Behavioral and Emotional Disorders and Transportation Noise among Children and Adolescents: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question and Study Eligibility
2.2. Information Sources and Search
2.3. Study Selection and Data Collection
- study design,
- region,
- study population size,
- population characteristics (age and sex distributions),
- population sampling information (recruitment times, response and follow-up),
- outcomes considering how they were assessed (instruments used),
- noise exposures sources considered,
- noise assessment, including the noise levels considered, and
- relevant study results.
2.4. Rating of Methodological Study Quality
2.5. Meta-Analysis
3. Results
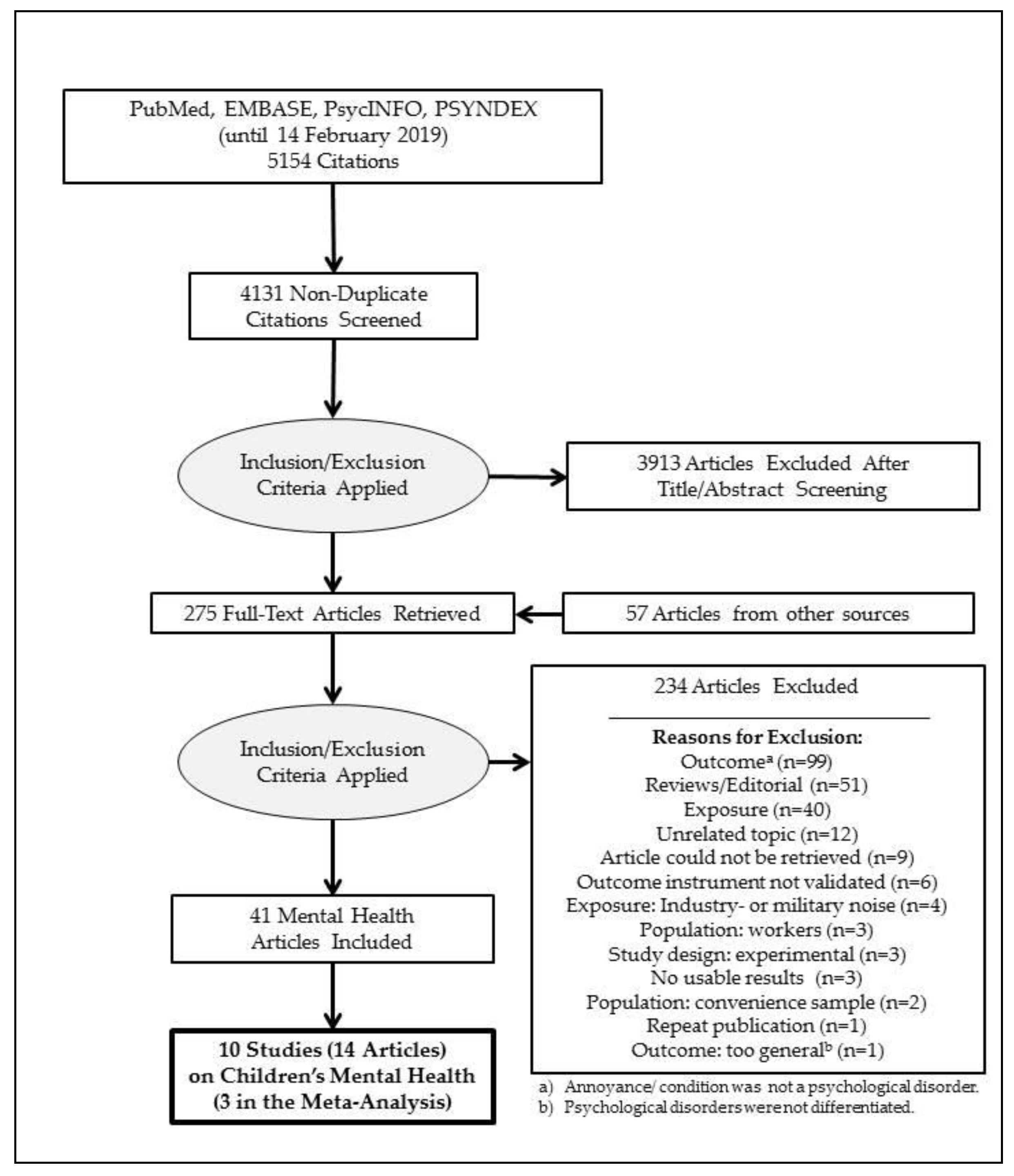
3.1. Study Selection
3.2. Study Characteristics
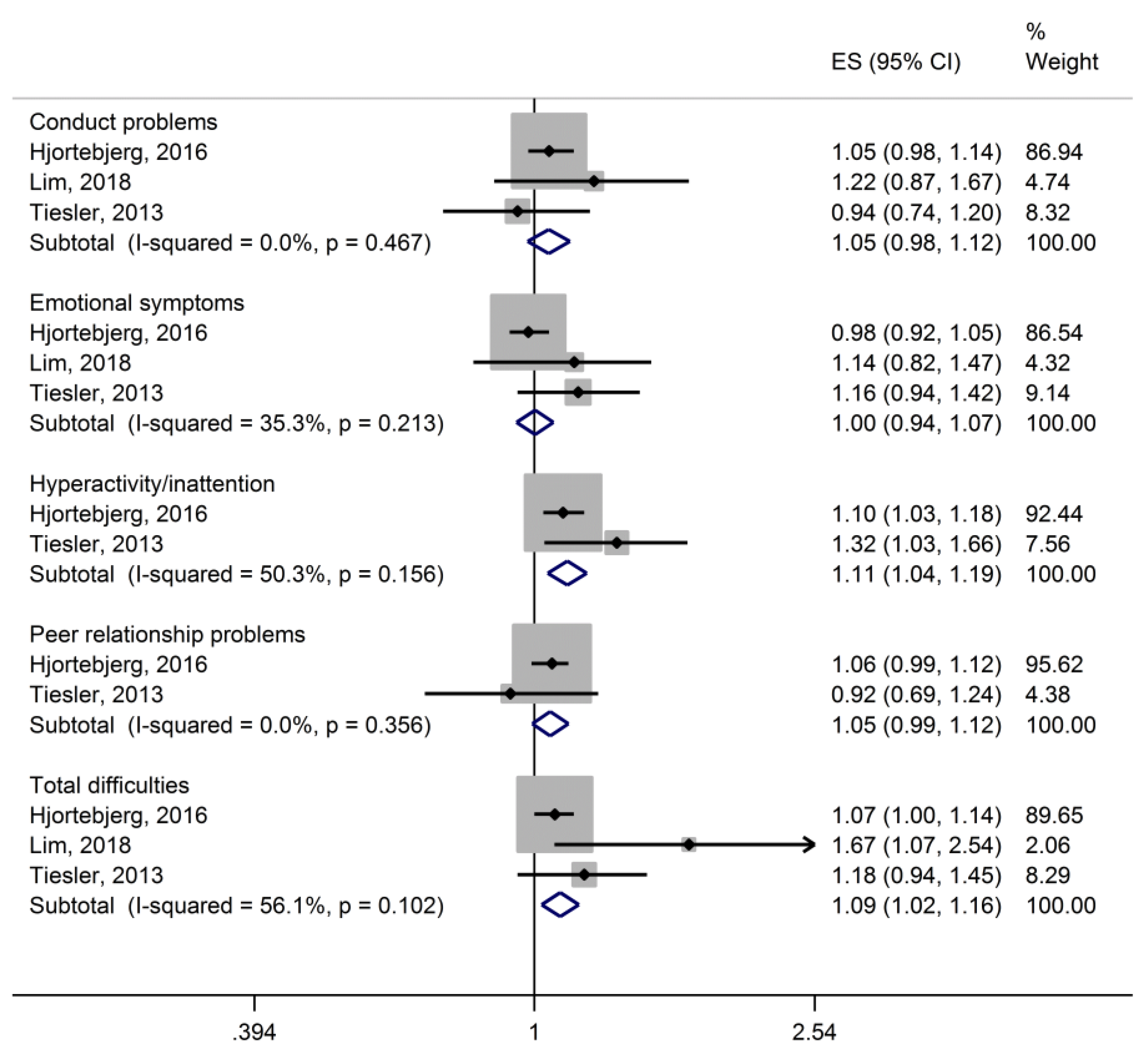
3.2.1. Synthesis of Results
3.2.2. Risk of Bias Across Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Investing in Mental Health; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- WHO. Mental Health: Fact Sheet; Regional Office for Europe of the World Health Organisation: Copenhagen, Denmark, 2019. [Google Scholar]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual Research Review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child. Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.; De Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Grobe, T.G.; Dörning, H.; Schwartz, F.W. Barmer GEK Arztreport 2013. Schr. Zur Gesundh. 2013, 18, 160–173. [Google Scholar]
