Media Exposure and General Trust as Predictors of Post-traumatic Stress Disorder: Ten Years after the 5.12 Wenchuan Earthquake in China


Abstract
:1. Introduction
2. Materials and Methods
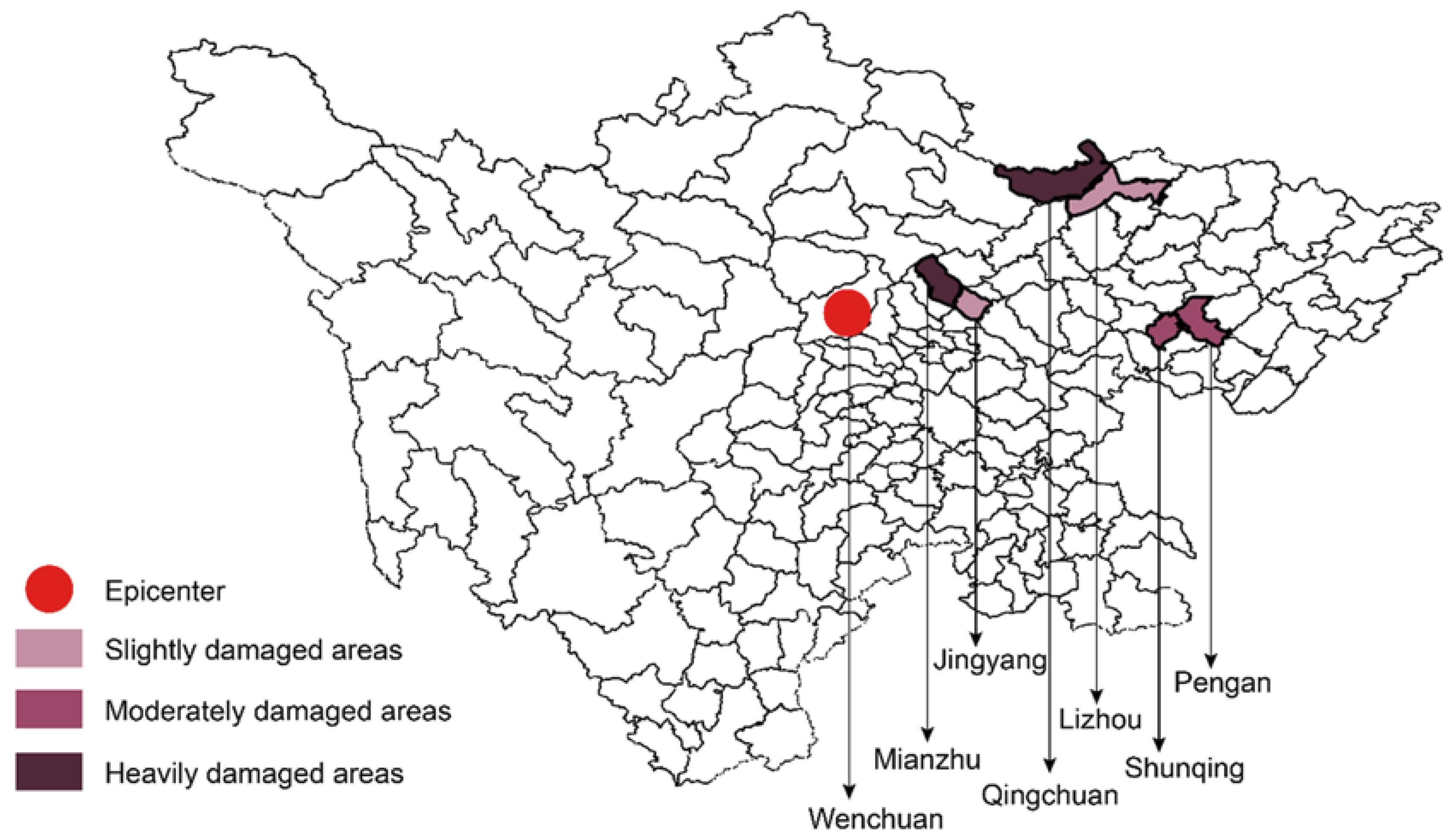
2.1. Sampling Procedures
2.2. Measures
2.2.1. PTSD Symptoms
2.2.2. Media Exposure
2.2.3. General Trust
2.2.4. Control Variables
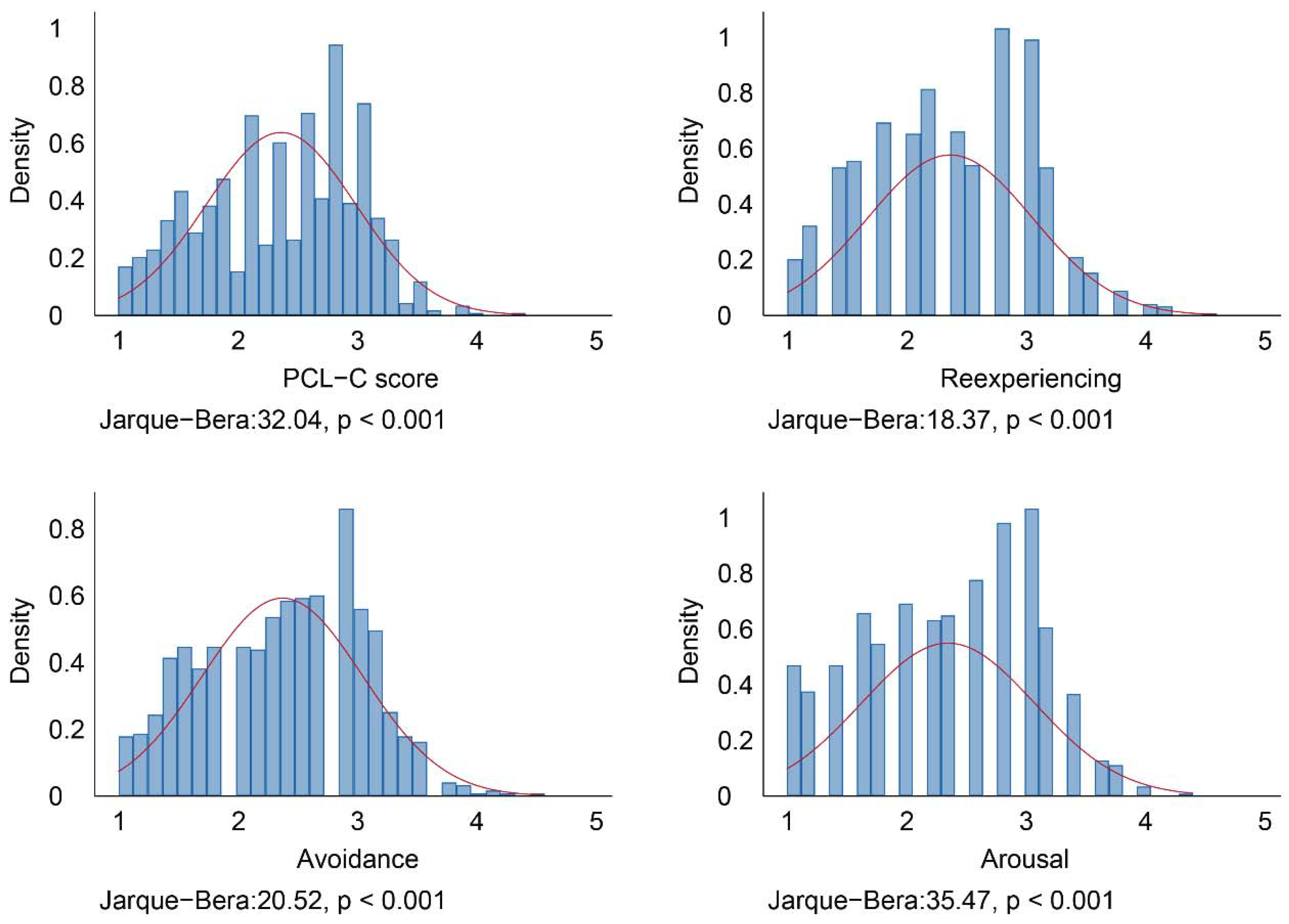
2.3. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Main Effects
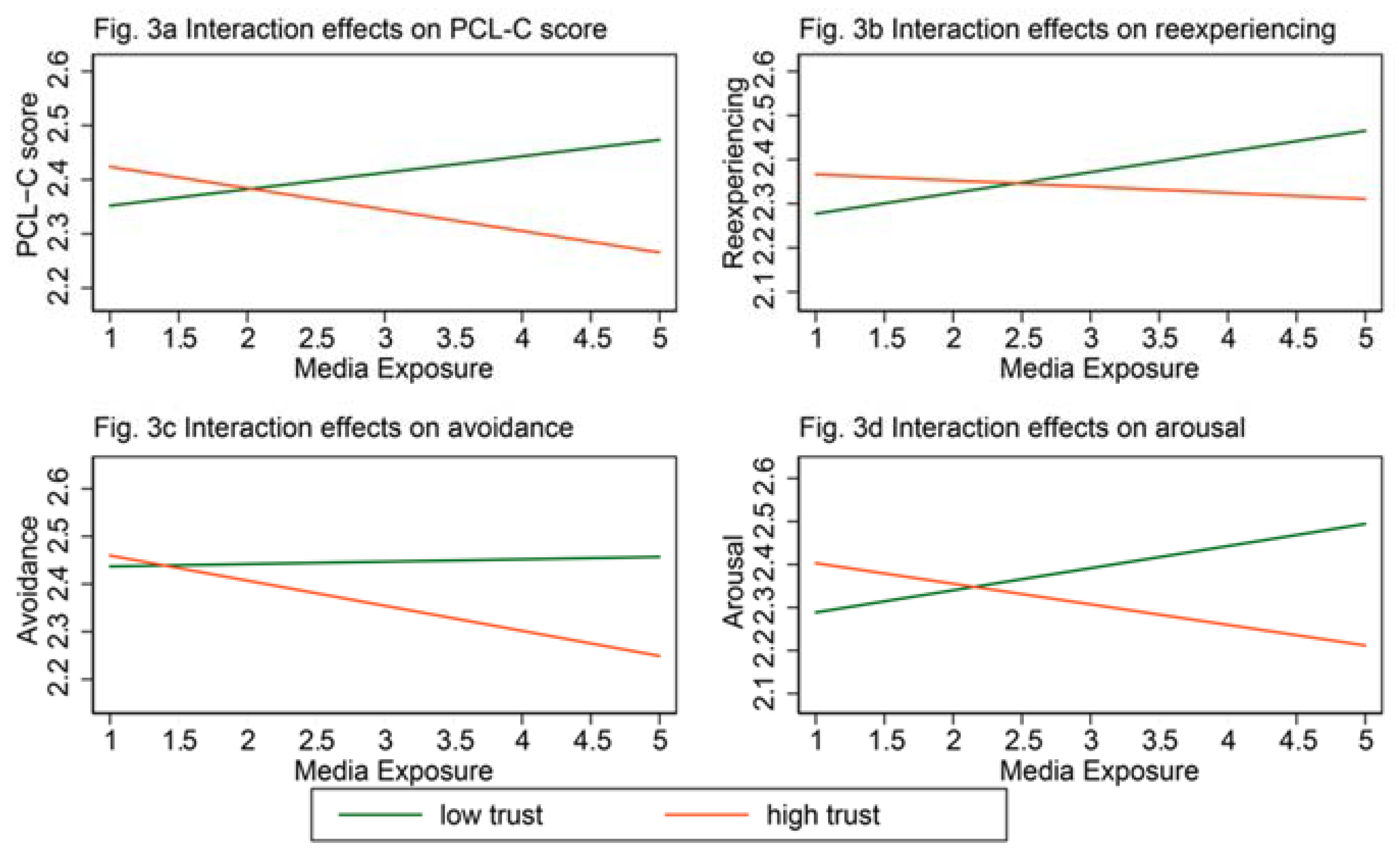
3.3. Interaction Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 |
|---|---|---|---|---|---|---|---|---|
| Low Trust | High Trust | |||||||
| PCL-C Score | Reexperiencing | Avoidance | Arousal | PCL-C Score | Reexperiencing | Avoidance | Arousal | |
| Independent variables | ||||||||
| Media exposure | 0.04 | 0.07 * | 0.02 | 0.06 + | −0.05 + | −0.03 | −0.06 * | −0.06 |
| (0.03) | (0.03) | (0.03) | (0.03) | (0.03) | (0.03) | (0.03) | (0.03) | |
| Demographic and socioeconomic variables | ||||||||
| Male | −0.00 | 0.02 | 0.01 | −0.04 | 0.08 | 0.13 * | 0.03 | 0.11 + |
| (0.06) | (0.06) | (0.06) | (0.06) | (0.05) | (0.06) | (0.06) | (0.06) | |
| Age | 0.01 * | 0.01 + | 0.01 + | 0.01 ** | 0.01 * | 0.01 | 0.01 * | 0.01 + |
| (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | |
| Rural site | 0.10 | 0.10 | 0.06 | 0.15 + | 0.05 | 0.05 | 0.05 | 0.03 |
| (0.06) | (0.07) | (0.07) | (0.07) | (0.06) | (0.07) | (0.06) | (0.07) | |
| Married | −0.11 | −0.17 * | −0.09 | −0.09 | −0.01 | −0.09 | 0.05 | −0.02 |
| (0.07) | (0.08) | (0.08) | (0.08) | (0.07) | (0.08) | (0.07) | (0.09) | |
| Educational background (0 = primary school and below) | ||||||||
| Junior high school | 0.14 | 0.06 | 0.12 | 0.24 * | 0.09 | 0.13 | 0.07 | 0.10 |
| (0.10) | (0.11) | (0.11) | (0.11) | (0.09) | (0.10) | (0.10) | (0.11) | |
| Senior high school | 0.31 ** | 0.22 + | 0.29 * | 0.44 *** | 0.13 | 0.16 | 0.13 | 0.11 |
| (0.11) | (0.13) | (0.13) | (0.13) | (0.10) | (0.12) | (0.11) | (0.13) | |
| Associate college and above | 0.57 *** | 0.36 * | 0.56 *** | 0.80 *** | 0.19 | 0.20 | 0.21 | 0.19 |
| (0.13) | (0.15) | (0.15) | (0.15) | (0.12) | (0.14) | (0.13) | (0.15) | |
| Annual household income (0 = less than 40,000 RMB) | ||||||||
| 40,000–59,999 RMB | −0.15 + | −0.14 | −0.21 * | −0.08 | −0.02 | −0.02 | 0.02 | −0.06 |
| (0.08) | (0.09) | (0.09) | (0.09) | (0.08) | (0.09) | (0.08) | (0.10) | |
| 60,000–89,999 RMB | −0.31 *** | −0.39 *** | −0.34 *** | −0.20 * | −0.07 | −0.03 | −0.04 | −0.19 + |
| (0.08) | (0.10) | (0.10) | (0.10) | (0.09) | (0.10) | (0.09) | (0.11) | |
| 90,000 RMB and above | −0.10 | −0.08 | −0.16 | −0.00 | 0.01 | 0.11 | −0.01 | −0.07 |
| (0.10) | (0.12) | (0.11) | (0.12) | (0.09) | (0.11) | (0.10) | (0.12) | |
| Earthquake exposure | ||||||||
| Being buried | 0.08 | −0.04 | 0.12 | 0.15 | 0.02 | −0.03 | −0.01 | 0.14 |
| (0.15) | (0.17) | (0.17) | (0.18) | (0.20) | (0.23) | (0.22) | (0.25) | |
| Being injured | −0.16 * | −0.16 + | −0.17 * | −0.14 | −0.10 | −0.01 | −0.09 | −0.21 * |
| (0.08) | (0.09) | (0.09) | (0.09) | (0.08) | (0.09) | (0.09) | (0.10) | |
| Being disabled | 0.03 | −0.07 | 0.12 | −0.02 | 0.58 | 0.56 | 0.77 + | 0.31 |
| (0.15) | (0.17) | (0.17) | (0.17) | (0.42) | (0.48) | (0.46) | (0.52) | |
| Family died | 0.17 | 0.10 | 0.15 | 0.26 + | −0.05 | −0.02 | 0.02 | −0.23 |
| (0.12) | (0.13) | (0.13) | (0.14) | (0.13) | (0.15) | (0.14) | (0.16) | |
| Family injured | 0.19 * | 0.30 *** | 0.11 | 0.19 * | 0.08 | 0.11 | 0.01 | 0.15 |
| (0.07) | (0.08) | (0.08) | (0.09) | (0.08) | (0.09) | (0.09) | (0.10) | |
