The Efficacy of Device Designs (Mono-block or Bi-block) in Oral Appliance Therapy for Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
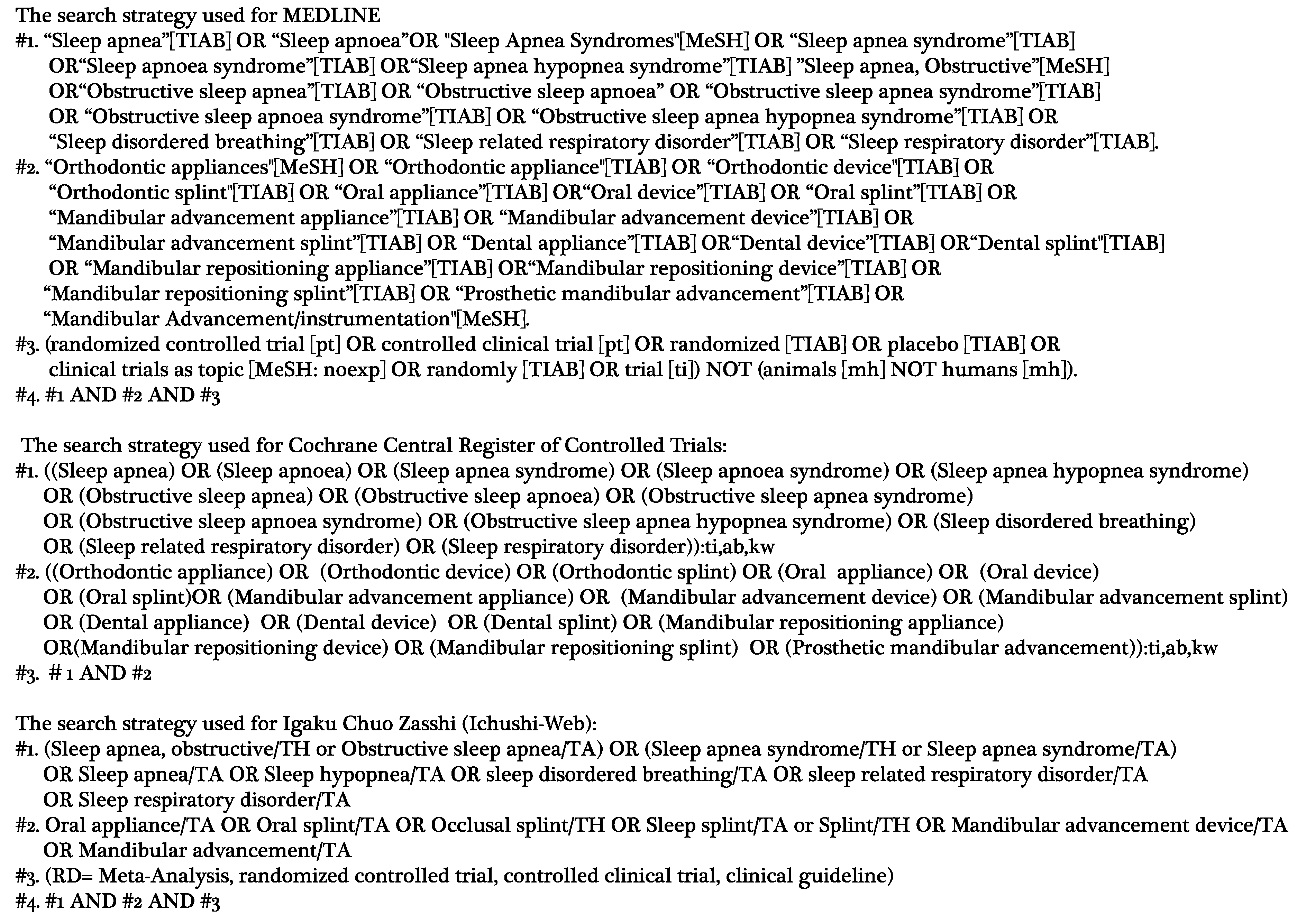
2.2. Literature Search
2.3. Study Selection Procedure
2.4. Data Extraction
2.5. Data Synthesis and Statistical Analysis
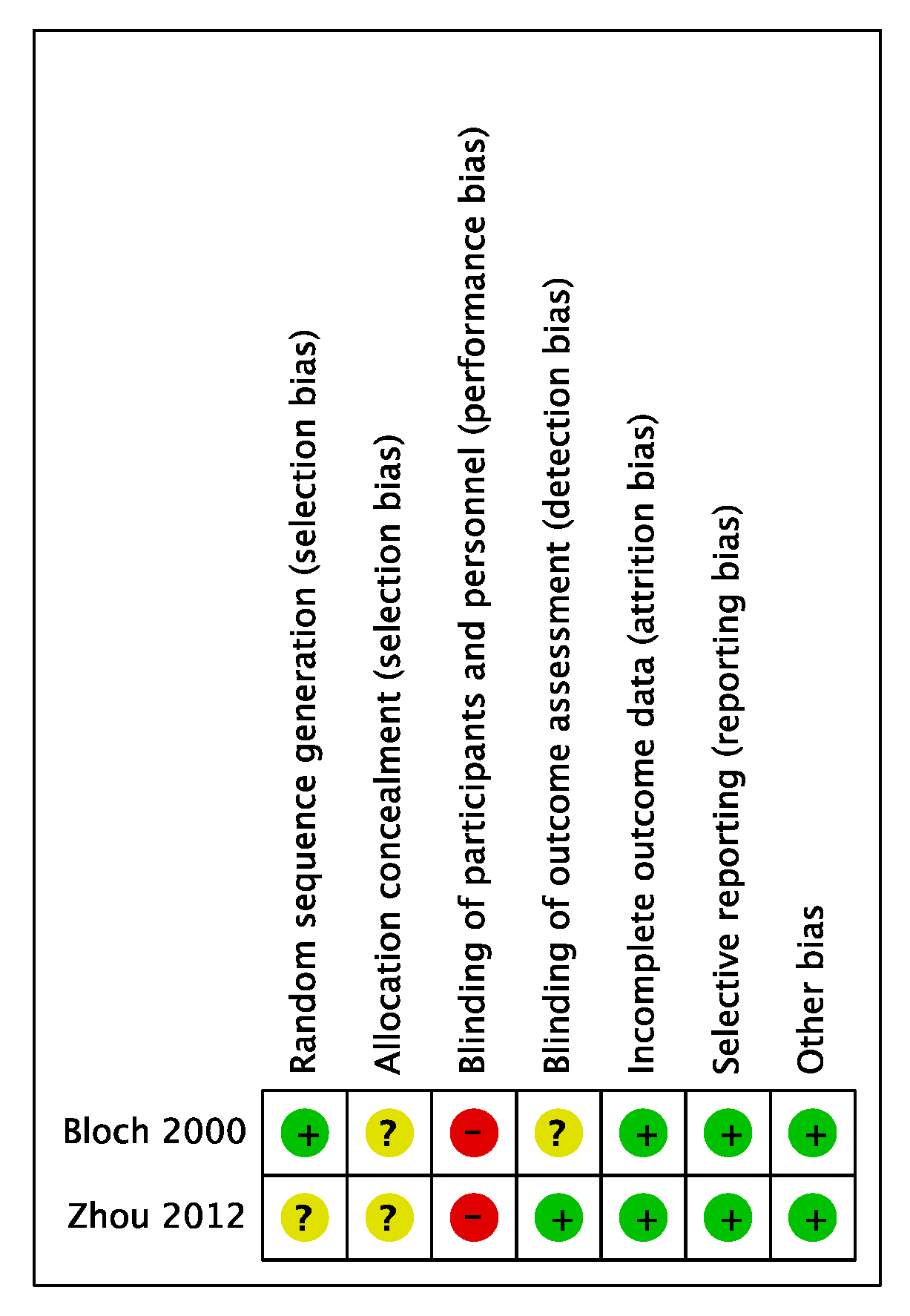
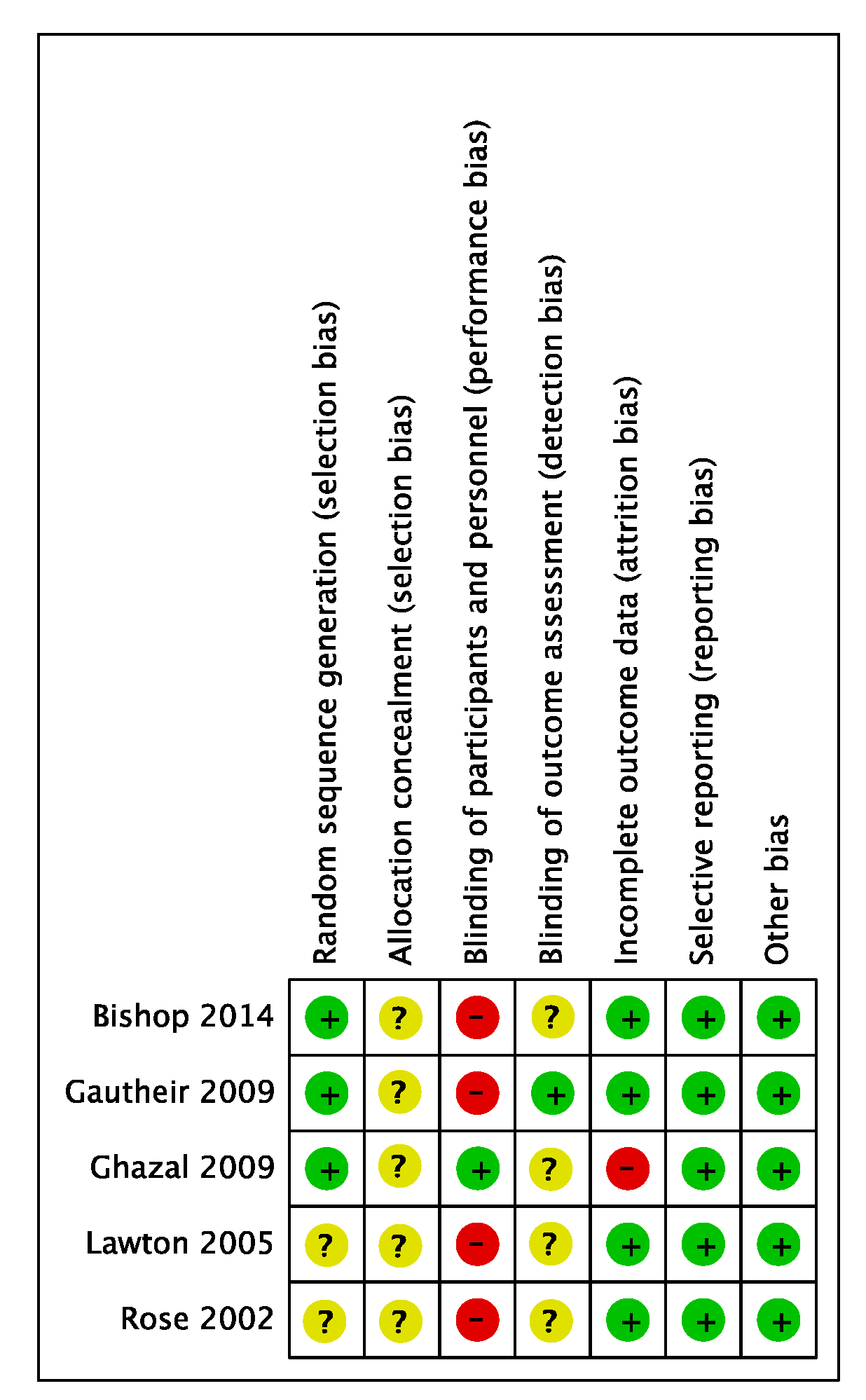
2.6. Quality Assessment of Included Studies
3. Results
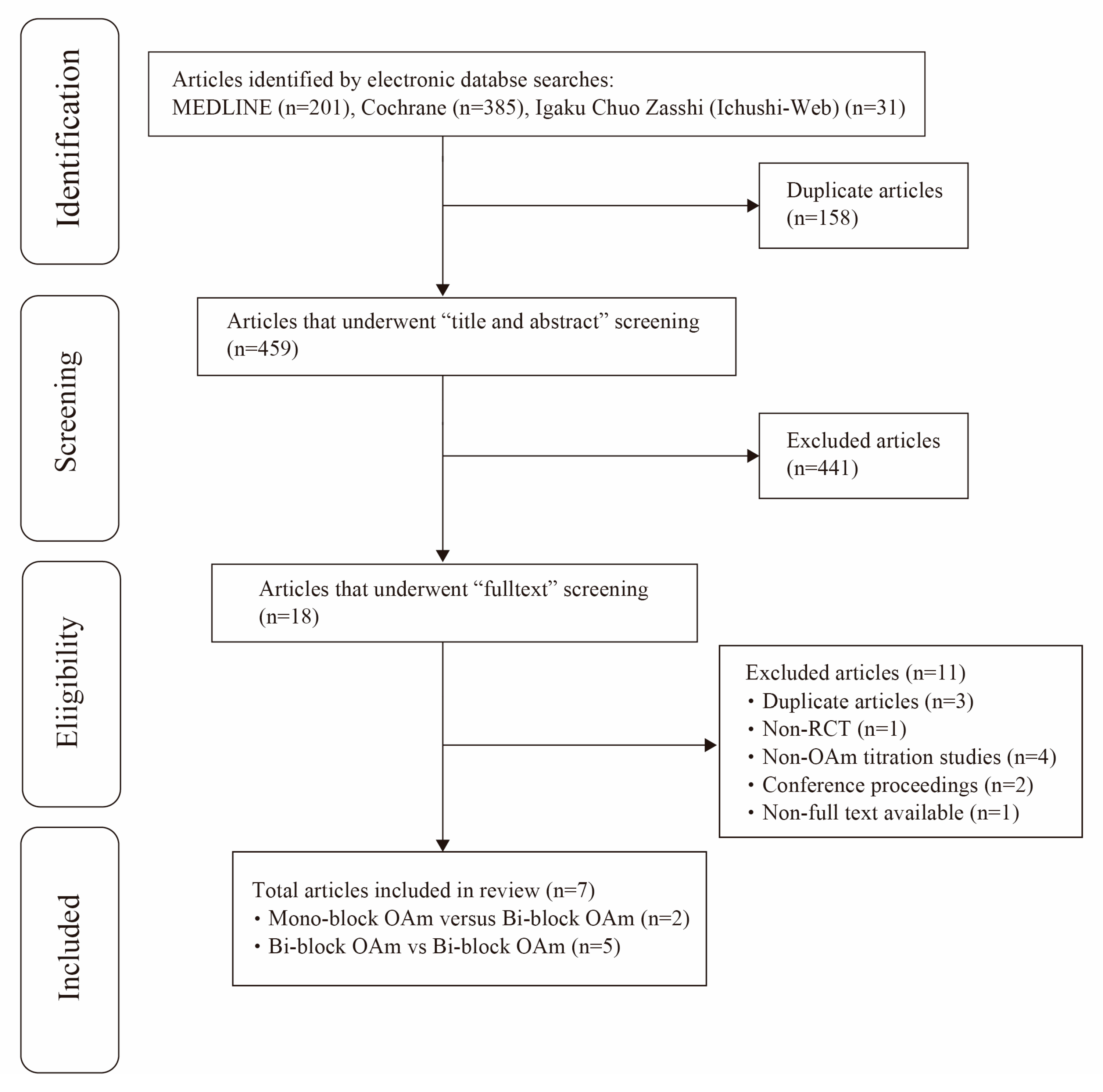
3.1. Literature Search and Selection Results
3.2. Key Features of the Included Studies
3.3. Meta-Analysis
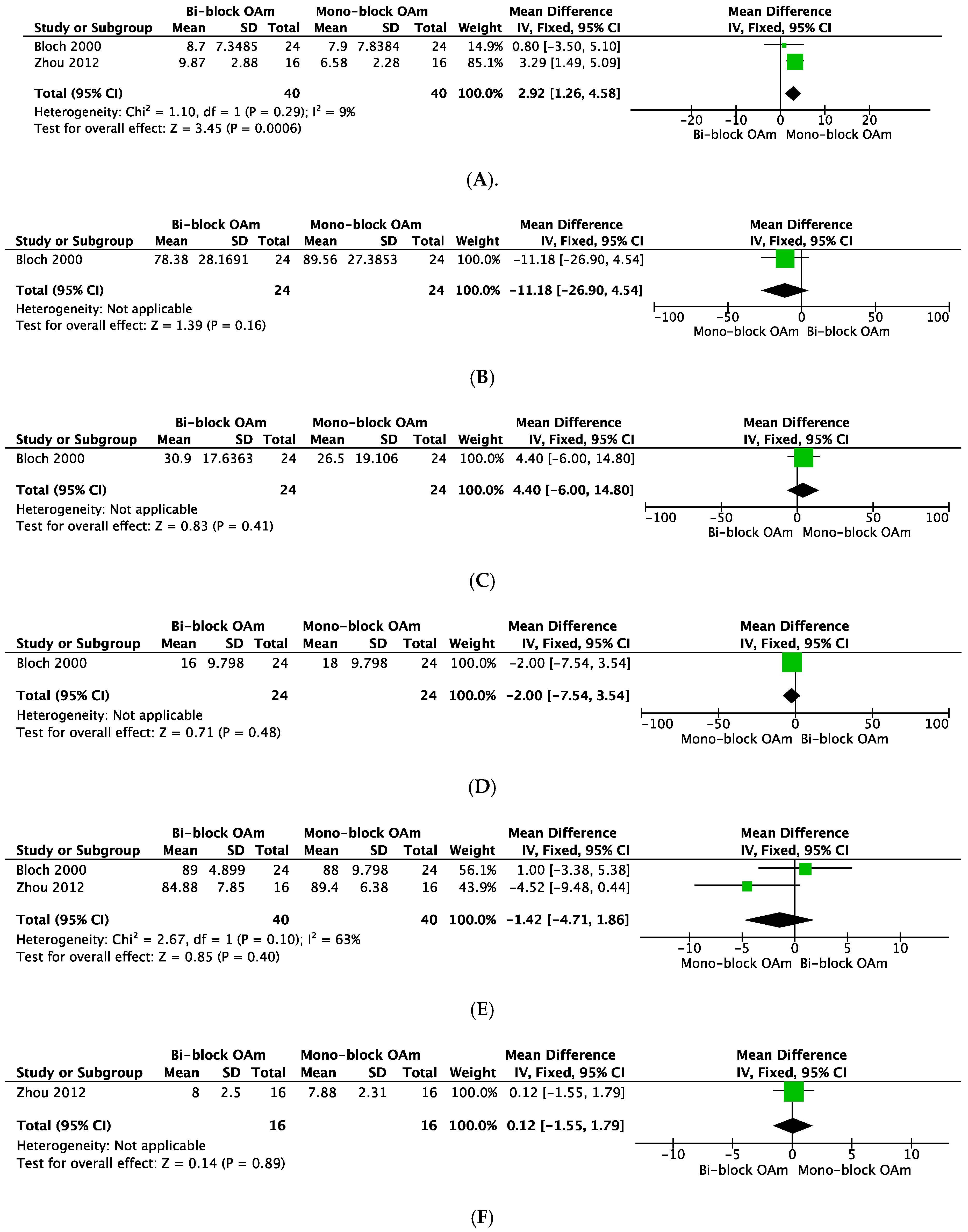
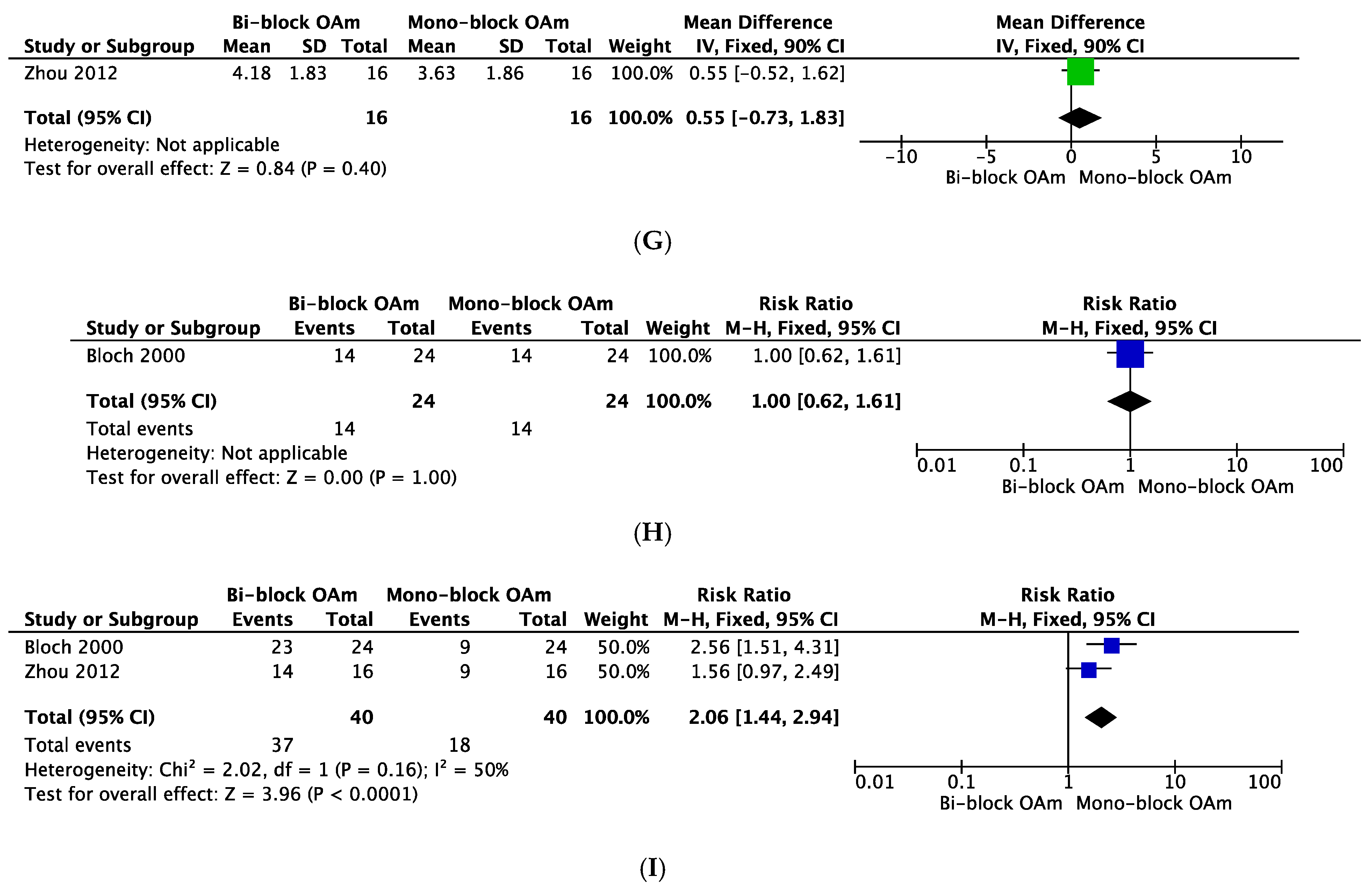
3.3.1. Mono-Block OAm Versus Bi-Block OAm
3.3.2. Bi-Block OAm Versus Bi-Block OAm
3.4. GRADE Evidence Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef]
- Flemons, W.W. Clinical practice. Obstructive sleep apnea. N. Engl. J. Med. 2002, 347, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Horner, R.L. Motor control of the pharyngeal musculature and implications for the pathogenesis of obstructive sleep apnea. Sleep 1996, 19, 827–853. [Google Scholar] [CrossRef] [PubMed]
- White, D.P. Pathogenesis of obstructive and central sleep apnea. Am. J. Respir. Crit. Care Med. 2005, 172, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Isono, S. Contribution of obesity and craniofacial abnormalities to pharyngeal collapsibility in patients with obstructive sleep apnea. Sleep Biol. Rhythms. 2004, 2, 17–21. [Google Scholar] [CrossRef]
- Kushida, C.A.; Morgenthaler, T.I.; Littner, M.R.; Alessi, C.A.; Bailey, D.; Coleman, J., Jr.; Friedman, L.; Hirshkowitz, M.; Kapen, S.; Kramer, M.; et al. Practice parameters for the treatment of snoring and Obstructive Sleep Apnea with oral appliances: An update for 2005. Sleep 2005, 29, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Sutherland, K.; Schwab, R.J.; Zeng, B.; Petocz, P.; Lee, R.W.; Darendeliler, M.A.; Cistulli, P.A. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax 2010, 65, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Mehta, A.; Qian, J.; Petocz, P.; Darendeliler, M.A.; Cistulli, P.A. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2001, 163, 1457–1461. [Google Scholar] [CrossRef] [PubMed]
