How to Manage Diversity and Enhance Team Performance: Evidence from Online Doctor Teams in China


Abstract
:1. Introduction
2. Literature Review
2.1. Doctor Teams and Medical Collaboration
2.2. Diversity and Team Performance
2.3. Research Gap
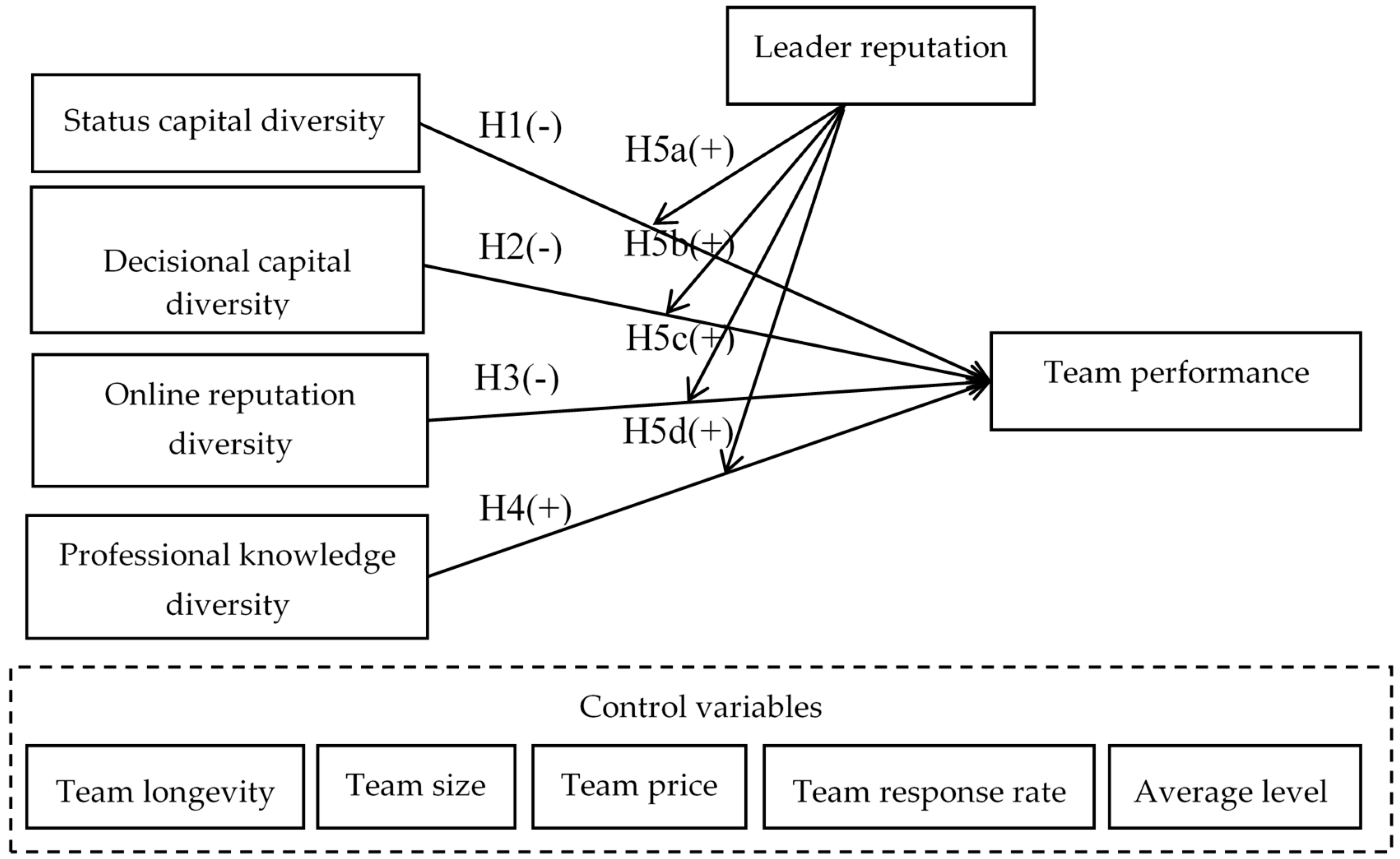
3. Development of Hypotheses
3.1. Diversity and Team Performance: The Social Categorization View
3.2. Diversity and Team Performance: The Information Processing View
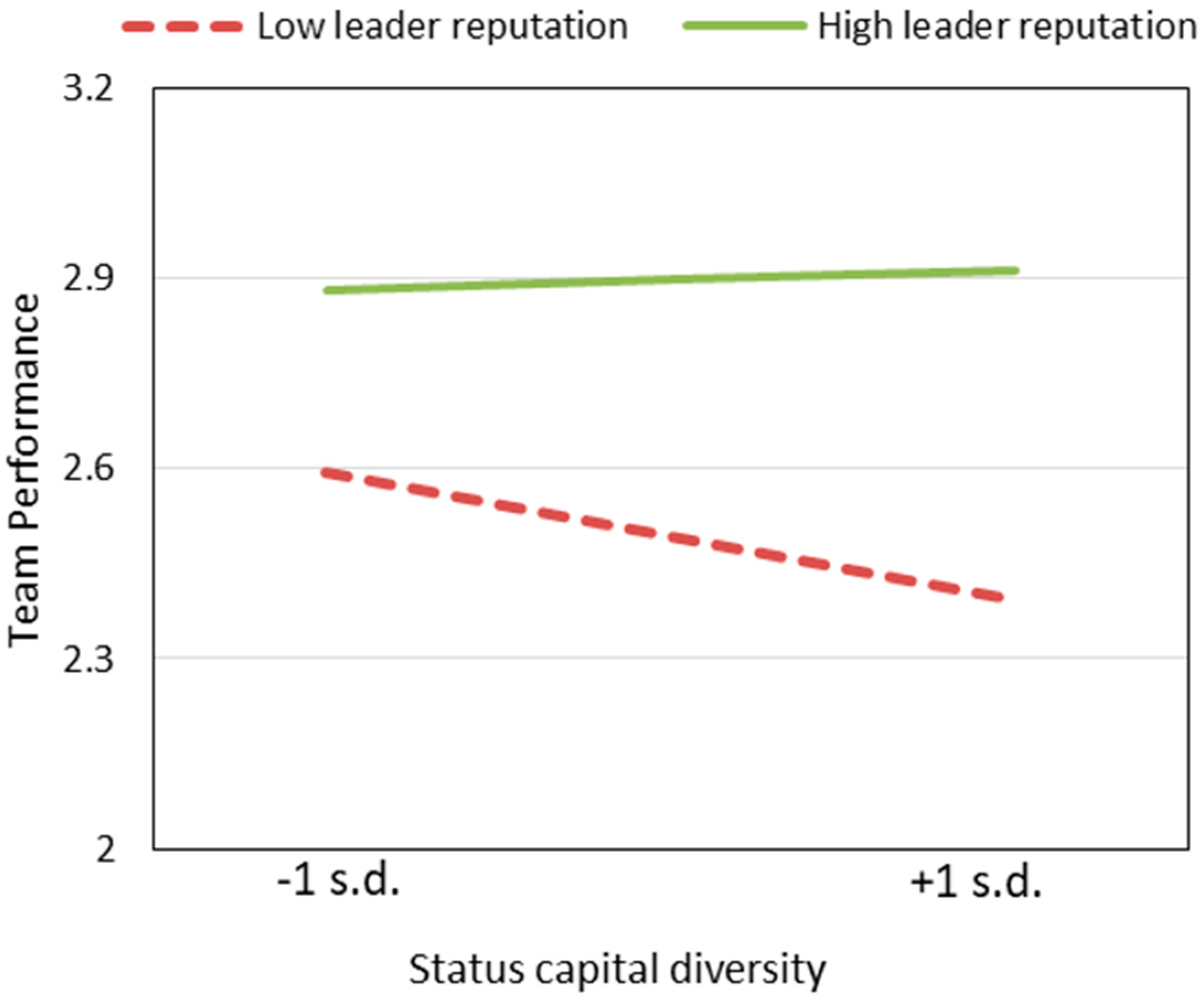
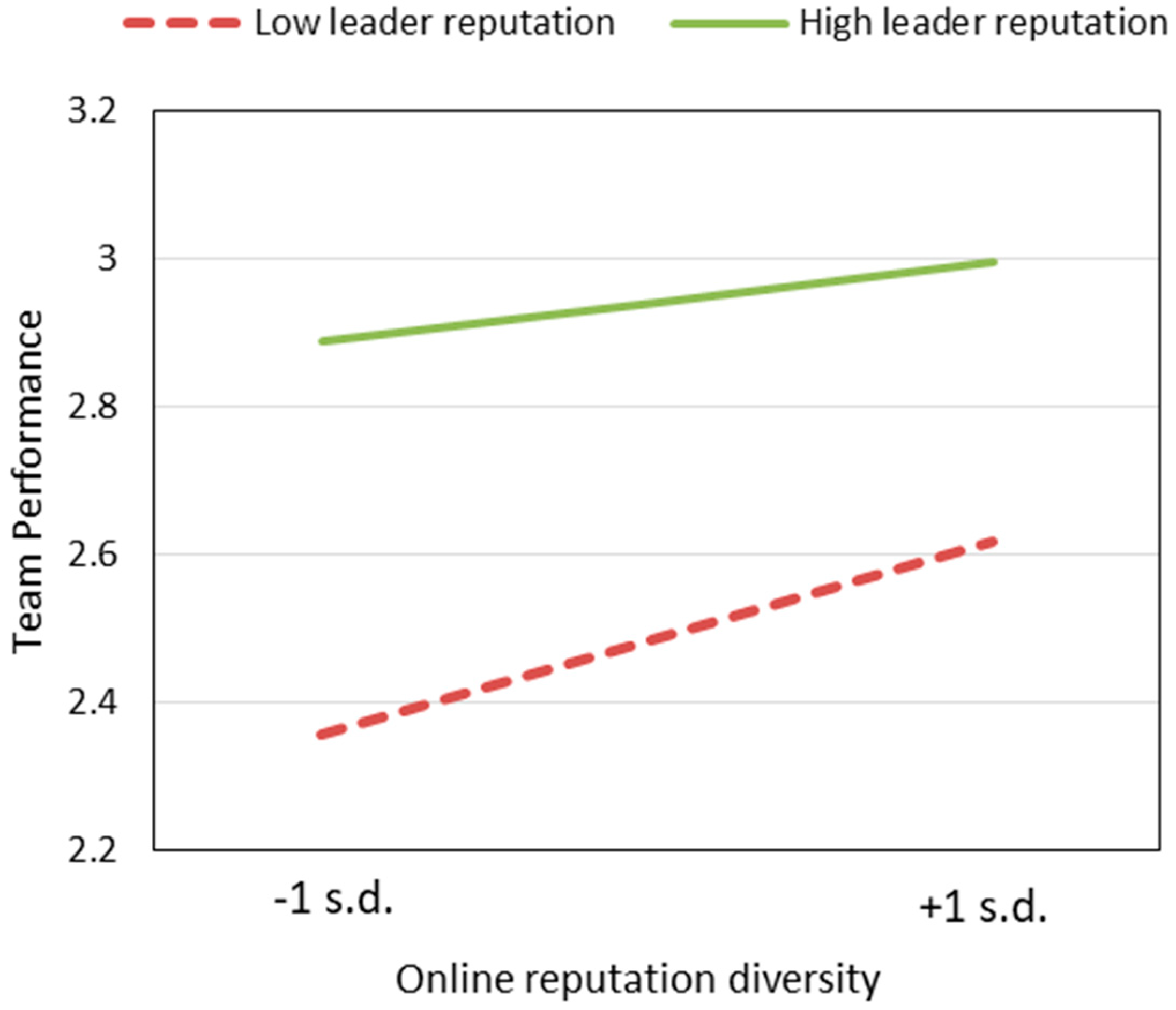
3.3. Leader Reputation as a Moderator
4. Methodology
4.1. Sample and Data Collection
4.2. Measures
4.2.1. Dependent Variable
4.2.2. Independent Variables
4.2.3. Control Variables
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yan, Z.; Wang, T.; Chen, Y.; Zhang, H. Knowledge sharing in online health communities: A social exchange theory perspective. Inform. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Casalino, L.P.; Devers, K.J.; Lake, T.K.; Marie, R.; Stoddard, J.J. Benefits of and barriers to large medical group practice in the United States. Arch. Intern. Med. 2003, 163, 1958–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solberg, L.I.; Hroscikoski, M.C.; Sperl-Hillen, J.M.; Harper, P.G.; Crabtree, B.F. Transforming medical care: case study of an exemplary, small medical group. Ann. Fam. Med. 2006, 4, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Van Knippenberg, D.; Schippers, M.C. Work group diversity. Annu. Rev. Psychol. 2007, 58, 515–541. [Google Scholar] [CrossRef] [Green Version]
- Guillaume, Y.R.F.; Dawson, J.F.; Otaye-Ebede, L.; Woods, S.A.; West, M.A. Harnessing demographic differences in organizations: What moderates the effects of workplace diversity? J. Organ. Behav. Manag. 2015, 38, 276–303. [Google Scholar] [CrossRef]
- Boughzala, I. Ingénierie de la collaboration: théories, technologies et pratiques; Hermès Science Publications: Paris, France, 2007; pp. 1–10. [Google Scholar]
- Song, H.G.; Restivo, M.; Rijt, A.V.D.; Scarlatos, L.; Tonjes, D.; Orlov, A. The hidden gender effect in online collaboration: An experimental study of team performance under anonymity. Comput. Hum. Behav. 2015, 50, 274–282. [Google Scholar] [CrossRef]
- Constant, D.; Sproull, L.; Kiesler, S. The Kindness of strangers: The usefulness of electronic weak ties for technical advice. Organ. Sci. 1996, 7, 119–135. [Google Scholar] [CrossRef]
