The Most Effective Amount of Forward Movement for Oral Appliances for Obstructive Sleep Apnea: A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.1.1. Inclusion Criteria
- The definition of OA
- Equipment that acquires upper and lower jaw impressions for every patient, which is thus precisely produced.
- A device that exerts an effect by maintaining the lower jaw in the forward direction.
- The diagnostic and therapeutic effects of OSA are determined by either polysomnography (PSG) or out-of-center sleep testing (OCST).
2.1.2. Exclusion Criteria
- Subject is under 18 years of age.
- The device is ready-made.
- The device exerts an effect by maintaining the tongue in the forward orientation.
2.1.3. Conditions Not Included in the Definition
- Equipment size, design
- Material characteristics (e.g., hard, soft, and hybrid)
- Thickness
- Detailed design of the device (e.g., type of connector in separate type and presence of integral air hole)
- Excluding comparison with forward movement of 0 mm (placebo)
2.2. Literature Search
- #1. “Sleep apnea”[TIAB] OR “Sleep apnoea” OR “Sleep Apnea Syndromes”[MeSH] OR “Sleep apnea syndrome”[TIAB] OR “Sleep apnoea syndrome”[TIAB] OR “Sleep apnea hypopnea syndrome”[TIAB] ”Sleep apnea, Obstructive”[MeSH] OR “Obstructive sleep apnea”[TIAB] OR “Obstructive sleep apnoea” OR “Obstructive sleep apnea syndrome”[TIAB] OR “Obstructive sleep apnoea syndrome”[TIAB] OR “Obstructive sleep apnea hypopnea syndrome”[TIAB] OR “Sleep disordered breathing”[TIAB] OR “Sleep related respiratory disorder”[TIAB] OR “Sleep respiratory disorder”[TIAB].
- #2. “Orthodontic appliances”[MeSH] OR “Orthodontic appliance”[TIAB] OR “Orthodontic device”[TIAB] OR “Orthodontic splint”[TIAB] OR “Oral appliance”[TIAB] OR “Oral device”[TIAB] OR “Oral splint”[TIAB] OR “Mandibular advancement appliance”[TIAB] OR “Mandibular advancement device”[TIAB] OR “Mandibular advancement splint”[TIAB] OR “Dental appliance”[TIAB] OR “Dental device”[TIAB] OR “Dental splint”[TIAB] OR “Mandibular repositioning appliance”[TIAB] OR “Mandibular repositioning device”[TIAB] OR “Mandibular repositioning splint”[TIAB] OR “Prosthetic mandibular advancement”[TIAB] OR “Mandibular Advancement/instrumentation”[MeSH].