- Gotsopoulos, H.; Chen, C.; Qian, J.; Cistulli, P.A. Oral appliance therapy improves symptoms in obstructive sleep apnea: A randomized, controlled trial. Am. J. Respir. Crit. Care Med. 2002, 166, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 11, 773–827. [Google Scholar] [PubMed] [Green Version]
- Chan, A.S.; Lee, R.W.; Cistulli, P.A. Dental appliance treatment for obstructive sleep apnea. Chest 2007, 132, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. Br. Med. J. 2004, 328, 1490. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. Br. Med. J. 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting ltems for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Br. Med. J. 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Bloch, K.E.; Iseli, A.; Zhang, J.N.; Xie, X.; Kaplan, V.; Stoeckli, P.W.; Russi, E.W. A Randomized, Controlled Crossover Trial of Two Oral Appliances for Sleep Apnea Treatment. Am. J. Respir. Crit. Care Med. 2000, 162, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Liu, Y.H. A randomised titrated crossover study comparing two oral appliances in the treatment for mild to moderate obstructive sleep apnoea/hypopnoea syndrome. J. Oral Rehabil. 2012, 39, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Bishop, B.; Verrett, R.; Girvan, T. A randomized crossover study comparing two mandibular repositioning appliances for treatment of obstructive sleep apnea. Sleep Breath. 2014, 18, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Lawton, H.M.; Battagel, J.M.; Kotecha, B. A comparison of the Twin Block and Herbst mandibular advancement splints in the treatment of patients with obstructive sleep apnoea: A prospective study. Eur. J. Orthod. 2005, 27, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Rose, E.; Staats, R.; Virchow, C.; Jonas, I.E. A comparative study of two mandibular advancement appliances for the treatment of obstructive sleep apnoea. Eur. J. Orthod. 2002, 24, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Ghazal, A.; Sorichter, S.; Jonas, I.; Rose, E.C. A randomized prospective long-term study of two oral appliances for sleep apnoea treatment. J. Sleep Res. 2009, 18, 321–328. [Google Scholar] [CrossRef]
