Household Food Insecurity, Dietary Diversity, Stunting, and Anaemia among Left-Behind Children in Poor Rural Areas of China


 , and
, and
Abstract
:1. Introduction
2. Method
2.1. Ethical Approval
2.2. Participant Recruitment and Enrollment
2.3. Outcome Variables
2.4. Assessment of Household Food Insecurity
2.5. Assessment of Dietary Intake
2.6. Socioeconomic and Demographic Characteristics
2.7. Statistical Analysis
3. Results
3.1. General Characteristics and Household Food Insecurity
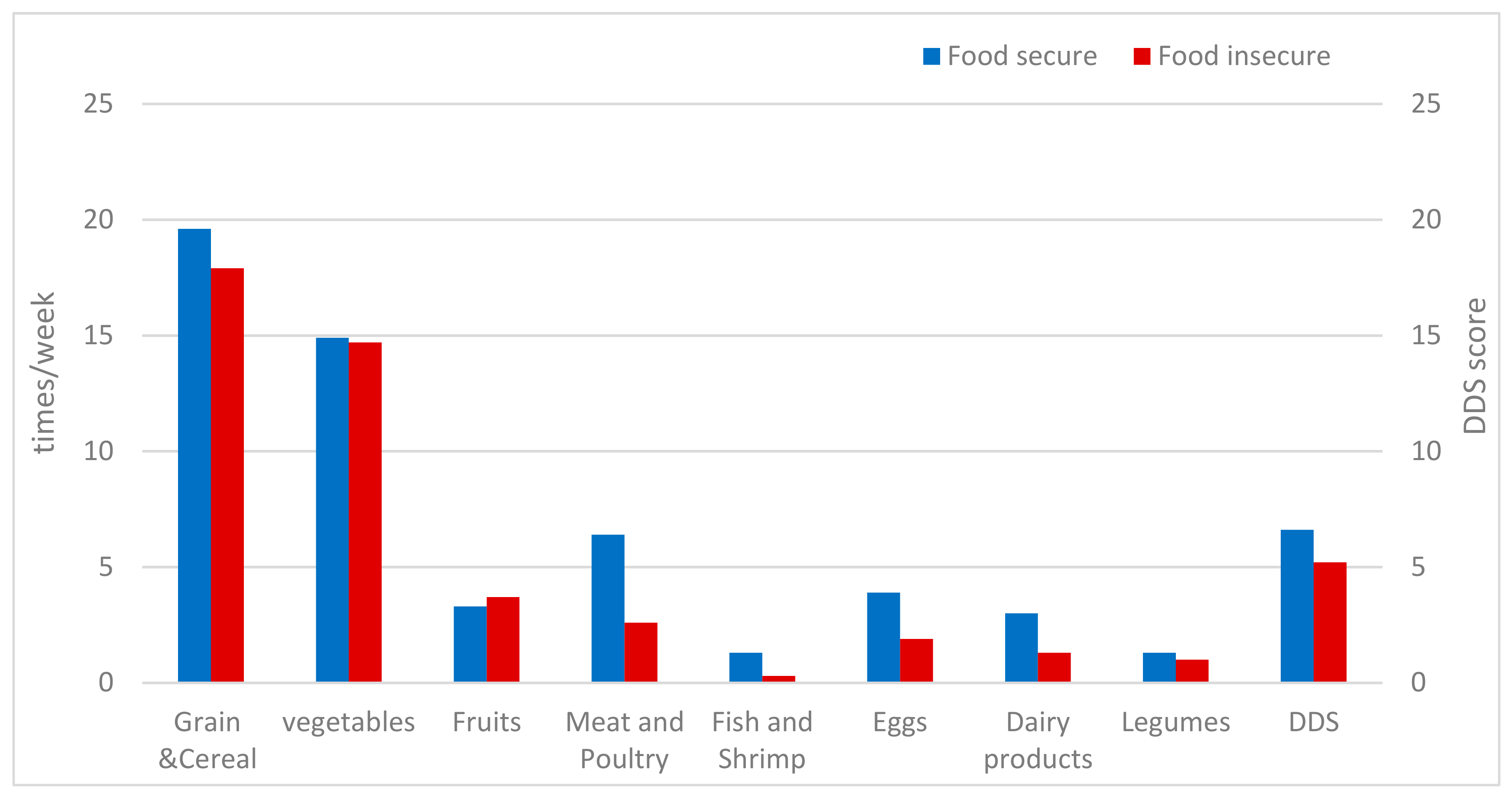
3.2. Household Food Insecure Status and LBC’s Dietary Diversity, Dietary Consumption Frequency
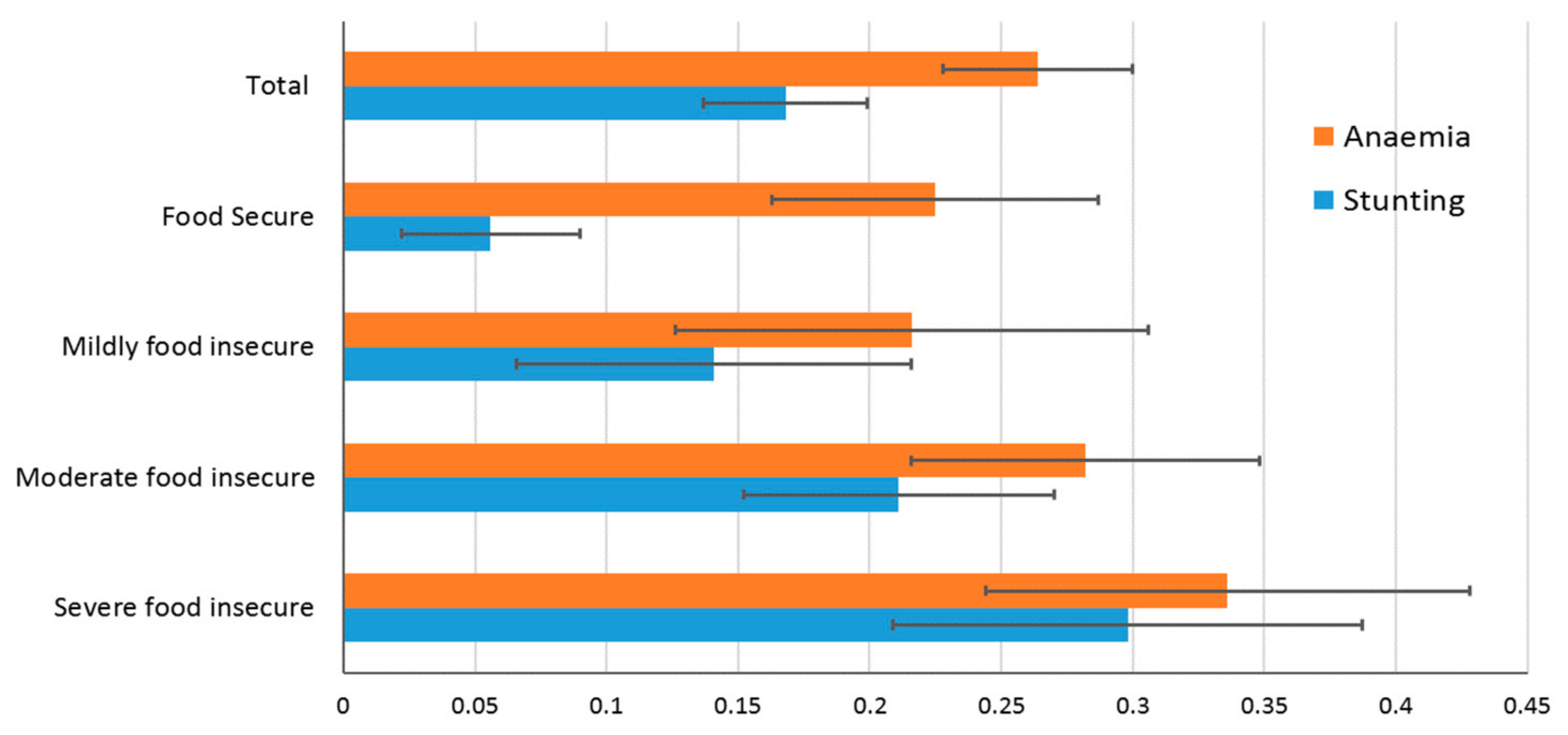
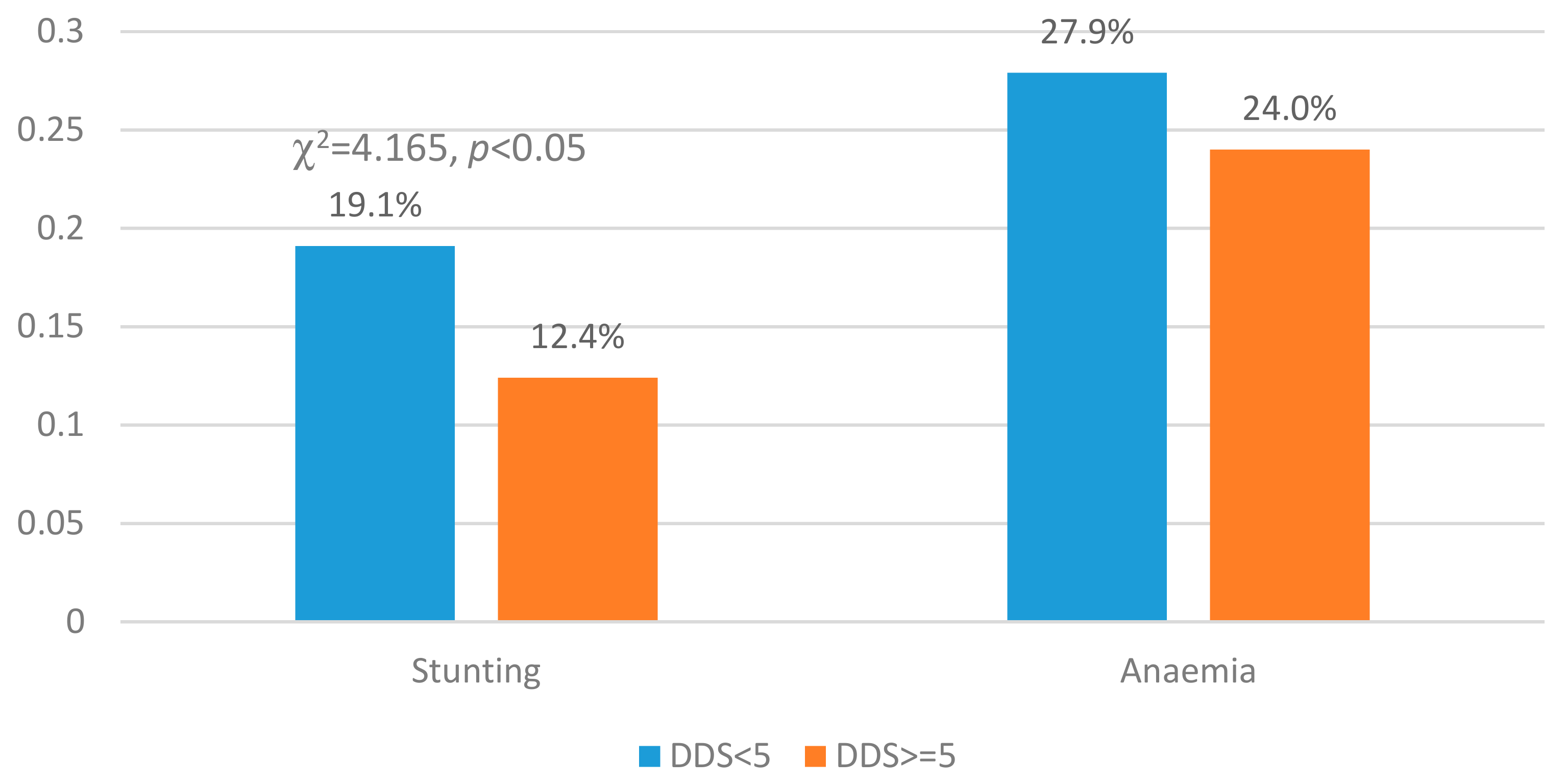
3.3. Stunting and Anaemia by Household Food Insecure Status and DDS
3.4. Association between LBC Stunting and Anaemia and Household Food-Insecure Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chang, H.; Dong, X.Y.; Macphail, F.J.W.D. Labor Migration and Time Use Patterns of the Left-behind Children and Elderly in Rural China. World Dev. 2011, 39, 2199–2210. [Google Scholar] [CrossRef]
- Zhang, J.; Shi, J.; Himes, J.H.; Du, Y.; Yang, S.; Shi, S.; Zhang, J. Undernutrition status of children under 5 years in Chinese rural areas - data from the National Rural Children Growth Standard Survey, 2006. Asia Pac. J. Clin. Nutr. 2011, 20, 584–592. [Google Scholar]
- All-China Women’s Federation. National Rural Left-behind Children Research Report on the Situation of Urban and Rural Migrant Children. Chin. Women’s Mov. 2013, 6, 30–34. [Google Scholar]
- Zhang, N.; Bécares, L.; Chandola, T. A multilevel analysis of the relationship between parental migration and left-behind children’s macronutrient intakes in rural China. Public Health Nutr. 2016, 19, 1913–1927. [Google Scholar] [CrossRef]
