A Systematic Review of Sexual and Reproductive Health Knowledge, Experiences and Access to Services among Refugee, Migrant and Displaced Girls and Young Women in Africa

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
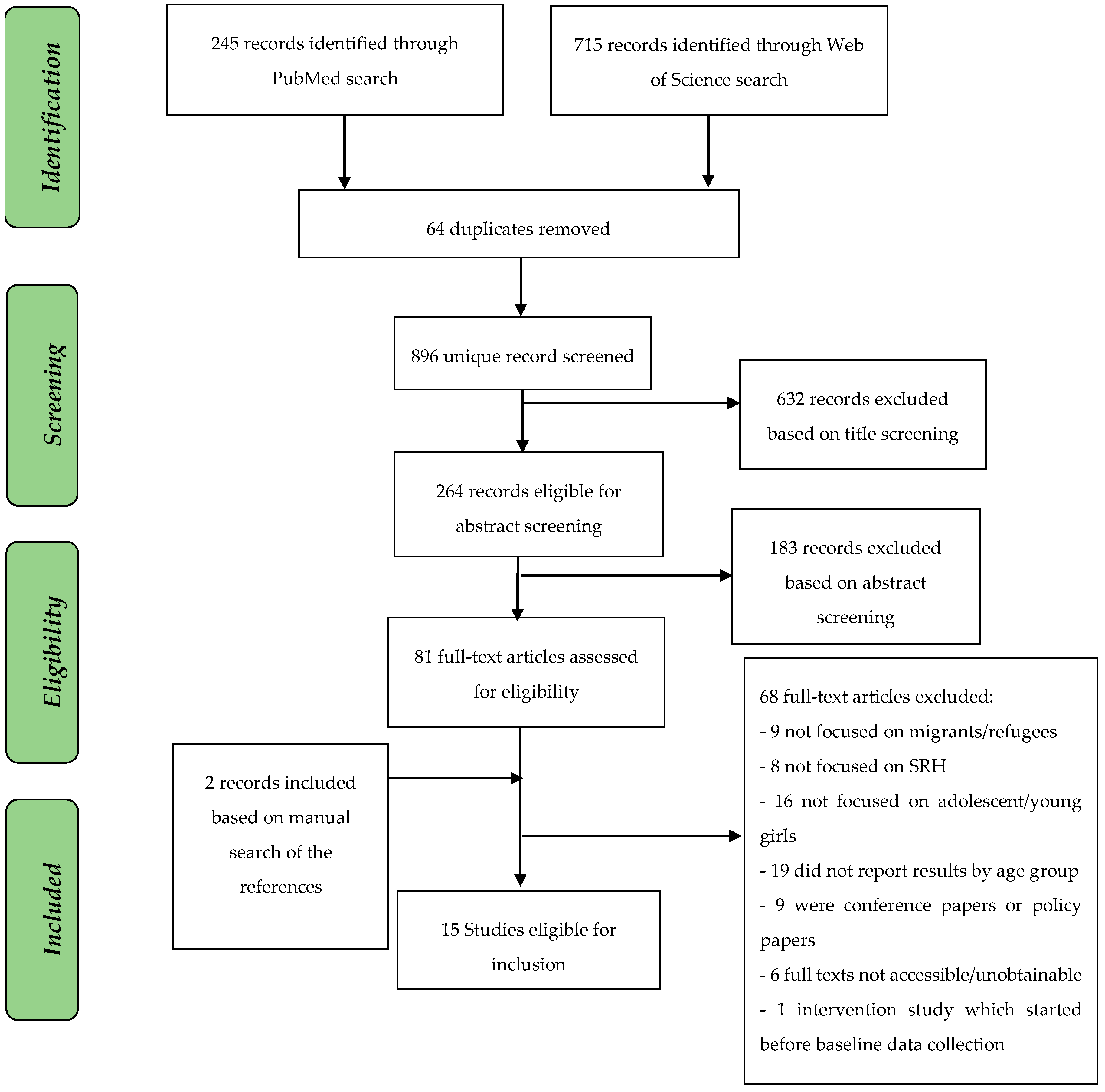
2.2. Study Selection
2.3. Critical Appraisal
2.4. Data Extraction and Analysis
3. Results
3.1. Study Characteristics
3.2. Sexual and Reproductive Health Knowledge
3.3. Sexual and Reproductive Health Experiences and Practices
3.4. Access to Sexual and Reproductive Health Services, Commodities and Information
3.5. Criticial Appraisal of Included Studies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AIDS | Acquired immune deficiency syndrome |
| HIV | Human immunodeficiency virus |
| IAWG | Inter-agency Working Group (IAWG) |
| IDP | Internally displaced people |
| FGD | Focus group discussion |
| MMAT | Mixed Methods Appraisal Tool |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| SRH | Sexual and reproductive health |
| STI | Sexually transmitted infection |
| UNFPA | United Nations Population Fund |
| UNHCR | The United Nations Refugee Agency |
References
- UNFPA; Save the Children USA. A Companion to the Inter-Agency Field Manual on Reproductive Health in Humanitarian Settings: A Companion to the Inter-Agency Field Manual on Reproductive Health in Humanitarian, 1st ed.; UNFPA: New York, NY, USA; Save the Children USA: Fairfield, CT, USA, 2009; pp. 1–92. [Google Scholar]
- Ward, J.; Marsh, M. Sexual Violence against Women and Girls in War and Its Aftermath: Realities, Responses, and Required Resources. Available online: http://www.svri.org/sites/default/files/attachments/2016-01-15/CCEF504C15AB277E852571AB0071F7CE-UNFPA.pdf (accessed on 15 May 2018).
