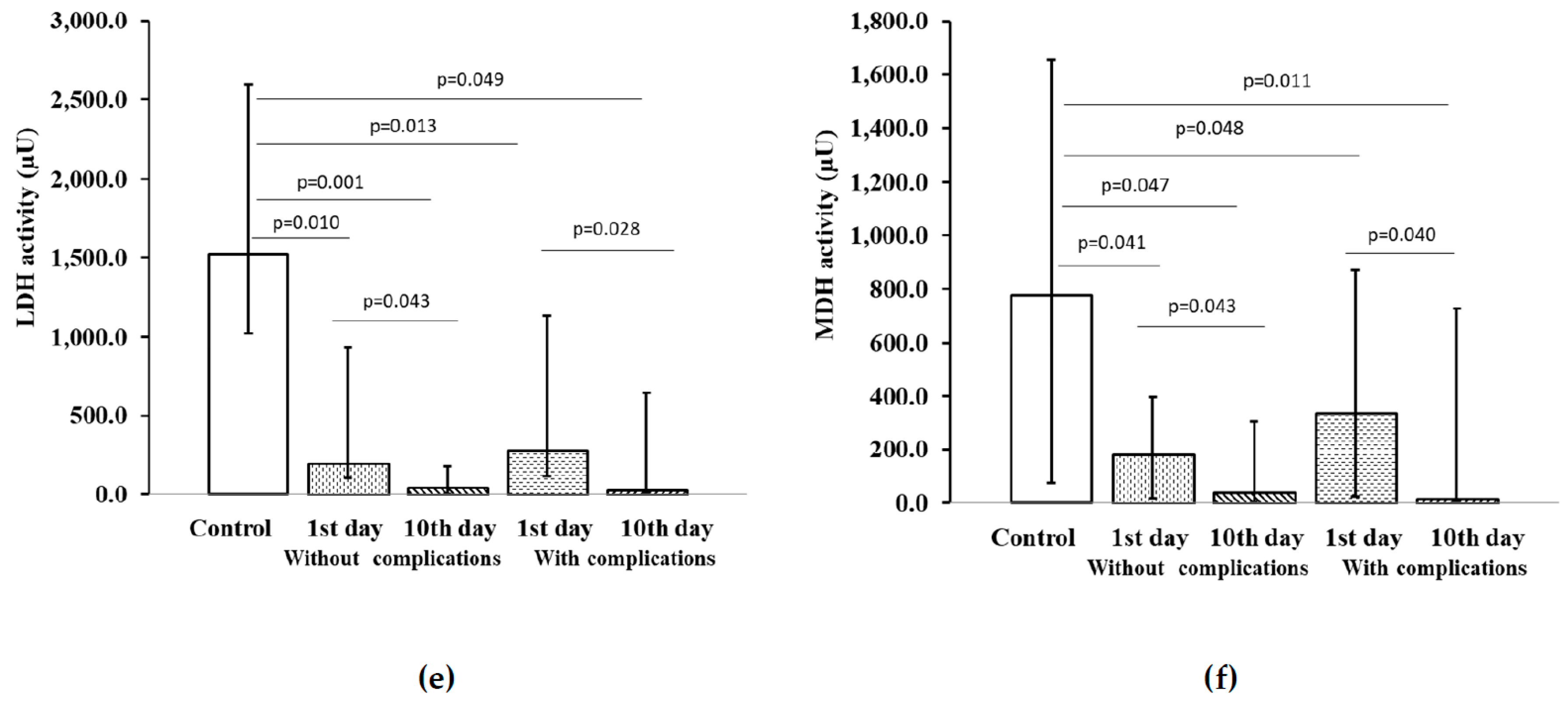
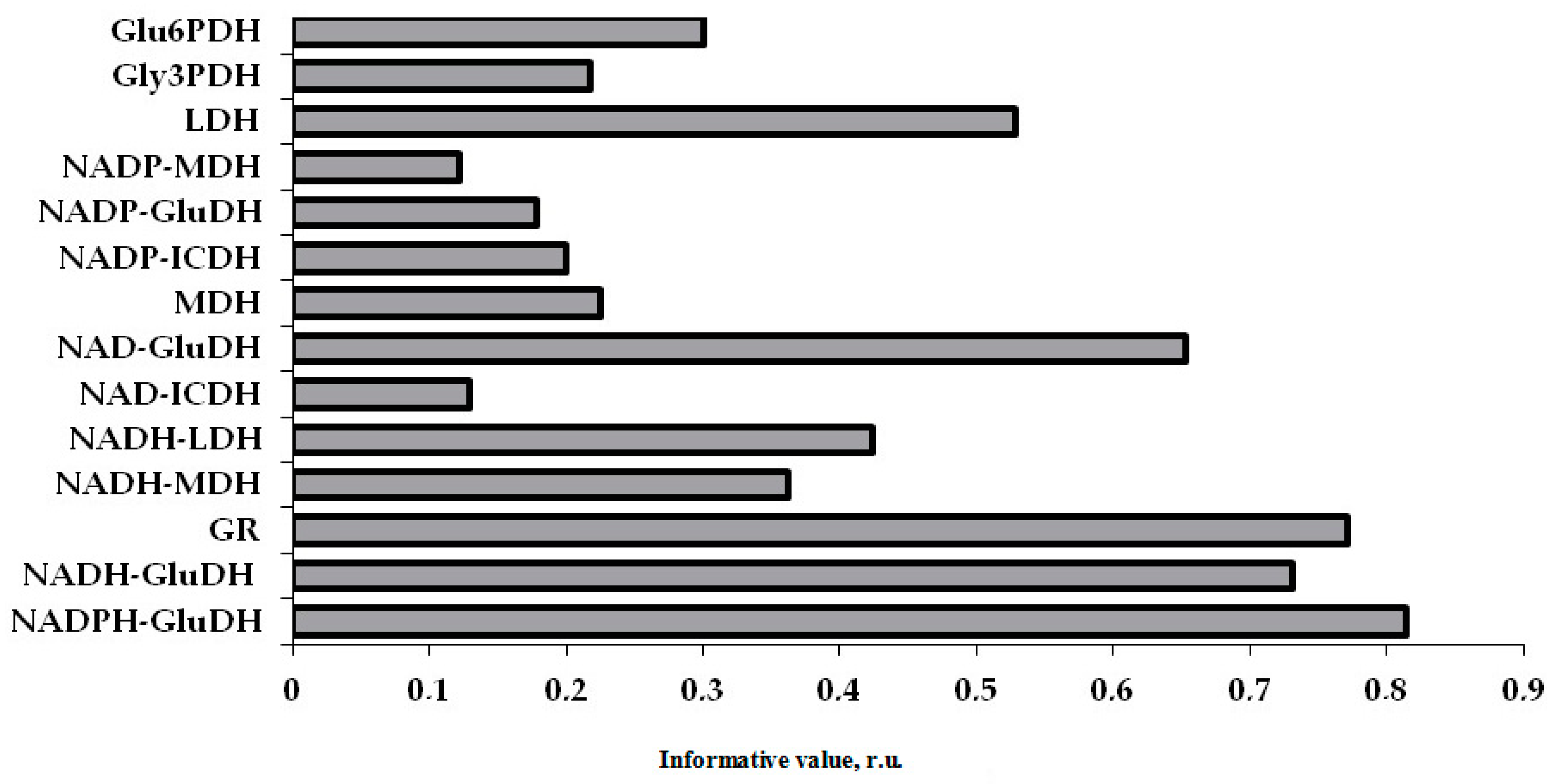
2. Results
3. Discussion
4. Materials and Methods
4.1. Participants and Procedures
4.2. Platelet Isolation
4.3. Bioluminescent Analysis
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cohen, B.E.; Edmondson, D.; Kronish, I.M. State of the Art Review: Depression, Stress, Anxiety, and Cardiovascular Disease. Am. J. Hypertens. 2015, 28, 1295–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Hert, M.; Detraux, J.; Vancampfort, D. The intriguing relationship between coronary heart disease and mental disorders. Dialogues Clin. Neurosci. 2018, 20, 31–40. [Google Scholar] [PubMed]
- Carney, R.M.; Freedland, K.E. Depression and coronary heart disease. Nat. Rev. Cardiol. 2017, 14, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Raič, M. Depression and Heart Diseases: Leading Health Problems. Psychiatr. Danub. 2017, 29, 770–777. [Google Scholar]
- Chauvet-Gelinier, J.C.; Bonin, B. Stress, anxiety and depression in heart disease patients: A major challenge for cardiac rehabilitation. Ann. Phys. Rehabil. Med. 2017, 60, 6–12. [Google Scholar] [CrossRef]
- Bremner, J.D.; Campanella, C.; Khan, Z.; Fani, N.; Kasher, N.; Evans, S.; Reiff, C.; Mishra, S.; Ladd, S.; Nye, J.A.; et al. Brain mechanisms of stress and depression in coronary artery disease. J. Psychiatr. Res. 2019, 109, 76–88. [Google Scholar] [CrossRef]
- Halaris, A. Inflammation-Associated Co-morbidity Between Depression and Cardiovascular Disease. Curr. Top. Behav. Neurosci. 2017, 31, 45–70. [Google Scholar] [CrossRef]
- Varghese, T.P.; Kumar, A.V.; Varghese, N.M.; Chand, S. Depression Related Pathophysiologies Relevant In Heart Disease: Insights Into Mechanism Based On Pharmacological Treatments. Curr. Cardiol Rev. 2020, 16, 125–131. [Google Scholar] [CrossRef]
- Tibaut, M.; Mekis, D.; Petrovic, D. Pathophysiology of Myocardial Infarction and Acute Management Strategies. Cardiovasc. Hematol. Agents Med. Chem. 2017, 14, 150–159. [Google Scholar] [CrossRef]
- Han, Y.L. De-escalation of anti-platelet therapy in patients with acute coronary syndromes undergoing percutaneous coronary intervention: A narrative review. Chin. Med. J. 2019, 132, 197–210. [Google Scholar] [CrossRef]
