The Association between Difficulty Seeing and Physical Activity among 17,777 Adults Residing in Spain



Abstract
:1. Introduction
2. Methods
2.1. The Survey
2.2. Difficulty Seeing (Exposure)
2.3. Physical Activity (Outcome)
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Blindness and Vision Impairment. Available online: https://www.who.int/blindness/en/ (accessed on 22 August 2019).
- Liu, Y.C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J.S. Cataracts. Lancet 2017, 390, 600–612. [Google Scholar] [CrossRef]
- Seddon, J.; Fong, D.; West, S.K.; Valmadrid, C.T. Epidemiology of risk factors for age-related cataract. Surv. Ophthalmol. 1995, 39, 323–334. [Google Scholar] [CrossRef]
- Chatterjee, A.; Milton, R.C.; Thyle, S. Prevalence and aetiology of cataract in Punjab. Br. J. Ophthalmol. 1982, 66, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Vrensen, G.F. Early cortical lens opacities: A short overview. Acta Ophthalmol. 2009, 87, 602–610. [Google Scholar] [CrossRef]
- Klein, B.; Klein, R.; Jensen, S.C.; Linton, K.L. Hypertension and lens opacities from the Beaver Dam Eye Study. Am. J. Ophthalmol. 1995, 119, 640–646. [Google Scholar] [CrossRef]
- Leske, M.C.; Wu, S.Y.; Hennis, A.; Connell, A.M.; Hyman, L.; Schachat, A. Diabetes, hypertension, and central obesity as cataract risk factors in a black population: The Barbados Eye Study. Ophthalmology 1999, 106, 35–41. [Google Scholar] [CrossRef]
- Pollreisz, A.; Schmidt-Erfurth, U. Diabetic Cataract—Pathogenesis, Epidemiology and Treatment. J. Ophthalmol. 2010, 608751, 1–8. [Google Scholar] [CrossRef]
- Keel, S.; He, M. Risk factors for age-related cataract. Clin. Exp. Ophthalmol. 2018, 46, 327–328. [Google Scholar] [CrossRef]
- Capella-McDonnall, M. The need for health promotion for adults who are visually impaired. J. Vis. Impair. Blind. 2007, 101, 133–145. [Google Scholar] [CrossRef]
- NHS UK: Physical Activity Guidelines for Older Adults. Available online: https://www.nhs.uk/live-well/exercise/physical-activity-guidelines-older-adults/ (accessed on 22 August 2019).
- Smith, L.; Timmis, M.A.; Pardhan, S.; Latham, K.; Johnstone, J.; Hamer, M. Physical inactivity in relation to self-rated eyesight: Cross-sectional analysis from the English Longitudinal Study of Ageing. BMJ Open Ophth. 2016, 1, e000046. [Google Scholar] [CrossRef]
- Smith, L.; Jackson, S.E.; Pardhan, S.; López-Sánchez, G.F.; Liang, H.; Cao, C.; Vancampfort, D.; Koyanagi, A.; Stubbs, B.; Firth, J.; et al. Visual impairment and objectively measured physical activity and sedentary behaviour in US adolescents and adults: A cross-sectional study. BMJ Open 2019, 9, e027267. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.K.; Ozturk, M.A.; Kozub, F.M. Physical activity and social engagement patterns during physical education of youth with visual impairments. ProQuest 2004, 36, 39e49. [Google Scholar] [CrossRef]
- Houwen, S.; Hartman, E.; Visser, C. Physical activity and motor skills in children with and without visual impairments. Med. Sci. Sports Exerc. 2009, 41, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Keil, S.; Lord, C.; Lloyd, C.L. Sight Impairment at Age Eleven: Secondary Analysis of the Millennium Cohort Survey. Available online: https://www.bl.uk/britishlibrary/~/media/bl/global/social-welfare/pdfs/non-secure/s/i/g/sight-impairment-at-age-eleven-secondary-analysis-of-the-millennium-cohort-survey.pdf (accessed on 2 November 2019).