- Jamieson, D.J.; Meikle, S.F.; Hillis, S.D.; Mtsuko, D.; Mawji, S.; Duerr, A. An evaluation of poor pregnancy outcomes among Burundian refugees in Tanzania. JAMA 2000, 3, 397–402. [Google Scholar] [CrossRef]
- Bartlett, L.A.; Jamieson, D.J.; Kahn, T.; Sultana, M.; Wilson, H.G.; Duerr, A. Maternal mortality among Afghan refugees in Pakistan, 1999–2000. Lancet 2002, 359, 643–649. [Google Scholar] [CrossRef]
- UNFPA. Adolescent Girls in Disaster & Conflict: Interventions for Improving Access to Sexual and Reproductive Health Services, 1st ed.; UNFPA: New York, NY, USA, 2016; pp. 1–88. [Google Scholar]
- Yakaremye, I.; Mukagatare, C. Forced migration and sexual abuse: Experience of congolese adolescent girls in Kigeme refugee camp, Rwanda. Health Psychol. Rep. 2016, 4, 261–271. [Google Scholar] [CrossRef]
- McGinn, T.; Austin, J.; Anfinson, K.; Amsalu, R.; Casey, S.E.; Fadulalmula, S.I.; Langston, A.; Lee-Jones, L.; Meyers, J.; Mubiru, F.K.; et al. Family planning in conflict: results of cross-sectional baseline surveys in three African countries. Confl. Health 2011, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- UNFPA. Inter-Agency Field Manual on Reproductive Health in Humanitarian Settings: 2010 Revision for Field Review, 1st ed.; Inter-Agency Working Group (IAWG) on Reproductive Health in Crises: New York, NY, USA, 2010; pp. 1–217. [Google Scholar]
- Casey, S.E. Evaluations of reproductive health programs in humanitarian settings: A systematic review. Confl. Health 2015, 9, S1. [Google Scholar] [CrossRef] [PubMed]
- UNHCR. Inter-Agency Global Evaluation of Reproductive Health Services for Refugees and Internally Displaced Persons. 2004. Available online: http://www.unhcr.org/41c846f44.pdf (accessed on 15 May 2018).