- Gauthier, L.; Laberge, L.; Beaudry, M.; Laforte, M.; Rompré, P.H.; Lavigne, G.J. Efficacy of two mandibular advancement appliances in the management of snoring and mild-moderate sleep apnea: A cross-over randomized study. Sleep Med. 2009, 10, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.A.; Soler-Cataluña, J.J.; Ejarque-Martínez, L.; Soriano, Y.; Román-Sánchez, P.; Illa, F.B.; Canal, J.M.; Durán-Cantolla, J. Continuous positive airway pressure treatment reduces mortality in patients with ischemic stroke and obstructive sleep apnea: A 5-year follow-up study. Am. J. Respir. Crit. Care Med. 2009, 180, 36–41. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Kryger, M.H.; Zorick, F.J.; Conway, W.; Roth, T. Mortality and apnea index in obstructive sleep apnea: Experience in 385 male patients. Chest 1988, 94, 9–14. [Google Scholar] [CrossRef] [PubMed]
- McDaid, C.; Griffin, S.; Weatherly, H.; Durée, K.; van der Burgt, M.; van Hout, S.; Akers, J.; Davies, R.J.; Sculpher, M.; Westwood, M. Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea-hypopnoea syndrome: A systematic review and economic analysis. Health Technol. Assess. 2009, 13, 1–119. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, A.; McGrath, C.; Hägg, U. Subjective efficacy of oral appliance design features in the management of obstructive sleep apnea: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 559–576. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, A.; McGrath, C.; Hägg, U. A systematic review of the efficacy of oral appliance design features in the management of obstructive sleep apnea. Eur. J. Orthod. 2011, 33, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Serra-Torres, S.; Bellot-Arcís, C.; Montiel-Company, J.M.; Marco-Algarra, J.; Almerich-Silla, J.M. Effectiveness of mandibular advancement appliances in treating obstructive sleep apnea syndrome: A systematic review. Laryngoscope 2016, 126, 507–514. [Google Scholar] [CrossRef]
