Standing Desks in a Grade 4 Classroom over the Full School Year

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
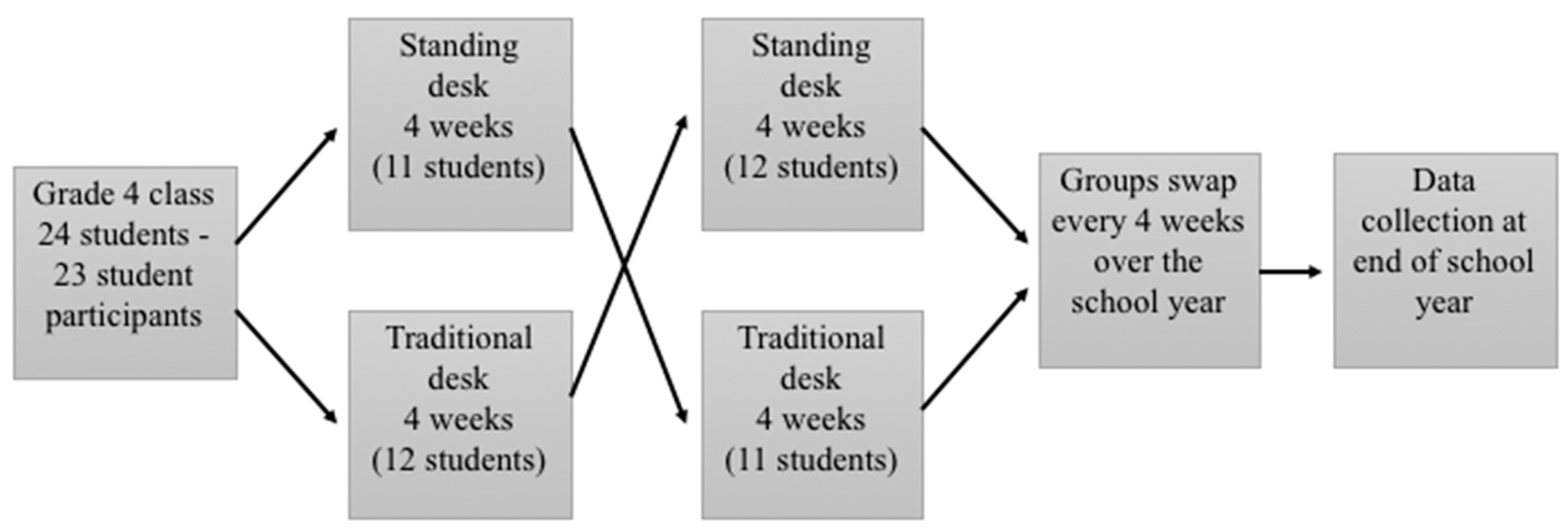
2.1. Study Design and Equipment
2.2. Participants
2.3. Outcome Measures
2.3.1. Accelerometer Data
2.3.2. Musculoskeletal Data
2.4. Analysis
3. Results
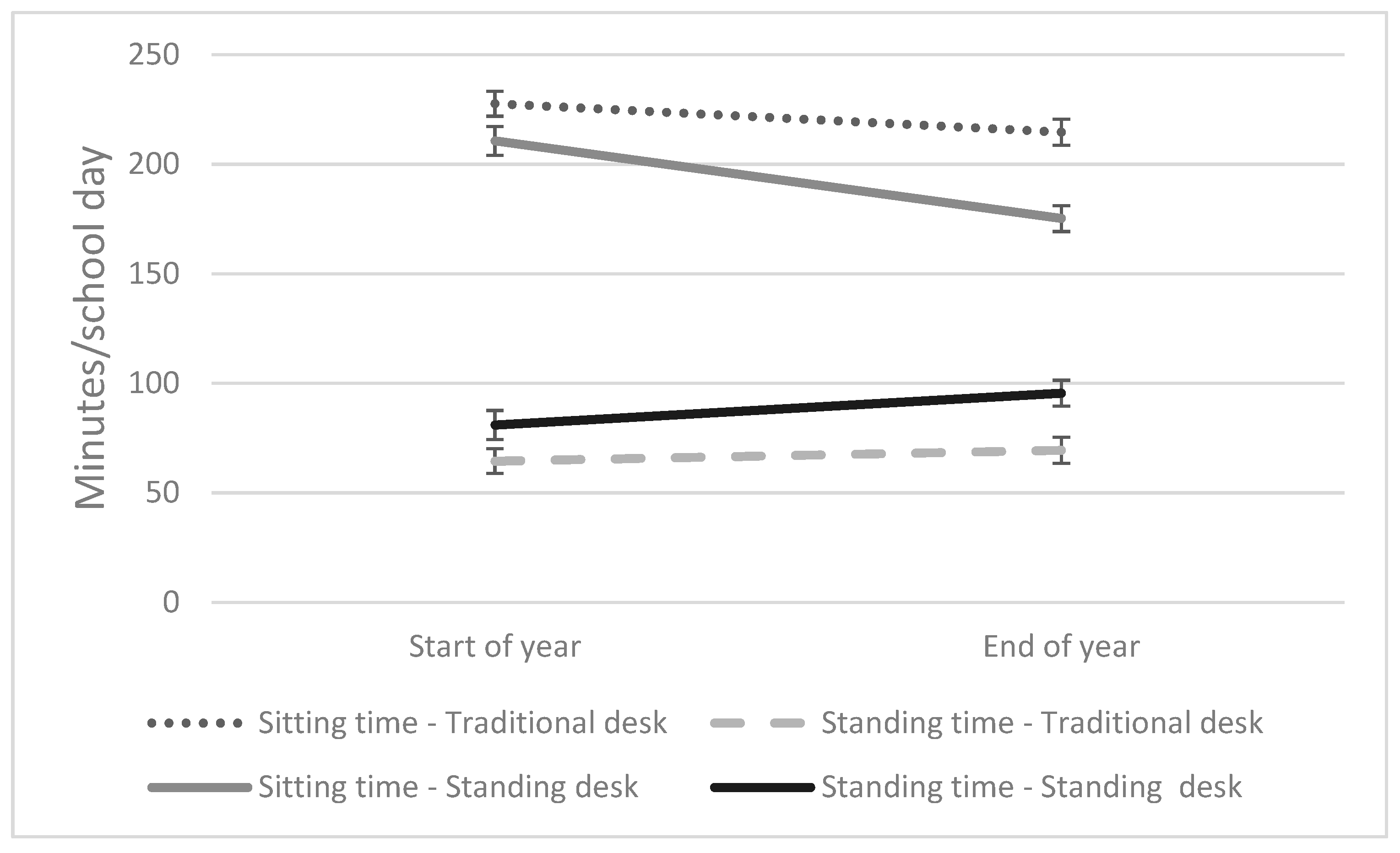
3.1. School-Time Standing and Sitting Time
3.2. Waking-Time Physical Activity and Sedentary Time
3.3. Muculoskeletal Discomfort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yang, L.; Cao, C.; Kantor, E.D.; Nguyen, L.H.; Zheng, X.; Park, Y.; Giovannucci, E.L.; Matthews, C.E.; Colditz, G.A.; Cao, Y. Trends in Sedentary Behavior Among the US Population, 2001-2016. JAMA 2019, 321, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- Alley, S.; Wellens, P.; Schoeppe, S.; de Vries, H.; Rebar, A.L.; Short, C.E.; Duncan, M.J.; Vandelanotte, C. Impact of increasing social media use on sitting time and body mass index. Health Promot. J. Aust. 2017, 28, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Arundell, L.; Salmon, J.; Veitch, J.; Timperio, A. The Relationship between Objectively Measured and Self-Reported Sedentary Behaviours and Social Connectedness among Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 18. [Google Scholar] [CrossRef] [PubMed]
- Colley, R.C.; Garriguet, D.; Janssen, I.; Craig, C.L.; Clarke, J.; Tremblay, M.S. Physical activity of Canadian children and youth: Accelerometer results from the 2007 to 2009 Canadian health measures survey. Health Rep. 2011, 22, 15–23. [Google Scholar] [PubMed]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Gorber, S.C. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T. Role of low energy expenditure and sitting in obesity, metabolic syndrome, Type-2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in sedentary time. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Television time and continuous metabolic risk in physically active adults. Med. Sci. Sports Exerc. 2008, 40, 639–645. [Google Scholar] [CrossRef]
- Larsson, S.C.; Wolk, A. Sedentary leisure-time in relation to mortality and survival time. J. Sci. Med. Sport 2019, 22, 562–567. [Google Scholar] [CrossRef]