- Roick, C.; Waltersbacher, A. Hyperkinetische Störungen bei Kindern und Jugendlichen in Deutschland: Administrative Prävalenz und regionale Unterschiede in der Diagnosehäufigkeit. Psychiatr. Prax. 2015, 42, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, C.J.; Philipsen, A.; Hoffmann, F. ADHD in Germany: Trends in Diagnosis and Pharmacotherapy: A Country-wide Analysis of Health Insurance Data on Attention-Deficit/Hyperactivity Disorder (ADHD) in Children, Adolescents and Adults From 2009–2014. Dtsch. Ärztebl. Int. 2017, 114, 141. [Google Scholar]
- Köster, I.; Schubert, I.; Döpfner, M.; Adam, C.; Ihle, P.; Lehmkuhl, G. Hyperkinetische Störungen bei Kindern und Jugendlichen: Zur Häufigkeit des Behandlungsanlasses in der ambulanten Versorgung nach den Daten der Versichertenstichprobe AOK Hessen/KV Hessen (1998–2001). Z. Kinder Jugendpsychiatr. Psychother. 2004, 32, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Sibley, M.H.; Mitchell, J.T.; Becker, S.P. Method of adult diagnosis influences estimated persistence of childhood ADHD: A systematic review of longitudinal studies. Lancet Psychiatry 2016, 3, 1157–1165. [Google Scholar] [CrossRef]
- Fayyad, J.; Sampson, N.A.; Hwang, I.; Adamowski, T.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Andrade, L.H.; Borges, G.; de Girolamo, G.; Florescu, S. The descriptive epidemiology of DSM-IV adult ADHD in the world health organization world mental health surveys. Adhd Atten. Deficit Hyperact. Disord. 2017, 9, 47–65. [Google Scholar] [CrossRef]
- Pilling, S.; Gould, N.; Whittington, C.; Taylor, C.; Scott, S. Recognition, intervention, and management of antisocial behaviour and conduct disorders in children and young people: Summary of NICE-SCIE guidance. BMJ Br. Med. J. 2013, 346, f1298. [Google Scholar] [CrossRef]
