Translation of the Child and Adolescent HARDSHIP (Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation) Questionnaire into the Lithuanian Language and Validation of Its HRQoL (Headache-Related Quality of Life) Scale



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. The HARDSHIP Questionnaire and HRQoL Scale
2.3. Translation of the Child and Adolescent HARDSHIP Questionnaires
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Descriptive Statistics of the HRQoL Scale
3.3. Internal Consistency
3.4. Discriminant Validity
3.5. Test-Retest Reliability
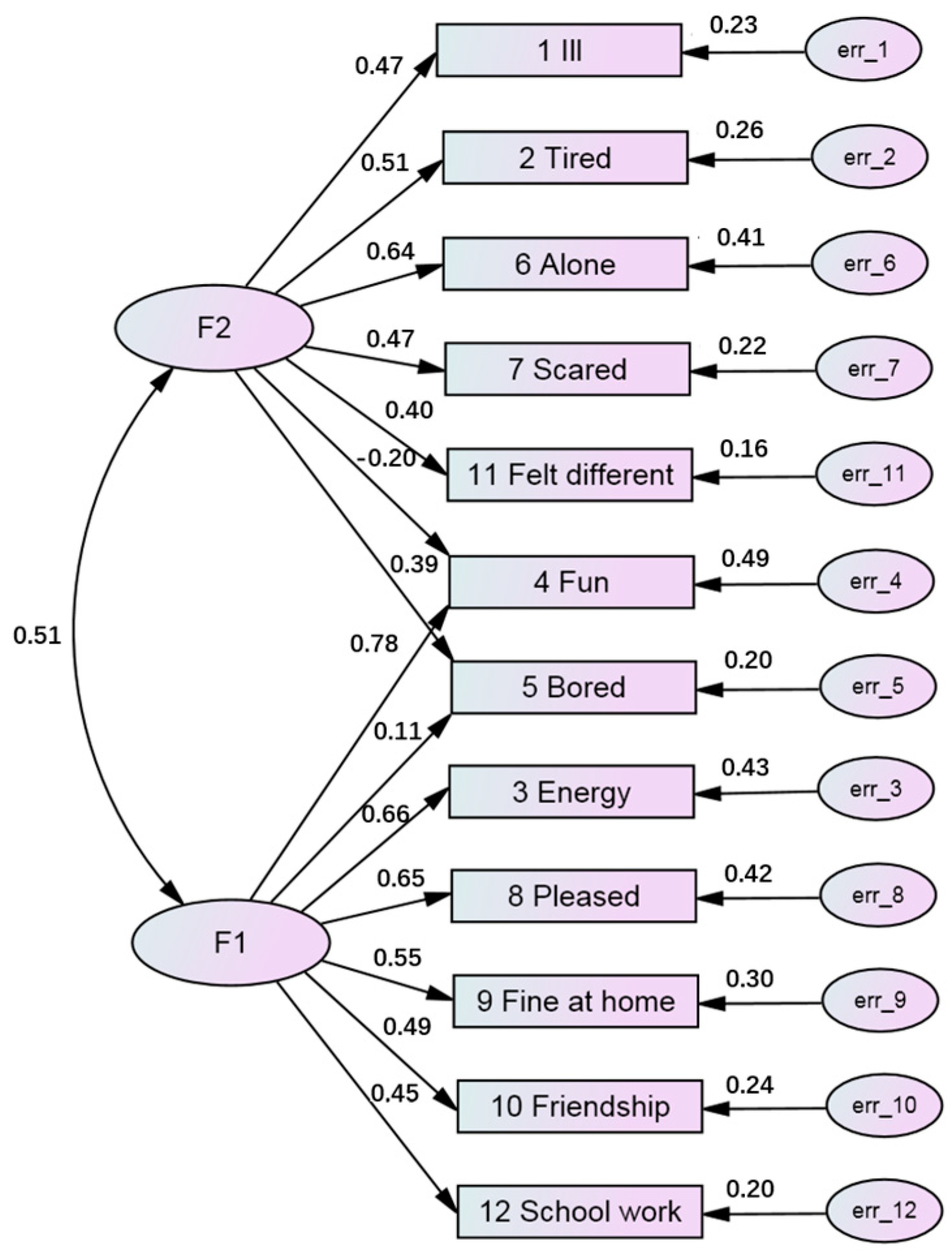
3.6. Factor Analysis
4. Discussion
4.1. Lithuanian Version of the Child and Adolescent HARDSHIP Questionnaires
4.2. Psychometric Characteristics of the HRQoL Scale
4.3. The Extent of Burden of Headache in Schoolchildren in Lithuania
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| HRQoL | Quality of Life |
| PedsQLI | Pediatric Quality of Life Inventory |
| HARDSHIP | Headache-attributed restriction, disability, social handicap and impaired participation |
| SPSS | The Statistical Package for the Social Sciences |
| EFA | Explanatory Factorial Analysis |
| KMO | Kaiser-Meyer-Olkin |
| CFA | Confirmatory factor analysis |
| CFI | Comparative Fit Index |
| TLI | Tucker–Lewis Index |
| RMSEA | Root Mean Square Error of Approximation |
| ICC | Intraclass Correlation Coefficient |
| SEM | Structural Equation Modeling |
| WHO-5 | World Health Organization Well-Being Index |
References
- Steiner, T.J.; Stovner, L.J.; Katsarava, Z.; Lainez, J.M.; Lampl, C.; Lantéri-Minet, M.; Rastenyte, D.; Ruiz de la Torre, E.; Tassorelli, C.; Barré, J.; et al. The impact of headache in Europe: Principal results of the Eurolight project. J. Headache Pain 2014, 15, 31. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abate, K.H.; Abd-Allah, F. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Blume, H.K. Childhood Headache: A Brief Review. Pediatr. Ann. 2017, 46, e155–e165. [Google Scholar] [CrossRef] [PubMed]
- Wöber-Bingöl, Ç.; Wöber, C.; Uluduz, D.; Uygunoğlu, U.; Aslan, T.S.; Kernmayer, M.; Zesch, H.E.; Gerges, N.T.A.; Wagner, G.; Siva., A.; et al. The global burden of headache in children and adolescents—Developing a questionnaire and methodology for a global study. J. Headache Pain 2014, 15, 86. [Google Scholar]