- Hammer, Y.; Iakobishvili, Z.; Hasdai, D.; Goldenberg, I.; Shlomo, N.; Einhorn, M.; Bental, T.; Witberg, G.; Kornowski, R.; Eisen, A. Guideline-Recommended Therapies and Clinical Outcomes According to the Risk for Recurrent Cardiovascular Events After an Acute Coronary Syndrome. J. Am. Heart Assoc. 2018, 7, e009885. [Google Scholar] [CrossRef] [Green Version]
- Rossello, X.; Bueno, H.; Pocock, S.J.; Van de Werf, F.; Danchin, N.; Annemans, L.; Medina, J.; Zeymer, U. Predictors of all-cause mortality and ischemic events within and beyond 1 year after an acute coronary syndrome: Results from the EPICOR registry. Clin. Cardiol. 2019, 42, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amadio, P.; Colombo, G.I.; Tarantino, E.; Gianellini, S.; Ieraci, A.; Brioschi, M.; Banfi, C.; Werba, J.P.; Parolari, A.; Lee, F.S.; et al. BDNFVal66met polymorphism: A potential bridge between depression and thrombosis. Eur. Heart J. 2017, 38, 1426–1435. [Google Scholar] [CrossRef] [Green Version]
- Dietrich-Muszalska, A.; Wachowicz, B. Platelet haemostatic function in psychiatric disorders: Effects of antidepressants and antipsychotic drugs. World J. Biol. Psychiatry 2017, 18, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Aibibula, M.; Naseem, K.M.; Sturmey, R.G. Glucose metabolism and metabolic flexibility in blood platelets. J. Thromb. Haemost. 2018, 16, 2300–2314. [Google Scholar] [CrossRef] [Green Version]
- Corona de la Peña, N.; Gutiérrez-Aguilar, M.; Hernández-Reséndiz, I.; Marín-Hernández, Á.; Rodríguez-Enríquez, S. Glycoprotein Ib activation by thrombin stimulates the energy metabolism in human platelets. PLoS ONE 2017, 12, e0182374. [Google Scholar] [CrossRef] [Green Version]
- Sellés Vidal, L.; Kelly, C.L.; Mordaka, P.M.; Heap, J.T. Review of NAD(P)H-dependent oxidoreductases: Properties, engineering and application. Biochim. Biophys. Acta Proteins Proteom. 2018, 1866, 327–347. [Google Scholar] [CrossRef] [PubMed]
- Holinstat, M. Normal platelet function. Cancer Metastasis Rev. 2017, 36, 195–198. [Google Scholar] [CrossRef]
- Yeung, J.; Li, W.; Holinstat, M. Platelet Signaling and Disease: Targeted Therapy for Thrombosis and Other Related Diseases. Pharmacol. Rev. 2018, 70, 526–548. [Google Scholar] [CrossRef] [Green Version]