- Wu, J.; Wu, Z.; Si, S. The influences of Internet-based collaboration and intimate interactions in buyer–supplier relationship on product innovation. Int. J. Bus. Res. 2016, 69, 3780–3787. [Google Scholar] [CrossRef]
- Chu, S.K.W.; Kennedy, D.M. Using online collaborative tools for groups to co-construct knowledge. Online. Inform. Rev. 2011, 35, 581–597. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, K.; Bannon, L. Taking CSCW seriously. CSCW. 1992, 1, 7–40. [Google Scholar] [CrossRef]
- Pratt, W.; Reddy, M.C.; Mcdonald, D.W.; Tarczy-Hornoch, P.; Gennari, J.H. Incorporating ideas from computer-supported cooperative work. J. Biomed. Inform. 2004, 37, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Stephens, M.R.; Lewis Wgbrewster, A.E.; Lord, I.; Blackshaw, G.R.; Hodzovic, I.; Thomas, G.V.; Roberts, S.A.; Crosby, T.D.; Gent, C.; Allison, M.C. Multidisciplinary team management is associated with improved outcomes after surgery for esophageal cancer. Dis. Esophagus. 2010, 19, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Wolf, F.A.; Way, L.W.; Stewart, L. The efficacy of medical team training: Improved team performance and decreased operating room delays: A detailed analysis of 4863 cases. Ann. Surg. 2010, 252, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.L.; Jackson, J.E.; Hickey, B.E.; Szallasi, F.G.; Bond, C.A. Multidisciplinary clinic care improves adherence to best practice in head and neck cancer. Am. J. Otolaryngol. Head Neck Surg. 2013, 34, 57–60. [Google Scholar] [CrossRef]
- Korman, H.; Lanni, T.J.; Shah, C.; Parslow, J.; Tull, J.; Ghilezan, M.; Krauss, D.; Balaraman, S.; Kernen, K.; Cotant, M.; et al. Impact of a prostate multidisciplinary clinic program on patient treatment decisions and on adherence to NCCN guidelines: the William Beaumont Hospital experience. Am. J. Clin. Oncol. 2013, 36, 121–125. [Google Scholar] [CrossRef]
- Phyllis, B.; Harrison, J.D.; Choy, E.T.; Young, J.M.; Andrew, S.; Alison, E. Health professional and consumer views on involving breast cancer patients in the multidisciplinary discussion of their disease and treatment plan. Cancer 2007, 110, 1937–1944. [Google Scholar] [CrossRef]