- Tian, X.; Ding, C.; Shen, C.; Wang, H. Does Parental Migration Have Negative Impact on the Growth of Left-Behind Children?—New Evidence from Longitudinal Data in Rural China. Int. J. Environ. Res. Public Health 2017, 14, 1308. [Google Scholar] [CrossRef]
- Song, S.; Chen, C.; Zhang, A. Effects of Parental Migration on Life Satisfaction and Academic Achievement of Left-Behind Children in Rural China-A Case Study in Hubei Province. Children 2018, 5, 87. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Bécares, L.; Chandola, T. Patterns and Determinants of Double-Burden of Malnutrition among Rural Children: Evidence from China. PLoS ONE 2016, 11, e0158119. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Sylvia, S.; Zhang, L.; Luo, R.; Yi, H.; Liu, C.; Shi, Y.; Loyalka, P.; Chu, J.; Medina, A.J.H.A. China’s Left-Behind Children: Impact Of Parental Migration On Health, Nutrition, And Educational Outcomes. Health Aff. 2015, 34, 1964–1971. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; He, W.; Wang, Y.; Deng, L.; Jia, F. Nutritional status of children during and post-global economic crisis in China. Biomed. Environ. Sci. 2011, 24, 321–328. [Google Scholar]
- Li, C.M.; Yang, N.; Zhang, J.N. Investigation of Physical Development among Left-behind Children in Rural Areas in Western Hunan Province. Zhong Guo Quan Ke Yi Xue 2011, 9, 26. [Google Scholar]
- Fang, H.; Yu, D.; Guo, Q.; Ju, L.; Xu, X.; Yu, W.; Jia, F.; Zhao, L. Anemia prevalence of among 0–5 years old children in China, 2013. Chin. J. Public Health 2018, 34, 86–89. [Google Scholar]
- UNICEF. Conceptual Frameworks. In The State of the World’s Children; United Nations Children’s Fund: New York, NY, USA, 2016; Available online: http://www.unicef.org/sowc98/pdf.htm (accessed on 7 January 2016).
