Age, Period, and Cohort Effects on Suicide Mortality in South Korea, 1992–2015

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Analysis
3. Results
3.1. Trends in Suicide Rates
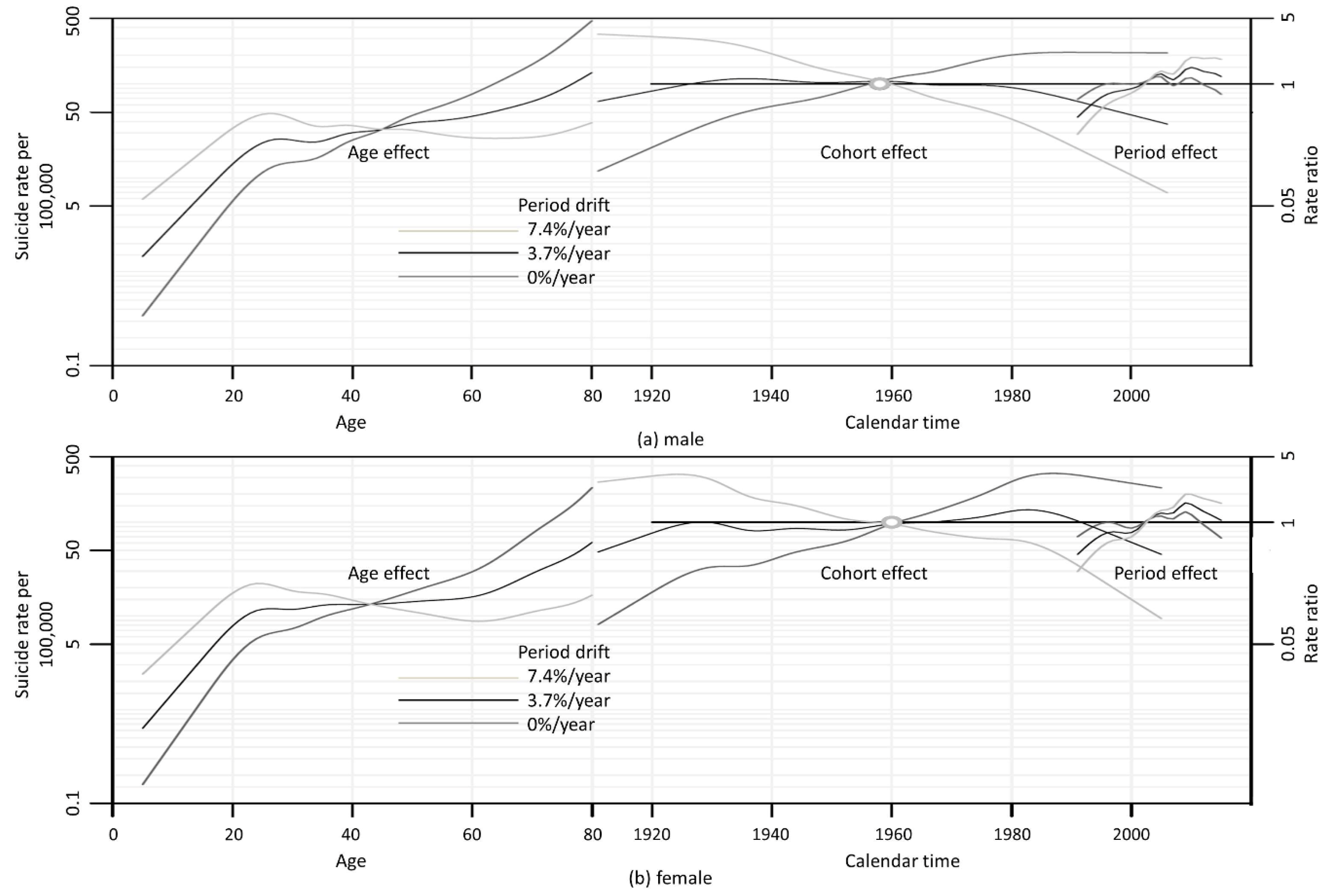
3.2. APC Effects
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- OECD Health at a Glance 2015: OECD Indicators. Available online: http://www.oecd.org/health/healthdata (accessed on 1 June 2018).
- Khang, Y.-H.; Lynch, J.W.; Kaplan, G.A. Impact of economic crisis on cause-specific mortality in South Korea. Int. J. Epidemiol. 2005, 34, 1291–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD Society at a Glance 2016. A Spotlight on Youth: How Does KOREA Compare? Available online: https://www.oecd.org/korea/sag2016-korea.pdf (accessed on 8 June 2018).