- Clark, G.T. Mandibular advancement devices and sleep disordered breathing. Sleep Med. Rev. 1998, 2, 163–174. [Google Scholar] [CrossRef]
- Sutherland, K.; Vanderveken, O.M.; Tsuda, H.; Marklund, M.; Gagnadoux, F.; Kushida, C.A.; Cistulli, P.A. Oral appliance treatment for obstructive sleep apnea: An update. J. Clin. Sleep Med. 2014, 10, 215–227. [Google Scholar] [CrossRef]
- Almeida, F.R.; Tsuiki, S.; Hattori, Y.; Takei, Y.; Inoue, Y.; Lowe, A.A. Dose-dependent effects of mandibular protrusion on genioglossus activity in sleep apnoea. Eur. Respir. J. 2011, 37, 209–212. [Google Scholar] [CrossRef]
- Aarab, G.; Lobbezoo, F.; Hamburger, H.L.; Naeije, M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin. Oral. Investig. 2010, 14, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Hamoda, M.M.; Kohzuka, Y.; Almeida, F.R. Oral Appliances for the Management of OSA: An Updated Review of the Literature. Chest 2018, 153, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Thie, N.M.; Montplaisir, R.; Lavigne, G.J. Bruxism and Orofacial movements during sleep. Dent. Clin. North Am. 2001, 45, 657–684. [Google Scholar] [PubMed]
- Kato, T.; Montplaisir, J.Y.; Guitard, F.; Sessle, B.J.; Lund, J.P.; Lavigne, G.J. Evidence that experimentally-induced sleep bruxism is a consequence of transient arousal. J. Dent. Res. 2003, 82, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Tangel, D.J.; Mezzanotte, W.S.; Sandberg, E.J.; White, D.P. Influences of NREM sleep on the activity of tonic vs. inspiratory phasic muscles in normal men. J. Appl. Physiol. 1992, 73, 1058–1066. [Google Scholar] [CrossRef]
- Kataoka, H.; Miyatake, N.; Ichikawa, H.; Arakawa, Y.; Mori, Y. Sub-analysis of the prevalence of locomotive syndrome and its relationship with health-related quality of life in patients with obstructive sleep apnea syndrome as classified by age and sex. Sleep Biol. Rhythm. 2019, 17, 149–153. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Design | Subjects | Interventions | Age | BMI | Follow-up | Outcomes |
|---|---|---|---|---|---|---|---|