- US Department of Agriculture, Economic Research Service. Definitions of Food Security; USDA: Washington, DC, USA, 2016. Available online: http://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security.aspx (accessed on 15 May 2016).
- Schmeer, K.K.; Piperata, B.A. Household food insecurity and child health. Matern. Child Nutr. 2017, 13. [Google Scholar] [CrossRef] [PubMed]
- Mary, A.; Marie, T.R. Dietary Diversity Is Associated with Child Nutritional Status: Evidence from 11 Demographic and Health Surveys. J. Nutr. 2004, 134, 2579–2585. [Google Scholar]
- Anqi, W.; Robert, W.S.; Xiaona, H.; Sufang, G. The dietary diversity and stunting prevalence in minority children under 3 years old: A cross-sectional study in forty-two counties of Western China. Br. J. Nutr. 2017, 118, 840–848. [Google Scholar]
- Patric, H.C.; Kitty, S.; Sheely, L.; Margaret, B.; Judy, W. Children in food-insufficient, low-income families: Prevalence, health, and nutrition status. Arch. Pediatr. Adolesc. Med. 2001, 155, 508–514. [Google Scholar]
- Disha, A.; Kuntal, K.K.; Phuong, H.N.; Michael, T.D.; Maire, T.R.; Purnima, M.; Rahul, R. Household food insecurity is associated with higher child undernutrition in Bangladesh, Ethiopia, and Vietnam, but the effect is not mediated by child dietary diversity. J. Nutr. 2013, 143, 2015–2021. [Google Scholar]
- Bernal, J.; Frongillo, E.A.; Herrera, H.A.; Rivera, J.A. Food insecurity in children but not in their mothers is associated with altered activities, school absenteeism, and stunting. J. Nutr. 2014, 144, 1619–1626. [Google Scholar] [CrossRef]
- Mutisya, M.; Kandala, N.B.; Ngware, M.W.; Kabiru, C.W. Household food (in)security and nutritional status of urban poor children aged 6 to 23 months in Kenya. BMC Public Health 2015, 15, 1052. [Google Scholar] [CrossRef]