- Meltzer, H.; Gatward, R.; Goodman, R.; Ford, T. Mental health of children and adolescents in Great Britain. Int. Rev. Psychiatry 2003, 15, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Stansfeld, S.A.; Matheson, M.P. Noise pollution: Non-auditory effects on health. Br. Med. Bull. 2003, 68, 243–257. [Google Scholar] [CrossRef] [PubMed]
- Kempen, E.V.; Casas, M.; Pershagen, G.; Foraster, M. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Cardiovascular and Metabolic Effects: A Summary. Int. J. Environ. Res. Public Health 2018, 15, 379. [Google Scholar] [CrossRef] [PubMed]
- Weihofen, V.M.; Hegewald, J.; Euler, U.; Schlattmann, P.; Zeeb, H.; Seidler, A. Aircraft Noise and the Risk of Stroke. Dtsch. Arztebl. Int. 2019, 116, 237–244. [Google Scholar] [CrossRef]
- Bullinger, M.; Hygge, S.; Evans, G.W.; Meis, M.; Mackensen, S.V. The psychological cost of aircraft noise for children. Zent. Hyg. Umweltmed. 1999, 202, 127–138. [Google Scholar] [CrossRef]
- Lercher, P.; Evans, G.W.; Meis, M.; Kofler, W.W. Ambient neighbourhood noise and children’s mental health. Occup. Environ. Med. 2002, 59, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Bergström, K.; Spilski, J.; Mayerl, J.; Möhler, U.; Lachmann, T.; Klatte, M. Effects of Aircraft Noise on Annoyance and Quality of Life in German Children near Frankfurt/Main Airport: Results of the NORAH (Noise-Related Annoyance, Cognition, and Health)-Study. 2015. Available online: https://www.researchgate.net/publication/289532204_Effects_of_aircraft_noise_on_annoyance_and_quality_of_life_in_German_children_near_FrankfurtMain_airport_Results_of_the_NORAH_noise-related_annoyance_cognition_and_health-study (accessed on 8 August 2019).