| Mono-block OAm vs Bi-block OAm | |||||||
| Bloch 2000 | Cross over- RCT | 24 | Mono-block | 50.6 ± 1.5 a | 27.4 ± 0.8 a | (156 ± 14 days) + 1 week | AHI, ESS, Snoring (VAS), QOL, Side effect, Adherence, Patients preference |
| Herbst | |||||||
| Zhou 2012 | Cross over- RCT | 16 | Mono-block | 45.23 (26.3–55.4) b | 26.67 (22.3–29.8 ) b | 3 months | AHI, ESS, Snoring Scale, Airway space, Side effect, Adherence, Patient preference |
| SILENT NITE | |||||||
| Bi-block OAm vs Bi-block OAm | |||||||
| Lawton 2005 | Cross over- RCT | 16 | Herbst | 44.8 (24.0–68.4) c | 29.2 (23.8–51.1) c | 4–6 weeks | AHI, LowestspO2, ESS, Sleepiness (VAS), Snoring (VAS), SF-36, Side effects |
| Twin Block | |||||||
| Bishop 2014 | Cross over- RCT | 18 | TAP | 47.6 ± 2.6 a | 31.4 ± 1.0 a | 1–2 months | RDI, ESS, SAQLI, Patient preference |
| Klearway | |||||||
| Ghazal 2009 | RCT | 103 | IST | 55.5 ± 10.6 d | 25.9 ± 2.9 d | 6 months, 24 months | AHI, LowestspO2, Arousal Index, Sleep stage, Sleep efficiency, ESS, PSQI, SF-36, Adherence, Patient preference |
| TAP | |||||||
| Rose 2002 | Cross over- RCT | 26 | Silencer | 56.8 ± 5.2 d | 27.5 ± 3.1 d | 6–8 weeks | RDI, LowestspO2, Sleepiness (VAS), Sleep quality (VAS), Snoring (VAS), Adherence |
| Karwetzky activator | |||||||
| Gautheir 2009 | Cross over- RCT | 16 | Silencer | 56.8 ± 5.3 a | 25.9 ± 2.1 a | 3 months | RDI, LowestspO2, Sleep stage, Sleep efficiency, Blood pressure, ESS, FSS, FOSQ, Patient preference |
| Klearway | |||||||
| Study | Interventions | Follow Up | AHI (RDI) | Key Results | Conclusion | ||
|---|---|---|---|---|---|---|---|
| Baseline | wth OAm | %Reuction | |||||
| Mono-block OAm vs Bi-blockOAm | |||||||
| Bloch 2000 | Mono-block | 156 ± 14 days | 22.6 ± 3.1 a | 7.9 ± 1.6 a | 65.0 | Fifteen patients preferred the Monobloc, eight patients had no preference, and one patient preferred the Herbst device | Both the Herbst and the Mono-bloc are effective therapeutic devices for sleep apnea. The Mono-bloc relieved symptoms to a greater extent than the OSA-Herbst, and was preferred by the majority of patients on the basis of its simple application. |
