Comparison of ICDAS, CAST, Nyvad’s Criteria, and WHO-DMFT for Caries Detection in a Sample of Italian Schoolchildren



Abstract
:
1. Introduction
2. Material and Methods
2.1. Training and Calibration of the Examiners
2.2. Data Collection (Clinical Examinations)
2.3. Caries Detection Methods
2.4. Data Analysis
3. Results
3.1. Calibration
3.2. Survey
4. Discussion
5. Conclusions
- A certain grade of accordance among all the methods was found for severe caries levels, while no accordance for the initial (enamel) lesions.
- From a clinical, epidemiological, and research prospective, both the severity and the activity of a caries lesion are important factors to consider.
- A common language in caries detection is crucial when different studies are compared.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lagerweij, M.D.; van Loveren, C. Declining caries trends: Are we satisfied? Curr. Oral Health Rep. 2015, 2, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. GBD 2015 Oral Health Collaborators: Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [PubMed]
- Hosseinpoor, A.R.; Itani, L.; Petersen, P.E. Socio-economic inequality in oral healthcare coverage: Results from the World Health Survey. J. Dent. Res. 2012, 91, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Machiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A.; et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Klein, H.; Palmer, C. Studies on dental caries vs. familial resemblance in the caries experience of siblings. Pub. Health Rep. 1938, 53, 1353–1364. [Google Scholar] [CrossRef]
- Larmas, M. Has dental caries prevalence some connection with caries index values in adults? Caries Res. 2010, 44, 81–84. [Google Scholar] [CrossRef] [PubMed]
- WHO (World Health Organization). Oral Health Surveys: Basic Methods, 5th ed.; WHO: Monts, France, 2013; pp. 42–47. [Google Scholar]
- Wang, H.Y.; Petersen, P.E.; Bian, J.Y.; Zhang, B.X. The second national survey of oral health status of children and adults in China. Int. Dent. J. 2002, 54, 283–290. [Google Scholar]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Commun. Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef]
- Pitts, N.B.; Ekstrand, K.R. ICDAS Foundation: International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)-Methods for staging of the caries process and enabling dentists to manage caries. Commun. Dent. Oral Epidemiol. 2013, 41, 41–52. [Google Scholar] [CrossRef]
- Frencken, J.E.; de Souza, A.L.; van der Sanden, W.J.; Bronkhorst, E.M.; Leal, S.C. The Caries Assessment and Treatment (CAST) instrument. Commun. Dent. Oral Epidemiol. 2013, 41, 71–77. [Google Scholar] [CrossRef]
- Leal, S.C.; Ribeiro, A.P.D.; Frencken, J.E. Caries Assessment Spectrum and Treatment (CAST): A Novel Epidemiological Instrument. Caries Res. 2017, 51, 500–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frencken, J.E.; de Amorim, R.G.; Faber, J.; Leal, S.C. The Caries Assessment Spectrum and Treatment (CAST) index: Rational and development. Int. Dent. J. 2011, 61, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Nyvad, B.; Machiulskiene, V.; Baelum, V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res. 1999, 33, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Nyvad, B.; Baelum, V. Nyvad Criteria for Caries Lesion Activity and Severity Assessment: A Validated Approach for Clinical Management and Research. Caries Res. 2018, 52, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.L.S.; Vianna, M.I.P.; Mendes, C.M.C. Comparison of caries lesion detection methods in epidemiological surveys: CAST, ICDAS and DMF. BMC Oral Health 2018, 18, 122. [Google Scholar] [CrossRef]
- Mutsvari, T.; Declerck, D.; Lesaffre, E. Correction for misclassification of caries experience in the absence of internal validation data. Clin. Oral Invest. 2013, 17, 1799–1805. [Google Scholar] [CrossRef]
- Istat National Institute of Statistics. Available online: https://www.istat.it (accessed on 6 September 2016).