| Family disabled | −0.04 | −0.09 | −0.02 | −0.01 | −0.19 + | −0.23 + | −0.14 | −0.25 + |
| (0.12) | (0.14) | (0.14) | (0.14) | (0.11) | (0.13) | (0.12) | (0.14) | |
| Kinsfolk died | −0.06 | −0.02 | −0.05 | −0.13 | −0.23 ** | −0.20 * | −0.20 * | −0.32 ** |
| (0.08) | (0.09) | (0.09) | (0.09) | (0.08) | (0.09) | (0.09) | (0.10) | |
| Kinsfolk injured | −0.17 ** | −0.21 ** | −0.14 * | −0.18 ** | −0.14 * | −0.11 + | −0.13 * | −0.16 * |
| (0.06) | (0.07) | (0.07) | (0.07) | (0.06) | (0.07) | (0.06) | (0.07) | |
| Kinsfolk disabled | −0.02 | 0.00 | −0.01 | −0.05 | −0.14 + | −0.22 ** | −0.07 | −0.16 + |
| (0.08) | (0.09) | (0.09) | (0.09) | (0.07) | (0.08) | (0.08) | (0.09) | |
| Acquaintance died | −0.24 *** | −0.22 ** | −0.25 ** | −0.28 ** | −0.03 | 0.05 | −0.06 | −0.04 |
| (0.07) | (0.08) | (0.08) | (0.09) | (0.06) | (0.07) | (0.07) | (0.08) | |
| Acquaintance injured | −0.03 | 0.03 | −0.07 | −0.05 | 0.01 | 0.09 | −0.03 | −0.02 |
| (0.06) | (0.07) | (0.07) | (0.07) | (0.05) | (0.06) | (0.06) | (0.07) | |
| Acquaintance disabled | 0.02 | −0.02 | 0.04 | 0.01 | 0.03 | 0.03 | 0.01 | 0.05 |
| (0.06) | (0.07) | (0.07) | (0.07) | (0.06) | (0.06) | (0.06) | (0.07) | |
| Witness to others’ burial | −0.03 | −0.10 | 0.02 | −0.02 | −0.13 + | −0.08 | −0.19 * | −0.14 |
| (0.09) | (0.11) | (0.10) | (0.11) | (0.07) | (0.08) | (0.08) | (0.09) | |
| Witness to others’ death | −0.16 * | −0.14 + | −0.19 * | −0.16 + | −0.03 | −0.00 | −0.03 | −0.07 |
| (0.07) | (0.08) | (0.08) | (0.08) | (0.06) | (0.07) | (0.07) | (0.08) | |
| Witness to others’ injury | 0.02 | −0.03 | 0.03 | 0.04 | −0.08 | −0.09 | −0.10 | −0.02 |
| (0.06) | (0.07) | (0.07) | (0.07) | (0.06) | (0.07) | (0.07) | (0.07) | |
| Loss of house and property (0 = mildly) | ||||||||
| Moderate | 0.16 * | 0.13 | 0.19 * | 0.15 + | 0.39 *** | 0.40 *** | 0.37 *** | 0.46 *** |
| (0.08) | (0.09) | (0.09) | (0.09) | (0.06) | (0.07) | (0.07) | (0.08) | |
| Serious | 0.22 ** | 0.22 * | 0.21 * | 0.21 * | 0.56 *** | 0.51 *** | 0.54 *** | 0.70 *** |
| (0.08) | (0.09) | (0.09) | (0.09) | (0.07) | (0.08) | (0.08) | (0.09) | |
| Constant | 1.81 *** | 1.89 *** | 2.01 *** | 1.43 *** | 1.86 *** | 1.79 *** | 1.88 *** | 1.84 *** |
| (0.26) | (0.30) | (0.30) | (0.31) | (0.25) | (0.28) | (0.27) | (0.31) | |
| Observations | 425 | 425 | 425 | 425 | 575 | 575 | 575 | 575 |
| df | 28 | 28 | 28 | 28 | 28 | 28 | 28 | 28 |
| chi2 | 97.87 | 89.84 | 78.43 | 87.40 | 108.7 | 91 | 91.13 | 104.4 |
| Log likelihood | −347.4 | −404.5 | −397.5 | −416.8 | −504.3 | −582 | −558.5 | −634 |
| PR2 | 0.123 | 0.100 | 0.0898 | 0.0949 | 0.0973 | 0.0725 | 0.0754 | 0.0761 |
Appendix B
| Variables | High Trust (1 = yes) |
|---|---|
| Demographic and socioeconomic variables | |
| Male | −0.26 ** |
| (0.08) | |
| Age | 0.00 |
| (0.01) | |
| Rural site | −0.06 |
| (0.10) | |
| Married | 0.09 |
| (0.11) | |
| Educational background (0 = primary school and below) | |
| Junior high school | −0.24 + |
| (0.14) | |
| Senior high school | −0.23 |
| (0.17) | |
| Associate college and above | 0.01 |
| (0.20) | |
| Annual household income (0 = less than 40,000 RMB) | |
| 40,000–59,999 RMB | 0.20 + |
| (0.12) | |
| 60,000–89,999 RMB | 0.23 + |
| (0.14) | |
| 90,000 RMB and above | 0.36 * |
| (0.15) | |
| Earthquake exposure | |
| Being buried | −0.37 |
| (0.28) | |
| Being injured | −0.01 |
| (0.12) | |
| Being disabled | −1.33 ** |
| (0.41) | |
| Family died | 0.12 |
| (0.19) | |
| Family injured | −0.04 |
| (0.12) | |
| Family disabled | 0.10 |
| (0.18) | |
| Kinsfolk died | −0.06 |
| (0.13) | |
| Kinsfolk injured | −0.06 |
| (0.09) | |
| Kinsfolk disabled | −0.17 |
| (0.12) | |