- Thorp, A.; Owen, N.; Neuhaus, M.; Dunstan, D. Sedentary behaviours and subsequent health outcomes in adults—A systematic review of longitudinal studies 1996-2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, C.M.; Srinivasan, K.; Gilligan, B.; Razjouyan, J.; Lee, H.; Najafi, B.; Canada, K.J.; Mehl, M.R.; Currim, F.; Ram, S.; et al. Effects of office workstation type on physical activity and stress. Occup. Environ. Med. 2018, 75, 689–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupont, F.; Leger, P.M.; Begon, M.; Lecot, F.; Senecal, S.; Labonte-Lemoyne, E.; Mathieu, M.E. Health and productivity at work: Which active workstation for which benefits: A systematic review. Occup. Environ. Med. 2019, 76, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Straker, L. Evidence to design ‘just right’ work using active workstations is currently limited. Occup. Environ. Med. 2019, 76, 279–280. [Google Scholar] [CrossRef] [PubMed]
- Mielke, G.I.; Brown, W.J.; Wehrmeister, F.C.; Goncalves, H.; Oliveira, I.; Menezes, A.M.; Hallal, P.C. Associations between self-reported physical activity and screen time with cardiometabolic risk factors in adolescents: Findings from the 1993 Pelotas (Brazil) Birth Cohort Study. Prev. Med. 2019, 119, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Russ, S.A.; Larson, K.; Franke, T.M.; Halfon, N. Associations between media use and health in US children. Acad. Pediatr. 2009, 9, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Sibley, B.A.; Etnier, J. The relationship between physical activity and cognition in children: A meta-analysis. Pediatr. Exerc. Sci. 2003, 15, 243–256. [Google Scholar] [CrossRef]
- Stanczykiewicz, B.; Banik, A.; Knoll, N.; Keller, J.; Hohl, D.H.; Rosinczuk, J.; Luszczynska, A. Sedentary behaviors and anxiety among children, adolescents and adults: A systematic review and meta-analysis. BMC Public Health 2019, 19, 459. [Google Scholar] [CrossRef]
- Hakala, P.T.; Rimpelä, A.H.; Saarni, L.A.; Salminen, J.J. Frequent computer-related activities increase the risk of neck–shoulder and low back pain in adolescents. Eur. J. Public Health 2006, 16, 536–541. [Google Scholar] [CrossRef]
- Jacobs, K.; Hudak, S.; McGiffert, J. Computer-related posture and musculoskeletal discomfort in middle school students. Work 2009, 32, 275–283. [Google Scholar] [CrossRef]
- Torsheim, T.; Eriksson, L.; Schnohr, C.W.; Hansen, F.; Bjarnason, T.; Välimaa, R. Screen-based activities and physical complaints among adolescents from the Nordic countries. BMC Public Health 2010, 10, 324. [Google Scholar] [CrossRef] [PubMed]
- Ee, J.; Parry, S.; Oliveira, B.I.; McVeigh, J.A.; Howie, E.; Straker, L. Does a Classroom Standing Desk Intervention Modify Standing and Sitting Behaviour and Musculoskeletal Symptoms during School Time and Physical Activity during Waking Time? Int. J. Environ. Res. Public Health 2018, 15, 1668. [Google Scholar] [CrossRef] [PubMed]