- Merién, A.E.R.; Van De Ven, J.; Mol, B.W.; Houterman, S.; Oei, S.G. Multidisciplinary team training in a simulation setting for acute obstetric emergencies: a systematic review. Obstet. Gynecol. 2010, 115, 1021–1031. [Google Scholar] [CrossRef]
- Mechanic, R.E.; Santos, P.; Landon, B.E.; Chernew, M.E. Medical group responses to global payment: early lessons from the ‘Alternative Quality Contract’ in Massachusetts. Health. Affair. 2011, 30, 1734–1742. [Google Scholar] [CrossRef]
- Nahapiet, J.; Ghoshal, S. Social Capital, Intellectual Capital, and the Organizational Advantage. Acad Manag. Rev. 1998, 23, 242–266. [Google Scholar] [CrossRef]
- Billinghurst, B.; Whitfield, M. Why do patients change their general practitioner? A postal questionnaire study of patients in Avon. Br. J. Gen. Pract. 1993, 43, 336–338. [Google Scholar] [CrossRef]
- Hoerger, T.J.; Howard, L.Z. Search behavior and choice of physician in the market for prenatal care. Med. Care 1995, 33, 332–349. [Google Scholar] [CrossRef] [PubMed]
- Hagen, P.V.; Spaander, M.; Gaast, A.; Rij, C.; Tilanus, H.; Lanschot, J.; Wijnhoven, B. Impact of a multidisciplinary tumour board meeting for upper-GI malignancies on clinical decision making: a prospective cohort study. Int. J. Clin. Oncol. 2013, 18, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Ritholz, M.D.; Beverly, E.A.; Abrahamson, M.J.; Brooks, K.M.; Hultgren, B.A.; Weinger, K. Physicians’ perceptions of the type 2 diabetes multi-disciplinary treatment team: a qualitative study. Diabetes. Educator. 2011, 37, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Macht, G.A.; Nembhard, D.A. Measures and models of personality and their effects on communication and team performance. Int. J. Ind. Ergonom. 2015, 49, 78–89. [Google Scholar] [CrossRef]
- Bell, S.T.; Villado, A.J.; Lukasik, M.A.; Belau, L.; Briggs, A.L. Getting Specific about Demographic Diversity Variable and Team Performance Relationships: A Meta-Analysis. J. Manag. 2011, 37, 709–743. [Google Scholar] [CrossRef]
- Van Knippenberg, D.; Mell, J.N. Past, present, and potential future of team diversity research: From compositional diversity to emergent diversity. Organ. Behav. Hum. Decis. Process. 2016, 136, 135–145. [Google Scholar] [CrossRef]
- Schaubroeck, J.; Lam, S.S.K.; Peng, A.C. Cognition-based and affect-based trust as mediators of leader behavior influences on team performance. J. Appl. Psychol. 2011, 96, 863–871. [Google Scholar] [CrossRef]
