
Rare Clinical Association between Clostridioides difficile Infection and Ischemic Colitis: Case Report and Literature Review

Abstract
:1. Introduction
2. Case Report
3. Discussions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ley, R.E.; Peterson, D.A.; Gordon, J.I. Ecological and evolutionary forces shaping microbial diversity in the human intestine. Cell 2006, 124, 837–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falony, G.; Vlachou, A.; Verbrugghe, K.; De Vuyst, L. Cross-feeding between Bifidobacterium longum BB536 and acetate-converting, butyrate-producing colon bacteria during growth on oligofructose. Appl. Environ. Microbiol. 2006, 72, 7835–7841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, J.; Lee, S.M.; Shen, Y.; Khosravi, A.; Mazmanian, S.K. Host-bacterial symbiosis in health and disease. In Advances in Immunology; Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar] [CrossRef] [Green Version]
- Banaei, N.; Anikst, V.; Schroeder, L.F. Burden of Clostridium difficile infection in the United States. N. Engl. J. Med. 2015, 372, 2368–2369. [Google Scholar] [CrossRef] [PubMed]
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile Infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McFarland, L.V.; Beneda, H.W.; Clarridge, J.E.; Raugi, G.J. Implications of the changing face of Clostridium difficile disease for health care practitioners. Am. J. Infect. Control 2007, 35, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Bishara, J.; Farah, R.; Mograbi, J.; Khalaila, W.; Abu-Elheja, O.; Mahamid, M.; Nseir, W. Obesity as a Risk Factor for Clostridium difficile Infection. Clin. Infect. Dis. 2013, 57, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Leung, J.; Burke, B.; Ford, D.; Garvin, G.; Korn, C.; Sulis, C.; Bhadetlia, N. Possible association between obesity and Clostridium difficile infection. Emerg. Infect. Dis. 2013, 19, 1791–1796. [Google Scholar] [CrossRef]
- Furuya-Kanamori, L.; Stone, J.C.; Clark, J.; McKenzie, S.J.; Yakob, L.; Paterson, D.; Riley, T.V.; Doi, S.; Clements, A.C. Comorbidities, exposure to medications, and the risk of community-acquired clostridium difficile infection: A systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2015, 36, 132–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Permpalung, N.; Upala, S.; Sanguankeo, A.; Sornprom, S. Association between NSAIDs and clostridium difficile -associated diarrhea: A systematic review and meta-analysis. Can. J. Gastroenterol. Hepatol. 2016, 2016, 7431838. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.K.; Sferra, T.J.; Hernandez, A.V.; Donskey, C.J. Community-associated Clostridium difficile infection and antibiotics: A meta-analysis. J. Antimicrob. Chemother. 