- Castiglia, P.; Campus, G.; Solinas, G.; Maida, C.; Strohmenger, L. Children’s oral health in Italy: Training and clinical calibration of examiners for the National Pathfinder about caries disease. Oral Health Prev. Dent. 2007, 5, 255–261. [Google Scholar]
- Bolin, A.K.; Bolin, A.; Koch, G.; Alfredsson, L. Children’s dental health in Europe. Clinical calibration of dental examiners in eight EU countries. Swed. Dent. J. 1995, 19, 183–193. [Google Scholar]
- Whelton, H. Overview of the impact of changing global patterns of dental caries experience on caries clinical trials. J. Dent. Res. 2004, 83, 29–34. [Google Scholar] [CrossRef]
- Fleiss, J.L. Reliability of Measurements. In The Design and Analysis of Clinical Experiments; Fleiss, J.L., Ed.; John Wiley and Sons: New York, NY, USA, 1986; pp. 1–32. [Google Scholar]
- Jamieson, L.M.; Thomson, W.M.; Gee, R. An assessment of the validity and reliability of dental self-report items used in a National Child Nutrition Survey. Commun. Dent. Oral Epidemiol. 2004, 32, 49–54. [Google Scholar] [CrossRef]
- Solinas, G.; Campus, G.; Maida, C.; Sotgiu, G.; Cagetti, M.G.; Lesaffre, E.; Castiglia, P. What statistical method should be used to evaluate risk factors associated with dmfs index? Evidence from the National Pathfinder Survey of 4-year-old Italian children. Commun. Dent. Oral Epidemiol. 2009, 37, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Innes, N.P.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.J.; Ricketts, D.; Van Landuyt, K.; Banerjee, A.; Campus, G.; Doméjean, S.; et al. Managing Carious Lesions: Consensus Recommendations on Terminology. Adv. Dent. Res. 2016, 28, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melgar, R.A.; Pereira, J.T.; Luz, P.B.; Hugo, F.N.; Araujo, F.B. Differential Impacts of Caries Classification in Children and Adults: A Comparison of ICDAS and DMF-T. Braz. Dent. J. 2016, 27, 761–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.N.; Eaton, K.A.; Pitts, N.B.; Schulte, A.; Pieper, K.; White, S. Variation in methods used to determine national mean DMFT scores for 12-year-old children in European countries. Commun. Dent. Health 2013, 33, 286–291. [Google Scholar]
- Altman, D.G. Practical Statistics for Medical Research; Chapman & Hall: London, UK, 1991; pp. 396–409. [Google Scholar]
- Bhoopathi, P.H.; Patil, P.U.; Kamath, B.V.; Gopal, D.; Kumar, S.; Kulkarni, G. Caries Detection with ICDAS and the WHO Criteria: A Comparitive Study. J. Clin. Diagn. Res. 2017, 11, 9–12. [Google Scholar] [CrossRef]