- Abu-Arafeh, I.; Razak, S.; Sivaraman, B.; Graham, C. Prevalence of headache and migraine in children and adolescents: A systematic review of population-based studies. Dev. Med. Child. Neurol. 2010, 52, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Antonaci, F.; Voiticovschi-Iosob, C.; Di Stefano, A.L.; Galli, F.; Ozge, A.; Balottin, U. The evolution of headache from childhood to adulthood: A review of the literature. J. Headache Pain 2014, 15, 15. [Google Scholar] [CrossRef] [PubMed]
- Wöber-Bingöl, Ç. Epidemiology of migraine and headache in children and adolescents. Curr. Pain 2013, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Straube, A.; Heinen, F.; Ebinger, F.; von Kries, R. Headache in school children: Prevalence and risk factors. Dtsch. Arztebl. Int. 2013, 110, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Kernick, D.; Reinhold, D.; Campbell, J.L. Impact of headache on young people in a school population. Br. J. Gen. Pract. 2009, 59, 678–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Januškevičienė, A.; Vaitkaitienė, E.; Zaborskis, A. Headache in school age children, comorbid fatigue and quality of life. Vaikų Pulmonologija ir Alergologija 2013, XVII, 68–79. (In Lithuanian) [Google Scholar]
- Stovner, L.J.; Al Jumah, M.; Birbeck, G.L.; Gururaj, G.; Jensen, R.; Katsarava, Z.; Queiroz, L.P.; Scher, A.I.; Tekle-Haimanot, R.; Wang, S.J.; et al. The methodology of population surveys of headache prevalence, burden and cost: Principles and recommendations from the Global Campaign against Headache. J. Headache Pain 2014, 15, 5. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.J. World Headache Alliance: Lifting the burden: The global campaign against headache. Lancet. Neurol. 2004, 3, 204–205. [Google Scholar] [CrossRef]
- Steiner, T.J.; Gururaj, G.; Andrée, C.; Katsarava, Z.; Ayzenberg, I.; Yu, S.Y.; Al Jumah, M.; Tekle-Haimanot, R.; Birbeck, G.L.; Herekar, A.; et al. Diagnosis, prevalence estimation and burden measurement in population surveys of headache: Presenting the HARDSHIP questionnaire. J. Headache Pain 2014, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- KINDL®. Revised Questionnaire to Assess Health-Related Quality of Life in Children and Adolescents. Available online: http://kindl.org/english/ (accessed on 27 June 2018).