- Motbainor, A.; Worku, A.; Kumie, A. Stunting Is Associated with Food Diversity while Wasting with Food Insecurity among Underfive Children in East and West Gojjam Zones of Amhara Region, Ethiopia. PLoS ONE 2015, 10, e0133542. [Google Scholar] [CrossRef]
- Shen, X.; Gao, X.; Tang, W.; Mao, X.; Huang, J.; Cai, W. Food insecurity and malnutrition in Chinese elementary school students. Br. J. Nutr. 2015, 114, 952–958. [Google Scholar] [CrossRef]
- Cheng, Y.; Rosenberg, M.; Yu, J.; Zhang, H. Food security for community-living elderly people in Beijing, China. Health Soc. Care Community 2016, 24, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Adab, P.; Hemming, K.; Yang, L.; Qin, H.; Li, M.; Deng, J.; Shi, J.; Chen, J. Health allowance for improving the nutritional status and development of 3-5-year-old left-behind children in poor rural areas of China: Study protocol for a cluster randomised trial. Trials 2015, 16, 361. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; Vitamin and Mineral Nutrition Information System; World Health Organization: Genève, Switzerland, 2012; Available online: http://www.who.int/vmnis/indicators/haemoglobin.pdf (accessed on 1 December 2012).
- Jennifer, C.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide; Version 3; Academy for Educational Development: Washington, DC, USA, 2007; Available online: http://www.fao.org/fileadmin/user_upload/eufao-fsi4dm/doc-training/hfias.pdf (accessed on 15 July 2018).
- Naja, F.; Hwalla, N.; Fossian, T.; Zebian, D.; Nasreddine, L. Validity and reliability of the Arabic version of the Household Food Insecurity Access Scale in rural Lebanon. Public Health Nutr. 2015, 18, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Knueppel, D.; Demment, M.; Kaiser, L. Validation of the Household Food