- Grover, S.P.; Bergmeier, W.; Mackman, N. Platelet Signaling Pathways and New Inhibitors. Arterioscler. Thromb. Vasc. Biol. 2018, 38, e28–e35. [Google Scholar] [CrossRef] [Green Version]
- Khodadi, E. Platelet Function in Cardiovascular Disease: Activation of Molecules and Activation by Molecules. Cardiovasc. Toxicol. 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ossola, P.; Gerra, M.L.; De Panfilis, C.; Tonna, M.; Marchesi, C. Anxiety, depression, and cardiac outcomes after a first diagnosis of acute coronary syndrome. Health Psychol. 2018, 37, 1115–1122. [Google Scholar] [CrossRef] [Green Version]
- Xia, K.; Wang, L.F.; Yang, X.C.; Jiang, H.Y.; Zhang, L.J.; Yao, D.K.; Hu, D.Y.; Ding, R.J. Comparing the effects of depression, anxiety, and comorbidity on quality-of-life, adverse outcomes, and medical expenditure in Chinese patients with acute coronary syndrome. Chin. Med. J. 2019, 132, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Melchinger, H.; Jain, K.; Tyagi, T.; Hwa, J. Role of Platelet Mitochondria: Life in a Nucleus-Free Zone. Front. Cardiovasc. Med. 2019, 6, 153. [Google Scholar] [CrossRef] [PubMed]
- Braganza, A.; Annarapu, G.K.; Shiva, S. Blood-based bioenergetics: An emerging translational and clinical tool. Mol. Aspects Med. 2020, 71, 100835. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wu, Q.; Fan, Z.; Xie, R.; Wang, Z.; Lu, Y. Platelet mitochondrial dysfunction and the correlation with human diseases. Biochem. Soc. Trans. 2017, 45, 1213–1223. [Google Scholar] [CrossRef]
- Ravera, S.; Signorello, M.G.; Bartolucci, M.; Ferrando, S.; Manni, L.; Caicci, F.; Calzia, D.; Panfoli, I.; Morelli, A.; Leoncini, G. Extramitochondrial energy production in platelets. Biol. Cell 2018, 110, 97–108. [Google Scholar] [CrossRef]
- Paul, M.; Hemshekhar, M.; Kemparaju, K.; Girish, K.S. Aggregation is impaired in starved platelets due to enhanced autophagy and cellular energy depletion. Platelets 2019, 30, 487–497. [Google Scholar] [CrossRef]