- #3. (randomized controlled trial [pt] OR controlled clinical trial [pt] OR randomized [TIAB] OR placebo [TIAB] OR clinical trials as topic [MeSH: noexp] OR randomly [TIAB] OR trial [ti]) NOT (animals [mh] NOT humans [mh]).
- #4. #1 AND #2 AND #3
- #1. ((Sleep apnea) OR (Sleep apnoea) OR (Sleep apnea syndrome) OR (Sleep apnoea syndrome) OR (Sleep apnea hypopnea syndrome) OR (Obstructive sleep apnea) OR (Obstructive sleep apnoea) OR (Obstructive sleep apnea syndrome) OR (Obstructive sleep apnoea syndrome) OR (Obstructive sleep apnea hypopnea syndrome) OR (Sleep disordered breathing) OR (Sleep related respiratory disorder) OR (Sleep respiratory disorder)):ti,ab,kw
- #2. ((Orthodontic appliance) OR (Orthodontic device) OR (Orthodontic splint) OR (Oral appliance) OR (Oral device) OR (Oral splint) OR (Mandibular advancement appliance) OR (Mandibular advancement device) OR (Mandibular advancement splint) OR (Dental appliance) OR (Dental device) OR (Dental splint) OR (Mandibular repositioning appliance) OR (Mandibular repositioning device) OR (Mandibular repositioning splint) OR (Prosthetic mandibular advancement)):ti,ab,kw
- #3. #1 AND #2
- #1. “Sleep apnea, obstructive”[TH] OR “Obstructive sleep apnea”[TA] OR “Sleep apnea syndrome”[TH] OR “sleep apnea syndromes”[TA] OR “Sleep apnea”[TA] OR “Sleep hypopnea”[TA] OR “sleep disordered breathing”[TA] OR “sleep related respiratory disorder”[TA] OR “Sleep respiratory disorder”[TA]
- #2. “Oral appliance”[TA] OR “Oral splint”[TA] OR “Occlusal splints”[TH] OR “Sleep splint”[TA] OR “Splint”[TH] OR “Mandibular advancement device”[TA] OR “Mandibular advancement”[TA]
- #3. (RD= Meta-Analysis, randomized controlled trial, controlled clinical trial, clinical guideline)
- #4. #1 AND #2 AND #3