- Minges, K.E.; Chao, A.M.; Irwin, M.L.; Owen, N.; Park, C.; Whittemore, R.; Salmon, J. Classroom standing desks and sedentary behavior: A systematic review. Pediatrics 2016, 137, e20153087. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.R.; Minderico, C.S.; Pinto, F.; Collings, P.J.; Cyrino, E.S.; Sardinha, L.B. Impact of a classroom standing desk intervention on daily objectively measured sedentary behavior and physical activity in youth. J. Sci. Med. Sport 2018, 21, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Verloigne, M.; Ridgers, N.D.; De Bourdeaudhuij, I.; Cardon, G. Effect and process evaluation of implementing standing desks in primary and secondary schools in Belgium: A cluster-randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 94. [Google Scholar] [CrossRef] [PubMed]
- Waddington, G.S. Standing desks at school improve students overall standing time. J. Sci. Med. Sport 2018, 21, 871. [Google Scholar] [CrossRef]
- Wick, K.; Faude, O.; Manes, S.; Zahner, L.; Donath, L. I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children. Int. J. Environ. Res. Public Health 2018, 15, 356. [Google Scholar] [CrossRef]
- Rowlands, A.V. Accelerometer assessment of physical activity in children: An update. Pediatr. Exerc. Sci. 2007, 19, 252–266. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Rowlands, A.V.; Bunnewell, S.; Sanders, J.; Esliger, D.W.; Gorely, T.; O’Connell, S.; Davies, M.; Khunti, K.; Yates, T. Accuracy of posture allocation algorithms for thigh- and waist-worn accelerometers. Med. Sci. Sports Exerc. 2016, 48, 1085–1090. [Google Scholar] [CrossRef]
- Steeves, J.A.; Bowles, H.R.; McClain, J.J.; Dodd, K.W.; Brychta, R.J.; Wang, J.; Chen, K.Y. Ability of thigh-worn Actigraph and Activpal monitors to classify posture and motion. Med. Sci. Sports Exerc. 2015, 47, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Borghese, M.M.; Tremblay, M.S.; LeBlanc, A.G.; Leduc, G.; Boyer, C.; Chaput, J.P. Comparison of Actigraph GT3xX+ and Actical accelerometer data in 9–11-year-old Canadian children. J. Sports Sci. 2017, 35, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Robusto, K.M.; Trost, S.G. Comparison of three generations of Actigraph™ activity monitors in children and adolescents. J. Sports Sci. 2012, 30, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- McVeigh, J.A.; Winkler, E.A.H.; Healy, G.N.; Slater, J.; Eastwood, P.R.; Straker, L.M. Validity of an automated algorithm to identify waking and in-bed wear time in hip-worn accelerometer data collected with a 24 h wear protocol in young adults. Physiol. Meas. 2016, 37, 1636–1652. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Rich, C.; Geraci, M.; Griffiths, L.; Sera, F.; Dezateux, C.; Cortina-Borja, M. Quality control methods in accelerometer data processing: Defining minimum wear time. PLoS ONE 2013, 8, e67206. [Google Scholar] [CrossRef]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic Questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Straker, L.M. Body discomfort assessment tools. In The Occupational Ergonomics Handbook; Karwowski, W., Marras, W.S., Eds.; CRC Press: Boca Raton, FL, USA, 1999; pp. 1239–1252. [Google Scholar]
- Aminian, S.; Hinckson, E.A.; Stewart, T. Modifying the classroom environment to increase standing and reduce sitting. Build. Res. Inf. 2015, 43, 631–645. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Aminian, S.; Ikeda, E.; Stewart, T.; Oliver, M.; Duncan, S.; Schofield, G. Acceptability of standing workstations in elementary schools: A pilot study. Prev. Med. 2013, 56, 82–85. [Google Scholar] [CrossRef]
- Legault, E.P.; Cantin, V.; Descarreaux, M. Assessment of musculoskeletal symptoms and their impacts in the adolescent population: Adaptation and validation of a questionnaire. BMC Pediatr. 2014, 14, 173. [Google Scholar] [CrossRef]
- Baker, R.; Coenen, P.; Howie, E.; Lee, J.; Williamson, A.; Straker, L. Musculoskeletal and Cognitive Effects of a Movement Intervention During Prolonged Standing for Office Work. Hum. Factors 2018, 60, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Coenen, P.; Parry, S.; Willenberg, L.; Shi, J.W.; Romero, L.; Blackwood, D.M.; Healy, G.N.; Dunstan, D.W.; Straker, L.M. Associations of prolonged standing with musculoskeletal symptoms-A systematic review of laboratory studies. Gait Posture 2017, 58, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Coenen, P.; van der Molen, H.F.; Burdorf, A.; Huysmans, M.A.; Straker, L.; Frings-Dresen, M.H.; van der Beek, A.J. Associations of screen work with neck and upper extremity symptoms: A systematic review with meta-analysis. Occup. Environ. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Cardon, G.; De Clercq, D.; De Bourdeaudhuij, I.; Breithecker, D. Sitting habits in elementary schoolchildren: A traditional versus a “moving school”. Patient Educ. Couns. 2004, 54, 133–142. [Google Scholar] [CrossRef]
- Coenen, P.; Willenberg, L.; Parry, S.; Shi, J.W.; Romero, L.; Blackwood, D.M.; Maher, C.G.; Healy, G.N.; Dunstan, D.W.; Straker, L.M. Associations of occupational standing with musculoskeletal symptoms: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 176–183. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Start of School Year | End of School Year | Interaction Effect * (95% Confidence Intervals) | ||