- Campus, G.; Solinas, G.; Cagetti, M.G.; Senna, A.; Minelli, L.; Majori, S.; Montagna, M.T.; Reali, D.; Castiglia, P.; Strohmenger, L. National Pathfinder survey of 12-year-old Children’s Oral Health in Italy. Caries Res. 2007, 41, 512–517. [Google Scholar] [CrossRef]

{kind=link}
| Lesion Stage | WHO-DMFT | ICDAS | CAST | Nyvad Criteria |
|---|---|---|---|---|
| No lesion (sound) | ||||
| First visual change in enamel (dry) | ||||
| Distinct visual change in enamel | ||||
| Active intact surface | ||||
| Inactive intact surface | ||||
| Enamel discontinuity | ||||
| Integrity loss/Active discontinuity | ||||
| Grey shadow/Dentine | + | |||
| Distinct/Active cavity | + | |||
| Extensive distinct cavity | ||||
| Inactive caries discontinuity | ||||
| Inactive cavity | ||||
| Pulp involvement | ||||
| Abscess/Fistula | ||||
| Missing tooth for caries | ||||
| Missing tooth for other reason | ||||
| Unerupted | ||||
| Sealant | ^ | |||
| Filling (sound surface) | * | |||
| Filling + active caries | ||||
| Filling + inactive caries | ||||
| Temporary filling |
| Measure | Samples |
|---|---|
| n (%) | |
| Gender | |
| Males | 236 (47.20) |
| Females | 264 (52.80) |
| Maternal Nationality | |
| European Union | 455 (91.00) |
| Not European Union | 45 (9.00) |
| Educational level of the mother | |
| Compulsory education | 224 (44.80) |
| Secondary school | 121 (24.20) |
| University | 155 (31.00) |
| Educational level of the father | |
| Compulsory education | 242 (48.40) |
| Secondary school | 141 (28.20) |
| University | 117 (23.40) |
| Occupational status of the mother | |
| Housewife | 126 (25.20) |
| Unemployed | 102 (20.40) |
| Clerks | 131 (26.20) |
| Self-employed | 141 (28.20) |
| Frequency of toothbrushing | |
| 1/day | 28 (5.60) |
| 2/day | 73 (14.60) |
| >2 day | 399 (79.80) |
| Inter-Examiner Agreement vs. Benchmark | Intra-Examiner Calibration | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Session 1 | Session 2 | Session1/Session 2 | ||||||||
| Methods | Examiner | K-Cohen | K-Cohen | K-Cohen | K-Cohen | K-Cohen | K-Cohen | K-Cohen | K-Cohen | K-Cohen |
| (Sound) | (Distinct Caries) | (Total) | (Sound) | (Distinct Caries) | (Total) | (Sound) | (Distinct Caries) | (Total) | ||
| WHO-DMFT | A | 0.83 | 0.81 | 0.87 | 0.91 | 0.87 | 0.88 | 0.94 | 0.83 | 0.84 |