- Jorgensen, J.E.; McGirr, K.A.; Korsgaard, H.O.; Rathleff, M.S. Translation and validation of the Child and the Adolescent HARDSHIP (Headache-atributed restriction, disability, social handicap and impaired participation) questionnaire into Danish language. Peer J. 2016, 4, e1927. [Google Scholar] [CrossRef] [PubMed]
- Lifting the Burden. The Global Campaign Against Headache. Available online: http://www.l-t-b.org/index.cfm/spKey/people.child_adolescent_burden.html (accessed on 27 June 2018).
- Lifting the Burden. The Global Campaign Against Headache. Translation Protocols. Available online: http://www.l-t-b.org/index.cfm/spKey/people.translation_protocols.html (accessed on 27 June 2018).
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation and cultural adaption process for patient-reported outcomes (PRO) measures: Report of the ISPOR task force for translation and cultural adaption. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, J.L. IBM SPSS AMOS 21 User’s Guide; Amos Development Corporation: Mount Pleasant, SC, USA, 2012. [Google Scholar]
- Albright, J.J. Confirmatory Factor Analysis Using AMOS, LISREL and MPLUS. The Trustees of Indiana University 2006–2008. Available online: http://www.iu.edu/~statmath/stat/all/cfa/cfa2008.pdf (accessed on 27 June 2018).
- Schmitt, T.A. Current methodological considerations in exploratory and confirmatory factor analysis. J. Psychoeduc. Ass. 2011, 29, 304–321. [Google Scholar] [CrossRef]
- Streiner, D.; Norman, G. Health Measurement Scales. A practical Guide to their Development and Use, 2nd ed.; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Whiston, S.C. Principles and Applications of Assessment in Counselling, 3rd ed.; Cengage Learning: Boston, MA, USA, 2009. [Google Scholar]
- Aldridge, V. Reliability Assessment Using SPSS. University of York, Centre for Applied Statistics Courses, UCL Institute of Child Health. 2015. Available online: http://www.spssusers.co.uk/Events/2015/ALDRIDGE2015.pdf (accessed on 27 June 2018).
- Rothman, M.L.; Beltran, P.; Cappelleri, J.C.; Lipscomb, J.; Teschendorf, B.; the Mayo/FDA Patient-Reported Outcomes Consensus Meeting Group. Patient-Reported Outcomes: Conceptual Issues. Value Health 2007, 10, S66–S75. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Fenny, D.; Patrick, D. Issues in quality-of-life measurement in clinical trials. Control Clin. Trial. 1991, 12, 81S–90S. [Google Scholar] [CrossRef]
- Houle, T.T.; Turner, D.P.; Houle, T.A.; Smitherman, T.A.; Martin, V.; Penzien, D.B.; Lipton, R.B. Rounding behavior in the reporting of headache frequency complicates headache chronification research. Headache 2013, 53, 908–919. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994; Chapter 7. [Google Scholar]
- Wöber, C.; Wöber-Bingöl, Ç.; Uluduz, D.; Aslan, T.S.; Uygunoglu, U.; Tüfekçi, A.; Alp, S.I.; Duman, T.; Sürgün, F.; Emir, G.K.; et al. Undifferentiated headache: Broadening the approach to headache in children and adolescents, with supporting evidence from a nationwide school-based cross-sectional survey in Turkey. J. Headache Pain 2018, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- The WHO-5 Website. Available online: https://www.psykiatri-regionh.dk/who-5/who-5-questionnaires/Pages/default.aspx (accessed on 27 June 2018).