- Sarin, S.; Mcdermott, C. The Effect of Team Leader Characteristics on Learning, Knowledge Application, and Performance of Cross-Functional New Product Development Teams. Decis. Sci. J. 2010, 34, 707–739. [Google Scholar] [CrossRef]
- Harrison, D.A.; Klein, K.J. What’s the difference? Diversity constructs as separation, variety, or disparity in organizations. Acad. Manag. Rev. 2007, 32, 1199–1228. [Google Scholar] [CrossRef] [Green Version]
- Ren, R.; Bei, Y. Crowd Diversity and Performance in Wikipedia: The Mediating Effects of Task Conflict and Communication. In Proceedings of the Chi Conference on Human Factors in Computing Systems, New York, NY, USA, 6–11 May 2017. [Google Scholar]
- Williams, K.Y.; O’reilly, C.A. Demography and diversity in organizations: A review of 40 years of research. Res. Organ. Behav. 1998, 20, 77–140. [Google Scholar] [CrossRef]
- Van Knippenberg, D.; De Dreu, C.K.W.; Homan, A.C. Work group diversity and group performance: An integrative model and research agenda. J. Appl. Psychol. 2004, 89, 1008–1022. [Google Scholar] [CrossRef]
- Chen, J.; Lim, W.Y.; Tan, B.C.Y.; Ling, H. The Role of Functional Diversity, Collective Team Identification, and Task Cohesion in Influencing Innovation Speed: Evidence From Software Development Teams. J. Global. Inform. Manag. 2018, 26, 163–192. [Google Scholar] [CrossRef]
- Surowiecki, J. The Wisdom of Crowds; Anchor: New York, NY, USA, 2005. [Google Scholar]
- Page, S.E. Diversity and Complexity. Nature 1988, 336, 113–114. [Google Scholar] [CrossRef]
- Paulus, P.B.; Nijstad, B.A. Group Creativity: Innovation through Collaboration; Oxford University Press: New York, NY, USA, 2003; p. 3. [Google Scholar]
- Kearney, E.; Gebert, D. Managing diversity and enhancing team outcomes: the promise of transformational leadership. J. Appl. Psychol. 2009, 94, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, H.; Van Engen, M.L.; Van Knippenberg, D. Defying conventional wisdom: A meta-analytical examination of the differences between demographic and job-related diversity relationships with performance. Organ. Behav. Hum. Decis. Process. 2012, 119, 38–53. [Google Scholar] [CrossRef]