- Tiesler, C.M.; Birk, M.; Thiering, E.; Kohlbock, G.; Koletzko, S.; Bauer, C.P.; Berdel, D.; von Berg, A.; Babisch, W.; Heinrich, J.; et al. Exposure to road traffic noise and children’s behavioural problems and sleep disturbance: Results from the GINIplus and LISAplus studies. Environ. Res. 2013, 123, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chervin, R.D.; Archbold, K.H.; Dillon, J.E.; Panahi, P.; Pituch, K.J.; Dahl, R.E.; Guilleminault, C. Inattention, hyperactivity, and symptoms of sleep-disordered breathing. Pediatr. Springf. 2002, 109, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Faraone, S.V.; Konofal, E.; Lecendreux, M. Sleep in children with attention-deficit/hyperactivity disorder: Meta-analysis of subjective and objective studies. J. Am. Acad. Child. Adolesc. Psychiatry 2009, 48, 894–908. [Google Scholar] [CrossRef]
- Hysing, M.; Lundervold, A.J.; Posserud, M.-B.; Sivertsen, B. Association between sleep problems and symptoms of attention deficit hyperactivity disorder in adolescence: Results from a large population-based study. Behav. Sleep Med. 2016, 14, 550–564. [Google Scholar] [CrossRef]
- Huhdanpää, H.; Morales-Muñoz, I.; Aronen, E.T.; Pölkki, P.; Saarenpää-Heikkilä, O.; Paunio, T.; Kylliäinen, A.; Paavonen, E.J. Sleep Difficulties in Infancy Are Associated with Symptoms of Inattention and Hyperactivity at the Age of 5 Years: A Longitudinal Study. J. Dev. Behav. Pediatrics 2019, 40, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Stansfeld, S.A.; Clark, C.; Cameron, R.M.; Alfred, T.; Head, J.; Haines, M.M.; Van Kamp, I.; Van Kempen, E.; López-Barrio, I. Aircraft and road traffic noise exposure and children’s mental health. J. Environ. Psychol. 2009, 29, 203–207. [Google Scholar] [CrossRef]
- Clark, C.; Paunovic, K. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Quality of Life, Wellbeing and Mental Health. Int. J. Environ. Res. Public Health 2018, 15, 2400. [Google Scholar] [CrossRef] [PubMed]
- Zare Sakhvidi, F.; Zare Sakhvidi, M.J.; Mehrparvar, A.H.; Dzhambov, A.M. Environmental Noise Exposure and Neurodevelopmental and Mental Health Problems in Children: A Systematic Review. Curr. Environ. Health Rep. 2018, 5, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.; Bolm-Audorff, U.; Hegewald, J.; Fishta, A.; Schlattmann, P.; Schmitt, J.; Seidler, A. Occupational polycyclic aromatic hydrocarbon exposure and risk of larynx cancer: A systematic review and meta-analysis. Occup. Environ. Med. 2015, 72, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Seidler, A.; Euler, U.; Müller-Quernheim, J.; Gaede, K.; Latza, U.; Groneberg, D.; Letzel, S. Systematic review: Progression of beryllium sensitization to chronic beryllium disease. Occup. Med. 2012, 62, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Brink, M.; Schaffer, B.; Pieren, R.; Wunderli, J.M. Conversion between noise exposure indicators Leq24h, LDay, LEvening, LNight, Ldn and Lden: Principles and practical guidance. Int. J. Hyg. Environ. Health 2018, 221, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Fixed-Effect Versus Random-Effects Models. In Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Chichester, UK, 2009; pp. 77–86. [Google Scholar] [CrossRef]
- Clark, C.; Head, J.; Stansfeld, S.A. Longitudinal effects of aircraft noise exposure on children’s health and cognition: A six-year follow-up of the UK RANCH cohort. J. Environ. Psychol. 2013, 35, 1–9. [Google Scholar] [CrossRef]
- Crombie, R.; Clark, C.; Stansfeld, S.A. Environmental noise exposure, early biological risk and mental health in nine to ten year old children: A cross-sectional field study. Environ. Health A Glob. Access Sci. Source 2011, 10, 39. [Google Scholar] [CrossRef]