| B | 0.84 | 0.77 | 0.81 | 0.86 | 0.84 | 0.85 | 0.89 | 0.80 | 0.83 | |
| C | 0.89 | 0.81 | 0.86 | 0.92 | 0.86 | 0.88 | 0.91 | 0.84 | 0.85 | |
| D | 0.84 | 0.79 | 0.82 | 0.83 | 0.89 | 0.87 | 0.90 | 0.88 | 0.89 | |
| ICDAS | A | 0.74 | 0.75 | 0.76 | 0.77 | 0.80 | 0.79 | 0.84 | 0.83 | 0.83 |
| B | 0.79 | 0.76 | 0.77 | 0.81 | 0.80 | 0.80 | 0.87 | 0.89 | 0.88 | |
| C | 0.76 | 0.84 | 0.80 | 0.85 | 0.85 | 0.85 | 0.91 | 0.88 | 0.89 | |
| D | 0.72 | 0.77 | 0.74 | 0.74 | 0.82 | 0.78 | 0.87 | 0.86 | 0.86 | |
| CAST | A | 0.73 | 0.72 | 0.72 | 0.81 | 0.83 | 0.82 | 0.87 | 0.84 | 0.86 |
| B | 0.74 | 0.76 | 0.75 | 0.82 | 0.85 | 0.84 | 0.85 | 0.82 | 0.83 | |
| C | 0.82 | 0.78 | 0.80 | 0.83 | 0.90 | 0.86 | 0.92 | 0.89 | 0.90 | |
| D | 0.74 | 0.75 | 0.74 | 0.81 | 0.83 | 0.82 | 0.94 | 0.88 | 0.91 | |
| Nyvad Criteria | A | 0.71 | 0.73 | 0.72 | 0.76 | 0.81 | 0.79 | 0.91 | 0.84 | 0.87 |
| B | 0.77 | 0.74 | 0.75 | 0.80 | 0.82 | 0.81 | 0.92 | 0.88 | 0.90 | |
| C | 0.81 | 0.78 | 0.80 | 0.83 | 0.87 | 0.85 | 0.92 | 0.87 | 0.90 | |
| D | 0.79 | 0.76 | 0.77 | 0.85 | 0.83 | 0.84 | 0.96 | 0.90 | 0.94 | |
| WHO-DMFT | ICDAS | CAST | Nyvad Criteria | |||
|---|---|---|---|---|---|---|
| Sound | Session 1 | Sum of squares | 3971.44 | 3428.16 | 3562.56 | 3629.17 |
| F ratio | 104.27 | 93.63 | 98.18 | 99.25 | ||
| p-value | 0.17 | 0.10 | 0.13 | 0.16 | ||
| Session 2 | Sum of squares | 4217.84 | 3823.54 | 3924.34 | 4202.71 | |
| F ratio | 448.34 | 203.62 | 336.19 | 442.74 | ||
| p-value | 0.21 | 0.16 | 0.16 | 0.17 | ||
| Distinct caries | Session 1 | Sum of squares | 376.220 | 3644.71 | 3802.57 | 3784.71 |
| F ratio | 100.41 | 97.85 | 102.72 | 101.57 | ||
| p-value | 0.13 | 0.12 | 0.14 | 0.13 | ||
| Session 2 | Sum of squares | 428.331 | 4072.56 | 4188.67 | 4266.51 | |
| F ratio | 477.53 | 284.52 | 432.32 | 461.74 | ||
| p-value | 0.17 | 0.16 | 0.17 | 0.17 |
| WHO-DMFT | Sound | Distinct Cavity | Filling | Missing Tooth | Sealant | Total | Misclassification |
|---|---|---|---|---|---|---|---|
| N % | |||||||
| Sound | 563 | 2 | 0 | 0 | 0 | 565 | 5 (0.89) |
| Distinct cavity | 5 | 90 | 0 | 0 | 0 | 95 | 5 (5.55) |
| Filling | 0 | 0 | 19 | 0 | 1 | 20 | 1 (5.26) |
| Missing tooth | 0 | 0 | 0 | 1 | 0 | 1 | - |
| Sealant | 0 | 1 | 1 | 0 | 17 | 19 | 2 (7.14) |
| Total | 568 | 93 | 20 | 1 | 18 | 700 | 13 (1.86) |