2013, 68, 1951–1961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz, C.; Abujudeh, H.H.; Nazarian, R.M.; Thrall, J.H. Ischemic colitis: Spectrum of CT findings, sites of involvement and severity. Emerg. Radiol. 2015, 22, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Yngvadottir, Y.; Karlsdottir, B.R.; Hreinsson, J.P.; Ragnarsson, G.; Mitetv, R.U.M.; Jonasson, J.G.; Möller, P.H.; Björnsson, E.S. The incidence and outcome of ischemic colitis in a population-based setting. Scand. J. Gastroenterol. 2017, 52, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Montoro, M.A.; Brandt, L.J.; Santolaria, S.; Gomollon, F.; Puértolas, B.S.; Vera, J.; Bujanda, L.; Cosme, A.; Cabriada, J.L.; Durán, M.; et al. Clinical patterns and outcomes of ischaemic colitis: Results of the Working Group for the Study of Ischaemic Colitis in Spain (CIE study). Scand. J. Gastroenterol. 2011, 46, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Shinji, A.; Horiuchi, A.; Tanaka, N.; Nagaya, T.; Shigeno, T.; Nakamura, N.; Komatsu, M.; Umemura, T.; Arakura, N.; et al. Clinical characteristics of Young-Onset ischemic colitis. Dig. Dis. Sci. 2012, 57, 1652–1659. [Google Scholar] [CrossRef]
- Park, C.J.; Jang, M.K.; Shin, W.G.; Kim, H.S.; Kim, H.S.; Lee, K.S.; Lee, J.Y.; Kim, K.H.; Park, J.Y.; Lee, J.H.; et al. Can we predict the development of ischemic colitis among patients with lower abdominal pain? Dis. Colon Rectum. 2007, 50, 232–238. [Google Scholar] [CrossRef]
- Longstreth, G.F.; Yao, J.F. Epidemiology, Clinical Features, High-Risk Factors, and Outcome of Acute Large Bowel Ischemia. Clin. Gastroenterol. Hepatol. 2009, 7, 1075–1080. [Google Scholar] [CrossRef]
- Valle Gottlieb, M.G.; Closs, V.E.; Junges, V.M.; Schwanke, C.H.A. Impact of human aging and modern lifestyle on gut microbiota. Crit. Rev. Food Sci. Nutr. 2018, 58, 1557–1564. [Google Scholar] [CrossRef]
- Jernberg, C.; Löfmark, S.; Edlund, C.; Jansson, J.K. Long-term impacts of antibiotic exposure on the human intestinal microbiota. Microbiology 2010, 156, 3216–3223. [Google Scholar] [CrossRef] [Green Version]
- Brandt, L.; Boley, S.; Goldberg, L.; Mitsudo, S.; Berman, A. Colitis in the Elderly: A Reappraisal. Am. J. Gastroenterol. 1981, 76, 239–245. [Google Scholar] [CrossRef]
- Brandt, L.J.; Feuerstadt, P.; Blaszka, M.C. Anatomic patterns, patient characteristics, and clinical outcomes in ischemic colitis: A study of 313 cases supported by histology. Am. J. Gastroenterol. 2010, 105, 2245–2252. [Google Scholar] [CrossRef]
- Gewertz, B.L.; Ottinger, L.W.; Rogers, A.L. American gastroenterological association medical position statement: Guidelines on intestinal ischemia. Gastroenterology 2000, 118, 951–953. [Google Scholar] [CrossRef]