- Chynoweth, S.K. Advancing reproductive health on the humanitarian agenda: The 2012–2014 global review. Confl. Health. 2015, 9, I1. [Google Scholar] [CrossRef]
- Casey, S.E.; Chynoweth, S.K.; Cornier, N.; Gallagher, M.C.; Wheeler, E.E. Progress and gaps in reproductive health services in three humanitarian settings: Mixed-methods case studies. Confl. Health 2015, 9, S3. [Google Scholar] [CrossRef] [PubMed]
- Sandelowski, M.; Voils, C.I.; Barroso, J. Defining and designing mixed research synthesis studies. Res. Sch. 2006, 13, 29. [Google Scholar] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 151, 264–269. [Google Scholar]
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J.; Seller, R. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Casey, S.E.; Larsen, M.M.; McGinn, T.; Sartie, M.; Dauda, M.; Lahai, P. Changes in HIV/AIDS/STI knowledge, attitudes, and behaviours among the youth in Port Loko, Sierra Leone. Glob. Public Health 2006, 1, 249–263. [Google Scholar] [CrossRef] [PubMed]
- Feseha, G.; Gerbaba, M. Intimate partner physical violence among women in Shimelba refugee camp, northern Ethiopia. BMC Public Health 2012, 12, 125. [Google Scholar] [CrossRef] [PubMed]
- Gure, F.; Yusuf, M.; Foster, A.M. Exploring Somali women’s reproductive health knowledge and experiences: Results from focus group discussions in Mogadishu. Reprod. Health Matters 2015, 23, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Harrison, K.M.; Claass, J.; Spiegel, P.B.; Bamuturaki, J.; Patterson, N.; Muyonga, M.; Tatwebwa, L. HIV behavioural surveillance among refugees and surrounding host communities in Uganda, 2006. Afr. J. AIDS Res. 2009, 8, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Kågesten, A.E.; Zimmerman, L.; Robinson, C.; Lee, C.; Bawoke, T.; Osman, S.; Schlecht, J. Transitions into puberty and access to sexual and reproductive health information in two humanitarian settings: A cross-sectional survey of very young adolescents from Somalia and Myanmar. Confl. Health 2017, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Okanlawon, K.; Reeves, M.; Agbaje, O.F. Contraceptive use: Knowledge, perceptions and attitudes of refugee youths in Oru Refugee Camp, Nigeria. Afr. J. Reprod. Health 2010, 14, 16–25. [Google Scholar] [PubMed]
- Ortiz-Echevarria, L.; Greeley, M.; Bawoke, T.; Zimmerman, L.; Robinson, C.; Schlecht, J. Understanding the unique experiences, perspectives and sexual and reproductive health needs of very young adolescents: Somali refugees in Ethiopia. Confl. Health 2017, 11, 26. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.H.; Muyinda, H.; Sewankambo, N.K.; Oyat, G.; Atim, S.; Spittal, P.M. In the face of war: Examining sexual vulnerabilities of Acholi adolescent girls living in displacement camps in conflict-affected Northern Uganda. BMC Int. Health Hum. Rights 2012, 12, 38. [Google Scholar] [CrossRef] [PubMed]
- Schlecht, J.; Rowley, E.; Babirye, J.; Schlecht, J.; Rowley, E. Early relationships and marriage in conflict and post-conflict settings: Vulnerability of youth in Uganda. RHM. Reprod. Health Matters 2013, 21, 234–242. [Google Scholar] [CrossRef]
- Stark, L.; Asghar, K.; Yu, G.; Bora, C.; Baysa, A.A.; Falb, K.L. Prevalence and associated risk factors of violence against conflict-affected female adolescents: A multi-country, cross-sectional study. J. Glob. Health 2017, 7, 10416. [Google Scholar] [CrossRef] [PubMed]
- Stark, L.; Sommer, M.; Davis, K.; Asghar, K.; Baysa, A.A.; Abdela, G.; Tanner, S.; Falb, K. Disclosure bias for group versus individual reporting of violence amongst conflict-affected adolescent girls in DRC and Ethiopia. PLoS ONE 2017, 12, e0174741. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, M.; Myers, A.; Bhandari, P.; Cornier, N.; Doraiswamy, S.; Krause, S. Family planning in refugee settings: Findings and actions from a multi-country study. Confl. Health 2017, 11, 9. [Google Scholar] [CrossRef]
- Tanabe, M.; Nagujjah, Y.; Rimal, N.; Bukania, F.; Krause, S. Intersecting sexual and reproductive health and disability in humanitarian settings: Risks, needs, and capacities of refugees with disabilities in Kenya, Nepal, and Uganda. Sex. Disabil. 2015, 33, 411–427. [Google Scholar] [CrossRef] [PubMed]
- Whelan, A.; Blogg, J. ‘Halfway people’: Refugee views of reproductive health services. Glob. Public Health 2007, 2, 373–394. [Google Scholar] [CrossRef] [PubMed]
- Ackerson, K.; Zielinski, R. Factors influencing use of family planning in women living in crisis affected areas of Sub-Saharan Africa: A review of the literature. Midwifery 2017, 54, 35–60. [Google Scholar] [CrossRef] [PubMed]
- Lalor, K. Child Sexual Abuse in Sub-Saharan Africa: Child Protection Implications for Development Policy Makers and Practitioners. 2005. Available online: https://arrow.dit.ie/aaschsslrep/2/ (accessed on 1 June 2018).