- Yao, P.; Sun, H.; Xu, C.; Chen, T.; Zou, B.; Jiang, P.; Du, W. Evidence for a direct cross-talk between malic enzyme and the pentose phosphate pathway via structural interactions. J. Biol. Chem. 2017, 292, 17113–17120. [Google Scholar] [CrossRef] [Green Version]
- Roosterman, D.; Meyerhof, W.; Cottrell, G.S. Proton Transport Chains in Glucose Metabolism: Mind the Proton. Front. Neurosci. 2018, 12, 404. [Google Scholar] [CrossRef]
- Wang, T.; Yao, W.; Li, J.; He, Q.; Shao, Y.; Huang, F. Acetyl-CoA from inflammation-induced fatty acids oxidation promotes hepatic malate-aspartate shuttle activity and glycolysis. Am. J. Physiol. Endocrinol. Metab. 2018, 315, E496–E510. [Google Scholar] [CrossRef] [PubMed]
- Bailis, W.; Shyer, J.A.; Zhao, J.; Canaveras, J.C.G.; Al Khazal, F.J.; Qu, R.; Steach, H.R.; Bielecki, P.; Khan, O.; Jackson, R.; et al. Distinct modes of mitochondrial metabolism uncouple T cell differentiation and function. Nature 2019, 571, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.Q.; Li, C.; Stanley, C.A.; Smith, T.J. Glutamate Dehydrogenase, a Complex Enzyme at a Crucial Metabolic Branch Point. Neurochem. Res. 2019, 44, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Boukouris, A.E.; Zervopoulos, S.D.; Michelakis, E.D. Metabolic Enzymes Moonlighting in the Nucleus: Metabolic Regulation of Gene Transcription. Trends Biochem. Sci. 2016, 8, 712–730. [Google Scholar] [CrossRef]
- Ferrari, A.; Longo, R.; Silva, R.; Mitro, N.; Caruso, D.; De Fabiani, E.; Crestani, M. Epigenome modifiers and metabolic rewiring: New frontiers in therapeutics. Pharmacol. Ther. 2019, 193, 178–193. [Google Scholar] [CrossRef]
- Hino, S.; Nagaoka, K.; Nakao, M. Metabolism-epigenome crosstalk in physiology and diseases. J. Hum. Genet. 2013, 58, 410–415. [Google Scholar] [CrossRef] [Green Version]
- Kopinski, P.K.; Janssen, K.A.; Schaefer, P.M.; Trefely, S.; Perry, C.E.; Potluri, P.; Tintos-Hernandez, J.A.; Singh, L.N.; Karch, K.R.; Campbell, S.L.; et al. Regulation of nuclear epigenome by mitochondrial DNA heteroplasmy. Proc. Natl. Acad. Sci. USA 2019, 116, 16028–16035. [Google Scholar] [CrossRef] [Green Version]