| Acquaintance died | 0.15 |
| (0.11) | |
| Acquaintance injured | 0.09 |
| (0.09) | |
| Acquaintance disabled | −0.06 |
| (0.09) | |
| Witness to others’ burial | 0.09 |
| (0.13) | |
| Witness to others’ death | 0.03 |
| (0.10) | |
| Witness to others’ injury | −0.02 |
| (0.10) | |
| Loss of house and property (0 = mildly) | |
| Moderate | −0.14 |
| (0.11) | |
| Serious | −0.29 * |
| (0.12) | |
| Constant | 0.19 |
| (0.37) | |
| Observations | 1000 |
| df | 27 |
| chi2 | 72.94 |
| Log likelihood | −645.4 |
| PR2 | 0.0535 |
References
- Sanderson, D.; Sharma, A. IFRC World Disasters Report, Resilience: Saving Lives Today, Investing for Tomorrow; International Federation of Red Cross and Red Crescent Societies (IFRC): Geneva, Switzerland, 2016. [Google Scholar]
- Ando, S.; Saito, Y.; Nakamura, H.; Sone, M.; Sunmoto, E.Y. Report on the 2008 Great Sichuan Earthquake; United Nations Centre for Regional Development (UNCRD): Nagoya, Japan, 2009. [Google Scholar]
- China News Service Wenchuan Earthquake Has already Caused 69,227 Fatalities and 17,923 Missing. Available online: http://www.chinanews.com/gn/news/2008/09-25/1394600.shtml (accessed on 10 September 2018).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 9780890425541. [Google Scholar]
- Flores, E.C.; Carnero, A.M.; Bayer, A.M. Social capital and chronic post-traumatic stress disorder among survivors of the 2007 earthquake in Pisco, Peru. Soc. Sci. Med. 2014, 101, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.R.T.; McFarlane, A.C. The extent and impact of mental health problems after disaster. J. Clin. Psychiatry 2006, 67 (Suppl. 2), S9–S14. [Google Scholar]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 Disaster Victims Speak: Part I. An Empirical Review of the Empirical Literature, 1981–2001. Psychiatry Interpers. Biol. Process. 2002, 65, 207–239. [Google Scholar] [CrossRef]
- Udomratn, P. Mental health and the psychosocial consequences of natural disasters in Asia. Int. Rev. Psychiatry 2008, 20, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Deng, Q.; Glik, D.; Dong, J.; Zhang, L. A meta-analysis of risk factors for post-traumatic stress disorder (PTSD) in adults and children after earthquakes. Int. J. Environ. Rese. Public Health 2017, 14, 1537. [Google Scholar] [CrossRef] [PubMed]
- Kira, I.A.; Templin, T.; Lewandowski, L.; Ramaswamy, V.; Ozkan, B.; Mohanesh, J. The physical and mental health effects of Iraq war media exposure on Iraqi refugees. J. Muslim Ment. Health 2008, 3, 193–215. [Google Scholar] [CrossRef]
- Nevdal, R.; Gravdal, H.W.; Laberg, J.C.; Dyregrov, K. Should the population limit its exposure to media coverage after a terrorist attack? Scand. Psychol. 2016, 3, e6. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Nitiéma, P.; Pfefferbaum, R.L.; Houston, J.B.; Tucker, P.; Jeon-Slaughter, H.; North, C.S. Reactions of Oklahoma City bombing survivors to media coverage of the September 11, 2001, attacks. Compr. Psychiatry 2016, 65, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, Y.; Shi, Z.; Wang, W. Symptoms of Posttraumatic Stress Disorder among Adult Survivors Two Months after the Wenchuan Earthquake. Psychol. Rep. 2009, 105, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, J.; Zhou, M.; Shi, Z.; Liu, P. Symptoms of Posttraumatic Stress Disorder among Health Care Workers in Earthquake-Affected Areas in Southwest China. Psychol. Rep. 2010, 106, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, Y.; Wang, W.; Shi, Z.; Shen, J.; Li, M.; Xin, Y. Symptoms of posttraumatic stress disorder among adult survivors three months after the Sichuan earthquake in China. J. Traum. Stress 2009, 22, 444–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, J.; He, H.; Qu, Z.; Wang, X.; Liu, C. Post-traumatic stress disorder and depression among adult survivors 8 years after the 2008 Wenchuan earthquake in China. J. Affect. Disord. 