- Hefaiedh, R.; Sabbah, M.; Ennaifer, R.; Hyafa, R.; Attaoui, A.; Bel Hadj, N.; Lassad, G.; Mohamed, T.K. Ischemic colitis in five points: An update 2013. Tunis. Med 2014, 95, 299–303. [Google Scholar]
- Deardorff, D.L. Osmotic strength, osmolality, and osmolarity. Am. J. Hosp. Pharm. 1980, 37, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.R.; Cote, T.R.; Lawhorne, L.; Levenson, S.A.; Rubenstein, L.; Smith, D.A.; Stefanacci, R.G.; Tangalos, E.G.; Morley, J.E. Understanding Clinical Dehydration and Its Treatment. J. Am. Med. Dir. Assoc. 2008, 9, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Lucas, W.; Schroy, P.C. Reversible ischemic colitis in a high endurance athlete. Am. J. Gastroenterol. 1998, 93, 2231–2234. [Google Scholar] [CrossRef]
- Fiddian-Green, R.; Dial, S. Clostridium difficile colitis: A marker for ischemic colitis? CMAJ 2004, 171, 1325–1327. [Google Scholar] [CrossRef] [Green Version]
- Dial, S.; Alrasadi, K.; Manoukin, C.; Huang, A.; Menzies, D. Risk of Clostridium difficile diaarhea among hospital inpatients prescribed proton pump inhibitors: Cohort and case-control studies. CMAJ 2004, 171, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Dallal, R.M.; Harbrecht, B.G.; Boujoukas, A.J.; Sirio, C.A.; Farkas, L.M.; Lete, K.K.; Simmons, R.L. Fulminant Clostridium difficile: An underappreciated and increasing cause of death and complications. Ann. Surg. 2002, 235, 363–372. [Google Scholar] [CrossRef]
- Okada, M.; Iwashita, A.; Yanai, J.; Oh, K.; Hoshiko, K.; Seo, M. A Case Report of Clostridium D-l Toxin Positive Colitis with Ischemic Changes after Antibiotic Treatment. Dig. Endosc. 1997, 9, 136–140. [Google Scholar] [CrossRef]
- Veroux, M.; Puzzo, L.; Corona, D.; Buffonet, A.; Tallarita, T.; Murabito, P.; Veroux, P. Cytomegalovirus and Clostridium difficile ischemic colitis in a renal transplant recipient: A lethal complication of anti-rejection therapy? Urol. Int. 2007, 79, 177–179. [Google Scholar] [CrossRef]
- Wadhwa, V.; Alomari, M.; Shah, B.; Shen, B. Ischemic Colitis Is a Risk Factor for Clostridium difficile. Infection: 200. Off. J. Am. Coll. Gastroenterol. 2017, 112. [Google Scholar] [CrossRef]
- Negrón, M.E.; Rezaie, A.; Barkema, H.W.; Rioux, K.; De Buck, J.; Checkley, S.; Beck, P.L.; Carroll, M.; Fedorak, R.; Dieleman, L.; et al. Ulcerative colitis patients with clostridium difficile are at increased risk of death, colectomy, and postoperative complications: A population-based inception cohort study. Am. J. Gastroenterol. 2016, 111, 691–704. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Gender and Age (Years) | Symptoms | Stool Study Results | Presumed Etiology | Endoscopy Findings | Histology Findings | Treatment and Outcome |