- Greguol, M.; Gobbi, E.; Carraro, A. Physical activity practice, body image and visual impairment: A comparison between Brazilian and Italian children and adolescents. Res. Dev. Disabil. 2014, 35, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.; Aggio, D.; Stubbs, B.; Pardhan, S.; Gardner, B.; Smith, L. Physical activity levels in children with sensory problems: Cross-sectional analyses from the Millennium Cohort Study. Disabil. Health J. 2018, 1, 58–61. [Google Scholar] [CrossRef]
- Esteban, J.J.; Martínez, M.S.; Navalón, P.G.; Serrano, O.P.; Patiño, J.R.; Purón, M.E.; Martínez-Vizcaíno, V. Visual impairment and quality of life: Gender differences in the elderly in Cuenca, Spain. Qual. Life Res. 2008, 17, 37–45. [Google Scholar] [CrossRef]
- Guisasola, L.; Tresserras-Gaju, R.; García-Subirats, I.; Rius, A.; Brugulat-Guiteras, P. Prevalence and burden of visual impairment in Catalonia, Spain. Med. Clin. (Barc) 2011, 137, 22–26. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Servicios Sociales e Igualdad & Instituto Nacional de Estadística: Spanish National Health Survey 2017: Methodology. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_Metodologia.pdf (accessed on 22 August 2019).
- IPAQ group: Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ). Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 22 August 2019).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Yawson, A.E.; Ackuaku-Dogbe, E.M.; Seneadza, N.A.; Mensah, G.; Minicuci, N.; Naidoo, N.; Chatterji, S.; Kowal, P.; Biritwum, R.B. Self-reported cataracts in older adults in Ghana: Sociodemographic and health related factors. BMC Public Health 2014, 14, 1–8. [Google Scholar] [CrossRef]
- World Health Organization. Prevalence of Insufficient Physical Activity. Available online: https://www.who.int/gho/ncd/risk_factors/physical_activity_text/en/ (accessed on 22 August 2019).
- Zheng Selin, J.; Orsini, N.; Ejdervik Lindblad, B.; Wolk, A. Long-term physical activity and risk of age-related cataract: A population-based prospective study of male and female cohorts. Ophthalmology 2015, 122, 274–280. [Google Scholar] [CrossRef]