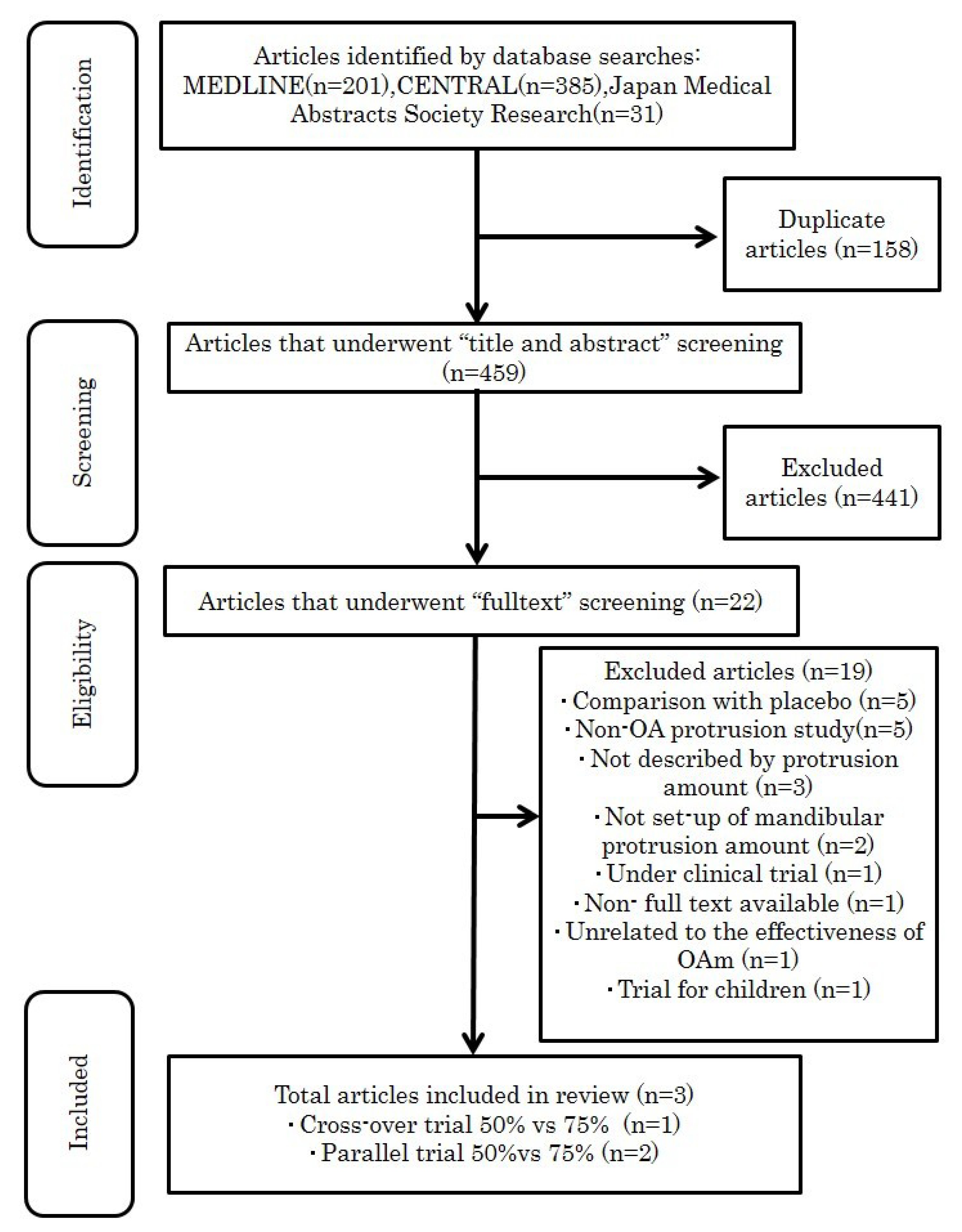
2.3. Study Selection Procedure
2.4. Data Extraction
2.5. Quality Assessment of Included Studies
3. Results
3.1. Identification and Description of Included Studies
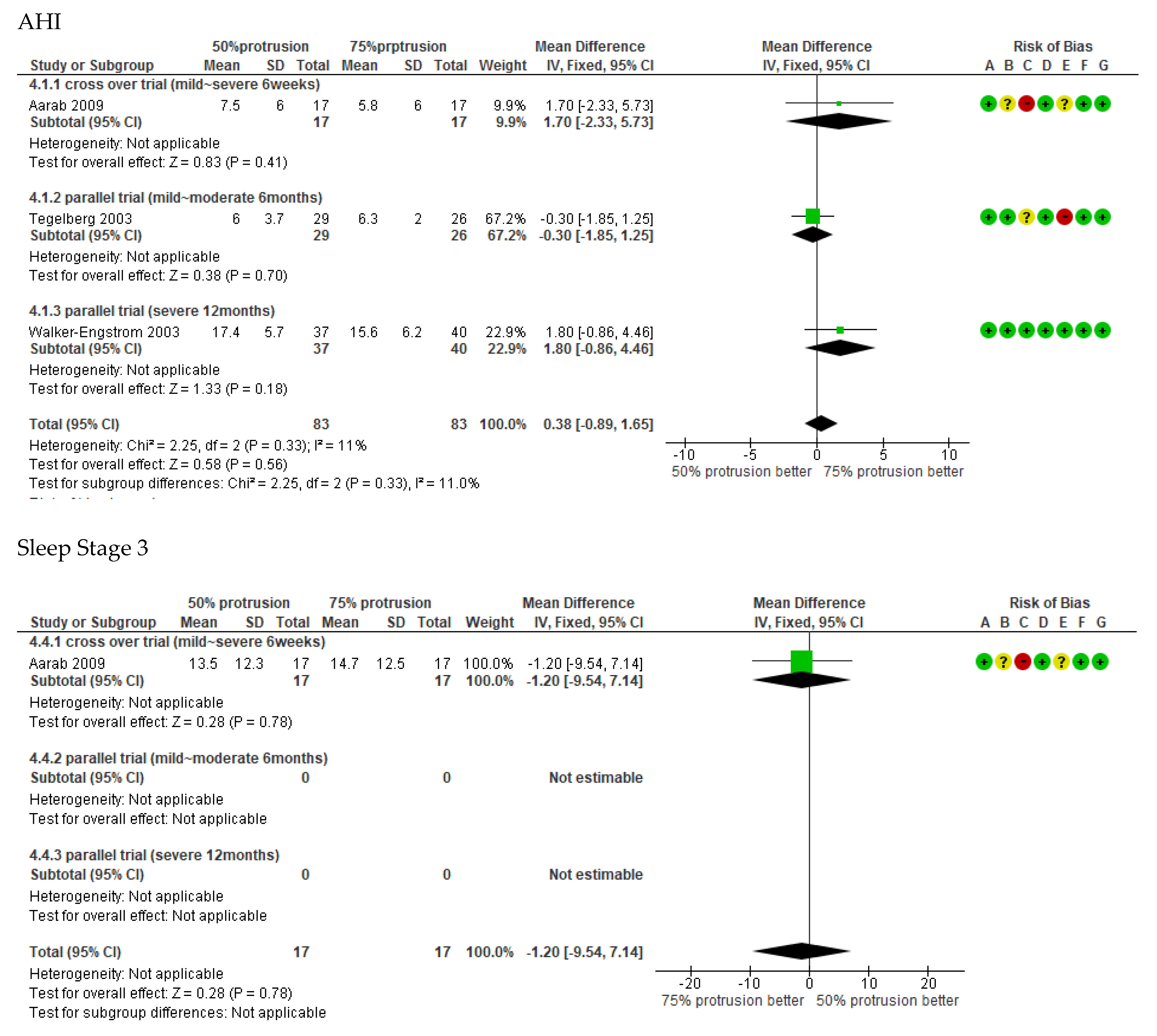
3.2. Meta-Analysis
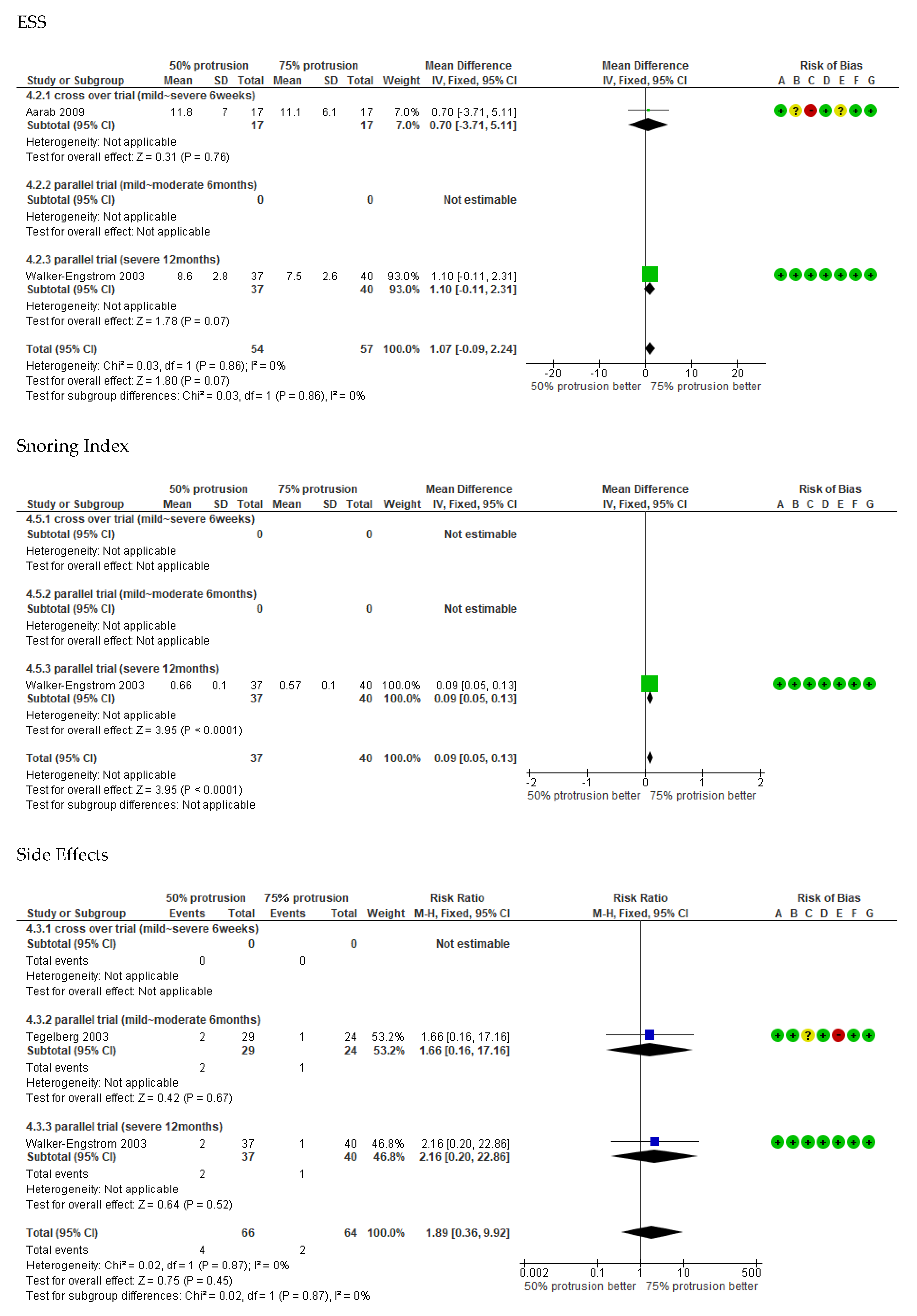
3.2.1. Treatment Effect
3.2.2. Side Effects
3.3. GRADE Evidence Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shamsuzzaman, A.S.; Gersh, B.J.; Somers, V.K. Obstructive Sleep Apnea: Implications for Cardiac and Vascular Disease. JAMA 2003, 290, 1906–1914. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment panel III). Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Mesarwi, O.A.; Sharma, E.V.; Jun, J.C.; Polotsky, V.Y. Metabolic Dysfunction in Obstructive Sleep Apnea: A Critical Examination of Underlying Mechanisms. Sleep Biol. Rhythms 2015, 13, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, M.L.; Bortolotti, F.; Raffaelli, E.; D’Antò, V.; Michelotti, A.; Alessandri Bonetti, G. The Effectiveness of Different Mandibular Advancement Amounts in OSA Patients: a Systematic Review and Meta-Regression Analysis. Sleep Breath. 2016, 20, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Aarab, G.; Lobbezoo, F.; Hamburger, H.L.; Naeije, M. Effects of an Oral Appliance with Different Mandibular Protrusion Positions at a Constant Vertical Dimension on Obstructive Sleep Apnea. Clin. Oral Investig. 2010, 14, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Tegelberg, A.; Walker-Engström, M.L.; Vestling, O.; Wilhelmsson, B. Two Different Degrees of Mandibular Advancement with a Dental Appliance in Treatment of Patients with Mild to Moderate Obstructive Sleep Apnea. Acta Odontol. Scand. 2003, 61, 356–362. [Google Scholar] [CrossRef]