- Haines, M.M.; Stansfeld, S.A.; Brentnall, S.; Head, J.; Berry, B.; Jiggins, M.; Hygge, S. The West London Schools Study: The effects of chronic aircraft noise exposure on child health. Psychol. Med. 2001, 31, 1385–1396. [Google Scholar] [CrossRef]
- Haines, M.M.; Stansfeld, S.A.; Job, R.F.; Berglund, B.; Head, J. Chronic aircraft noise exposure, stress responses, mental health and cognitive performance in school children. Psychol. Med. 2001, 31, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Haines, M.M.; Stansfeld, S.A.; Job, R.F.; Berglund, B.; Head, J. A follow-up study of effects of chronic aircraft noise exposure on child stress responses and cognition. Int. J. Epidemiol. 2001, 30, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Hjortebjerg, D.; Andersen, A.M.N.; Christensen, J.S.; Ketzel, M.; Raaschou-Nielsen, O.; Sunyer, J.; Julvez, J.; Forns, J.; Sorensen, M. Exposure to road traffic noise and behavioral problems in 7-year-old children: A cohort study. Environ. Health Perspect. 2016, 124, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Kweon, K.; Kim, H.W.; Cho, S.W.; Park, J.; Sim, C.S. Negative impact of noise and noise sensitivity on mental health in childhood. Noise Health 2018, 20, 199–211. [Google Scholar] [PubMed]
- Stansfeld, S.A.; Haines, M.M.; Berry, B.; Burr, M. Reduction of road traffic noise and mental health: An intervention study. Noise Health 2009, 11, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Weyde, K.V.; Krog, N.H.; Oftedal, B.; Magnus, P.; White, R.; Stansfeld, S.; Overland, S.; Aasvang, G.M. A Longitudinal Study of Road Traffic Noise and Body Mass Index Trajectories from Birth to 8 Years. Epidemiology 2018, 29, 729–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forns, J.; Dadvand, P.; Foraster, M.; Alvarez-Pedrerol, M.; Rivas, I.; Lopez-Vicente, M.; Suades-Gonzalez, E.; Garcia-Esteban, R.; Esnaola, M.; Cirach, M.; et al. Traffic-Related Air Pollution, Noise at School, and Behavioral Problems in Barcelona Schoolchildren: A Cross-Sectional Study. Environ. Health Perspect. 2016, 124, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Belojevic, G.; Evans, G.W.; Paunovic, K.; Jakovljevic, B. Traffic noise and executive functioning in urban primary school children: The moderating role of gender. J. Environ. Psychol. 2012, 32, 337–341. [Google Scholar] [CrossRef]
- Stansfeld, S.A.; Berglund, B.; Clark, C.; Lopez-Barrio, I.; Fischer, P.; Ohrstrom, E.; Haines, M.M.; Head, J.; Hygge, S.; van Kamp, I.; et al. Aircraft and road traffic noise and children’s cognition and health: A cross-national study. Lancet 2005, 365, 1942–1949. [Google Scholar] [CrossRef]
- Clark, C.; Crombie, R.; Head, J.; van Kamp, I.; van Kempen, E.; Stansfeld, S.A. Does traffic-related air pollution explain associations of aircraft and road traffic noise exposure on children’s health and cognition? A secondary analysis of the United Kingdom sample from the RANCH project. Am. J. Epidemiol. 2012, 176, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Dreger, S.; Meyer, N.; Fromme, H.; Bolte, G. Environmental noise and incident mental health problems: A prospective cohort study among school children in Germany. Environ. Res. 2015, 143, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Ristovska, G.; Gjorgjev, D.; Jordanova, N.P. Psychosocial effects of community noise: Cross sectional study of school children in urban center of Skopje, Macedonia. Croat. Med. J. 2004, 45, 473–476. [Google Scholar] [PubMed]