- Allgaier, A.K.; Pietsch, K.; Frühe, B.; Prast, E.; Sigl-Glöckner, J.; Schulte-Körne, G. Depression in pediatric care: is the WHO-Five Well-Being Index a valid screening instrument for children and adolescents? Gen. Hosp. Psychiatry 2012, 34, 234–241. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Item Code | Specified Event |
|---|---|
| 1 Ill | I felt ill |
| 2 Tired | I was tired and worn-out |
| 3 Energy | I felt full of energy |
| 4 Fun | I had fun and laughed a lot |
| 5 Bored | I was bored |
| 6 Alone | I felt alone |
| 7 Scared | I was scared |
| 8 Pleased | I felt pleased with myself |
| 9 Fine at home | I felt fine at home |
| 10 Friendship | I got along with my friends |
| 11 Felt different | I felt different from other children |
| 12 School work | Doing my schoolwork was easy |
| Characteristics | Gender | Age Group | Total Sample (N = 2505) | |||||
|---|---|---|---|---|---|---|---|---|
| Boys (n = 1169) | Girls (n = 1336) | p-Value a | 7–11 (n = 1382) | 12–17 (n = 1123) | p-Value a | |||
| Headache in life | 90.8 | 93.4 | 0.014 | 88.6 | 96.6 | <0.001 | 92.2 | |
| Headache in the last year | 67.8 | 79.7 | <0.001 | 62.7 | 88.3 | <0.001 | 74.2 | |
| Headache in the last week | 50.3 | 65.5 | <0.001 | 54.6 | 62.9 | <0.001 | 59.0 | |
| Have taken pills or medication due to headache | 22.7 | 32.4 | <0.001 | 24.8 | 31.2 | 0.002 | 28.3 | |
| Duration of headache | no pain | 32.2 | 20.3 | <0.001 | 37.3 | 11.7 | <0.001 | 25.8 |
| less than hour | 37.4 | 40.0 | 0.182 | 39.9 | 37.3 | 0.183 | 38.8 | |
| 1-2 h | 17.4 | 25.5 | <0.001 | 13.8 | 31.4 | <0.001 | 21.7 | |
| 2.1-4 h | 8.4 | 9.1 | 0.536 | 5.3 | 13.0 | <0.001 | 8.7 | |
| more than 4 h | 4.7 | 5.2 | 0.569 | 3.6 | 6.6 | 0.001 | 5.0 | |
| p-value b | <0.001 | <0.001 | ||||||
| Severity of headache | no pain | 32.2 | 20.3 | <0.001 | 37.3 | 11.7 | <0.001 | 25.8 |
| not bad | 33.7 | 33.0 | 0.711 | 28.7 | 39.1 | <0.001 | 33.4 | |
| quite bad | 30.8 | 41.8 | <0.001 | 29.7 | 45.2 | <0.001 | 36.6 | |
| very bad | 3.3 | 4.9 | 0.043 | 4.3 | 4.0 | 0.708 | 4.2 | |
| p-value b | <0.001 | <0.001 | ||||||
| Item | Never (0) | Seldom (1) | Often (2) | Always (3) | Distribution Asymmetry a (%) | Corrected Item-Total Correlation |
|---|---|---|---|---|---|---|
| 1 Ill b | 32.6 | 56.8 | 8.9 | 1.6 | −39.4 | 0.312 |
| 2 Tired b | 17.8 | 52.6 | 24.4 | 5.1 | −20.4 | 0.342 |
| 3 Energy | 12.7 | 34.0 | 36.4 | 17.0 | +3.3 | 0.482 |
| 4 Fun | 9.5 | 26.7 | 40.1 | 23.7 | +13.8 | 0.448 |
| 5 Bored b | 28.0 | 56.9 | 11.5 | 3.6 | −34.9 | 0.385 |
| 6 Alone b | 56.6 | 31.7 | 8.0 | 3.7 | −38.3 | 0.417 |
| 7 Scared b | 58.8 | 34.4 | 4.9 | 1.9 | −40.5 | 0.284 |
| 8 Pleased | 12.7 | 33.3 | 33.7 | 20.3 | +4.0 | 0.500 |
| 9 Fine at home | 3.9 | 12.6 | 24.4 | 59.2 | +33.5 | 0.413 |
| 10 Friendship | 2.5 | 13.6 | 36.2 | 47.7 | +33.9 | 0.391 |
| 11 Felt different b | 39.9 | 37.6 | 13.1 | 9.3 | −27.5 | 0.242 |
| 12 School work | 12.9 | 43.0 | 30.0 | 14.1 | −5.9 | 0.377 |
| Group | n | Mean | SD | Median | p-Value * |
|---|---|---|---|---|---|
| Total | 2505 | 24.23 | 5.13 | 25 | |
| Boys | 1169 | 24.86 | 4.95 | 25 | <0.001 |
| Girls | 1336 | 23.68 | 5.23 | 24 | |
| 7–11 years | 1382 | 24.49 | 5.36 | 25 | 0.001 |
| 12–17 years | 1123 | 23.91 | 4.83 | 24 |
| Occurrence and Character of Headache | n | Mean | SD | Median | p-Value a | |
|---|---|---|---|---|---|---|
| Headache | in the last year | 1858 | 23.68 | 4.68 | 24 | <0.001 |
| no headache | 647 | 25.82 | 5.17 | 26 | ||
