Association between Dietary Mineral Intake and Chronic Kidney Disease: The Health Examinees (HEXA) Study

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
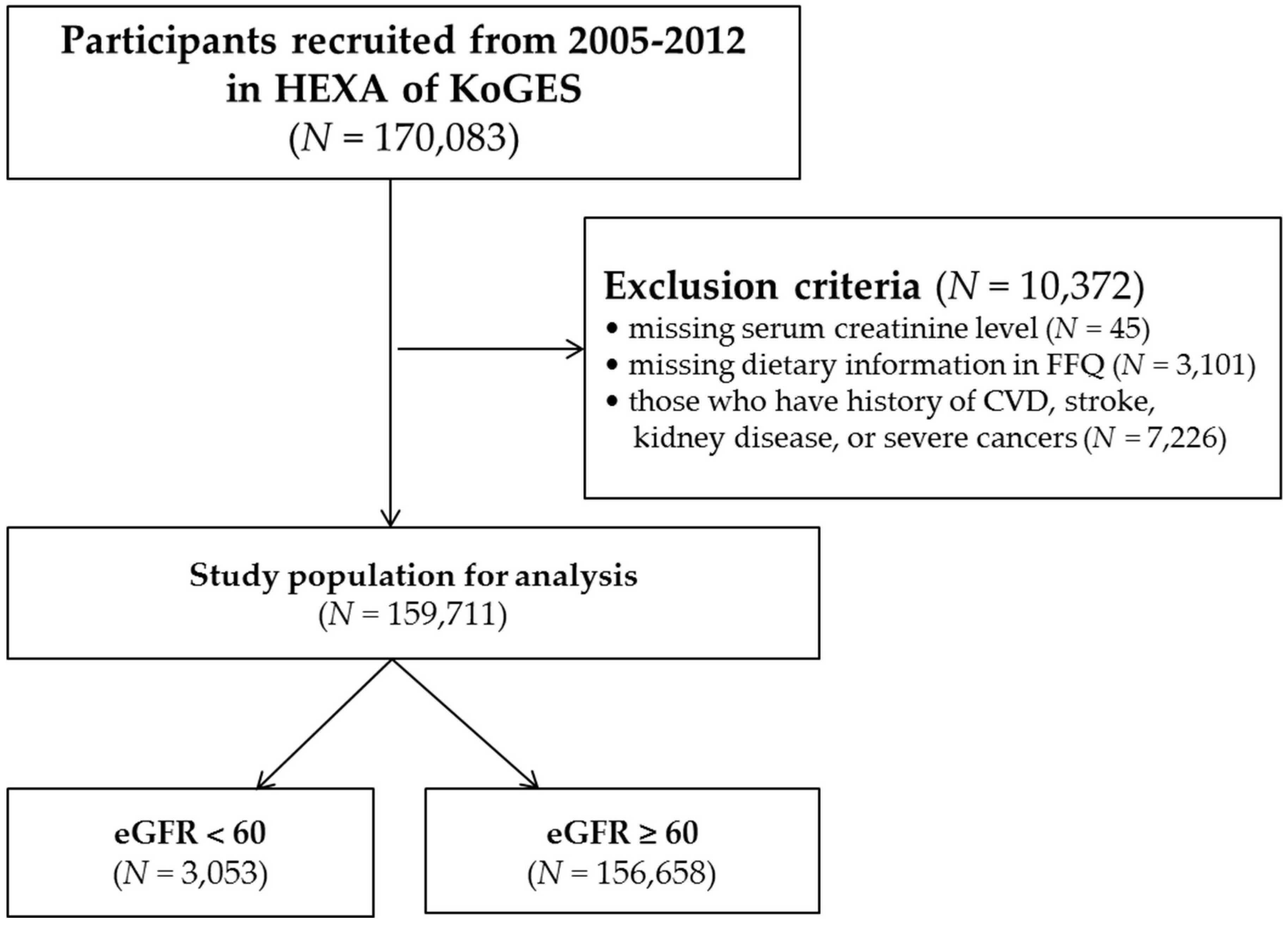
2.1. Study Population
2.2. Definition of CKD
2.3. Dietary Assessment
2.4. Clinical and Laboratory Measurements
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
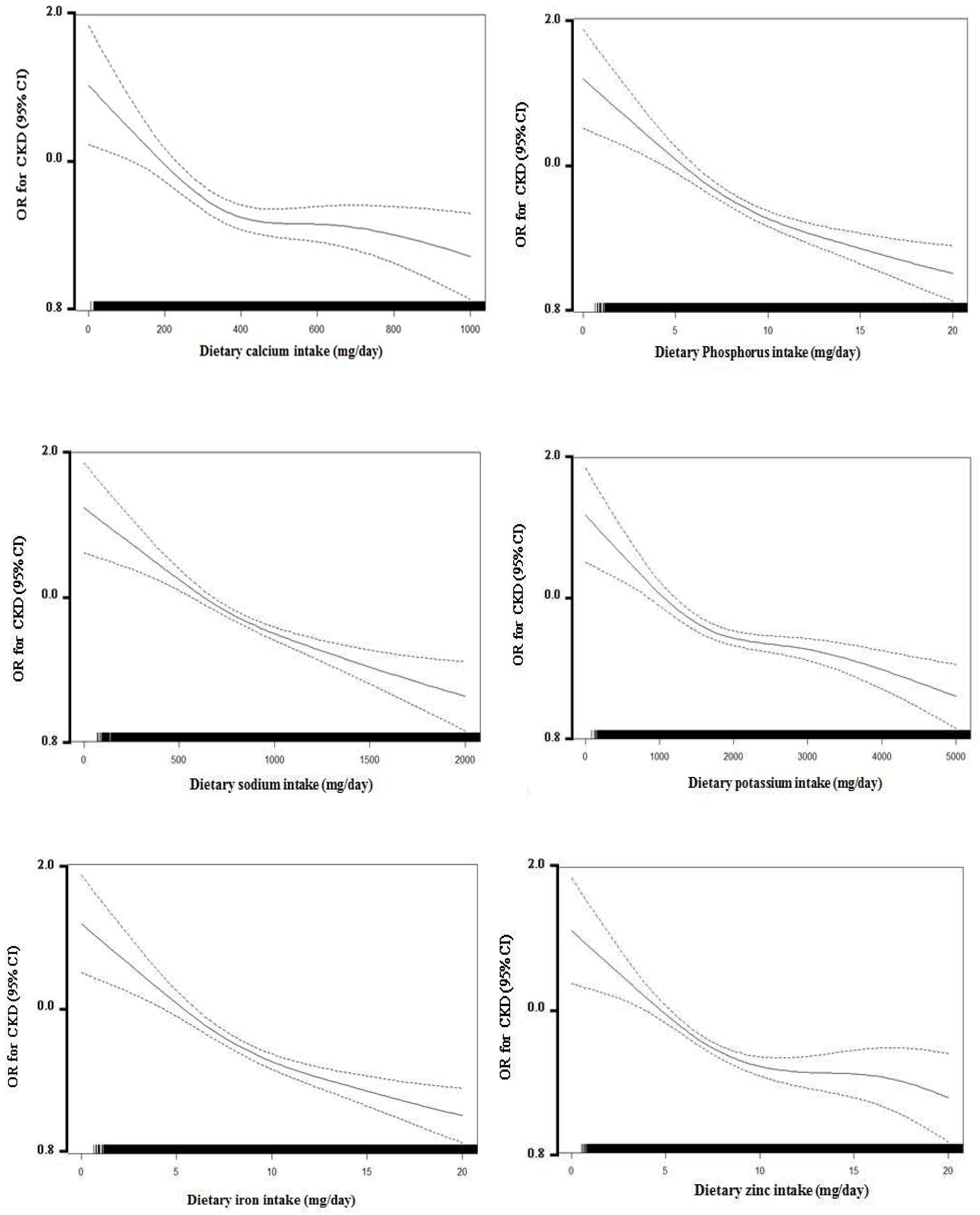
3.2. The Associations between Dietary Mineral Intake and CKD
3.3. The Associations between Dietary Mineral Intake and CKD Stratified by Hypertension Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Group, K.W. Definition and classification of stages of chronic kidney disease. Am. J. Kidney Dis. 2002, 39, S46–S75. [Google Scholar]
- Woo, K.-T.; Choong, H.L.; Wong, K.-S.; Tan, H.B.; Chan, C.-M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2012, 81, 1044–1045. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C.W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Eggers, P.W. Has the incidence of end-stage renal disease in the USA and other countries stabilized? Curr. Opin. Nephrol. Hypertens. 2011, 20, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Park, J.I.; Baek, H.; Jung, H.H. Prevalence of chronic kidney disease in korea: The korean national health and nutritional examination survey 2011–2013. J. Korean Med. Sci. 2016, 31, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, K.; Levey, A.S.; Sarnak, M.J. Traditional Cardiac Risk Factors in Individuals with Chronic Kidney Disease. Semin Dial. 2003, 16, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar] [CrossRef]
- Chartsrisak, K.; Vipattawat, K.; Assanatham, M.; Nongnuch, A.; Ingsathit, A.; Domrongkitchaiporn, S.; Sumethkul, V.; Distha-Banchong, S. Mineral metabolism and outcomes in chronic kidney disease stage 2–4 patients. BMC Nephrol. 2013, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Farhadnejad, H.; Asghari, G.; Mirmiran, P.; Yuzbashian, E.; Azizi, F. Micronutrient intakes and incidence of chronic kidney disease in adults: Tehran lipid and glucose study. Nutrients 2016, 8, 217. [Google Scholar] [CrossRef] [PubMed]