- Van Kempen, E.E.; Van Kamp, I.; Stellato, R.K.; Lopez-Barrio, I.; Haines, M.M.; Nilsson, M.E.; Clark, C.; Houthuijs, D.; Brunekreef, B.; Berglund, B. Children’s annoyance reactions to aircraft and road traffic noise. J. Acoust. Soc. Am. 2009, 125, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Stansfeld, S.; Clark, C. Health effects of noise exposure in children. Curr. Environ. Health Rep. 2015, 2, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Klatte, M.; Spilski, J.; Mayerl, J.; Möhler, U.; Lachmann, T.; Bergström, K. Effects of Aircraft Noise on Reading and Quality of Life in Primary School Children in Germany: Results from the NORAH Study. Environ. Behav. 2017, 49, 390–424. [Google Scholar] [CrossRef]
- Klatte, M.; Hellbrück, J.; Seidel, J.; Leistner, P. Effects of classroom acoustics on performance and well-being in elementary school children: A field study. Environ. Behav. 2010, 42, 659–692. [Google Scholar] [CrossRef]
- Paavonen, E.J.; Porkka-Heiskanen, T.; Lahikainen, A.R. Sleep quality, duration and behavioral symptoms among 5-6-year-old children. Eur. Child Adolesc. Psychiatry 2009, 18, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Paavonen, E.J.; Raikkonen, K.; Lahti, J.; Komsi, N.; Heinonen, K.; Pesonen, A.K.; Jarvenpaa, A.L.; Strandberg, T.; Kajantie, E.; Porkka-Heiskanen, T. Short sleep duration and behavioral symptoms of attention-deficit/hyperactivity disorder in healthy 7-to 8-year-old children. Pediatrics 2009, 123, e857–e864. [Google Scholar] [CrossRef]
- Yoon, S.Y.; Jain, U.; Shapiro, C. Sleep in attention-deficit/hyperactivity disorder in children and adults: Past, present, and future. Sleep Med. Rev. 2012, 16, 371–388. [Google Scholar] [CrossRef]
- Goodman, R.; Scott, S. Comparing the Strengths and Difficulties Questionnaire and the Child Behavior Checklist: Is Small Beautiful? J. Abnorm. Child. Psychol. 1999, 27, 17–24. [Google Scholar] [CrossRef]
- Miedema, H.M.E.; Vos, H. Associations Between Self-Reported Sleep Disturbance and Environmental Noise Based on Reanalyses of Pooled Data From 24 Studies. Behav. Sleep Med. 2007, 5, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Van Kamp, I.; Davies, H. Noise and health in vulnerable groups: A review. Noise Health 2013, 15, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Hornberg, C.; Pauli, A. Child poverty and environmental justice. Int. J. Hyg. Environ. Health 2007, 210, 571–580. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Category | Inclusion | Exclusion |
|---|---|---|
| Population | Children sampled from the general population | Animal studies; occupational populations, non-representative (i.e., convenience) samples |
| Exposure | Road traffic, railway or aircraft noise assessed objectively (i.e., measurements or noise modelling at place of residence or at school) | Military aircraft noise; industrial noise; studies considering only neighborhood noise |
| Outcomes | Behavioral and emotional disorders in children (ICD-10 F90–F98) (i.e., diagnosed disorders, e.g., self-reported, routine data; prescribed medications specific to a psychological disorder; validated screening instrument) | Annoyance; sleep disturbance; conditions not directly related to a clinical diagnosis; screening instrument was not validated |
| Study | Region(s) Study Design Quality Score (++,+,-) | Population | Outcome Assessment | Noise Source/Location | Noise Parameters | Noise Categories | Effect Estimates; Meta-Analysis (Yes, No With Reasons) |
|---|---|---|---|---|---|---|---|
| Belojevic et al. 2012 [42] | Serbia cross-sectional (-) | N = 311 (M = 146, F = 165) 7–11 Years | Adapted ADD Questionnaire | Road home and at school | calculated L24h | Continuous analysis | Beta (adjusted) no: continuous endpoints |
| Clark et al. 2013 [32] | UK cohort (-) | N = 461 (M = 202, F = 259) 15–17 Years | SDQ | aircraft road at school | Leq, 07–23h | Continuous analysis | Beta (adjusted) no: continuous endpoints |
| Crombie et al. 2011 [33] with Stansfeld et al. 2005 [43], Clark et al. 2012 [44] | UK, Spain, NL cross-sectional (-) | N = 1900 (M = 897, F = 1003) Mean Age: 10.6 Years | SDQ | aircraft road at school | Leq, 07–23h | Continuous analysis | Beta (adjusted) no: continuous endpoints |