- Park, C.; Jee, Y.H.; Jung, K.J. Age-period-cohort analysis of the suicide rate in Korea. J. Affect. Disord. 2016, 194, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.Y.; Reither, E.N.; Masters, R.K. A population-based analysis of increasing rates of suicide mortality in Japan and South Korea, 1985–2010. BMC Public Health 2016, 16, 356. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.-W.; Chun, H.; Cho, S.-I. A closer look at the increase in suicide rates in South Korea from 1986–2005. BMC Public Health 2009, 9, 72. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Nishimura, Y.; Nishida, A.; Fukunaga, T.; Masaki, M.; Fujita, Y.; Nata, M.; Okazaki, Y.; Ono, Y. Relationships between suicide and three economic factors in South Korea. Leg. Med. 2010, 12, 100–101. [Google Scholar] [CrossRef] [PubMed]
- Park, B.B.; Lester, D. Social integration and suicide in South Korea. Crisis 2006, 27, 48–50. [Google Scholar] [CrossRef] [PubMed]
- Koo, C.Y.; Kim, J.S.; Yu, J. A study on factors influencing elders’ suicidal ideation: Focused on comparison of gender differences. J. Korean Acad. Community Health Nurs. 2014, 25, 24–32. [Google Scholar] [CrossRef]
- Kim, H.; Sohn, Y. A study on the characteristics of elderly suicide and suicidal type. Korean J. Psychol. Soc. Issues 2006, 12, 1–19. [Google Scholar]
- Chang, S.-S.; Gunnell, D.; Sterne, J.A.; Lu, T.-H.; Cheng, A.T. Was the economic crisis 1997–1998 responsible for rising suicide rates in East/Southeast Asia? A time–trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc. Sci. Med. 2009, 68, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.; Jones, K. The impossibility of separating age, period and cohort effects. Soc. Sci. Med. 2013, 93, 163–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, L. Paradigm shift in age-period-cohort analysis: A response to Yang and Land, O’Brien, Held and Riebler, and Fienberg. Demography 2013, 50, 1985–1988. [Google Scholar] [CrossRef]
- Bopp, M.; Gostynski, M.; Lauber, C.; Gutzwiller, F.; Rössler, W. Age-period-cohort analysis of Swiss suicide data, 1881–2000. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 207–214. [Google Scholar]
- Morrell, S.; Page, A.; Taylor, R. Birth cohort effects in New South Wales suicide, 1865–1998. Acta Psychiatr. Scand. 2002, 106, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Richiardi, L.; Ekbom, A.; Pukkala, E.; Cuninkova, M.; Møller, H. Trends in testicular cancer incidence and mortality in 22 European countries: Continuing increases in incidence and declines in mortality. Int. J. Cancer 2006, 118, 3099–3111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO International Statistical Classification on Diseases and Related Health Problems 10th Revision. Available online: http://apps.who.int/classifications/icd10/browse/2016/en (accessed on 25 July 2018).
- Holford, T.R. Age-period-cohort analysis. In Encyclopedia of Biostastistics; John Wiley & Sons, Inc.: Chichester, UK, 1998; pp. 82–99. [Google Scholar]
- Carstensen, B. Age-period-cohort models for the Lexis diagram. Stat. Med. 2007, 26, 3018–3045. [Google Scholar] [CrossRef] [PubMed]
- Carroll, R.; Metcalfe, C.; Gunnell, D. Hospital presenting self-harm and risk of fatal and non-fatal repetition: Systematic review and meta-analysis. PLoS ONE 2014, 9, e89944. [Google Scholar] [CrossRef] [PubMed]
- Waern, M.; Rubenowitz, E.; Wilhelmson, K. Predictors of suicide in the old elderly. Gerontology 2003, 49, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Shulman, K. Suicide and parasuicide in old age: A review. Age Ageing 1978, 7, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.A. A changing epidemiology of suicide? The influence of birth cohorts on suicide rates in the United States. Soc. Sci. Med. 2014, 114, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Joiner, T.E., Jr.; Van Orden, K.A.; Witte, T.K.; Selby, E.A.; Ribeiro, J.D.; Lewis, R.; Rudd, M.D. Main predictions of the interpersonal–psychological theory of suicidal behavior: Empirical tests in two samples of young adults. J. Abnorm. Psychol. 2009, 118, 634–646. [Google Scholar] [CrossRef] [PubMed]
- Odagiri, Y.; Uchida, H.; Nakano, M. Gender differences in age, period, and birth-cohort effect on suicide mortality rate in Japan 1985–2006. Asia-Pac. J. Public Health 2009, 23, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Moon, H. The role of social pensions in Korea. In Proceedings of the World Bank-MOF-Hitotsubashi Workshop, on Closing the Coverage Gap: The Role of Social Pension, Tokyo, Japan, 20–22 February 2008. [Google Scholar]
- Supreme Court of Korea Judicial Crime Statistics. Available online: https://www.scourt.go.kr/portal/justicesta/JusticestaListAction.work?gubun=10 (accessed on 8 June 2018).