- Noori, N.; Kalantar-Zadeh, K.; Kovesdy, C.P.; Bross, R.; Benner, D.; Kopple, J.D. Association of dietary phosphorus intake and phosphorus to protein ratio with mortality in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2010, 5, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Noori, N.; Kalantar-Zadeh, K.; Kovesdy, C.P.; Murali, S.B.; Bross, R.; Nissenson, A.R.; Kopple, J.D. Dietary potassium intake and mortality in long-term hemodialysis patients. Am. J. Kidney Dis. 2010, 56, 338–347. [Google Scholar] [CrossRef] [PubMed]
- McMahon, E.J.; Bauer, J.D.; Hawley, C.M.; Isbel, N.M.; Stowasser, M.; Johnson, D.W.; Campbell, K.L. A randomized trial of dietary sodium restriction in ckd. J. Am. Soc. Nephrol. 2013, 24, 2096–2103. [Google Scholar] [CrossRef] [PubMed]
- Strippoli, G.F.; Craig, J.C.; Rochtchina, E.; Flood, V.M.; Wang, J.J.; Mitchell, P. Fluid and nutrient intake and risk of chronic kidney disease. Nephrology 2011, 16, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The korea national health and nutrition examination survey (knhanes). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G. Cohort profile: The korean genome and epidemiology study (koges) consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. The national academies collection: Reports funded by national institutes of health. In Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin d, and Fluoride; National Academies Press (US): Washington, DC, USA; National Academy of Sciences: Washington, DC, USA, 1997. [Google Scholar]
- Trumbo, P.; Yates, A.A.; Schlicker, S.; Poos, M. Dietary Reference Intakes for Vitamin a, Vitamin k, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press (US): Washington, DC, USA, 2001. [Google Scholar]
- Sawka, M. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; The National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- World Health Organization. Guideline: Sodium intake for adults and children. In Guideline: Sodium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Yang, J.J.; Yang, J.H.; Kim, J.; Cho, L.Y.; Park, B.; Ma, S.H.; Song, S.H.; Min, W.-K.; Kim, S.S.; Park, M.S. Reliability of quadruplicated serological parameters in the Korean genome and epidemiology study. Epidemiol. Health 2011, 33, e2011004. [Google Scholar] [CrossRef] [PubMed]