2017, 210, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Fu, W.; Wu, J.; Ma, X.-C.; Sun, X.-L.; Huang, Y.; Hashimoto, K.; Gao, C.-G. Prevalence of ptsd and depression among junior middle school students in a rural town far from the epicenter of the Wenchuan Earthquake in China. PLoS ONE 2012, 7, e41665. [Google Scholar] [CrossRef]
- An, Y.; Fu, F.; Wu, X.; Lin, C.; Zhang, Y. Longitudinal Relationships between Neuroticism, Avoidant Coping, and Posttraumatic Stress Disorder Symptoms in Adolescents Following the 2008 Wenchuan Earthquake in China. J. Loss Trauma 2013, 18, 556–571. [Google Scholar] [CrossRef]
- Hamilton, J.D.; Workman, R.H., Jr. Persistence of combat-related posttraumatic stress symptoms for 75 years. J. Traum. Stress 1998, 11, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Liu, W.; Deng, G.; Liu, T.; Yan, J.; Tang, Y.; Dong, W.; Cui, Y.; Xu, M. Symptoms of posttraumatic stress disorder, depression, and anxiety among junior high school students in worst-hit areas 3 years after the Wenchuan earthquake in china. Asia-Pac. J. Public Health 2015, 27, NP1985–NP1994. [Google Scholar] [CrossRef] [PubMed]
- Neria, Y.; Sullivan, G.M. Understanding the Mental Health Effects of Indirect Exposure to Mass Trauma Through the Media. JAMA 2011, 306, 1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Zur, H.; Gil, S.; Shamshins, Y. The relationship between exposure to terror through the media, coping strategies and resources, and distress and secondary traumatization. Int. J. Stress Manag. 2012, 19, 132–150. [Google Scholar] [CrossRef]
- Ahern, J.; Galea, S.; Resnick, H.; Vlahov, D. Television Images and Probable Posttraumatic Stress Disorder after September 11: The Role of Background Characteristics, Event Exposures, and Perievent Panic. J. Nervous Ment. Dis. 2004, 192, 217–226. [Google Scholar] [CrossRef]
- Silver, R.C.; Holman, E.A.; Andersen, J.P.; Poulin, M.; McIntosh, D.N.; Gil-Rivas, V. Mental- and Physical-Health Effects of Acute Exposure to Media Images of the September 11, 2001, Attacks and the Iraq War. Psychol. Sci. 2013, 24, 1623–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saylor, C.F.; Cowart, B.L.; Lipovsky, J.A.; Jackson, C.; Finch, A.J. Media exposure to September 11: Elementary school students’ experiences and posttraumatic symptoms. Am. Behav. Sci. 2003, 46, 1622–1642. [Google Scholar] [CrossRef]
- Propper, R.E.; Stickgold, R.; Keeley, R.; Christman, S.D. Is Television Traumatic?: Dreams, Stress, and Media Exposure in the Aftermath of September 11, 2001. Psychol. Sci. 2007, 18, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Boyle, M.P.; Schmierbach, M.; Armstrong, C.L.; McLeod, D.M.; Shah, D.V.; Pan, Z. Information Seeking and Emotional Reactions to the September 11 Terrorist Attacks. Journal. Mass Commun. Q. 2004, 81, 155–167. [Google Scholar] [CrossRef]
- Kubey, R.; Peluso, T. Emotional response as a cause of interpersonal news diffusion: The case of the space shuttle tragedy. J. Broadcast. Media 1990, 34, 69–76. [Google Scholar] [CrossRef]
- Liang, Y. Trust in Chinese Government and Quality of Life (QOL) of Sichuan Earthquake Survivors: Does Trust in Government Help to Promote QOL? Soc. Indic. Res. 2016, 127, 541–564. [Google Scholar] [CrossRef]