- Walker-Engström, M.L.; Ringqvist, I.; Vestling, O.; Wilhelmsson, B.; Tegelberg, A. A Prospective Randomized Study Comparing Two Different Degrees of Mandibular Advancement with a Dental Appliance in Treatment of Severe Obstructive Sleep Apnea. Sleep Breath. 2003, 7, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Aydin Guclu, O.; Ursavas, A.; Kasapoglu, F.; Ozarda, Y.; Bozyigit, C.; Ocakoglu, G.; Karadag, M. Relationship with Excessive Daytime Sleepiness and Serum Substance P Levels in OSAS Patients and the Effect of PAP Treatment. Sleep Biol. Rhythms 2019, 17, 355–361. [Google Scholar] [CrossRef]
- Lakadamyali, H.; Kivanc, T.; Yilmaz Avci, A.Y. Correlation of Changes in the Red Blood Cell Distribution Width with the Response to Continuous Positive Airway Pressure in Patients with Obstructive Sleep Apnea. Sleep Biol. Rhythms 2019, 17, 141–148. [Google Scholar] [CrossRef]
- Isono, S. Contribution of Obesity and Craniofacial Abnormalities to Pharyngeal Collapsibility in Patients with Obstructive Sleep Apnea. Sleep Biol. Rhythms 2004, 2, 17–21. [Google Scholar] [CrossRef]
- Piskin, B.; Karakoc, O.; Genc, H.; Akay, S.; Sipahi, C.; Erdem, M.; Karaman, B.; Gorgulu, S.; Yetkin, S.; Ayyildiz, S. Effects of Varying Mandibular Protrusion and Degrees of Vertical Opening on Upper Airway Dimensions in Apneic Dentate Subjects. J. Orofac. Orthop. 2015, 76, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Joosten, S.A.; Hamilton, G.S.; Naughton, M.T. Impact of Weight Loss Management in OSA. Chest 2017, 152, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Hamoda, M.M.; Kohzuka, Y.; Almeida, F.R. Oral Appliances for the Management of OSA: an Updated Review of Literature. Chest 2018, 153, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Lee, R.W.; Srinivasan, V.K.; Darendeliler, M.A.; Grunstein, R.R.; Cistulli, P.A. Nasopharyngoscopic Evaluation of Oral Appliance Therapy for Obstructive Sleep Apnoea. Eur. Respir. J. 2010, 35, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.T.; Qian, J.; Cistulli, P.A. Oropharyngeal Collapse Predicts Treatment Response with Oral Appliance Therapy in Obstructive Sleep Apnea. Sleep 2006, 29, 666–671. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study/Year | Study Design | OSA Severity | Duration | Control Type | Number of the Beginning Patients | Number of the Patients Completed Trial | Age (Mean SD) | BMI (Mean SD) | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1, Aarab 2009 | 2-armed crossover; randomised | mild OSA | 1.5 months | 50%, 75% protrusion | 50%: 20 | 50%: 17 | 50%: 51.8 (49.0–54.6) | 50%: 27.6 ± 3.3 | AHI, ODI, Lowest SPO2, Total sleep time, Stage3, Stage REM, ESS |
| 75%: 20 | 75%: 17 | 75%: 54.4 (52.4–56.4) | 75%: 27.6 ±3.0 | ||||||
| 2, Tegelberg 2003 | 2-armed Parallel; randomised | mild to moderate OSA | 12 months | 50%, 75% protrusion | 50%: 38 | 50%: 29 | 50%: 51.8 (49.0–54.6) | 50%: 27.4 (26.4–28.4) | AHI, AI, ODI |
| 75%: 36 | 75%: 26 | 75%: 54.4 (52.4–56.4) | 75%: 27.9 (26.6–29.3) | ||||||
| 3, Walker-Engstrom 2003 | 2-armed Parallel; randomised | severe OSA | 6 months | 50%, 75% protrusion | 50%: 42 | 50%: 37 | 50%: 54.3 (52.2–56.4) | 50%: 30.5 ± 1.4 | AHI, AI, ODI, SI, ESS |
| 75%: 42 | 75%: 40 | 75%: 50.4 (47.7–53.1) | 75%: 30.2 ± 1.2 |
| Certainty Assessment | No. of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | 50% Protrusion | 75% Protrusion | Relative | Absolute | |
| (95% CI) | (95% CI) | ||||||||||
| AHI | |||||||||||
| 3 | randomised trials | serious a | not serious | not serious | very serious b | none | 83 | 83 | - | MD 0.38 higher | VERY LOW |
| (0.89 lower to 1.65 higher) | |||||||||||
| AHI - Cross over trialmild~severe6weeks | |||||||||||
| 1 | randomised trials | serious b | not serious | not serious | very serious b | none | 17 | 17 | - | MD 1.7 higher | VERY LOW |
| (2.33 lower to 5.73 higher) | |||||||||||
| AHI – parallel trialmild~moderate6 months | |||||||||||
| 1 | randomised trials | serious a,c | not serious | not serious | very serious b | none | 29 | 26 | - | MD 0.3 lower | VERY LOW |
| (1.85 lower to 1.25 higher) | |||||||||||
| AHI - parallel trialsevere12 months | |||||||||||