- Da, J.; Xie, X.; Wolf, M.; Disthabanchong, S.; Wang, J.; Zha, Y.; Lv, J.; Zhang, L.; Wang, H. Serum phosphorus and progression of ckd and mortality: A meta-analysis of cohort studies. Am. J. Kidney Dis. 2015, 66, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Bellasi, A.; Mandreoli, M.; Baldrati, L.; Corradini, M.; Di Nicolo, P.; Malmusi, G.; Santoro, A. Chronic kidney disease progression and outcome according to serum phosphorus in mild-to-moderate kidney dysfunction. Clin. J. Am. Soc. Nephrol. CJASN 2011, 6, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Ibels, L.S.; Alfrey, A.C.; Haut, L.; Huffer, W.E. Preservation of function in experimental renal disease by dietary restriction of phosphate. N. Engl. J. Med. 1978, 298, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.R.; Miller, E.R., 3rd; Anderson, C.A.; Juraschek, S.P.; Moser, M.; White, K.; Henry, B.; Krekel, C.; Oh, S.; Charleston, J.; et al. Phosphorus additives and albuminuria in early stages of ckd: A randomized controlled trial. Am. J. Kidney Dis. 2016, 69, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Isakova, T.; Xie, H.; Yang, W.; Xie, D.; Anderson, A.H.; Scialla, J.; Wahl, P.; Gutiérrez, O.M.; Steigerwalt, S.; He, J. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. Jama 2011, 305, 2432–2439. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Soltero, L.; Zhang, P.; Huang, X.R.; Lan, H.Y.; Adrogue, H.J. Renal inflammation is modulated by potassium in chronic kidney disease: Possible role of smad7. Am. J. Physiol. Renal Physiol. 2007, 293, F1123–F1130. [Google Scholar] [CrossRef] [PubMed]
- Aaron, K.J.; Sanders, P.W. Role of dietary salt and potassium intake in cardiovascular health and disease: A review of the evidence. In Mayo Clinic Proceedings; Elsevier: New York, NY, USA, 2013; pp. 987–995. [Google Scholar]
- Macdougall, I.C.; Bircher, A.J.; Eckardt, K.-U.; Obrador, G.T.; Pollock, C.A.; Stenvinkel, P.; Swinkels, D.W.; Wanner, C.; Weiss, G.; Chertow, G.M. Iron management in chronic kidney disease: Conclusions from a “kidney disease: Improving global outcomes”(kdigo) controversies conference. Kidney Int. 2016, 89, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Cană-Ruiu, D.; Moţa, E.; Istrate, N.; Văduva, C.; Trican, E. Renal anemia-risk factor for chronic kidney disease. Curr. Health Sci. J. 2013, 39, 214. [Google Scholar] [PubMed]