|---|---|---|---|---|
| Mean (SD) total waking time/day (min) | Standing Desk | 785 (92) | 759 (92) | |
| Traditional Seated desk | 770 (119) | 730 (66) | ||
| Sedentary time (% waking hours (SD)) | Standing Desk | 51.4 (2.0) | 49.2 (1.9) | |
| Traditional Seated desk | 48.6 (1.9) | 45 (1.8) | −4.6 to 7.3 | |
| Light activity (% waking hours (SD)) | Standing Desk | 42.8 (1.8) | 44.6 (1.7) | |
| Traditional Seated desk | 44.9 (1.7) | 48.8 (1.6) | −7.4 to 3.7 | |
| Moderate activity (% waking hours (SD)) | Standing Desk | 4.8 (0.4) | 4.9 (0.4) | |
| Traditional Seated desk | 5.2 (0.4) | 5.3 (0.4) | −1.3 to 1.4 | |
| Vigorous activity (% waking hours (SD)) | Standing Desk | 1.1 (0.2) | 1.4 (0.2) | |
| Traditional Seated desk | 1.2 (0.2) | 1.0 (0.2) | −0.2 to 1.2 |
| Logistical Regression on Pain Indicator (Probability of Any Pain) | |||||||
|---|---|---|---|---|---|---|---|
| Condition | Start of School Year | End of School Year | |||||
| Probability (pain) | 95% CI | Probability (pain) | 95% CI | p * | p ** | ||
| Neck | Traditional Seated Desk | 0.50 | 0.35–0.66 | 0.50 | 0.34–0.65 | 0.890 | 0.004 |
| Standing Desk | 0.41 | 0.27–0.55 | 0.41 | 0.27–0.55 | |||
| Shoulder | Traditional Seated Desk | 0.48 | 0.30–0.66 | 0.47 | 0.29–0.65 | 0.837 | <0.001 |
| Standing Desk | 0.37 | 0.24–0.50 | 0.37 | 0.24–0.50 | |||
| Elbow | Traditional Seated Desk | 0.37 | 0.24–0.50 | 0.37 | 0.24–0.49 | 0.828 | 0.489 |
| Standing Desk | 0.35 | 0.23–0.47 | 0.35 | 0.23–0.48 | |||
| Wrist | Traditional Seated Desk | 0.45 | 0.29–0.62 | 0.44 | 0.28–0.61 | 0.835 | 0.479 |
| Standing Desk | 0.43 | 0.27–0.59 | 0.43 | 0.27–0.59 | |||
| Upper back | Traditional Seated Desk | 0.44 | 0.29–0.59 | 0.44 | 0.29–0.58 | 0.881 | 0.640 |
| Standing Desk | 0.43 | 0.28–0.57 | 0.43 | 0.28–0.57 | |||
| Lower back | Traditional Seated Desk | 0.34 | 0.23–0.45 | 0.33 | 0.23–0.43 | 0.829 | 0.327 |
| Standing Desk | 0.32 | 0.24–0.41 | 0.32 | 0.24–0.41 | |||
| Hips/thighs | Traditional Seated Desk | 0.49 | 0.33–0.64 | 0.48 | 0.32–0.63 | 0.856 | 0.985 |
| Standing Desk | 0.49 | 0.33–0.64 | 0.49 | 0.33–0.64 | |||
| Knees | Traditional Seated Desk | 0.47 | 0.29–0.65 | 0.46 | 0.28–0.64 | 0.753 | 0.174 |
| Standing Desk | 0.43 | 0.26–0.59 | 0.43 | 0.26–0.60 | |||
| Ankles/feet | Traditional Seated Desk | 0.63 | 0.49–0.76 | 0.62 | 0.48–0.76 | 0.837 | 0.345 |
| Standing Desk | 0.65 | 0.54–0.76 | 0.65 | 0.53–0.76 | |||
| Pain Intensity Score | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Condition | Start of School Year | End of School Year | |||||||