| ICDAS | Sound | Enamel Opacity | Enamel Opacity Wet | Integrity Loss | Grey Shadow | Distinct Cavity | Pulp Involv. | Filling | Missing Tooth | Sealant | Total | Misclassification N (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sound | 145 | 12 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 3 | 163 | 18 (12.41) |
| Enamel opacity | 11 | 93 | 13 | 0 | 4 | 0 | 0 | 0 | 0 | 0 | 121 | 28 (30.11) |
| Enamel opacity wet | 2 | 9 | 111 | 1 | 9 | 0 | 0 | 0 | 0 | 0 | 132 | 23 (20.72) |
| Integrity loss | 0 | 0 | 2 | 65 | 3 | 0 | 0 | 0 | 0 | 0 | 70 | 12 (18.46) |
| Grey shadow | 1 | 2 | 9 | 0 | 47 | 6 | 0 | 0 | 0 | 0 | 65 | 22(46.81) |
| Distinct cavity | 0 | 0 | 0 | 10 | 6 | 83 | 2 | 0 | 0 | 0 | 101 | 18 (21.69) |
| Pulp involvement | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 0 | 0 | 0 | 9 | - |
| Filling | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 19 | 0 | 1 | 20 | 1 (5.26) |
| Missing tooth | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 19 | - |
| Sealant | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 18 | 19 | 3 (16.67) |
| Total | 159 | 116 | 137 | 77 | 70 | 89 | 11 | 19 | 1 | 22 | 700 | 125 (17.86) |
| CAST | Sound | Enamel Discontinuity | Grey Shadow | Distinct Cavity | Pulp Involv. | Filling | Missing Tooth | Sealant | Total | Misclassification N (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Sound | 245 | 12 | 0 | 0 | 0 | 0 | 0 | 4 | 261 | 20 (8.16) |
| Enamel discontinuity | 20 | 178 | 5 | 3 | 0 | 0 | 0 | 0 | 206 | 24 (13.48) |
| Grey shadow | 0 | 10 | 67 | 0 | 0 | 0 | 0 | 0 | 77 | 20 (20.91) |
| Distinct cavity | 0 | 2 | 9 | 95 | 1 | 0 | 0 | 0 | 107 | 12 (12.63) |
| Pulp involvement | 0 | 0 | 0 | 1 | 9 | 0 | 0 | 0 | 10 | 1 (11.11) |
| Filling | 0 | 0 | 0 | 0 | 0 | 19 | 0 | 1 | 20 | 1 (5.26) |
| Missing tooth | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | - |
| Sealant | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 18 | 18 | 5 (21.73) |
| Total | 265 | 202 | 81 | 99 | 10 | 19 | 1 | 23 | 700 | 83 (11.86) |
| NYVAD | Sound | Activity No Cavity | Inactive No Cavity | Active Discontinuity | Active Cavity | Inactive Discontinuity | Inactive Cavity | Total | Misclassification N (%) |
|---|---|---|---|---|---|---|---|---|---|
| Sound | 169 | 0 | 12 | 0 | 0 | 0 | 0 | 181 | 12 (7.10) |
| Activity no cavity | 0 | 91 | 8 | 3 | 0 | 0 | 0 | 102 | 19 (20.90) |
| Inactive no cavity | 9 | 15 | 82 | 1 | 0 | 0 | 0 | 107 | 25 (30:49) |
| Active discontinuity | 0 | 4 | 3 | 75 | 1 | 0 | 0 | 83 | 8 (10.67) |
| Active cavity | 0 | 0 | 0 | 3 | 113 | 0 | 10 | 126 | 13 (11.50) |