| Herbst | 22.6 ± 3.1 a | 8.7 ± 1.5 a | 61.5 | ||||
| Zhou 2012 | Mono-block | 3 months | 26.38 ± 4.13 b | 6.58 ± 2.28 b* | 75.1 | The monoblock OAm was statistically more efficient in reducing AHI and Apnoea Index (AI) than the SILENT NITE (p < 0.05) | The Both OAm showed good efficacy in the treatment for mild to moderate OSA. Use of the monoblock appliance should be considered when patients with OSA choose OA treatment, as it was more efficient in reducing the AHI compared to the two-piece appliance and was preferred by most patients. |
| SILENT NITE | 26.38 ± 4.13 b | 9.87 ± 2.88 b* | 62.6 | ||||
| Bi-block OAm vs Bi-block OAm | |||||||
| Lawton 2005 | Twin Block | 4–6 weeks | 45.5 (29.0–68.0) c | 34.0 (9.0–63.0) c | 25.3 | The Herbst OAm proved to be the more effective appliance for reducing daytime sleepiness (p = 0.04) and was the more popular appliance among the patients. | The Twin Block OAm represents a viable alternative to the Herbst OAm in the treatment of patients with OSA. |
| Herbst | 45.5 (29.0–68.0) c | 24.5 (0.0–45.0) c | 46.2 | ||||
| Bishop 2014 | TAP | 1–2 months | 16.5 ± 3.2 a | 7.7 ± 3.3 a | 53.3 | There were no significant statistical differences in treatment outcomes between the two appliances. There was a statistically significant (p < 0.05) preference for a OAm design with minimal coverage of teeth and palate. | There was a trend toward greater improvement with the appliance with less acrylic resin bulk and less interocclusal contact. OA selection should favor titratable, unobtrusive designs with appropriate construction to promote acceptance and adherence to OA therapy. |
| Klearway | 16.5 ± 3.2 a | 10.3 ± 3.2 a | 37.6 | ||||
| Ghazal 2009 | IST | 6 months | 21.5 ± 13.5 b | 11.1 ± 11.8 b* | 48.4 | Quality of life, sleep quality, sleepiness, symptoms and sleep outcome showed significant improvement in the short-term evaluation with both appliances, but the TAP revealed a significantly greater effect. After more than 2 years of treatment, sleep outcomes revealed an equal effect with both appliances. | This study illustrates that both the IST and the TAP appliances are effective therapeutic devices for OSA after a period of over 24 months. |