Insecurity Access Scale in rural Tanzania. Public Health Nutr. 2010, 13, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Becquey, E.; Martin-Prevel, Y.; Traissac, P.; Dembélé, B.; Bambara, A.; Delpeuch, F. The household food insecurity access scale and an index-member dietary diversity score contribute valid and complementary information on household food insecurity in an urban West-African setting. J. Nutr. 2010, 140, 2233–2240. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Schatzkin, A.; Harris, T.B.; Ziegler, R.G.; Block, G. Dietary diversity and subsequent mortality in the First National Health and Nutrition Examination Survey Epidemiologic Follow-up Study. Am. J. Clin. Nutr. 1993, 57, 434–440. [Google Scholar] [CrossRef]
- Meng, L.; Wang, Y.; Li, T.; Loo-Bouwman, C.A.V.; Zhang, Y.; Man-Yau Szeto, I. Dietary Diversity and Food Variety in Chinese Children Aged 3–17 Years: Are They Negatively Associated with Dietary Micronutrient Inadequacy? Nutrients 2018, 10, 1674. [Google Scholar] [CrossRef]
- Gao, J.; Fei, J.-Q.; Jiang, L.-J.; Yao, W.-Q.; Lin, B.; Guo, H.-W. Assessment of the Reproducibility and Validity of A Simple Food-frequency Questionnaire Used in Dietary Pattern Studies. Acta Nutr. Sin. 2011, 33, 452–456. [Google Scholar]
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2018; Economic Research Report No. (ERR-270); U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2019.
- Pereira, A.L.; Handa, S.; Holmqvist, G. Prevalence and Correlates of Food Insecurity among Children across the Globe; Innocenti Working Paper WP-2017-09; UNICEF Office of Research: Florence, Italy, 2018; Available online: http://www.unicef-irc.org/publications/900-prevalence-and-correlates-of-food-insecurity-among-children-across-the-globe.html (accessed on 10 November 2019).