| Inactive discontinuity | 2 | 0 | 0 | 0 | 0 | 16 | 0 | 18 | 2 (12.50) |
| Inactive cavity | 0 | 0 | 0 | 0 | 12 | 0 | 33 | 45 | 12 (36.36) |
| Total | 180 | 110 | 105 | 82 | 126 | 16 | 43 | 662 | 91 (13.00) |
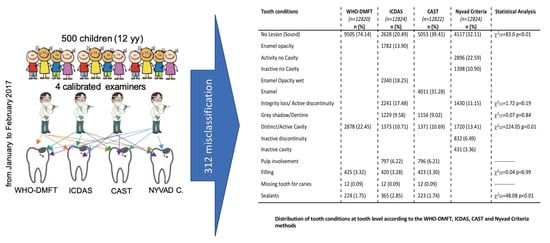
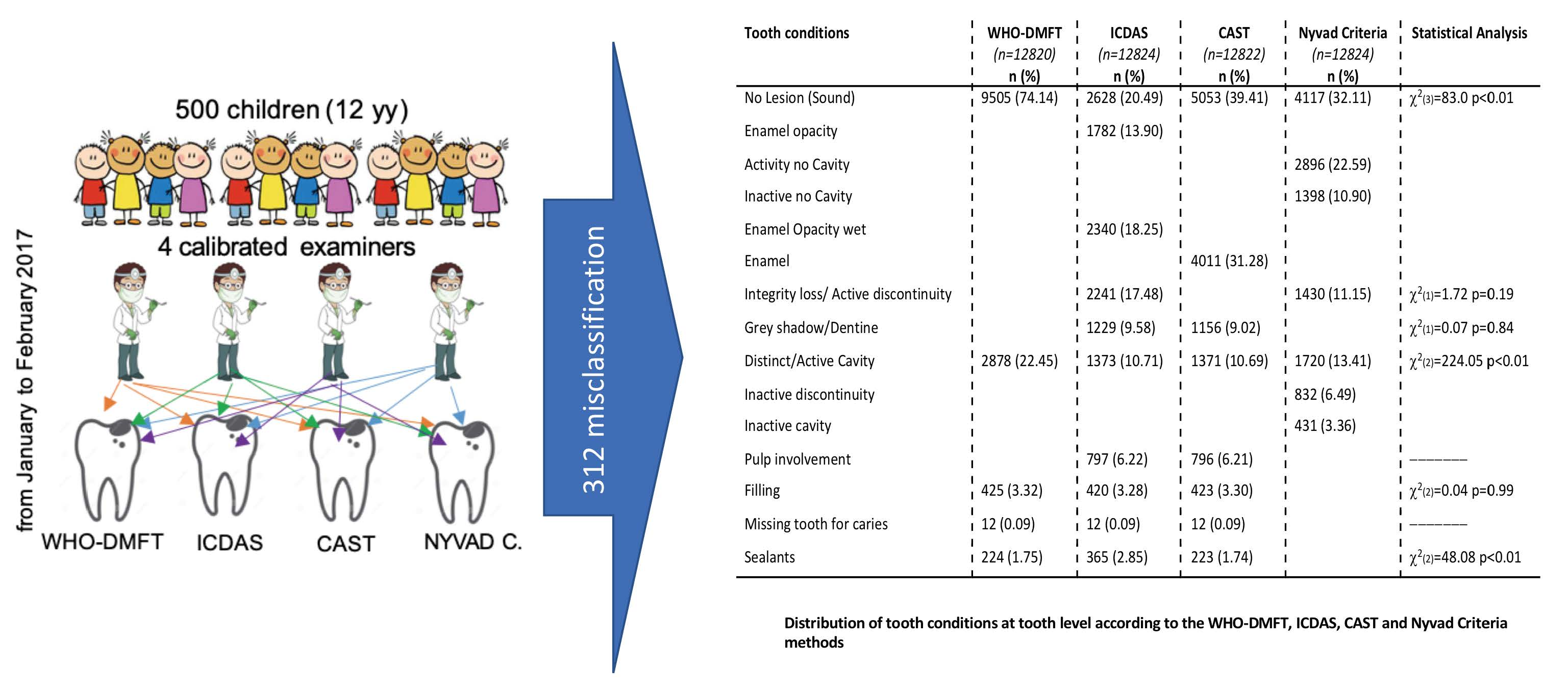
| Tooth Conditions | WHO-DMFT (n = 12,820) n (%) | ICDAS (n = 12,824) n (%) | CAST (n = 12,822) n (%) | Nyvad Criteria (n = 12,824) n (%) | Statistical Analysis |
|---|---|---|---|---|---|
| No lesion (Sound) | 9505 (74.14) | 2628 (20.49) | 5053 (39.41) | 4117 (32.11) | χ2(3) = 83.0 p < 0.01 |
| Enamel opacity | 1782 (13.90) | ||||
| Activity no cavity | 2896 (22.59) | ||||
| Inactive no cavity | 1398 (10.90) | ||||
| Enamel opacity wet | 2340 (18.25) | ||||
| Enamel | 4011 (31.28) | ||||
| Integrity loss/Active discontinuity | 2241 (17.48) | 1430 (11.15) | χ2(1) = 1.72 p = 0.19 | ||
| Grey shadow/Dentine | 1229 (9.58) | 1156 (9.02) | χ2(1) = 0.07 p = 0.84 | ||
| Distinct/Active cavity | 2878 (22.45) | 1373 (10.71) | 1371 (10.69) | 1720 (13.41) | χ2(2) = 224.05 p < 0.01 |
| Inactive discontinuity | 832 (6.49) | ||||
| Inactive cavity | 431 (3.36) | ||||
| Pulp involvement | 797 (6.22) | 796 (6.21) | ------------ | ||
| Filling | 425 (3.32) | 420 (3.28) | 423 (3.30) | χ2(2) = 0.04 p = 0.99 | |
| Missing tooth for caries | 12 (0.09) | 12 (0.09) | 12 (0.09) | ---------- | |
| Sealants | 224 (1.75) | 365 (2.85) | 223 (1.74) | χ2(2) = 48.08 p < 0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campus, G.; Cocco, F.; Ottolenghi, L.; Cagetti, M.G. Comparison of ICDAS, CAST, Nyvad’s Criteria, and WHO-DMFT for Caries Detection in a Sample of Italian Schoolchildren. Int. J. Environ. Res. Public Health 2019, 16, 4120. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214120
Campus G, Cocco F, Ottolenghi L, Cagetti MG. Comparison of ICDAS, CAST, Nyvad’s Criteria, and WHO-DMFT for Caries Detection in a Sample of Italian Schoolchildren. International Journal of Environmental Research and Public Health. 2019; 16(21):4120. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214120
Chicago/Turabian StyleCampus, Guglielmo, Fabio Cocco, Livia Ottolenghi, and Maria Grazia Cagetti. 2019. "Comparison of ICDAS, CAST, Nyvad’s Criteria, and WHO-DMFT for Caries Detection in a Sample of Italian Schoolchildren" International Journal of Environmental Research and Public Health 16, no. 21: 4120. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214120