| TAP | 21.5 ± 16.9 b | 6.7 ± 9.1 b* | 68.8 | ||||
| IST | 24 months | 18.4 ± 8.9 b | 4.6 ± 5.8 b | 75.0 | |||
| TAP | 19.8 ± 12.7 b | 5.4 ± 5.1 b | 72.7 | ||||
| Rose 2002 | Silencer | 6–8 weeks | 16.0 (4.4) b | 7.4 (5.3) b* | 53.8 | The results showed that a statistically significant improvement in the respiratory parameters was achieved with both appliances (p < 0.01). However, the activator was significantly more effective (p < 0.01) than the Silencor. | Both appliances reduced daytime sleepiness and snoring and improved sleep quality, and both influenced the treatment outcome. |
| Karwetzky activator | 16.2 (4.6) b | 5.5 (3.3) b* | 66.0 | ||||
| Gautheir 2009 | Silencer | 3 months | 10.0 ± 1.2 a | 4.7 ± 0.9 a* | 53.0 | The RDI was slightly lower with the Silencer (p < 0.05) but subjects’ preference for comfort was in favor of the Klearway (p = 0.04). | Although both OAm decreased RDI and subjective daytime sleepiness in a similar manner, the choice between various types of OAm needs to be taken into account when considering the benefit of RDI reduction over the benefit of subject compliance. |
| Klearway | 10.0 ± 1.2 a | 6.5 ± 1.3 a* | 35.0 | ||||
| Certainty Assessment | No. of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Mono-block OAm | Bi-block OAm | Relative | Absolute | |
| (95% CI) | (95% CI) | ||||||||||
| AHI | |||||||||||
| 2 | randomised trials | serious a | not serious | not serious | serious b | none | 40 | 40 | - | MD 2.92 higher | LOW |
| (1.26 higher to 4.58 higher) | |||||||||||
| Lowest SpO2 | |||||||||||
| 1 | randomised trials | serious a | not serious | not serious | very serious b,c | none | 24 | 24 | - | MD 11.18 lower | VERY LOW |
| (26.9 lower to 4.54 higher) | |||||||||||
| Arousal Index | |||||||||||
| 1 | randomised trials | serious a | not serious | not serious | very serious b,c | none | 24 | 24 | - | MD 4.4 higher | VERY LOW |
| (6 lower to 14.8 higher) | |||||||||||
| Non-REM Stage 3 | |||||||||||
| 1 | randomised trials | serious a | not serious | not serious | very serious b,c | none | 24 | 24 | - | MD 2 lower | VERY LOW |