- Kearney, E.; Gebert, D.; Voelpel, S.C. When and how diversity benefits teams: the importance of team members’ need for cognition. Acad. Manag. J. 2009, 52, 581–598. [Google Scholar] [CrossRef]
- Joshi, A.; Liao, H.; Roh, H. Bridging Domains in Workplace Demography Research: A Review and Reconceptualization. J. Manag. 2011, 37, 521–552. [Google Scholar] [CrossRef]
- Muhdi, L.; Boutellier, R. Diffusion of potential health-related e-services: An analysis of Swiss health customer perspectives. J. Manag. Market. Healthc. 2013, 3, 60–72. [Google Scholar] [CrossRef]
- Elbedweihy, A.M.; Jayawardhena, C.; Elsharnouby, M.H.; Elsharnouby, T.H. Customer relationship building: The role of brand attractiveness and consumer-brand identification. J. Bus. Res. 2016, 69, 2901–2910. [Google Scholar] [CrossRef]
- Yang, Y.F.; Zhang, X.F.; Lee, P.K.C. Improving the effectiveness of online healthcare platforms: An empirical study with multi-period patient-doctor consultation data. Int. J. Prod. Econ. 2019, 207, 70–80. [Google Scholar] [CrossRef]
- Nolan, A.; Molla, T. Teacher confidence and professional capital. Teach. Teach. Educ. 2017, 62, 10–18. [Google Scholar] [CrossRef]
- Guo, S.; Guo, X.; Zhang, X.; Vogel, D. Doctor–patient relationship strength’s impact in an online healthcare community. Inform. Tech. Dev. 2018, 24, 279–300. [Google Scholar] [CrossRef]
- Guo, S.; Guo, X.; Fang, Y.; Vogel, D. How Doctors Gain Social and Economic Returns in Online Health-Care Communities: A Professional Capital Perspective. J. Manag. Inform. Syst. 2017, 34, 487–519. [Google Scholar] [CrossRef]
- Cropanzano, R. Social Exchange Theory: An Interdisciplinary Review. J. Manag. 2005, 31, 874–900. [Google Scholar] [CrossRef] [Green Version]
- Hargreaves, A. The place for professional capital and community. J. Prof. Capital. Commun. 2016, 1, 1–5. [Google Scholar] [CrossRef]
- Dai, L.; Guo, Q.; Liu, X.L.; Liu, J.G.; Zhang, Y.C. Identifying online user reputation in terms of user preference. Physica A 2018, 494, 403–409. [Google Scholar] [CrossRef]
- Manaman, H.S.; Jamali, S.; Aleahmad, A. Online reputation measurement of companies based on user-generated content in online social networks. Comput. Hum. Behav. 2016, 54, 94–100. [Google Scholar] [CrossRef]
- Fu, X.; Yue, K.; Li, L.; Liu, L. Aggregating Ordinal User Preferences for Effective Reputation Computation of Online Services. In Proceedings of the IEEE International Conference on Web Services, San Francisco, CA, USA, 27 June–2 July 2016. [Google Scholar]