| 1 | randomised trials | not serious | not serious | not serious | very serious b | none | 37 | 40 | - | MD 1.8 higher | LOW |
| (0.86 lower to 4.46 higher) | |||||||||||
| ESS | |||||||||||
| 2 | randomised trials | not serious | not serious | not serious | very serious b | none | 54 | 57 | - | MD 1.07 higher | LOW |
| (0.09 lower to 2.24 higher) | |||||||||||
| side effect | |||||||||||
| 2 | randomised trials | serious a | not serious | not serious | very serious b | none | 4/66 (6.1%) | 2/64 (3.1%) | RR 1.89 | 28 more per 1000 | VERY LOW |
| (0.36 to 9.92) | (from 20 fewer to 279 more) | ||||||||||
| Stage 3,4 | |||||||||||
| 1 | randomised trials | serious b | not serious | not serious | very serious b | none | 17 | 17 | - | MD 1.2 lower | VERY LOW |
| (9.54 lower to 7.14 higher) | |||||||||||
| Snoring Index | |||||||||||
| 1 | randomised trials | not serious | not serious | not serious | very serious b | none | 37 | 40 | - | MD 0.09 higher | LOW |
| (0.05 higher to 0.13 higher) | |||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakamoto, Y.; Furuhashi, A.; Komori, E.; Ishiyama, H.; Hasebe, D.; Sato, K.; Yuasa, H. The Most Effective Amount of Forward Movement for Oral Appliances for Obstructive Sleep Apnea: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 3248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183248
Sakamoto Y, Furuhashi A, Komori E, Ishiyama H, Hasebe D, Sato K, Yuasa H. The Most Effective Amount of Forward Movement for Oral Appliances for Obstructive Sleep Apnea: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(18):3248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183248
Chicago/Turabian StyleSakamoto, Yuki, Akifumi Furuhashi, Eri Komori, Hiroyuki Ishiyama, Daichi Hasebe, Kazumichi Sato, and Hidemichi Yuasa. 2019. "The Most Effective Amount of Forward Movement for Oral Appliances for Obstructive Sleep Apnea: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 18: 3248. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183248