| (7.54 lower to 3.54 higher) | |||||||||||
| Sleep Efficiency | |||||||||||
| 2 | randomised trials | serious a | serious d | not serious | very serious b,c | none | 40 | 40 | - | MD 1.42 lower | VERY LOW |
| (4.71 lower to 1.86 higher) | |||||||||||
| ESS | |||||||||||
| 1 | randomised trials | serious a | not serious | not serious | very serious b,c | none | 16 | 16 | - | MD 0.12 higher | VERY LOW |
| (1.55 lower to 1.79 higher) | |||||||||||
| Snoring Scale | |||||||||||
| 1 | randomised trials | serious a | not serious | not serious | very serious b,c | none | 16 | 16 | - | MD 0.55 higher | VERY LOW |
| (0.73 lower to 1.83 higher) | |||||||||||
| Side effect | |||||||||||
| 1 | randomised trials | serious a | not serious | not serious | very serious b,c | none | 14/24 (58.3%) | 14/24 (58.3%) | RR 1.00 | 0 fewer per 1000 | VERY LOW |
| (0.62 to 1.61) | (from 222 fewer to 356 more) | ||||||||||
| Patient preference | |||||||||||
| 2 | randomised trials | serious a | not serious e | not serious | serious b | none | 37/40 (92.5%) | 18/40 (45.0%) | RR 2.06 | 477 more per 1000 | LOW |
| (1.44 to 2.94) | (from 198 more to 873 more) | ||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishiyama, H.; Hasebe, D.; Sato, K.; Sakamoto, Y.; Furuhashi, A.; Komori, E.; Yuasa, H. The Efficacy of Device Designs (Mono-block or Bi-block) in Oral Appliance Therapy for Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173182
Ishiyama H, Hasebe D, Sato K, Sakamoto Y, Furuhashi A, Komori E, Yuasa H. The Efficacy of Device Designs (Mono-block or Bi-block) in Oral Appliance Therapy for Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(17):3182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173182
Chicago/Turabian StyleIshiyama, Hiroyuki, Daichi Hasebe, Kazumichi Sato, Yuki Sakamoto, Akifumi Furuhashi, Eri Komori, and Hidemichi Yuasa. 2019. "The Efficacy of Device Designs (Mono-block or Bi-block) in Oral Appliance Therapy for Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 17: 3182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173182