- Del Fabbro, P.; Luthi, J.-C.; Carrera, E.; Michel, P.; Burnier, M.; Burnand, B. Anemia and chronic kidney disease are potential risk factors for mortality in stroke patients: A historic cohort study. BMC Nephrol. 2010, 11, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, L.G.; Norman, J.T. Chronic hypoxia as a mechanism of progression of chronic kidney diseases: From hypothesis to novel therapeutics. Kidney Int. 2008, 74, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, C.; Oh, Y.; Joo, K.; Kim, Y.; Kim, S.; Lim, C. The effects of oral iron supplementation on the progression of anemia and renal dysfunction in patients with chronic kidney disease. Clin. Nephrol. 2011, 75, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Tomat, A.L.; Weisstaub, A.R.; Jauregui, A.; Pineiro, A.; Balaszczuk, A.M.; Costa, M.A.; Arranz, C.T. Moderate zinc deficiency influences arterial blood pressure and vascular nitric oxide pathway in growing rats. Pediatr. Res. 2005, 58, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Yanagisawa, H.; Nojima, Y.; Tamura, J.; Wada, O. Zn deficiency aggravates hypertension in spontaneously hypertensive rats: Possible role of cu/zn-superoxide dismutase. Clin. Exp. Hypertens. 2002, 24, 355–370. [Google Scholar] [CrossRef] [PubMed]
- Bidani, A.K.; Griffin, K.A. Pathophysiology of hypertensive renal damage: Implications for therapy. Hypertension 2004, 44, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Pupim, L.B.; Cuppari, L.; Ikizler, T.A. Nutrition and Metabolism in Kidney Disease. In Seminars in Nephrology; Elsevier: New York, NY, USA, 2006; pp. 134–157. [Google Scholar]
- Reinivuo, H.; Valsta, L.M.; Laatikainen, T.; Tuomilehto, J.; Pietinen, P. Sodium in the finnish diet: Ii trends in dietary sodium intake and comparison between intake and 24-h excretion of sodium. Eur. J. Clin. Nutr. 2006, 60, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Hyun, Y.Y.; Lee, K.-B.; Han, S.H.; Kim, Y.H.; Kim, Y.-S.; Lee, S.W.; Oh, Y.K.; Chae, D.W.; Ahn, C. Nutritional status in adults with predialysis chronic kidney disease: Know-ckd study. J. Korean Med. Sci. 2017, 32, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.-R.; Park, S.K.; Jung, J.Y.; Kim, Y.H.; Oh, Y.K.; Yoo, T.H.; Sung, S. The prevalence and management of anemia in chronic kidney disease patients: Result from the korean cohort study for outcomes in patients with chronic kidney disease (know-ckd). J. Korean Med. Sci. 2017, 32, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Schwandt, A.; Denkinger, M.; Fasching, P.; Pfeifer, M.; Wagner, C.; Weiland, J.; Zeyfang, A.; Holl, R.W. Comparison of mdrd, ckd-epi, and cockcroft-gault equation in relation to measured glomerular filtration rate among a large cohort with diabetes. J. Diabetes Complicat. 2017, 31, 1376–1383. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CKD 1 (N = 3053) | Non-CKD 1 (N = 156,658) | p-Value | |