- Vallerga, C.L.; Zhang, F.; Fowdar, J.; McRae, A.F.; Qi, T.; Nabais, M.F.; Zhang, Q.; Kassam, I.; Henders, A.K.; Wallace, L.; et al. Analysis of DNA methylation associates the cystine-glutamate antiporter SLC7A11 with risk of Parkinson’s disease. Nat. Commun. 2020, 11, 1238. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.X.; He, Z.; Feng, B.; Shao, H. An epigenome-wide DNA methylation study of workers with an occupational exposure to lead. J. Appl. Toxicol. 2019, 39, 1311–1319. [Google Scholar] [CrossRef]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [CrossRef]
- Chiang, J.Y.; Lee, S.H.; Chen, Y.C.; Wu, C.K.; Chuang, J.Y.; Lo, S.C.; Yeh, H.M.; Yeh, S.S.; Hsu, C.A.; Lin, B.B.; et al. Metabolomic Analysis of Platelets of Patients With Aspirin Non-Response. Front. Pharmacol. 2019, 10, 1107. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Gulati, G.; Uppal, G.; Gong, J. Assessment of the Reliability of the Sysmex XE-5000 Analyzer to Detect Platelet Clumps. Lab. Med. 2016, 47, 189–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savchenko, A.A. Evaluation of NAD(P)-dependent dehydrogenase activities in neutrophilic granulocytes by the bioluminescent method. Bull. Exp. Biol. Med. 2015, 159, 692–695. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients with ACS (1) and ADD (2) (n = 161) | Patients with ACS without ADD (n = 154) | p-Value |
|---|---|---|---|
| Age, mean ± SD | 64.2 ± 0.8 | 62 ± 1.1 | p > 0.05 ns |
| Men, n (%) | 86 (53.4) | 83 (53.9) | p > 0.05 ns |
| Women, n (%) | 75 (46.6) | 71 (46.1) | p > 0.05 ns |
| STEMI (3), n (%) | 40 (24.8) | 29 (18.8) | p > 0.05 ns |
| NSTEMI (4), n (%) | 49 (30.4) | 58 (37.7) | p > 0.05 ns |
| Unstable angina, n (%) | 72 (44.7) | 67 (43.2) | p > 0.05 ns |
| Associated conditions, n (%) | |||
| Smoking | 81 (50.3) | 75 (48.7) | p > 0.05 ns |
| Arterial hypertension | 148 (91.9) | 134 (87.0) | p > 0.05 ns |
| History of MI (5) | 46 (28.6) | 33 (21.4) | p > 0.05 ns |
| History of stroke/TIA (6) | 25 (15.5) | 20 (13.0) | p > 0.05 ns |
| History of coronary angioplasty and stenting | 22 (13.7) | 19 (12.3) | p > 0.05 ns |
| Dyslipidemia | 90 (55.9) | 83 (53.9) | p > 0.05 ns |
| Use of antiplatelet agents before hospitalization | 72 (44.7) | 63 (40.9) | p > 0.05 ns |
| Management of ACS in the hospital, n (%) | |||
| Aspirin | 156 (96.9) | 147 (95.5) | p > 0.05 ns |
| Clopidogrel | 146 (90.7) | 143 (92.9) | p > 0.05 ns |