- Lindstrom, M.; Axelsson, J.; Moden, B.; Rosvall, M. Sexual orientation, social capital and daily tobacco smoking: A population-based study. BMC Public Health 2014, 14, 565. [Google Scholar] [CrossRef] [PubMed]
- Carpiano, R.M. Toward a neighborhood resource-based theory of social capital for health: Can Bourdieu and sociology help? Soc. Sci. Med. 2006, 62, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Kopacz, M.S.; Ames, D.; Koenig, H.G. Association Between Trust and Mental, Social, and Physical Health Outcomes in Veterans and Active Duty Service Members with Combat-Related PTSD Symptomatology. Front. Psychiatry 2018, 9, 408. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, M.; Boyraz, G. Mindfulness, General Trust, and Social Support Among Trauma-Exposed College Students. J. Loss Trauma 2017, 22, 150–162. [Google Scholar] [CrossRef]
- Kuhlicke, C.; Steinführer, A.; Begg, C.; Bianchizza, C.; Bründl, M.; Buchecker, M.; De Marchi, B.; Di Masso Tarditti, M.; Höppner, C.; Komac, B.; et al. Perspectives on social capacity building for natural hazards: Outlining an emerging field of research and practice in Europe. Environ. Sci. Policy 2011, 14, 804–814. [Google Scholar] [CrossRef]
- Babcicky, P.; Seebauer, S. The two faces of social capital in private flood mitigation: Opposing effects on risk perception, self-efficacy and coping capacity. J. Risk Res. 2017, 20, 1017–1037. [Google Scholar] [CrossRef]
- Norris, F.H.; Stevens, S.P.; Pfefferbaum, B.; Wyche, K.F.; Pfefferbaum, R.L. Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. Am. J. Community Psychol. 2008, 41, 127–150. [Google Scholar] [CrossRef] [PubMed]
- Sawada, Y. Is trust really social capital? Commentary on Carpiano and Fitterer (2014). Soc. Sci. Med. 2014, 116, 237–238. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.D. Particularistic Trust and General Trust: A Network Analysis in Chinese Organizations. Manag. Organ. Rev. 2005, 1, 437–458. [Google Scholar] [CrossRef]
- Takakura, M. Does social trust at school affect students’ smoking and drinking behavior in Japan? Soc. Sci. Med. 2011, 72, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Baum, C.F.; Ganz, M.L.; Subramanian, S.V.; Kawachi, I. The contextual effects of social capital on health: A cross-national instrumental variable analysis. Soc. Sci. Med. 2011, 73, 1689–1697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, J.; Burns, W.; Mertz, C.K.; Slovic, P. Trust as a Determinant of Opposition to a High-Level Radioactive Waste Repository: Analysis of a Structural Model. Risk Anal. 1992, 12, 417–429. [Google Scholar] [CrossRef]
- Vasterman, P.; Yzermans, C.J.; Dirkzwager, A.J.E. The role of the media and media hypes in the aftermath of disasters. Epidemiol. Rev. 2005, 27, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Miura, I.; Nagai, M.; Maeda, M.; Harigane, M.; Fujii, S.; Oe, M.; Yabe, H.; Suzuki, Y.; Takahashi, H.; Ohira, T.; et al. Perception of radiation risk as a predictor of mid-term mental health after a nuclear disaster: The fukushima health management survey. Int. J. Environ. Res. Public Health 2017, 14, 1067. [Google Scholar] [CrossRef] [PubMed]
- Binder, A.R.; Scheufele, D.A.; Brossard, D.; Gunther, A.C. Interpersonal Amplification of Risk? Citizen Discussions and Their Impact on Perceptions of Risks and Benefits of a Biological Research Facility. Risk Anal. 2011, 31, 324–334. [Google Scholar] [CrossRef] [PubMed]
- PRC, T.S.C. of Overall Post-Disaster Recovery and Reconstruction Planning for Wenchuan Earthquake. Available online: http://www.gov.cn/zwgk/2008-09/23/content_1103686.htm (accessed on 5 September 2018).