- Williams, P.T. Walking and running are associated with similar reductions in cataract risk. Med. Sci. Sports Exerc. 2013, 45, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.T. Prospective Epidemiological Cohort Study of Reduced Risk for Incident Cataract with Vigorous Physical Activity and Cardiorespiratory Fitness during a 7-Year Follow-up. Invest. Ophthalmol. Vis. Sci. 2009, 50, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Phoenix, C.; Griffin, M.; Smith, B. Physical activity among older people with sight loss: A qualitative research study to inform policy and practice. Public Health 2015, 129, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Trott, M.; Smith, L. What are the associations between extroversion, enjoyment, and wellness in group vs non-group physical activity? A pilot study. Atena J. Sports Sci. 2019, 1, 1–11. [Google Scholar]


{kind=link}
| Characteristic | Category | n | Column% | n (%) Doing Less than 600 MET-min/week of PA a | p-Value b | |
|---|---|---|---|---|---|---|
| Age (years) | 15–49 | 10,089 | 56.8 | 2950 | (29.2) | <0.001 |
| 50–64 | 5977 | 33.6 | 1915 | (32.0) | ||
| ≥65 | 1711 | 9.6 | 501 | (29.3) | ||
| Sex | Female | 9248 | 52.0 | 2990 | (32.3) | <0.001 |
| Male | 8529 | 48.0 | 2376 | (27.9) | ||
| Marital status | Married | 10,010 | 56.3 | 3189 | (31.9) | <0.001 |
| Not married | 7767 | 43.7 | 2177 | (28.0) | ||
| Education | ≤Primary | 3324 | 18.7 | 1303 | (39.2) | <0.001 |
| Secondary | 9004 | 50.6 | 2712 | (30.1) | ||
| ≥Tertiary | 5449 | 30.7 | 1351 | (24.8) | ||
| Obesity (BMI ≥ 30 kg/m2) | No | 14,424 | 83.5 | 3992 | (27.7) | <0.001 |
| Yes | 2849 | 16.5 | 1137 | (39.9) | ||
| Missing | 504 | |||||
| Diabetes | No | 16,763 | 94.3 | 5007 | (29.9) | <0.001 |
| Yes | 1014 | 5.7 | 359 | (35.4) | ||
| Hypertension | No | 14,633 | 82.3 | 4261 | (29.1) | <0.001 |
| Yes | 3144 | 17.7 | 1105 | (35.1) | ||
| Cataracts | No | 17,113 | 96.3 | 5113 | (29.9) | <0.001 |
| Yes | 664 | 3.7 | 253 | (38.1) | ||
| Glasses or contact lenses | No | 6653 | 37.4 | 1996 | (30.0) | 0.680 |
| Yes | 11,124 | 62.6 | 3370 | (30.3) | ||
| Smoking | Never | 8198 | 46.1 | 2355 | (28.7) | <0.001 |
| Current | 5071 | 28.5 | 1737 | (34.3) | ||
| Former | 4497 | 25.3 | 1265 | (28.1) | ||
| Missing | 11 | |||||
| Alcohol Consumption | No | 5371 | 30.2 | 1853 | (34.5) | <0.001 |
| Yes | 12,392 | 69.8 | 3505 | (28.3) | ||
| Missing | 14 | |||||
| Difficulty seeing | No | 15,828 | 89.0 | 4646 | (29.4) | <0.001 |