{kind=link}
| Category | Search Terms Combined with AND |
|---|---|
| Age Group | youth OR teenager OR teen OR girl OR young female OR adolescent OR woman OR young woman OR women OR young person OR adolescence OR female OR reproductive age |
| Age | 10 to 24 |
| Status | refugee OR migrant OR displaced OR displaced person OR foreigner OR immigrant OR ethnic minority OR indigenous OR internally displaced OR asylum |
| SRH topics | sexual OR sexual health OR reproductive health OR early marriage OR child marriage OR female genital mutilation OR cutting OR female circumcision OR circumcised OR sexual behavior OR sexual experience OR sexual activity OR early sexual debut OR sexual initiation OR menstruation OR menstrual hygiene OR contraception OR family planning OR pregnancy OR antenatal OR birth OR post-natal OR sexually transmitted infection OR STI OR sexual intercourse OR HIV OR violence OR sexuality education OR reproduction OR sexual well-being OR condom OR human immunodeficiency virus OR AIDS OR sex education OR sex OR relationship OR physical relationship OR sexual coercion OR rape OR sexual violence OR sexual abuse OR abortion OR maternal health OR fistula OR motherhood OR gender OR forced sex OR intimate partner violence OR gender based violence OR transactional sex OR sex work OR HPV OR cervical cancer |
| Outcome | need OR unmet need OR access OR knowledge OR availability OR experience OR awareness OR perception |
| Countries/regions | Africa OR Algeria OR Angola OR Benin OR Botswana OR Burkina Faso OR Burundi OR Cameroon OR Cape Verde OR Central African Republic OR Chad OR Comoros OR Congo OR Democratic Republic of the Congo OR Cote d'Ivoire OR Djibouti OR Egypt OR Equatorial Guinea OR Eritrea OR Ethiopia OR Gabon OR Gambia OR Ghana OR Guinea OR Guinea-Bissau OR Kenya OR Lesotho OR Liberia OR Libya OR Madagascar OR Malawi OR Mali OR Mauritania OR Mauritius OR Morocco OR Mozambique OR Namibia OR Niger OR Nigeria OR Rwanda OR Sao Tome OR Senegal OR Seychelles OR Sierra Leone OR Somalia OR South Africa OR Sudan OR South Sudan OR Swaziland OR Tanzania OR Togo OR Tunisia OR Uganda OR Zambia OR Zimbabwe, NOT (Europe OR EU OR European Union OR Australia OR US OR New Zeeland OR United States OR France OR Greece OR Italy OR Austria OR Belgium OR Latvia OR Bulgaria OR Lithuania OR Croatia OR Luxembourg OR Cyprus OR Malta OR Czech Republic OR Netherlands OR Denmark OR Poland OR Estonia OR Portugal OR Finland OR Romania OR France OR Slovakia OR Germany OR Slovenia OR Greece OR Spain OR Hungary OR Sweden OR Ireland OR United Kingdom OR UK OR America OR Asia OR Brazil OR South America OR Latin America) |
| N | Author | Year | Country | Population | Age Group Included in the Review | Design | Main ResearchObjective/Aim | Quality of Studies (MMAT) |
|---|---|---|---|---|---|---|---|---|
| 1 | Casey et al. [16] | 2006 | Sierra Leone | Youth displaced by conflict (244 female and 293 male participants) | 15–24 | Quantitative Cross-sectional Survey (baseline data) | Explore the HIV/AIDS/STD knowledge, attitudes and behaviors of youth | 50% |
| 2 | Feseha et al. [17] | 2012 | Ethiopia | Refugee women (422) including 40 girls of 15–19 years old and 156 of 20–24 years old | 15–24 | Quantitative Cross-sectional Questionnaire | Assess the magnitude of intimate partner physical violence and associated factors among women | 100% |
| 3 | Gure et al. [18] | 2015 | Somalia | Unmarried girls in displacement camps (5) among total sample of 21 married and unmarried women | 18–20 | Qualitative Cross-sectional FGDs | Explore women’s knowledge of, experiences with, and need for reproductive health services | 50% |
| 4 | Harrison et al. [19] | 2009 | Uganda | Refugees and host communities (1600) with 120 (19.8%) of total female refugees (607) being girls of age 15–19 and 100 (16.6%) of 20–24 years old | 15–24 | Quantitative Cross-sectional Standardized behavioral surveillance survey (BSS) | Provide data on HIIV related knowledge, attitudes and behavior among refugees and surrounding hosts populations to allow for targeted HIV interventions | 100% |
| 5 | Iyakaremye and Mukagatare [6] | 2016 | Rwanda | Adolescent girls from DRC(10) in total sample (17) of boys, mothers, fathers and staff | Adolescent girls age not mentioned | Qualitative Cross-sectional Interviews and FGDs | Explore the experience of sexual abuse of adolescent girls in refugee camp | 75% |
| 6 | Kågesten et al. [20] | 2017 | Ethiopia and Thailand | Young Somali adolescents (406) in Kobe refugee camp, from which 214 (52.7%) were girls; and young adolescents from Myanmar (399) | 10–14 | Quantitative Cross-sectional Household survey | Describe transition into puberty and access to SRH information among very young adolescents in humanitarian setting | 75% |