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD Checklist: Reliability, validity, and diagnostic utility. Int. Soc. Traum. Stress Stud. 1993, 2, 90–92. [Google Scholar]
- Forbes, D.; Creamer, M.; Biddle, D. The validity of the PTSD checklist as a measure of symptomatic change in combat-related PTSD. Behav. Res. Ther. 2001, 39, 977–986. [Google Scholar] [CrossRef]
- Xu, J.; Song, X. Posttraumatic stress disorder among survivors of the Wenchuan earthquake 1 year after: Prevalence and risk factors. Compr. Psychiatry 2011, 52, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Galea, S.; Resnick, H.; Kilpatrick, D.; Bucuvalas, M.; Gold, J.; Vlahov, D. Television Images and Psychological Symptoms after the September 11 Terrorist Attacks. Psychiatry Interpers. Biol. Process. 2002, 65, 289–300. [Google Scholar] [CrossRef]
- Collimore, K.C.; McCabe, R.E.; Carleton, R.N.; Asmundson, G.J.G. Media exposure and dimensions of anxiety sensitivity: Differential associations with PTSD symptom clusters. J. Anxiety Disord. 2008, 22, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Giordano, G.N.; Merlo, J.; Ohlsson, H.; Rosvall, M.; Lindstrom, M. Testing the association between social capital and health over time: A family-based design. BMC Public Health 2013, 13, 665. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ho, S.M.Y. Risk Factors of Posttraumatic Stress Disorder among Survivors after the 512 Wenchuan Earthquake in China. PLoS ONE 2011, 6, e22371. [Google Scholar] [CrossRef] [PubMed]
- Kun, P.; Chen, X.; Han, S.; Gong, X.; Chen, M.; Zhang, W.; Yao, L. Prevalence of post-traumatic stress disorder in Sichuan Province, China after the 2008 Wenchuan earthquake. Public Health 2009, 123, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Jarque, C.M.; Bera, A.K. A test for normality of observations and regression residuals. Int. Stat. Rev./Revue Internationale de Statistique 1987, 55, 163–172. [Google Scholar] [CrossRef]
- McDonald, J.F.; Moffitt, R.A. The Uses of Tobit Analysis. Rev. Econ. Stat. 1980, 62, 318. [Google Scholar] [CrossRef]
- Kristensen, P.; Dyregrov, K.; Dyregrov, A.; Heir, T. Media exposure and prolonged grief: A study of bereaved parents and siblings after the 2011 utøya island terror attack. Psychol. Trauma Theory Res. Pract. Policy 2016, 8, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Bodas, M.; Siman-Tov, M.; Peleg, K.; Solomon, Z. Anxiety-Inducing Media: The Effect of Constant News Broadcasting on the Well-Being of Israeli Television Viewers. Psychiatry 2015, 78, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; Tucker, P.; Pfefferbaum, R.L.; Nelson, S.D.; Nitiéma, P.; Newman, E. Media Effects in Youth Exposed to Terrorist Incidents: A Historical Perspective. Curr. Psychiatry Rep. 2018, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Zhang, Y.; Yang, Y.; Mo, L.; Liu, X. Symptoms of posttraumatic stress disorder, depression, and anxiety among adolescents following the 2008 Wenchuan earthquake in China. J. Traum. Stress 2011, 24, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Musalia, J. Social capital and health in Kenya: A multilevel analysis. Soc. Sci. Med. 2016, 167, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Putnam, R.D. Bowling alone: Americas´s declining social capital. J. Democr. 1995, 6, 65–78. [Google Scholar] [CrossRef]
- Fei, X. From the Soil, the Foundations of Chinese Society: A Translation of Fei Xiaotong’s Xiangtu Zhongguo; University of California Press: Berkeley, CA, USA, 1992. [Google Scholar]
- Hu, A.; Zhou, Y. Revisiting the Negative Effects of Confucian Culture on Generalized Trust: A study based on 2007 Chinese spiritual life survey. Sociol. Stud. 2013, 28, 28–54. [Google Scholar]
- Brannon, L.A.; Tagler, M.J.; Eagly, A.H. The moderating role of attitude strength in selective exposure to information. J. Exp. Soc. Psychol. 2007, 43, 611–617. [Google Scholar] [CrossRef]
- Maercker, A.; Mehr, A. What if victims read a newspaper report about their victimization? A study on the relationship to PTSD symptoms in crime victims. Eur. Psychol. 2006, 11, 137–142. [Google Scholar] [CrossRef]
- Steinhardt, H.C. How is High Trust in China Possible? Comparing the Origins of Generalized Trust in Three Chinese Societies. Political Stud. 2012, 60, 434–454. [Google Scholar] [CrossRef]



| Variable | Obs | Mean | Std.Dev. | Min | Max |
|---|---|---|---|---|---|
| PTSD symptoms | |||||
| PCL-C score | 1000 | 2.364 | 0.626 | 1 | 4.412 |
| Reexperiencing | 1000 | 2.364 | 0.692 | 1 | 4.6 |
| Avoidance | 1000 | 2.374 | 0.673 | 1 | 4.571 |
| Arousal | 1000 | 2.349 | 0.726 | 1 | 4.4 |
| Independent variables | |||||
| Media exposure | 1000 | 3.765 | 0.985 | 1 | 5 |
| General trust (0 = low trust) | 1000 | 0.575 | 0.495 | 0 | 1 |
| Demographic and socioeconomic variables | |||||
| Male | 1000 | 0.435 | 0.496 | 0 | 1 |
| Age | 1000 | 45.618 | 11.628 | 28 | 74 |
| Rural site | 1000 | 0.557 | 0.497 | 0 | 1 |
| Married | 1000 | 0.827 | 0.378 | 0 | 1 |
| Educational background (0 = primary school and below) | |||||
| Junior high school | 1000 | 0.313 | 0.464 | 0 | 1 |
| Senior high school | 1000 | 0.277 | 0.448 | 0 | 1 |
| Associate college and above | 1000 | 0.253 | 0.435 | 0 | 1 |
| Annual household income (0 = less than 40,000 RMB) | |||||
| 40,000–59,999 RMB | 1000 | 0.286 | 0.452 | 0 | 1 |
| 60,000–89,999 RMB | 1000 | 0.255 | 0.436 | 0 | 1 |
| 90,000 RMB and above | 1000 | 0.221 | 0.415 | 0 | 1 |
| Earthquake exposure | |||||
| Being buried | 1000 | 0.024 | 0.153 | 0 | 1 |
| Being injured | 1000 | 0.152 | 0.359 | 0 | 1 |