- Loopstra, R.; Reeves, A.; Stuckler, D. Rising food insecurity in Europe. Lancet 2015, 385, 2041. [Google Scholar] [CrossRef]
- Massimo, P.M.; Jochen, E.; Michele, S.; Pietro, F.; Ida, G.; Lucian, P.T. Food Insecurity and Children’s Rights to Adequate Nutrition in Europe. J. Pediatr. 2018, 198, 329–330.e1. [Google Scholar]
- Devereux, S.; Tavener-Smith, L. Seasonal Food Insecurity among Farm Workers in the Northern Cape, South Africa. Nutrients 2019, 11, 1535. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Yu, K.; Tan, S.; Zheng, Y.; Zhao, A.; Wang, P.; Zhang, Y. Dietary diversity scores: An indicator of micronutrient inadequacy instead of obesity for Chinese children. BMC Public Health 2017, 17, 440. [Google Scholar] [CrossRef] [PubMed]
- Sriram, U.; Tarasuk, V. Economic predictors of household food insecurity in Canadian metropolitan areas. J. Hunger Environ. Nutr. 2016, 11, 1–13. [Google Scholar] [CrossRef]
- Loopstra, R.; Tarasuk, V. Severity of household food insecurity is sensitive to change in household income and employment status among low-income families. J. Nutr. 2013, 143, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ji, M.; Zou, J.; Yuan, T.; Deng, J.; Yang, L.; Li, M.; Qin, H.; Chen, J.; Lin, Q. Effect of a Conditional Cash Transfer Program on Nutritional Knowledge and Food Practices among Caregivers of 3-5-Year-Old Left-Behind Children in the Rural Hunan Province. Int. J. Environ. Res. Public Health 2018, 15, 525. [Google Scholar] [CrossRef]
- Weigel, M.M.; Armijos, R.X.; Racines, M.; Cevallos, W. Food Insecurity Is Associated with Undernutrition but Not Overnutrition in Ecuadorian Women from Low-Income Urban Neighborhoods. J. Environ. Public Health 2016, 2016, 8149459. [Google Scholar] [CrossRef]
- Hanson, K.L.; Connor, L.M. Food insecurity and dietary quality in US adults and children: A systematic review. Am. J. Clin. Nutr. 2014, 100, 684–692. [Google Scholar] [CrossRef]
- Duan, D.H.; Zhu, M.Y.; Luo, J.Y.; Wang, Z.; Gu, C.H.; Zhang, W.M.; Yao, M.L.; Duan, G.Q. Investigation on dietary nutrients among rural stranded children of 2–7 year olds in china. Zhonghua Liuxingbingxue Zazhi 2009, 30, 326–330. [Google Scholar]
- Heflin, C.; Kukla-Acevedo, S.; Darolia, R. Adolescent food insecurity and risky behaviors and mental health during the transition to adulthood. J. Child. Youth Serv. Rev. 2019, 105, 104416. [Google Scholar] [CrossRef]
- Loopstra, R.; Tarasuk, V. The relationship between food banks and household food insecurity among low-income Toronto families. Can. Public Policy 2012, 38, 497–514. [Google Scholar] [CrossRef]
- Loopstra, R. Interventions to address household food insecurity in high-income countries. Proc. Nutr. Soc. 2018, 77, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Li, Q.; Luo, B.; You, T.; Wang, H. Trend in the nutritional status of children aged 2–7 years in Luoding city, China: A panel study from 2004 to 2013. PLoS ONE 2018, 13, e0205163. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gan, Y.; Guo, C.; Sun, J.; Hao, L. Nutritional status of under-five children from urban low-income families in Xiangtan and Jilin in China. J. Huazhong Univ. Sci. Technol. Med. Sci. 2017, 27, 74–78. [Google Scholar] [CrossRef]
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2016; United States Department of Agriculture, Economic Research Service: Washington, DC, USA, 2017.