|---|---|---|---|
| N (%) | N (%) | ||
| Sex | |||
| Male | 1200 (39.3) | 52,680 (33.6) | <0.01 |
| Female | 1843 (60.7) | 103,978 (66.4) | |
| Marital status | |||
| Single | 466 (15.3) | 16,624 (10.6) | <0.01 |
| Married | 2426 (79.5) | 131,889 (84.2) | |
| Others | 161 (5.3) | 8145 (5.2) | |
| Education | |||
| Below middle school | 905 (29.6) | 26,265 (16.8) | <0.01 |
| High school | 1387 (45.4) | 86,169 (55.0) | |
| Higher than college | 699 (22.9) | 41,926 (26.8) | |
| Monthly household income (KRW) | |||
| <1,500,000 | 554 (18.2) | 14,705 (9.4) | <0.01 |
| 1,500,000–2,999,999 | 579 (19.0) | 26,275 (16.8) | |
| 3,000,000–3,999,999 | 836 (27.4) | 56,592 (36.1) | |
| ≥4,000,000 | 378 (12.4) | 33,472 (21.4) | |
| Regular exercise 2 | |||
| No | 1382 (45.3) | 74,342 (47.5) | 0.06 |
| Yes | 1660 (54.4) | 81,751 (52.2) | |
| Drinking | |||
| No | 1788 (58.6) | 78,378 (50.0) | <0.01 |
| Yes | 1249 (40.9) | 77,633 (49.6) | |
| Smoking | |||
| No | 1566 (51.3) | 61,049 (39.0) | <0.01 |
| Yes | 537 (17.6) | 20,572 (13.1) | |
| Passive smoking 3 | |||
| No | 2230 (73.0) | 107,865 (68.9) | <0.01 |
| Yes | 658 (21.6) | 40,542 (25.9) | |
| Hypertension 4 | |||
| No | 1234 (40.4) | 113,189 (72.2) | <0.01 |
| Yes | 1819 (59.6) | 43,469 (27.8) | |
| Diabetes 5 | |||
| No | 2448 (80.2) | 147,458 (94.1) | <0.01 |
| Yes | 605 (19.8) | 9200 (5.9) | |
| Use of dietary supplements | |||
| No | 2607 (85.4) | 139,902 (89.3) | <0.01 |
| Yes | 413 (13.5) | 15,636 (10.0) | |
| Mean (SD) | Mean (SD) | ||
| Age (year) | 60.58 (7.84) | 52.41 (8.28) | <0.01 |
| Height (cm) | 159.8 (8.48) | 160.5 (8.02) | <0.01 |
| Weight (kg) | 63.63 (10.32) | 61.77 (9.92) | <0.01 |
| Body Mass Index (BMI) (kg/m2) | 24.83 (3.02) | 23.90 (2.90) | <0.01 |
| Albumin (g/dL) | 4.60 (0.33) | 4.64 (0.27) | <0.01 |
| Protein intake (g) | 56.02 (24.04) | 60.36 (27.52) | <0.01 |
| Creatinine (mg/dL) | 1.40 (0.96) | 0.81 (0.16) | <0.01 |
| Uric acid (mg/dL) | 6.11 (1.76) | 4.68 (1.26) | <0.01 |
| Total cholesterol (mg/dL) | 199.6 (39.41) | 197.9 (35.22) | 0.02 |