| Duration | more than 4 h | 124 | 21.58 | 5.89 | 22 | <0.001 |
| about 2–4 h | 219 | 22.24 | 5.22 | 22 | <0.001 | |
| about 1 h | 544 | 23.02 | 5.06 | 23 | <0.001 | |
| about half hour | 971 | 24.63 | 4.92 | 25 | <0.001 | |
| no headache | 647 | 25.82 | 4.68 | 26 | - | |
| Severity | very bad | 647 | 21.16 | 6.14 | 21 | <0.001 |
| quite bad | 918 | 22.59 | 5.19 | 23 | <0.001 | |
| not bad | 835 | 25.19 | 4.56 | 26 | 0.006 | |
| no headache | 647 | 25.82 | 5.17 | 26 | - | |
| Item b | Component c | |
|---|---|---|
| 1 | 2 | |
| 8 Pleased | 0.785 | −0.036 |
| 4 Fun | 0.763 | −0.101 |
| 3 Energy | 0.734 | −0.040 |
| 9 Fine at home | 0.588 | 0.026 |
| 10 Friendship | 0.532 | 0.018 |
| 12 School work | 0.477 | 0.136 |
| 6 Alone | 0.040 | 0.672 |
| 2 Tired | 0.011 | 0.653 |
| 1 Ill | −0.039 | 0.606 |
| 7 Scared | −0.060 | 0.570 |
| 11 Felt different | −0.080 | 0.556 |
| 5 Bored | 0.245 | 0.481 |
| Estimates | |||
|---|---|---|---|
| Randomly Selected Sub-group of the Entire Sample (N = 1252) | No Headache in the Last Year (N = 647) | Headache in the Last Year (N = 1858) | |
| Standardized regression weights (factor loadings) and direction of associations: | |||
1 Ill  F2 F2 | 0.474 | 0.355 | 0.493 |
| 2 Tired F2 | 0.513 | 0.392 | 0.552 |
| 6 Alone F2 | 0.642 | 0.508 | 0.632 |
| 7 Scared F2 | 0.471 | 0.510 | 0.447 |
| 11 Felt different F2 | 0.401 | 0.406 | 0.391 |
| 4 Fun F2 | –0.200 | –0.080 | –0.152 |
| 4 Fun F1 | 0.783 | 0.592 | 0.771 |
| 5 Bored F2 | 0.387 | 0.329 | 0.403 |
| 5 Bored F1 | 0.107 | 0.158 | 0.153 |
| 3 Energy F1 | 0.658 | 0.543 | 0.681 |
| 8 Pleased F1 | 0.652 | 0.616 | 0.697 |
| 9 Fine at home F1 | 0.549 | 0.523 | 0.511 |
| 10 Friendship F1 | 0.492 | 0.553 | 0.439 |
| 12 School work F1 | 0.448 | 0.420 | 0.425 |
| Correlations | |||
F1  F2 F2 | 0.509 | 0.384 | 0.445 |
| Model fit estimates | |||
| Chi-squared | 246.2 | 80.0 | 513.7 |
| DF | 51 | 51 | 51 |
| Chi-squared/DF | 4.828 | 1.569 | 10.072 |
| p-value | <0.001 | - | < 0.001 |
| TLI | 0.901 | 0.956 | 0.852 |
| CFI | 0.924 | 0.966 | 0.886 |
| RAMSEA (90% CI) | 0.055 (0.048–0.062) | 0.030 (0.016–0.042) | 0.070 (0.064–0.075) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genc, D.; Zaborskis, A.; Vaičienė-Magistris, N. Translation of the Child and Adolescent HARDSHIP (Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation) Questionnaire into the Lithuanian Language and Validation of Its HRQoL (Headache-Related Quality of Life) Scale. Int. J. Environ. Res. Public Health 2018, 15, 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081579
Genc D, Zaborskis A, Vaičienė-Magistris N. Translation of the Child and Adolescent HARDSHIP (Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation) Questionnaire into the Lithuanian Language and Validation of Its HRQoL (Headache-Related Quality of Life) Scale. International Journal of Environmental Research and Public Health. 2018; 15(8):1579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081579
Chicago/Turabian StyleGenc, Diana, Apolinaras Zaborskis, and Nerija Vaičienė-Magistris. 2018. "Translation of the Child and Adolescent HARDSHIP (Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation) Questionnaire into the Lithuanian Language and Validation of Its HRQoL (Headache-Related Quality of Life) Scale" International Journal of Environmental Research and Public Health 15, no. 8: 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081579