- Ancona, D.G.; Caldwell, D.F. Demography and design: Predictors of new product team performance. Organ. Sci. 1992, 3, 321–341. [Google Scholar] [CrossRef] [Green Version]
- Yi, Y.Q.; Ndofor, H.A.; He, X.M.; Wei, Z.L. Top Management Team Tenure Diversity and Performance: The Moderating Role of Behavioral Integration. IEEE. Trans. Eng. Manag. 2018, 65, 21–33. [Google Scholar] [CrossRef]
- Postmes, T.; Spears, R.; Cihangir, S. Quality of decision making and group norms. J. Pers. Soc. Psychol. 2001, 80, 918–930. [Google Scholar] [CrossRef]
- Jackson, S.E.; Joshi, A. Diversity in social context: A multi-attribute, multilevel analysis of team diversity and sales performance. J. Organ. Behav. 2004, 25, 675–702. [Google Scholar] [CrossRef]
- Blondiau, A. Challenges for inter-departmental cooperation in hospitals: Results from cross-case analysis. Health. Policy. Techn. 2015, 4, 4–13. [Google Scholar] [CrossRef]
- Mcbeth, C.L.; Durbinjohnson, B.; Siegel, E.O. Interprofessional huddle: One children’s hospital’s approach to improving patient flow. Pediatr. Nurs. 2017, 43, 71–76. [Google Scholar] [PubMed]
- Konradt, U.; Schippers, M.C.; Garbers, Y.; Steenfatt, C. Effects of guided reflexivity and team feedback on team performance improvement: The role of team regulatory processes and cognitive emergent states. Eur. J. Work. Organ. Psychol. 2015, 24, 777–795. [Google Scholar] [CrossRef]
- Mcleod, P.L. Distributed People and Distributed Information: Vigilant Decision-Making in Virtual Teams. Small Group Res. 2013, 44, 627–657. [Google Scholar] [CrossRef]
- Hogan, R.; Kaiser, R.B. What we know about leadership. Rev. Gen. Psychol. 2005, 9, 169–180. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.C.; Vredenburgh, D.; Rogoff, E.G. Informational diversity and entrepreneurial team performance: Moderating effect of shared leadership. Int. Enterpren. Manag. J. 2015, 11, 39–55. [Google Scholar] [CrossRef]
- Choudhury, P.; Haas, M.R. Scope versus Speed: Team Diversity, Leader Experience, and Patenting Outcomes for Firms. Strat. Manag. J. 2018, 39, 977–1002. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.Y.; Zheng, Y.T.; Xu, W.; Liu, M.H.; Wang, J.Y. Secondhand seller reputation in online markets: A text analytics framework. Decis. Support. Syst. 2018, 108, 96–106. [Google Scholar] [CrossRef]