| Mineral Intake | Non-CKD 1 (n= 156,658) | Early stage CKD 2 (n = 2573) | Advanced stage CKD 2 (n = 480) | ||
|---|---|---|---|---|---|
| n (%) | n (%) | OR (95% CI) 3 | n (%) | OR (95% CI) 3 | |
| Calcium (mg/day) | |||||
| Q1 (<273.37) | 39,057 (24.9) | 715 (27.8) | 0.93 (0.79–1.08) | 155 (32.3) | 1.27 (0.88–1.82) |
| Q2 (273.38–401.36) | 39,169 (25.0) | 622 (24.2) | 0.94 (0.82–1.08) | 137 (28.5) | 1.33 (0.96–1.85) |
| Q3 (401.37–567.66) | 39,206 (25.0) | 623 (24.2) | 0.95 (0.83–1.08) | 99 (20.6) | 1.05 (0.76–1.45) |
| Q4 (≥567.67) | 39,226 (25.0) | 613 (23.8) | Reference | 89 (18.5) | Reference |
| Phosphorus (mg/day) | |||||
| Q1 (<663.68) | 39,004 (24.9) | 739 (28.7) | 1.04 (0.92–1.17) | 184 (38.3) | 1.64 (1.25–2.15) |
| Q2 (663.69–844.27) | 39,173 (25.0) | 646 (25.1) | Reference | 109 (22.7) | Reference |
| Q3 (844.28–1067.44) | 39,186 (25.0) | 637 (24.8) | 1.12 (0.95–1.32) | 105 (21.9) | 1.07 (0.72–1.59) |
| Q4 (≥1067.45) | 39,295 (25.1) | 551 (21.4) | 1.06 (0.87–1.29) | 82 (17.1) | 0.87 (0.54–1.38) |
| Sodium (mg/day) | |||||
| Q1 (<1541.09) | 39,089 (25.0) | 696 (27.1) | 1.02 (0.90–1.15) | 142 (29.6) | 0.96 (0.74–1.24) |
| Q2 (1541.10–2350.69) | 39,163 (25.0) | 630 (24.5) | Reference | 135 (28.1) | Reference |
| Q3 (2350.70–3260.41) | 39,218 (25.0) | 595 (23.1) | 0.93 (0.82–1.05) | 115 (24.0) | 0.94 (0.71–1.22) |
| Q4 (≥3260.42) | 39,188 (25.0) | 652 (25.3) | 1.02 (0.89–1.15) | 88 (18.3) | 0.74 (0.54–1.00) |
| Potassium (mg/day) | |||||
| Q1 (<1567.53) | 39,015 (24.9) | 731 (28.4) | 1.02 (0.86–1.20) | 181 (37.7) | 1.86 (1.27–2.74) |
| Q2 (1567.54–2114.26) | 39,166 (25.0) | 650 (25.3) | 1.01 (0.87–1.17) | 112(23.3) | 1.27 (0.89–1.83) |
| Q3 (2114.27–2803.07) | 39,204 (25.0) | 618 (24.0) | 1.03 (0.90–1.17) | 106 (22.1) | 1.30 (0.94–1.79) |
| Q4 (≥2803.08) | 39,273 (25.1) | 574 (22.3) | Reference | 81 (16.9) | Reference |
| Iron (mg/day) | |||||
| Q1 (<6.93) | 38,992 (24.9) | 753 (29.3) | 1.04 (0.92–1.17) | 182 (37.9) | 1.53 (1.17–2.01) |
| Q2 (6.94–9.16) | 39,160 (25.0) | 659 (25.6) | Reference | 109 (22.7) | Reference |
| Q3 (9.17–12.12) | 39,202 (25.0) | 618 (24.0) | 1.02 (0.89–1.17) | 108 (22.5) | 1.08 (0.78–1.49) |
| Q4 (≥12.13) | 39,304 (25.1) | 543 (21.1) | 0.93 (0.79–1.09) | 81 (16.9) | 0.79 (0.54–1.16) |
| Zinc (mg/day) | |||||
| Q1 (<5.86) | 39,019 (24.9) | 729 (28.3) | 1.00 (0.84–1.19) | 178 (37.1) | 1.52 (1.02–2.25) |