| 7 | Okanlawon et al. [21] | 2010 | Nigeria | Youth in Oru refugee camp (116 female of total 208) | 10–24 | Qualitative and Quantitative Cross-sectional Self-administered questionnaire, in depth interviews and FGDs | Examine the perceptions, beliefs, knowledge and attitudes of refugee youths towards contraceptive use and also the access to and use of contraceptives in this refugee camp | Qualitative—75% Quantitative—50% Mixed—50% |
| 8 | Ortiz-Echevarria et al. [22] | 2017 | Ethiopia | Somali refugees and host community (126–32 adults and 94 adolescents including 46 refugee girls) | 10–16 | Qualitative Cross-sectional FGD with community mapping and photo | Understand lived realities of very young adolescents in Kobe refugee camp, their health and development needs, expectations and goals | 75% |
| 9 | Patel et al. [23] | 2012 | Uganda | Acholi girls (67) and adult women (65) in three displacement camps in Gulu district | 14–19 | Qualitative Cross-sectional In-depth interviews and FGD | Provide a better understanding of adolescent girl’s enhanced risk for HIV infection in conflict settings and to inform the development of appropriate sexual education and HIV prevention initiatives in this population group | 100% |
| 10 | Schlecht et al. [24] | 2013 | Uganda | Displaced and refugee men and women from Uganda and DRC (133) | 10–24 | Qualitative Cross sectional FGDKey informant interviews | Describe the factors which contribute to early relationships and informal marriages in conflict and post-conflict settings | 75% |
| 11 | Stark et al. [25] | 2017 | DRC and Ethiopia | Displaced, conflict-affected adolescent girls (1296) | 13–19 | Quantitative Cross-sectional Survey questionnaire using computer-assisted personal interview and computer-assisted self-interview | Assess the prevalence and related risk factors of physical, emotional, and sexual violence | 100% |
| 12 | Stark et al. [26] | 2017 | DRC and Ethiopia | 87 internally displaced adolescent girls from DRC and 78 Sudanese girls in Ethiopian refugee camps | 10–19 | Qualitative Cross-sectional Qualitative participatory mapping activity | Provide insight into assessing gender based violence from two methodological approaches | 75% |
| 13 | Tanabe et al. [28] | 2015 | Kenya, Nepal and Uganda | 352 refugee female and male participants from them44 adolescent girls with any type of impairment in Kenya and Uganda | 15–19 | Qualitative Cross-sectional Individual interviews and FGDs | Explore the specific risks, needs and barriers for persons with disabilities to access SRH services, and the capacities and practical ways through which the challenges could be addressed | 75% |
| 14 | Tanabe et al. [27] | 2017 | Djibouti, Kenya, Uganda, Bangladesh, Jordan and Malaysia | Adolescents, women and men in refugee settings | 15–19 | Qualitative and Quantitative Cross-sectional Household survey, in-depth interviews, FGDs and facilities assessment | Document the knowledge of family planning, belief and practices of refugees, and the state of service provision | Qualitative—50% Quantitative—50% Mixed—50% |
| 15 | Whelan [29] | 2007 | Uganda, Yemen and DRC | Refugees (816) including sample of 78 girls from Uganda and DRC participating in FGDs | Adolescent girls age not mentioned | Qualitative Cross-sectional FGDs and interviews | Identify factors that facilitate or hinder access to, use of, and satisfaction with RH services in refugee settings | 50% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivanova, O.; Rai, M.; Kemigisha, E. A Systematic Review of Sexual and Reproductive Health Knowledge, Experiences and Access to Services among Refugee, Migrant and Displaced Girls and Young Women in Africa. Int. J. Environ. Res. Public Health 2018, 15, 1583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081583
Ivanova O, Rai M, Kemigisha E. A Systematic Review of Sexual and Reproductive Health Knowledge, Experiences and Access to Services among Refugee, Migrant and Displaced Girls and Young Women in Africa. International Journal of Environmental Research and Public Health. 2018; 15(8):1583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081583
Chicago/Turabian StyleIvanova, Olena, Masna Rai, and Elizabeth Kemigisha. 2018. "A Systematic Review of Sexual and Reproductive Health Knowledge, Experiences and Access to Services among Refugee, Migrant and Displaced Girls and Young Women in Africa" International Journal of Environmental Research and Public Health 15, no. 8: 1583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081583