- Ross, M.; Clayer, J.; Campbell, R. Parental rearing patterns and suicidal thoughts. Acta Psychiatr. Scand. 1983, 67, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Goldney, R.D. Parental representation in young women who attempt suicide. Acta Psychiatr. Scand. 1985, 72, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Benjaminsen, S.; Krarup, G.; Lauritsen, R. Personality, parental rearing behaviour and parental loss in attempted suicide: A comparative study. Acta Psychiatr. Scand. 1990, 82, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Qin, P.; Agerbo, E.; Westergård-Nielsen, N.; Eriksson, T.; Mortensen, P.B. Gender differences in risk factors for suicide in Denmark. Br. J. Psychiatry 2000, 177, 546–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehnvall, A.; Parker, G.; Hadzi-Pavlovic, D.; Malhi, G. Perception of rejecting and neglectful parenting in childhood relates to lifetime suicide attempts for females–but not for males. Acta Psychiatr. Scand. 2008, 117, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.H.; Caine, E.D.; You, S.; Fu, K.W.; Chang, S.S.; Yip, P.S.F. Suicide rates among working-age adults in South Korea before and after the 2008 economic crisis. J. Epidemiol. Community Health 2014, 68, 246–252. [Google Scholar] [CrossRef] [PubMed]
- OECD Society at a Glance 2016: Marriage and Divorce Rates. Available online: http://www.oecd.org/els/family/database.htm (accessed on 6 June 2018).
- Fu, K.-W.; Chan, C. A study of the impact of thirteen celebrity suicides on subsequent suicide rates in South Korea from 2005 to 2009. PLoS ONE 2013, 8, e53870. [Google Scholar] [CrossRef] [PubMed]
- Myung, W.; Lee, G.-H.; Won, H.-H.; Fava, M.; Mischoulon, D.; Nyer, M.; Kim, D.K.; Heo, J.-Y.; Jeon, H.J. Paraquat prohibition and change in the suicide rate and methods in South Korea. PLoS ONE 2015, 10, e0128980. [Google Scholar] [CrossRef] [PubMed]
- OECD Unemployment Rate. Available online: https://data.oecd.org/unemp/unemployment-rate.htm#indicator-chart (accessed on 17 July 2018).
- Cha, E.S.; Chang, S.-S.; Gunnell, D.; Eddleston, M.; Khang, Y.-H.; Lee, W.J. Impact of paraquat regulation on suicide in South Korea. Int. J. Epidemiol. 2015, 45, 470–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, C.H.; Caine, E.D.; Chang, S.S.; Lee, W.J.; Cha, E.S.; Yip, P.S.F. The impact of improving suicide death classification in South Korea: A comparison with Japan and Hong Kong. PLoS ONE 2015, 10, e0125730. [Google Scholar] [CrossRef] [PubMed] [Green Version]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Song, Y.-J.; Kim, J.; Ki, M.; Shin, J.-Y.; Kwon, Y.-M.; Lim, J. Age, Period, and Cohort Effects on Suicide Mortality in South Korea, 1992–2015. Int. J. Environ. Res. Public Health 2018, 15, 1580. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081580
Park S, Song Y-J, Kim J, Ki M, Shin J-Y, Kwon Y-M, Lim J. Age, Period, and Cohort Effects on Suicide Mortality in South Korea, 1992–2015. International Journal of Environmental Research and Public Health. 2018; 15(8):1580. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081580
Chicago/Turabian StylePark, Soonjoo, Yeong-Jun Song, Jinseob Kim, Myung Ki, Ji-Yeon Shin, Young-Man Kwon, and Jiseun Lim. 2018. "Age, Period, and Cohort Effects on Suicide Mortality in South Korea, 1992–2015" International Journal of Environmental Research and Public Health 15, no. 8: 1580. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081580