| Ticagrelor | 16 (9.9) | 17 (11.0) | p > 0.05 ns |
| Enoxaparin | 143 (88.9) | 134 (87.0) | p > 0.05 ns |
| Fondaparinux | 9 (5.6) | 11 (7.1) | p > 0.05 ns |
| Unfractionated heparin | 9 (5.6) | 9 (5.8) | p > 0.05 ns |
| PCI (7) with stenting | 115 (71.4) | 114 (74.0) | p > 0.05 ns |
| Antiplatelet agents after 12 months of follow-up, n (%) | |||
| Aspirin | 126 (78.2) | 132 (85.7) | p > 0.05 ns |
| Clopidogrel | 90 (55.9) | 89 (57.8) | p > 0.05 ns |
| Ticagrelor | 7 (4.3) | 6 (3.9) | p > 0.05 ns |
| Cardiovascular complications, n (%) | |||
| Relapse AMI (8) | 5 (3.1) | 3 (1.9) | p > 0.05 ns |
| Repeated AMI | 5 (3.1) | 2 (1.3) | p > 0.05 ns |
| Stroke | 4 (2.5) | 3 (1.9) | p > 0.05 ns |
| Post-infarction angina | 9 (5.6) | 5 (3.2) | p > 0.05 ns |
| Heart failure progression | 5 (3.1) | 3 (1.9) | p > 0.05 ns |
| Thromboembolism | 4 (2.5) | 1 (0.6) | p > 0.05 ns |
| Postinfarction left ventricular aneurysm | 4 (2.5) | 2 (1.3) | p > 0.05 ns |
| Fatal outcome | 5 (3.1) | 1 (0.6) | p > 0.05 ns |
| Total complications | 41 (25.5) | 20 (13.0) | p > 0.05 ns |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimokhina, N.Y.; Savchenko, A.A.; Petrova, M.M. Peculiarities of Platelet Metabolism in Patients with Acute Coronary Syndrome with Anxiety–Depressive Disorders and Informativity of Enzymes in the Forecast of Development of Cardiovascular Complications. Pharmaceuticals 2020, 13, 169. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080169
Shimokhina NY, Savchenko AA, Petrova MM. Peculiarities of Platelet Metabolism in Patients with Acute Coronary Syndrome with Anxiety–Depressive Disorders and Informativity of Enzymes in the Forecast of Development of Cardiovascular Complications. Pharmaceuticals. 2020; 13(8):169. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080169
Chicago/Turabian StyleShimokhina, Natalya Yu., Andrey A. Savchenko, and Marina M. Petrova. 2020. "Peculiarities of Platelet Metabolism in Patients with Acute Coronary Syndrome with Anxiety–Depressive Disorders and Informativity of Enzymes in the Forecast of Development of Cardiovascular Complications" Pharmaceuticals 13, no. 8: 169. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13080169