- Pelled, L.H.; Xin, K.R.; Weiss, A.M. No es como mí: Relational demography and conflict in a Mexican production facility. J. Occup. Organ. Psychol. 2001, 74, 63–84. [Google Scholar] [CrossRef]
- Besedeš, T.; Deck, C.; Quintanar, S.; Sarangi, S.; Shor, M. Effort and Performance: What Distinguishes Interacting and Non-Interacting Groups from Individuals? South. Econ. J. 2014, 81, 294–322. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, P.a.M.; Benders, J.; Vissers, G. Do Loafers Shirk? The Relation between Team Performance and Individual Effort. SSRN. Electron. J. 2000. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable Type | Variable Name | Original Data | Description |
|---|---|---|---|
| Dependent Variable | Team performance | The number of team consultations | Number of team’s helping patients |
| Control Variables | Team longevity | Team establishment time | The date teams were established |
| Team price | Team prices | Price of team consultation | |
| Team response rate | Team response rates | Probability of team reply within 24 h | |
| Team size | Team size | Number of team’s doctors | |
| Team average level | Members’ average number of consultations | Average individual performance of team members | |
| Independent Variables | Status capital diversity | Hospital | Doctor’s hospital |
| City | Doctor’s city | ||
| Title | Doctor’s title | ||
| Professional knowledge diversity | Department | Doctor’s department | |
| Online reputation diversity | The number of letters of thanks | Letters of thanks gave to doctor from the patients | |
| The number of virtual gifts | Virtual gifts gave to doctor from the patients | ||
| Decisional capital diversity | Medical articles | Articles written by doctors in website | |
| Doctor’s online frequency | Doctor’s online time | ||
| The number of consultations | Number of doctor’s helping patients | ||
| Moderation | Leader reputation | Leader’s gifts and letters | Letters of thanks and virtual gifts given to the leader from the patients |
| Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Team performance | 2.634 | 1.433 | ||||||||||
| 2. Team longevity | 7.63 | 3.357 | 0.366 ** | |||||||||