| Being disabled | 1000 | 0.018 | 0.133 | 0 | 1 |
| Family died | 1000 | 0.057 | 0.232 | 0 | 1 |
| Family injured | 1000 | 0.218 | 0.413 | 0 | 1 |
| Family disabled | 1000 | 0.061 | 0.239 | 0 | 1 |
| Kinsfolk died | 1000 | 0.138 | 0.345 | 0 | 1 |
| Kinsfolk injured | 1000 | 0.388 | 0.488 | 0 | 1 |
| Kinsfolk disabled | 1000 | 0.179 | 0.384 | 0 | 1 |
| Acquaintance died | 1000 | 0.197 | 0.398 | 0 | 1 |
| Acquaintance injured | 1000 | 0.423 | 0.494 | 0 | 1 |
| Acquaintance disabled | 1000 | 0.303 | 0.460 | 0 | 1 |
| Witness to others’ bury | 1000 | 0.130 | 0.336 | 0 | 1 |
| Witness to others’ death | 1000 | 0.232 | 0.422 | 0 | 1 |
| Witness to others’ injury | 1000 | 0.360 | 0.480 | 0 | 1 |
| Loss of house and property (0 = mildly) | |||||
| Moderate | 1000 | 0.420 | 0.494 | 0 | 1 |
| Serious | 1000 | 0.310 | 0.463 | 0 | 1 |
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 |
|---|---|---|---|---|---|---|---|---|
| PCL-C Score | Reexperiencing | Avoidance | Arousal | |||||
| Independent variables | ||||||||
| Media exposure | −0.01 | 0.01 | −0.03 | −0.00 | ||||
| (0.02) | (0.02) | (0.02) | (0.02) | |||||
| General trust (0 = low trust) | −0.12 ** | −0.08 + | −0.13 ** | −0.16 *** | ||||
| (0.04) | (0.04) | (0.04) | (0.05) | |||||
| Demographic and socioeconomic variables | ||||||||
| Male | 0.05 | 0.04 | 0.08 + | 0.07 | 0.03 | 0.02 | 0.05 | 0.04 |
| (0.04) | (0.04) | (0.04) | (0.04) | (0.04) | (0.04) | (0.05) | (0.05) | |
| Age | 0.01 *** | 0.01 *** | 0.01 ** | 0.01 ** | 0.01 ** | 0.01 ** | 0.01 *** | 0.01 *** |
| (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | |
| Rural site | 0.07 | 0.06 | 0.06 | 0.06 | 0.06 | 0.05 | 0.08 | 0.08 |
| (0.04) | (0.04) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | |
| Married | −0.07 | −0.06 | −0.14 * | −0.13 * | −0.03 | −0.02 | −0.05 | −0.05 |
| (0.05) | (0.05) | (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | |
| Educational background (0 = primary school and below) | ||||||||
| Junior high school | 0.13 * | 0.12 + | 0.12 | 0.11 | 0.12 + | 0.12 | 0.18 * | 0.16 * |
| (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | (0.08) | (0.08) | |
| Senior high school | 0.25 ** | 0.24 ** | 0.23 * | 0.22 * | 0.24 ** | 0.23 ** | 0.30 ** | 0.28 ** |
| (0.08) | (0.08) | (0.09) | (0.09) | (0.09) | (0.09) | (0.10) | (0.09) | |
| Associate college and above | 0.40 *** | 0.40 *** | 0.32 ** | 0.32 ** | 0.40 *** | 0.40 *** | 0.48 *** | 0.48 *** |
| (0.09) | (0.09) | (0.10) | (0.10) | (0.10) | (0.10) | (0.11) | (0.11) | |
| Annual household income (0 = less than 40,000 RMB) | ||||||||
| 40,000–59,999 RMB | −0.10 + | −0.09 | −0.10 | −0.09 | −0.11 + | −0.09 | −0.08 | −0.07 |
| (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | (0.07) | (0.07) | |
| 60,000–89,999 RMB | −0.22 *** | −0.20 *** | −0.22 ** | −0.21 ** | −0.22 ** | −0.21 ** | −0.22 ** | −0.20 ** |
| (0.06) | (0.06) | (0.07) | (0.07) | (0.07) | (0.07) | (0.08) | (0.07) | |
| 90,000 RMB and above | −0.12 + | −0.10 | −0.05 | −0.04 | −0.18 * | −0.15 * | −0.11 | −0.09 |
| (0.07) | (0.07) | (0.08) | (0.08) | (0.08) | (0.08) | (0.08) | (0.08) | |
| Earthquake exposure | ||||||||
| Being buried | 0.07 | 0.05 | −0.01 | −0.02 | 0.06 | 0.04 | 0.17 | 0.15 |
| (0.12) | (0.12) | (0.14) | (0.14) | (0.14) | (0.14) | (0.15) | (0.15) | |
| Being injured | −0.13 * | −0.13 * | −0.10 | −0.11 | −0.14 * | −0.14 * | −0.17 * | −0.17 * |
| (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | (0.07) | (0.07) | |
| Being disabled | 0.10 | 0.05 | 0.02 | −0.01 | 0.19 | 0.14 | 0.03 | −0.03 |
| (0.14) | (0.14) | (0.16) | (0.16) | (0.16) | (0.16) | (0.18) | (0.18) | |
| Family died | 0.05 | 0.05 | 0.03 | 0.03 | 0.06 | 0.07 | 0.02 | 0.03 |
| (0.09) | (0.09) | (0.10) | (0.10) | (0.10) | (0.10) | (0.11) | (0.11) | |
| Family injured | 0.12 * | 0.11 * | 0.19 ** | 0.19 ** | 0.06 | 0.06 | 0.12 + | 0.12 + |
| (0.05) | (0.05) | (0.06) | (0.06) | (0.06) | (0.06) | (0.07) | (0.06) | |
| Family disabled | −0.12 | −0.12 | −0.17 + | −0.16 + | −0.08 | −0.08 | −0.14 | −0.14 |
| (0.08) | (0.08) | (0.09) | (0.09) | (0.09) | (0.09) | (0.10) | (0.10) | |
| Kinsfolk died | −0.14 * | −0.14 * | −0.11 + | −0.12 + | −0.12 + | −0.12 + | −0.19 ** | −0.20 ** |
| (0.06) | (0.06) | (0.07) | (0.07) | (0.06) | (0.06) | (0.07) | (0.07) | |
| Kinsfolk injured | −0.15 *** | −0.15 *** | −0.16 *** | −0.16 *** | −0.12 ** | −0.13 ** | −0.17 *** | −0.17 *** |
| (0.04) | (0.04) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | |
| Kinsfolk disabled | −0.06 | −0.07 | −0.11 + | −0.11 + | −0.02 | −0.04 | −0.09 | −0.10 |
| (0.05) | (0.05) | (0.06) | (0.06) | (0.06) | (0.06) | (0.07) | (0.07) | |
| Acquaintance died | −0.12 * | −0.11 * | −0.06 | −0.05 | −0.14 ** | −0.13 * | −0.14 * | −0.13 * |
| (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.06) | (0.06) | |
| Acquaintance injured | −0.01 | −0.01 | 0.06 | 0.07 | −0.05 | −0.04 | −0.04 | −0.03 |
| (0.04) | (0.04) | (0.05) | (0.05) | (0.04) | (0.04) | (0.05) | (0.05) | |
| Acquaintance disabled | 0.04 | 0.04 | 0.04 | 0.04 | 0.05 | 0.05 | 0.05 | 0.05 |
| (0.04) | (0.04) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | |
| Witness to others’ burial | −0.11 + | −0.11 + | −0.10 | −0.10 | −0.13 * | −0.13 * | −0.11 | −0.11 |
| (0.06) | (0.06) | (0.07) | (0.07) | (0.06) | (0.06) | (0.07) | (0.07) | |
| Witness to others’ death | −0.09 + | −0.09 + | −0.06 | −0.06 | −0.10 * | −0.09 + | −0.12 * | −0.11 * |
| (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.06) | (0.06) | |
| Witness to others’ injury | −0.05 | −0.05 | −0.07 | −0.07 | −0.06 | −0.06 | −0.02 | −0.02 |
| (0.04) | (0.04) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | |
| Loss of house and property (0 = mildly) | ||||||||
| Moderate | 0.32 *** | 0.32 *** | 0.31 *** | 0.31 *** | 0.32 *** | 0.32 *** | 0.36 *** | 0.35 *** |
| (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.06) | (0.06) | |
| Serious | 0.42 *** | 0.41 *** | 0.40 *** | 0.39 *** | 0.41 *** | 0.39 *** | 0.49 *** | 0.48 *** |
| (0.05) | (0.05) | (0.06) | (0.06) | (0.06) | (0.06) | (0.07) | (0.07) | |
| Constant | 1.76 *** | 1.86 *** | 1.83 *** | 1.83 *** | 1.79 *** | 1.96 *** | 1.57 *** | 1.67 *** |
| (0.17) | (0.18) | (0.19) | (0.21) | (0.19) | (0.20) | (0.21) | (0.22) | |
| Observations | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 | 1000 |
| df | 27 | 29 | 27 | 29 | 27 | 29 | 27 | 29 |
| chi2 | 162 | 172 | 135.8 | 139 | 132 | 144.3 | 143.3 | 154.5 |
| Log likelihood | -882.9 | −877.9 | −1013 | −1011 | −984.3 | −978.2 | −1087 | −1081 |
| PR2 | 0.0841 | 0.0892 | 0.0628 | 0.0643 | 0.0629 | 0.0687 | 0.0619 | 0.0667 |
| Variables | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| PCL-C Score | Reexperiencing | Avoidance | Arousal | |
| Interaction Item | ||||
| Media exposure × General trust | −0.07 + | −0.06 | −0.06 | −0.10 * |
| (0.04) | (0.04) | (0.04) | (0.05) | |
| Independent variables | ||||
| Media exposure | 0.03 | 0.05 | 0.00 | 0.05 |
| (0.03) | (0.03) | (0.03) | (0.04) | |
| General trust (0 = low trust) | 0.14 | 0.15 | 0.08 | 0.21 |
| (0.15) | (0.17) | (0.16) | (0.18) | |
| Demographic and socioeconomic variables | ||||
| Male | 0.04 | 0.06 | 0.02 | 0.03 |
| (0.04) | (0.04) | (0.04) | (0.05) | |
| Age | 0.01 *** | 0.01 ** | 0.01 ** | 0.01 *** |
| (0.00) | (0.00) | (0.00) | (0.00) | |
| Rural site | 0.06 | 0.06 | 0.05 | 0.08 |
| (0.04) | (0.05) | (0.05) | (0.05) | |
| Married | −0.06 | −0.14 * | −0.02 | −0.05 |
| (0.05) | (0.06) | (0.06) | (0.06) | |
| Educational background (0 = primary school and below) | ||||
| Junior high school | 0.12 + | 0.11 | 0.11 | 0.16 * |
| (0.06) | (0.07) | (0.07) | (0.08) | |
| Senior high school | 0.24 ** | 0.22 * | 0.23 ** | 0.29 ** |
| (0.08) | (0.09) | (0.09) | (0.09) | |
| Associate college and above | 0.40 *** | 0.32 ** | 0.40 *** | 0.48 *** |
| (0.09) | (0.10) | (0.10) | (0.11) | |
| Annual household income (0 = less than 40,000 RMB) | ||||
| 40,000–59,999 RMB | −0.08 | −0.09 | −0.09 | −0.06 |
| (0.06) | (0.06) | (0.06) | (0.07) | |
| 60,000–89,999 RMB | −0.20 ** | −0.21 ** | −0.20 ** | −0.20 ** |
| (0.06) | (0.07) | (0.07) | (0.07) | |
| 90,000 RMB and above | −0.09 | −0.03 | −0.15 + | −0.08 |
| (0.07) | (0.08) | (0.08) | (0.08) | |
| Earthquake exposure | ||||
| Being buried | 0.06 | −0.02 | 0.05 | 0.16 |
| (0.12) | (0.14) | (0.14) | (0.15) | |
| Being injured | −0.14 * | −0.11 + | −0.14 * | −0.17 * |
| (0.06) | (0.06) | (0.06) | (0.07) | |
| Being disabled | 0.04 | −0.01 | 0.14 | −0.03 |
| (0.14) | (0.16) | (0.16) | (0.17) | |
| Family died | 0.06 | 0.04 | 0.08 | 0.04 |
| (0.09) | (0.10) | (0.10) | (0.11) | |
| Family injured | 0.12 * | 0.20 ** | 0.06 | 0.13 + |
| (0.05) | (0.06) | (0.06) | (0.06) | |
| Family disabled | −0.12 | −0.16 + | −0.08 | −0.14 |
| (0.08) | (0.09) | (0.09) | (0.10) | |
| Kinsfolk died | −0.14 * | −0.12 + | −0.12 + | −0.20 ** |
| (0.06) | (0.07) | (0.06) | (0.07) | |
| Kinsfolk injured | −0.16 *** | −0.16 *** | −0.13 ** | −0.18 *** |
| (0.04) | (0.05) | (0.05) | (0.05) | |
| Kinsfolk disabled | −0.08 | −0.12 + | −0.04 | −0.11 |
| (0.05) | (0.06) | (0.06) | (0.07) | |
| Acquaintance died | −0.11 * | −0.05 | −0.12 * | −0.13 * |
| (0.05) | (0.05) | (0.05) | (0.06) | |
| Acquaintance injured | −0.01 | 0.06 | −0.05 | −0.03 |
| (0.04) | (0.05) | (0.04) | (0.05) | |
| Acquaintance disabled | 0.04 | 0.04 | 0.05 | 0.05 |
| (0.04) | (0.05) | (0.05) | (0.05) | |
| Witness to others’ burial | −0.11 + | −0.10 | −0.13 * | −0.11 |
| (0.06) | (0.07) | (0.06) | (0.07) | |
| Witness to others’ death | −0.09 + | −0.06 | −0.10 + | −0.12 * |
| (0.05) | (0.05) | (0.05) | (0.06) | |
| Witness to others’ injury | −0.05 | −0.07 | −0.05 | −0.02 |
| (0.04) | (0.05) | (0.05) | (0.05) | |
| Loss of house and property (0 = mildly) | ||||
| Moderate | 0.32 *** | 0.31 *** | 0.32 *** | 0.35 *** |
| (0.05) | (0.05) | (0.05) | (0.06) | |
| Serious | 0.41 *** | 0.40 *** | 0.39 *** | 0.48 *** |
| (0.05) | (0.06) | (0.06) | (0.07) | |
| Constant | 1.71 *** | 1.70 *** | 1.84 *** | 1.46 *** |
| (0.20) | (0.23) | (0.22) | (0.24) | |
| Observations | 1000 | 1000 | 1000 | 1000 |
| Df | 30 | 30 | 30 | 30 |
| chi2 | 175.3 | 141 | 146.2 | 159 |
| Log likelihood | −876.2 | −1010 | −977.3 | −1079 |
| PR2 | 0.0909 | 0.0652 | 0.0696 | 0.0686 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, L.; Lai, K.; Lin, Z.; Ma, Z. Media Exposure and General Trust as Predictors of Post-traumatic Stress Disorder: Ten Years after the 5.12 Wenchuan Earthquake in China. Int. J. Environ. Res. Public Health 2018, 15, 2386. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112386
He L, Lai K, Lin Z, Ma Z. Media Exposure and General Trust as Predictors of Post-traumatic Stress Disorder: Ten Years after the 5.12 Wenchuan Earthquake in China. International Journal of Environmental Research and Public Health. 2018; 15(11):2386. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112386
Chicago/Turabian StyleHe, Lingnan, Kaisheng Lai, Zhongxuan Lin, and Zhihao Ma. 2018. "Media Exposure and General Trust as Predictors of Post-traumatic Stress Disorder: Ten Years after the 5.12 Wenchuan Earthquake in China" International Journal of Environmental Research and Public Health 15, no. 11: 2386. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112386