| Estimate Mean (Pain Score/10) | Estimate Mean (Pain Score/10) | Estimate Mean Diff | 95% CI | p * | Overall Estimate Mean Difference Between Conditions | 95% CI | p ** | ||
| Neck | Traditional Seated Desk | 4.73 | 4.68 | −0.01 | −0.21, 0.18 | 0.943 | −0.44 | −0.59, −0.29 | <0.001 |
| Standing Desk | 3.01 | 3.01 | 0.00 | −0.23, 0.23 | |||||
| Shoulder | Traditional Seated Desk | 5.06 | 4.97 | −0.02 | −0.23, 0.20 | 0.914 | −0.44 | −0.61, −0.27 | <0.001 |
| Standing Desk | 3.23 | 3.23 | 0.00 | −0.25, 0.25 | |||||
| Elbow | Traditional Seated Desk | 2.79 | 2.74 | −0.02 | −0.28, 0.25 | 0.896 | −0.27 | −0.47, −0.06 | 0.054 |
| Standing Desk | 2.11 | 2.13 | 0.01 | −0.28, 0.29 | |||||
| Wrist | Traditional Seated Desk | 4.85 | 4.77 | −0.02 | −0.20, 0.17 | 0.908 | −0.15 | −0.29, −0.01 | 0.120 |
| Standing Desk | 4.15 | 4.15 | 0.00 | −0.20, 0.20 | |||||
| Upper Back | Traditional Seated Desk | 3.75 | 3.69 | −0.02 | −0.25, 0.21 | 0.924 | −0.09 | −0.26, 0.09 | 0.436 |
| Standing Desk | 3.41 | 3.41 | 0.00 | −0.25, 0.24 | |||||
| Lower Back | Traditional Seated Desk | 1.61 | 1.61 | 0.00 | −0.21, 0.21 | 0.914 | −0.17 | −0.31, −0.05 | 0.051 |
| Standing Desk | 1.32 | 1.31 | −0.17 | −0.35, 0.02 | |||||
| Hips/thighs | Traditional Seated Desk | 3.34 | 3.29 | −0.02 | −0.20, 0.17 | 0.916 | −0.17 | −0.31, −0.03 | 0.084 |
| Standing Desk | 2.80 | 2.79 | 0.00 | −0.21, 0.21 | |||||
| Knees | Traditional Seated Desk | 4.81 | 4.72 | −0.02 | −0.22, 0.18 | 0.882 | −0.31 | −0.47, −0.15 | 0.004 |
| Standing Desk | 3.48 | 3.50 | 0.00 | −0.22, 0.23 | |||||
| Ankle/feet | Traditional Seated Desk | 5.32 | 5.24 | −0.02 | −0.20, 0.17 | 0.913 | −0.10 | −0.24, 0.04 | 0.279 |
| Standing Desk | 4.78 | 4.77 | −0.09 | −0.29, 0.10 | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parry, S.; IR de Oliveira, B.; McVeigh, J.A.; Ee, J.; Jacques, A.; Straker, L. Standing Desks in a Grade 4 Classroom over the Full School Year. Int. J. Environ. Res. Public Health 2019, 16, 3590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193590
Parry S, IR de Oliveira B, McVeigh JA, Ee J, Jacques A, Straker L. Standing Desks in a Grade 4 Classroom over the Full School Year. International Journal of Environmental Research and Public Health. 2019; 16(19):3590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193590
Chicago/Turabian StyleParry, Sharon, Beatriz IR de Oliveira, Joanne A. McVeigh, Joyln Ee, Angela Jacques, and Leon Straker. 2019. "Standing Desks in a Grade 4 Classroom over the Full School Year" International Journal of Environmental Research and Public Health 16, no. 19: 3590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193590