| Q2 (5.87–7.37) | 39,136 (25.0) | 681 (26.5) | 1.02 (0.88–1.18) | 112 (23.3) | 1.06 (0.74–1.51) |
| Q3 (7.38–9.35) | 39,227 (25.0) | 604 (23.5) | Reference | 97 (20.2) | Reference |
| Q4 (≥9.36) | 39,276 (25.1) | 559 (21.7) | 1.00 (0.88–1.14) | 93 (19.4) | 0.96 (0.70–1.32) |
| Mineral Intake | Hypertension 4 (N = 45,288) | Non-Hypertension 4 (N = 114,423) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Non-CKD 1 (N = 43,469) | Early Stage CKD 2 (N = 1457) | Advanced Stage CKD 2 (N = 362) | Non-CKD 1 (N = 113,189) | Early Stage CKD 2 (N = 1116) | Advanced Stage CKD 2 (N = 118) | |||||
| N (%) | N (%) | OR (95% CI) 3 | N (%) | OR (95% CI) 3 | N (%) | N (%) | OR (95% CI) 3 | N (%) | OR (95% CI) 3 | |
| Phosphorus (mg/day) | ||||||||||
| Q1 (<663.68) | 11,299 (26.0) | 432 (29.6) | 1.08 (0.92–1.25) | 152 (42.0) | 1.79 (1.34–2.39) | 27,705 (24.5) | 307 (27.5) | 0.94 (0.80–1.12) | 32 (27.1) | 1.03 (0.60–1.74) |
| Q2 (663.69–844.27) | 11,099 (25.5) | 358 (24.6) | Reference | 81 (22.4) | Reference | 28,074 (24.8) | 288 (25.8) | Reference | 28 (23.7) | Reference |
| Q3 (844.28–1067.44) | 10,754 (24.7) | 348 (23.9) | 1.11 (0.90–1.36) | 71 (19.6) | 0.96 (0.62–1.49) | 28,432 (25.1) | 289 (25.9) | 1.20 (0.96–1.50) | 34 (28.8) | 1.10 (0.56–2.19) |
| Q4 (≥1067.45) | 10,317 (23.7) | 319 (21.9) | 1.14 (0.89–1.46) | 58 (16.0) | 0.82 (0.49–1.37) | 28,978 (25.6) | 232 (20.8) | 1.07 (0.81–1.41) | 24 (20.3) | 0.84 (0.38–1.89) |
| P-interaction | 0.45 | <0.01 | ||||||||
| Potassium (mg/day) | ||||||||||
| Q1 (<1567.53) | 11,506 (26.5) | 427 (29.3) | 0.97 (0.79–1.20) | 148 (40.9) | 1.83 (1.21–2.78) | 27,509 (24.3) | 304 (27.2) | 0.97 (0.77–1.23) | 33 (28.0) | 1.28 (0.63–2.62) |
| Q2 (1567.54–2114.26) | 10,957 (25.2) | 361 (24.8) | 0.95 (0.79–1.15) | 84 (23.2) | 1.18 (0.80–1.76) | 28,209 (24.9) | 289 (25.9) | 1.05 (0.85–1.29) | 28 (23.7) | 1.16 (0.62–2.19) |
| Q3 (2114.27–2803.07) | 10,542 (24.2) | 340 (23.3) | 0.97 (0.83–1.14) | 73 (20.2) | 1.17 (0.82–1.68) | 28,662 (25.3) | 278 (24.9) | 1.09 (0.91–1.31) | 33 (28.0) | 1.35 (0.78–2.32) |
| Q4 (≥2803.08) | 10,464 (24.1) | 329 (22.6) | Reference | 57 (15.8) | Reference | 28,809 (25.4) | 245 (21.9) | Reference | 24 (20.3) | Reference |
| P-interaction | 0.61 | <0.01 | ||||||||
| Iron (mg/day) | ||||||||||
| Q1 (<6.93) | 11,359 (26.1) | 429 (29.4) | 1.04 (0.89–1.21) | 152 (42.0) | 1.71 (1.28–2.28) | 27,633 (24.4) | 324 (29.0) | 1.02 (0.86–1.21) | 30 (25.4) | 1.01 (0.59–1.75) |