| Forns et al. 2016 [41] | Spain cross-sectional (-) | N = 2897 (M = 1446, F = 1430) 7–11 Years | SDQADHD-DSM-IV | traffic in one classroom per school | - | Continuous analysis | Adjusted mean ratio no: continuous endpoints |
| Haines et al. 2001 [34,35,36] | UK cohort/ cross-sectional (+)/(-) | N = 275/N = 451 (M = 143, F = 132) 10 Years | SDQCDICMAS | aircraft at school | Leq, 07–23h | High noise: Leq,23–07h > 63 dBL eq,23–07h ≥ 66 dB | Averages (matched) no: only group averages reported |
| Hjortebjerg et al. 2016 [37] | Denmark cohort (+) | N = 46,940 7 years | SDQ | Road a railway b at home | Leq,23–07h LDEN | Continuous (per 10 dB) | Odds Ratio (adjusted) yes |
| Lim et al. 2018 [38] | South Korea cross-sectional (-) | N = 918 (M = 427, F = 491) Mean Age: 11.5 years | CBCL | roadat school | LDN | Continuous (per 5 dB) | Odds Ratio(adjusted) yes |
| Stansfeld et al. 2009 [39] | UK, Spain, NL cross-sectional (-) | N = 2014 9–10 years | SDQ | airwayroadat school | Leq, 07–23h | Continuous analysis | Beta (adjusted) no: continuous endpoints |
| Tiesler et al. 2013 [20] | Germany Cross-sectional (-) | N = 872 (M = 410, F = 462) 10 years | SDQ | roadat home | Leq,22–06h c LDEN | Continuous (per IQR d) | Odds Ratio (adjusted) yes |
| Weyde et al. 2018 [40] | Norwaycohort (+) | N = 1934 (prenatal) N = 1384 (postnatal) M = 47.5–52.5% | RSDBD | Road e at home | LDEN | Continuous analysis | Beta (adjusted) no: continuous endpoints |
| Depression | Anxiety | Hyperactivity/Inattention | Conduct Problems | Emotional Symptoms | Peer Problems | Psychosocial Behavior | SDQ/CBCL Total a | ||
|---|---|---|---|---|---|---|---|---|---|
| Noise at school | |||||||||
| Belojevic 2012 (road) | continuous | ↑ b | O | ||||||
| Clark 2013 (aircraft) | β per 1 dB | O | O | O | O | ||||
| Crombie et al. 2011 with Stansfeld et al. 2005 [43], Clark et al. 2012 [44] (aircraft/road) | β per 1 dB | Air (↑)/Road O | Air O/Road ↓ | Air O/Road O | Air O/Road O | ||||
| Forns 2016 (‘traffic’) | continuous | ↑ c | |||||||
| Haines 2001 (a,b,c) (aircraft) | Mean diff. High v. low | (a) O/(b) O | (a) O/(b) O | (a) O/(c) ↑ | (a) O/(c) O | (a) O/(c) O | (a) O/(c) O | (a) O | (a) O/(c) ↑ |
| Lim 2018 (road) | per 1 dB | O d | O d | ↑ d | |||||
| Stansfeld 2009 (aircraft/road) | β per 1 dB | Air ↑/Road O | Air O/Road ↑ | Air O/Road O | Air O/Road O | Air O/Road O | |||
| Noise at home | |||||||||
| Hjortebjerg 2016 (road/railway) e | OR per 10 dB | Road ↑/Rail O | Road O/Rail O | Road O/Rail O | Road O/Rail ↑ | ||||
| Tiesler 2013 (road) | OR per 10 dB | ↑ | O | O | O | O | |||
| Weyde 2017 (road) e | fractional logit (continuous) | ↑ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schubert, M.; Hegewald, J.; Freiberg, A.; Starke, K.R.; Augustin, F.; Riedel-Heller, S.G.; Zeeb, H.; Seidler, A. Behavioral and Emotional Disorders and Transportation Noise among Children and Adolescents: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183336
Schubert M, Hegewald J, Freiberg A, Starke KR, Augustin F, Riedel-Heller SG, Zeeb H, Seidler A. Behavioral and Emotional Disorders and Transportation Noise among Children and Adolescents: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(18):3336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183336
Chicago/Turabian StyleSchubert, Melanie, Janice Hegewald, Alice Freiberg, Karla Romero Starke, Franziska Augustin, Steffi G. Riedel-Heller, Hajo Zeeb, and Andreas Seidler. 2019. "Behavioral and Emotional Disorders and Transportation Noise among Children and Adolescents: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 18: 3336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183336