| Yes | 1949 | 11.0 | 720 | (36.9) | ||
| Characteristic | Less than 600 MET-Min/Week of Physical Activity | ||
|---|---|---|---|
| Difficulty seeing | Yes vs. No | 1.222 *** | (1.099, 1.357) |
| Age (years) | 15–49 | 1.515 *** | (1.317, 1.742) |
| 50–64 | 1.378 *** | (1.211, 1.569) | |
| ≥65 | 1.0 | ||
| Sex | Male vs. Female | 1.272 *** | (1.187, 1.364) |
| Marital status | Married vs. Not married | 1.236 *** | (1.154, 1.324) |
| Education | ≤ Primary | 1.763 *** | (1.587, 1.959) |
| Secondary | 1.235 *** | (1.140, 1.338) | |
| ≥ Tertiary | 1.0 | ||
| Obesity | Yes vs. No | 1.605 *** | (1.469, 1.752) |
| Diabetes | Yes vs. No | 1.013 | (0.875, 1.173) |
| Hypertension | Yes vs. No | 1.154 ** | (1.050, 1.270) |
| Cataracts | Yes vs. No | 1.253 * | (1.050, 1.495) |
| Glasses or contact lenses | Yes vs. No | 1.023 | (0.947, 1.106) |
| Smoking | Never | 1.0 | |
| Current | 1.394 *** | (1.287, 1.511) | |
| Former | 1.013 | (0.929, 1.105) | |
| Alcohol consumption | Yes vs. No | 1.190 *** | (1.104, 1.283) |
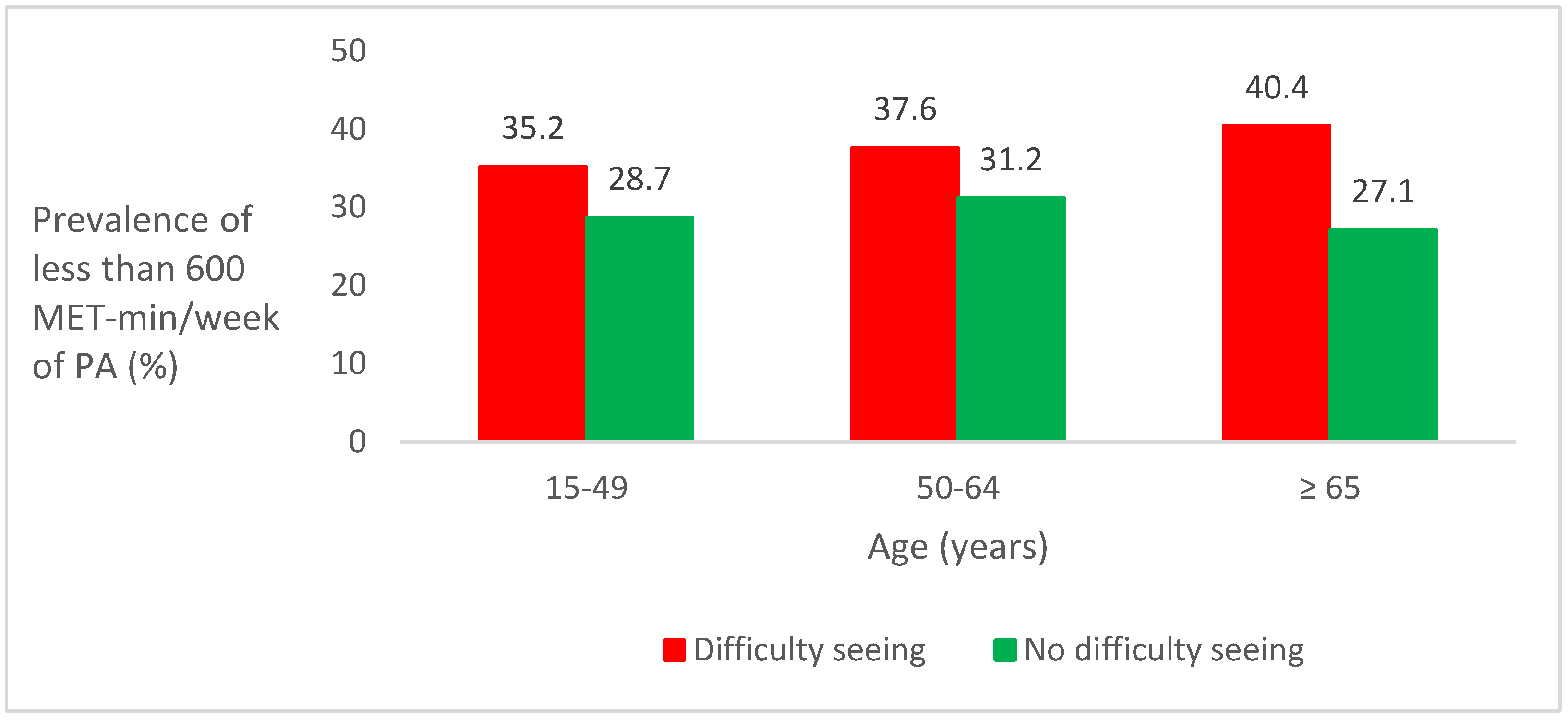
| Age (Years) | Association between Difficulty Seeing and Less than 600 MET-Min/Week of Physical Activity (Outcome) | |
|---|---|---|
| 15–49 | 1.200 * | (1.027, 1.402) |
| 50–64 | 1.149 | (0.972, 1.358) |
| ≥65 | 1.508 ** | (1.124, 2.023) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Sánchez, G.F.; Grabovac, I.; Pizzol, D.; Yang, L.; Smith, L. The Association between Difficulty Seeing and Physical Activity among 17,777 Adults Residing in Spain. Int. J. Environ. Res. Public Health 2019, 16, 4267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214267
López-Sánchez GF, Grabovac I, Pizzol D, Yang L, Smith L. The Association between Difficulty Seeing and Physical Activity among 17,777 Adults Residing in Spain. International Journal of Environmental Research and Public Health. 2019; 16(21):4267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214267
Chicago/Turabian StyleLópez-Sánchez, Guillermo F., Igor Grabovac, Damiano Pizzol, Lin Yang, and Lee Smith. 2019. "The Association between Difficulty Seeing and Physical Activity among 17,777 Adults Residing in Spain" International Journal of Environmental Research and Public Health 16, no. 21: 4267. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214267