| Q2 (6.94–9.16) | 10,947 (25.2) | 367 (25.2) | Reference | 83 (22.9) | Reference | 28,213 (24.9) | 292 (26.2) | Reference | 26 (22.0) | Reference |
| Q3 (9.17–12.12) | 10,797 (24.8) | 340 (23.3) | 1.01 (0.85–1.20) | 69 (19.1) | 0.91 (0.63–1.31) | 28,405 (25.1) | 278 (24.9) | 1.02 (0.84–1.23) | 39 (33.0) | 1.62 (0.92–2.84) |
| Q4 (≥12.13) | 10,366 (23.9) | 321 (22.0) | 1.02 (0.84–1.25) | 58 (16.0) | 0.80 (0.53–1.23) | 28,938 (25.6) | 222 (19.9) | 0.84 (0.67–1.05) | 23 (19.5) | 1.02 (0.51–2.02) |
| P-interaction | 0.53 | <0.01 | ||||||||
| Zinc (mg/day) | ||||||||||
| Q1 (<5.86) | 11,216 (25.8) | 432 (29.6) | 1.16 (0.93–1.43) | 146 (40.3) | 1.85 (1.19–2.88) | 27,804 (24.6) | 297 (26.6) | 0.82 (0.65–1.03) | 32 (27.1) | 0.82 (0.40–1.68) |
| Q2 (5.87–7.37) | 10,993 (25.3) | 379 (26.0) | 1.11 (0.92–1.34) | 86 (23.8) | 1.20 (0.80–1.79) | 28,142 (24.9) | 302 (27.1) | 0.93 (0.76–1.14) | 26 (22.0) | 0.77 (0.40–1.47) |
| Q3 (7.38–9.35) | 10,855 (25.0) | 334 (22.9) | Reference | 68 (18.8) | Reference | 28,372 (25.1) | 270 (24.2) | Reference | 29 (24.6) | Reference |
| Q4 (≥9.36) | 10,405 (23.9) | 312 (21.4) | 1.03 (0.87–1.21) | 62 (17.1) | 0.95 (0.67–1.37) | 28,871 (25.5) | 247 (22.1) | 1.01 (0.84–1.21) | 31 (26.3) | 1.22 (0.71–2.07) |
| P-interaction | 0.59 | <0.01 | ||||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Lee, J.; Kim, K.-N.; Oh, K.-H.; Ahn, C.; Lee, J.; Kang, D.; Park, S.K. Association between Dietary Mineral Intake and Chronic Kidney Disease: The Health Examinees (HEXA) Study. Int. J. Environ. Res. Public Health 2018, 15, 1070. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061070
Kim J, Lee J, Kim K-N, Oh K-H, Ahn C, Lee J, Kang D, Park SK. Association between Dietary Mineral Intake and Chronic Kidney Disease: The Health Examinees (HEXA) Study. International Journal of Environmental Research and Public Health. 2018; 15(6):1070. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061070
Chicago/Turabian StyleKim, Jeewoo, Juyeon Lee, Kyoung-Nam Kim, Kook-Hwan Oh, Curie Ahn, Jongkoo Lee, Daehee Kang, and Sue K. Park. 2018. "Association between Dietary Mineral Intake and Chronic Kidney Disease: The Health Examinees (HEXA) Study" International Journal of Environmental Research and Public Health 15, no. 6: 1070. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061070