{kind=link}
{kind=link}
{kind=link}
| Question | Frequency | ||
|---|---|---|---|
| Rarely: 1 | Sometimes: 2 | Often: 3 | |
| 1a | |||
| 2a | |||
| 3a | |||
| 4a | |||
| 5a | |||
| 6a | |||
| 7a | |||
| 8a | |||
| 9a | |||

| Variables † | Household Food Secure | Mild Food Insecure | Moderate Food Insecure | Severe Food Insecure | Total | p-Value # |
|---|---|---|---|---|---|---|
| N, % | 179, 32.4% | 85, 15.4% | 185, 33.4% | 104, 18.8% | 553, 100% | |
| Region (n, %) | ||||||
| Mountain area | 53, 29.6% | 48, 56.5% | 113, 61.1% | 61, 58.7% | 275, 49.7% | <0.01 |
| Gentle hills | 126, 70.4% | 37, 43.5% | 72, 38.9% | 43, 41.3% | 278, 50.3% | |
| Household SES level (n, %) (tertiles) * | ||||||
| Low | 35, 19.6% | 25, 29.4% | 71, 38.4% | 55, 52.9% | 186, 33.6% | <0.01 |
| Middle | 63, 35.2% | 31, 36.5% | 61, 33.0% | 28, 26.9% | 183, 33.1% | |
| High | 81, 45.2% | 29, 34.1% | 53, 28.6% | 21, 20.2% | 184, 33.3% | |
| LBC’s age (year) | 4.2 ± 0.9 | 4.1 ± 0.9 | 4.1 ± 0.9 | 4.1 ± 1.0 | 4.1 ± 0.9 | 0.920 |
| LBC’s sex (n, %) | ||||||
| Boy | 107, 59.8% | 42, 49.4% | 104, 56.2% | 54, 51.9% | 307, 55.5% | 0.365 |
| Girl | 72, 40.2% | 43, 50.6% | 81, 43.8% | 50, 48.1% | 246, 44.5% | |
| Ethnicity (n, %) | ||||||
| Han | 144, 80.4% | 50, 58.8% | 85, 45.9% | 63, 60.6% | 342, 61.8% | <0.01 |
| Minorities | 35, 19.6% | 35, 41.2% | 100, 54.1% | 41, 39.4% | 211, 38.2% | |
| Left-behind status (n, %) | ||||||
| Single parent out | 35, 19.6% | 18, 21.2% | 56, 30.3% | 31, 29.8% | 140, 25.3% | 0.059 |
| Both parents out | 144, 80.4% | 67, 78.8% | 129, 69.7% | 73, 70.2% | 413, 74.7% | |
| LBC’s DDS | ||||||
| 0–4 | 79, 44.1 | 54, 63.5 | 130, 70.3 | 88, 84.6 | 351, 63.5 | <0.01 |
| ≥5 | 100, 55.9 | 31, 36.5 | 55, 29.7 | 16, 15.4 | 202, 36.5 | |
| Number of LBC in the family (n, %) | ||||||
| 1 | 54, 30.2% | 21, 24.7% | 48, 25.9% | 25, 24.0% | 148, 26.8% | 0.205 |
| 2 | 84, 46.9% | 31, 36.5% | 86, 46.5% | 51, 49.0% | 252, 45.6% | |
| 3 and above | 41, 22.9% | 33, 38.8% | 51, 27.6% | 28, 26.9% | 153, 27.7% | |
| CLBC’s age (year) | 54.6 ± 12.0 | 56.0 ± 11.6 | 56.0 ± 12.7 | 56.0 ± 12.0 | 55.6 ± 12.1 | 0.677 |
| CLBC’s sex (n, %) | ||||||
| Male | 57, 31.8% | 27, 31.8% | 60, 32.4% | 37, 35.6% | 181, 32.7% | 0.921 |
| Female | 122, 68.2% | 58, 68.2% | 125, 67.6% | 67, 64.4% | 372, 67.3% | |
| CLBC’s relationship to LBC (n, %) | ||||||
| Mother | 12, 6.7% | 6, 7.1% | 22, 11.9% | 13, 12.5% | 53, 9.6% | 0.409 |
| Father | 8, 4.5% | 4, 4.7% | 8, 4.3% | 4, 3.8% | 24, 4.3% | |
| Grandparent | 152, 84.9% | 73, 85.9% | 152, 82.2% | 887, 83.7% | 464, 83.9% | |
| Other | 7, 3.9% | 2, 2.4% | 3, 1.6% | 0, 0.0% | 12, 2.2% | |
| CLBC’s education level (n, %) | ||||||
| No formal education | 31, 17.3% | 31, 36.5% | 69, 37.3% | 36, 34.6% | 167, 30.2% | < 0.01 |
| Primary school | 92, 51.4% | 43, 50.6% | 84, 45.4% | 48, 46.2% | 267, 48.3% | |
| Middle school and above | 56, 31.3% | 11, 12.9% | 32, 17.3% | 20, 19.2% | 119, 21.5% | |
| CLBC’s career (n, %) | ||||||