|---|---|---|---|---|---|---|---|
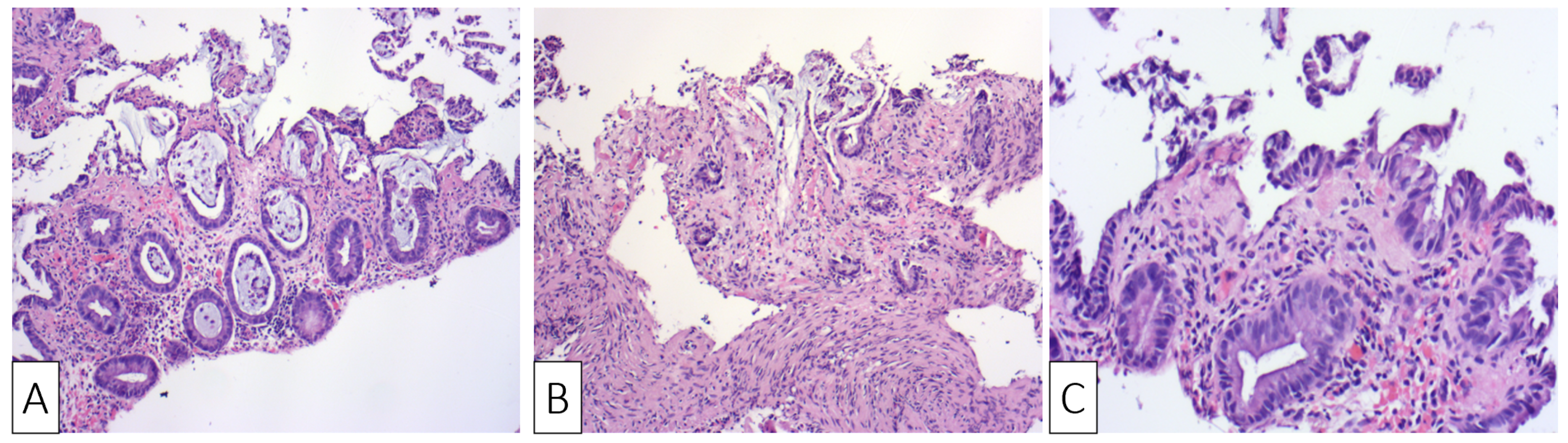
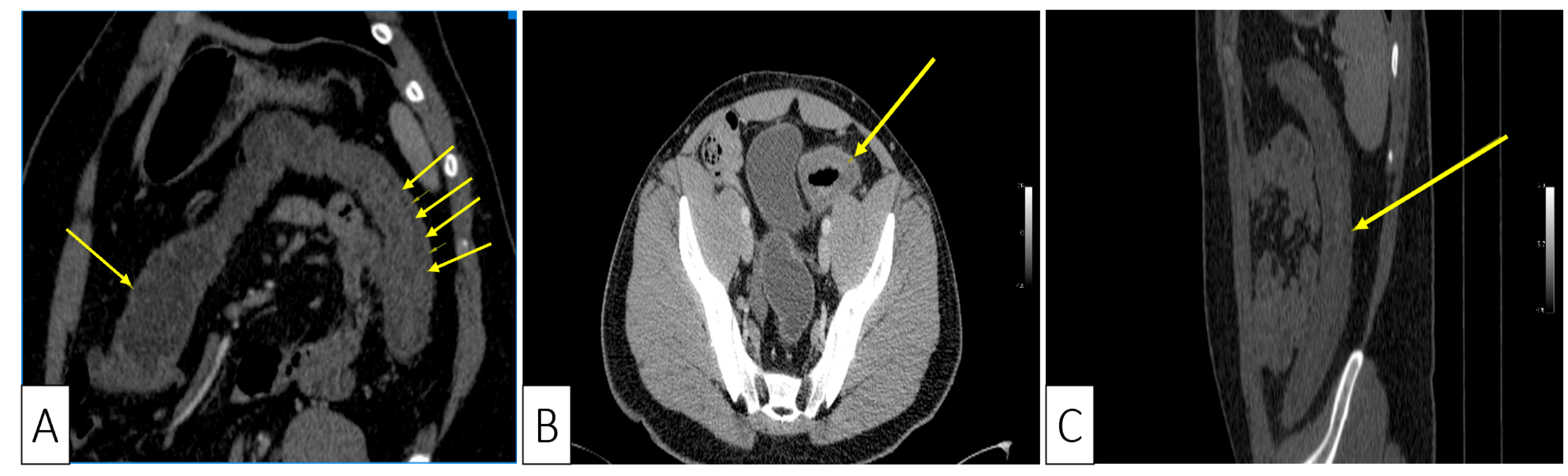
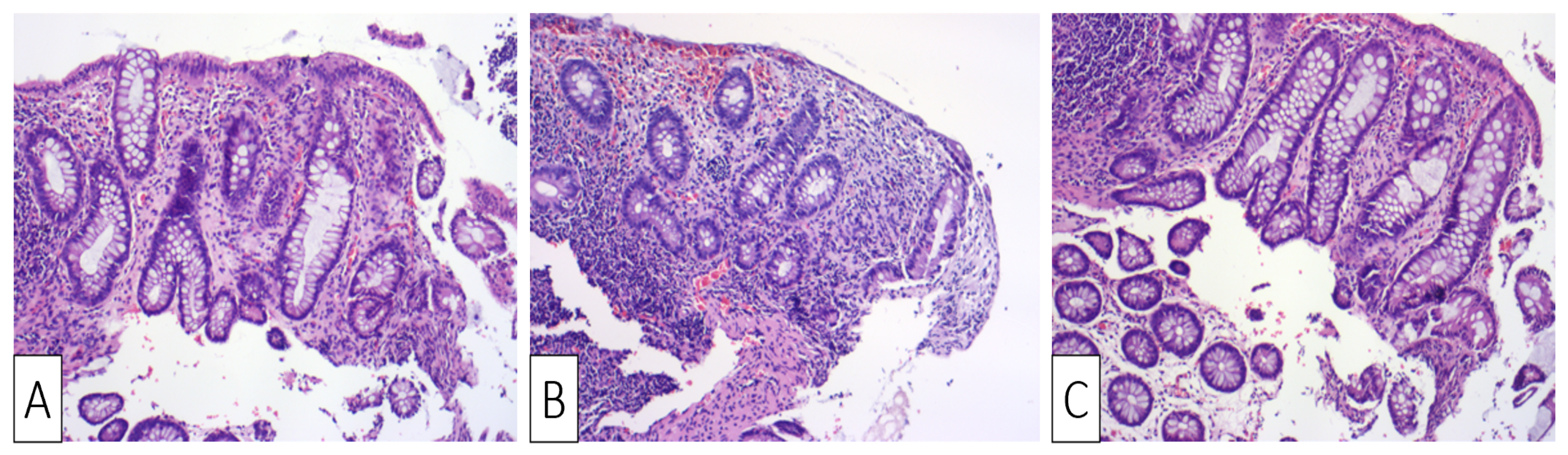
| Our patient | Male, 30 | Colicky left lower quadrant abdominal pain and bloody diarrhea | Negative fecal culture, positive toxins A, B, and GDH | Idiopathic | Several superficial longitudinal ulcerations with luminal narrowing spanning from sigmoid to the descending colon | Desquamation of superficial epithelium with focal necrosis, loss of superficial glands, edematous and necrotic lamina propria | Oral Vancomycin, symptoms resolved within two days of hospitalization |
| Okada et al., 1997 [30] | Male, 52 | Crampy lower abdominal pain followed by bloody diarrhea | Positive fecal culture and strongly positive D-1 toxin | Three-day use of Cefteram for gingivitis | Edematous mucosa with multiple longitudinal shallow ulcers, erosions, and luminal narrowing | Desquamation of superficial epithelium with crypt degeneration, fibrinous exudates in lamina propria, and mild neutrophilic infiltration | Supportive treatment, symptoms resolved by third day of hospitalization |
| Veroux et al., 2007 [31] | Female, 42 | High fever, diffuse abdominal pain with tenderness and bloody diarrhea | Positive toxins | Two weeks after renal transplant; CDI colitis was complicated by CMV colitis | Edematous mucosa with patchy erythema and longitudinal ulceration | Mucosal inflammation, hemorrhage, with leukocytoclastic vasculitis and lymphoplasmacytic perivascular infiltrate | Metronidazole and oral Vancomycin for seven days with no improvement; patient underwent subtotal colectomy but passed away two weeks later |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionescu, E.M.; Curte, A.-M.; Olteanu, A.O.; Preda, C.M.; Tieranu, I.; Klimko, A.; Tieranu, C.G. Rare Clinical Association between Clostridioides difficile Infection and Ischemic Colitis: Case Report and Literature Review. Medicina 2021, 57, 705. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070705
Ionescu EM, Curte A-M, Olteanu AO, Preda CM, Tieranu I, Klimko A, Tieranu CG. Rare Clinical Association between Clostridioides difficile Infection and Ischemic Colitis: Case Report and Literature Review. Medicina. 2021; 57(7):705. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070705
Chicago/Turabian StyleIonescu, Elena Mirela, Ana-Maria Curte, Andrei Ovidiu Olteanu, Carmen Monica Preda, Ioana Tieranu, Artsiom Klimko, and Cristian George Tieranu. 2021. "Rare Clinical Association between Clostridioides difficile Infection and Ischemic Colitis: Case Report and Literature Review" Medicina 57, no. 7: 705. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070705