| Non-farmer | 25, 14.0% | 6, 7.1% | 14, 7.6% | 16, 15.4% | 61, 11.0% | 0.066 |
| Farmer | 154, 86.0% | 79, 92.9% | 171, 92.4% | 88, 84.6% | 492, 89.0% | |
| Variables | COR | (95% CI) | AOR | (95% CI) |
|---|---|---|---|---|
| HFI (reference: food-secure) | ||||
| Mildly food-insecure | 2.245 * | (1.098–4.589) | 2.321 * | (1.143–4.714) |
| Moderate food-insecure | 3.511 *** | (1.917–6.428) | 3.585 *** | (1.961–6.554) |
| Severely food-insecure | 17.020 *** | (7.306–39.650) | 17.129 *** | (7.414–39.572) |
| Minorities | 2.084 ** | (1.216–3.572) | 2.143 ** | (1.260–3.644) |
| Socioeconomic status (reference: High) | ||||
| Middle | 1.591 | (0.932–2.718) | 1.582 | (0.932–2.684) |
| Low | 2.020 ** | (1.093–3.735) | 2.063 * | (1.121–3.799) |
| Caregiver’s sex (reference: male) | 0.046 *** | (0.025–0.083) | 0.048 *** | (0.027–0.086) |
| Caregiver’s education (reference: no formal education) | ||||
| Primary school | 0.665 | (0.365–1.210) | 0.656 | (0.363–1.185) |
| Middle school | 0.277 ** | (0.135–3.572) | 0.274 *** | (0.134–0.562) |
| Variables | Household Food Insecurity Status OR (95%CI) | |||
|---|---|---|---|---|
| Food Secure | Mild Food Insecure | Moderate Food Insecure | Severe Food Insecure | |
| Stunting | ||||
| Crude | 1 | 2.778 (1.149–6.718) *** | 4.514 (2.177–9.360) *** | 7.177 (3.344–15.404) * |
| Model 1 † | 1 | 2.925 (1.205–7.099) *** | 4.648 (2.236–9.660) *** | 7.575 (3.511–16.343) * |
| Model 2 ‡ | 1 | 2.454 (0.987–6.100) | 3.746 (1.743–8.049) ** | 6.798 (2.971–15.556) *** |
| Model 3 § | 1 | 2.251 (0.896–5.658) | 3.468 (1.596–7.537) ** | 6.495 (2.812–15.002) *** |
| Anemia | ||||
| Crude | 1 | 0.948 (0.505–1.780) | 1.349 (0.838–2.173) | 1.737 (1.014–2.975) * |
| Model 1 † | 1 | 0.974 (0.517–1.832) | 1.370 (0.849–2.209) | 1.787 (1.040–3.069) * |
| Model 2 ‡ | 1 | 1.074 (0.560–2.061) | 1.540 (0.920–2.576) | 1.903 (1.047–3.458) * |
| Model 3 § | 1 | 1.057 (0.538–2.076) | 1.591 (0.932–2.714) | 1.912 (1.025–3.566) * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Q.; Yuan, T.; Yang, L.; Zou, J.; Ji, M.; Zhang, Y.; Deng, J.; Lin, Q. Household Food Insecurity, Dietary Diversity, Stunting, and Anaemia among Left-Behind Children in Poor Rural Areas of China. Int. J. Environ. Res. Public Health 2019, 16, 4778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234778
Yang Q, Yuan T, Yang L, Zou J, Ji M, Zhang Y, Deng J, Lin Q. Household Food Insecurity, Dietary Diversity, Stunting, and Anaemia among Left-Behind Children in Poor Rural Areas of China. International Journal of Environmental Research and Public Health. 2019; 16(23):4778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234778
Chicago/Turabian StyleYang, Qiping, Tong Yuan, Lina Yang, Jiaojiao Zou, Meimei Ji, Yefu Zhang, Jing Deng, and Qian Lin. 2019. "Household Food Insecurity, Dietary Diversity, Stunting, and Anaemia among Left-Behind Children in Poor Rural Areas of China" International Journal of Environmental Research and Public Health 16, no. 23: 4778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234778