| 3. Team size | 3.5 | 1.492 | 0.222 ** | 0.184 ** | ||||||||
| 4. Team price (Ln) | 3.831 | 1.015 | 0.270 * | 0.117 ** | 0.136 ** | |||||||
| 5. Team response rate | 0.875 | 0.214 | 0.069 ** | 0.019 | 0 | 0.075 ** | ||||||
| 6. Team average level (Ln) | 5.953 | 1.656 | 0.429 ** | 0.230 ** | 0.039 | 0.273 ** | 0.169 ** | |||||
| 7. Leader reputation | 0.049 | 0.09 | 0.393 ** | 0.107 ** | 0.144 ** | 0.386* * | 0.136 ** | 0.504 ** | ||||
| 8. Status capital diversity | 0.13 | 0.081 | −0.056 * | −0.001 | 0.032 | 0.042 | −0.003 | −0.054 * | −0.006 | |||
| 9. Decisional capital diversity | 0.563 | 0.478 | −0.268 ** | 0.050 * | 0.172 ** | −0.134 ** | −0.063 * | −0.351 ** | −0.200 ** | 0.098 ** | ||
| 10. Online reputation diversity | 1.066 | 0.446 | 0.98 ** | −0.024 | 0.516 ** | 0.097 ** | 0.037 | −0.015 | 0.219 ** | 0.138 ** | 0.342 ** | |
| 11. Professional knowledge diversity | 0.19 | 0.261 | 0.168 ** | 0.055 * | 0.099 ** | 0.172 ** | 0.071 ** | 0.223 ** | 0.196 ** | 0.111 ** | −0.036 | 0.106 ** |
| Variable | Step 1 | Step 2 | Step 3 | Step 4 | Step 5 | Step 6 | Step 7 |
|---|---|---|---|---|---|---|---|
| Constant | −0.222 | 0.392 | 0.468 * | 0.44 * | 0.348 | 0.393 | 0.5 * |
| (−1.109) | (1.83) | (2.159) | (2.016) | (1.612) | (1.833) | (2.259) | |
| Control | |||||||
| Team longevity | 0.11 *** | 0.125 *** | 0.125 *** | 0.125 *** | 0.125 *** | 0.125 *** | 0.125 *** |
| (11.856) | (13.506) | (13.548) | (13.521) | (13.509) | (13.49) | (13.578) | |
| Team size | 0.125 *** | 0.124 *** | 0.123 *** | 0.124 *** | 0.129 *** | 0.124 *** | 0.133 *** |
| (6.037) | (5.235) | (5.231) | (5.243) | (5.403) | (5.236) | (5.596) | |
| Team price (Ln) | 0.051 | 0.019 | 0.018 | 0.017 | 0.018 | 0.019 | 0.011 |
| (1.512) | (0.591) | (0.542) | (0.514) | (0.562) | (0.583) | (0.323) | |
| Team response rate | −0.056 | −0.078 | −0.078 | −0.077 | −0.075 | −0.078 | −0.071 |
| (−0.395) | (−0.567) | (−0.569) | (−0.562) | (−0.541) | (−0.567) | (−0.519) | |
| Team average level (Ln) | 0.213 *** | 0.146 *** | 0.146 *** | 0.144 *** | 0.141 *** | 0.146 *** | 0.13 *** |
| (9.589) | (6.447) | (6.456) | (6.305) | (6.112) | (6.359) | (5.548) | |
| Leader reputation | 3.324 *** | 2.883 *** | 1.577 * | 2.469 *** | 4.619 *** | 2.951 *** | 3.801 ** |
| (8.242) | (7.126) | (2.182) | (4.536) | (3.918) | (5.005) | (3.099) | |
| Main effects | |||||||
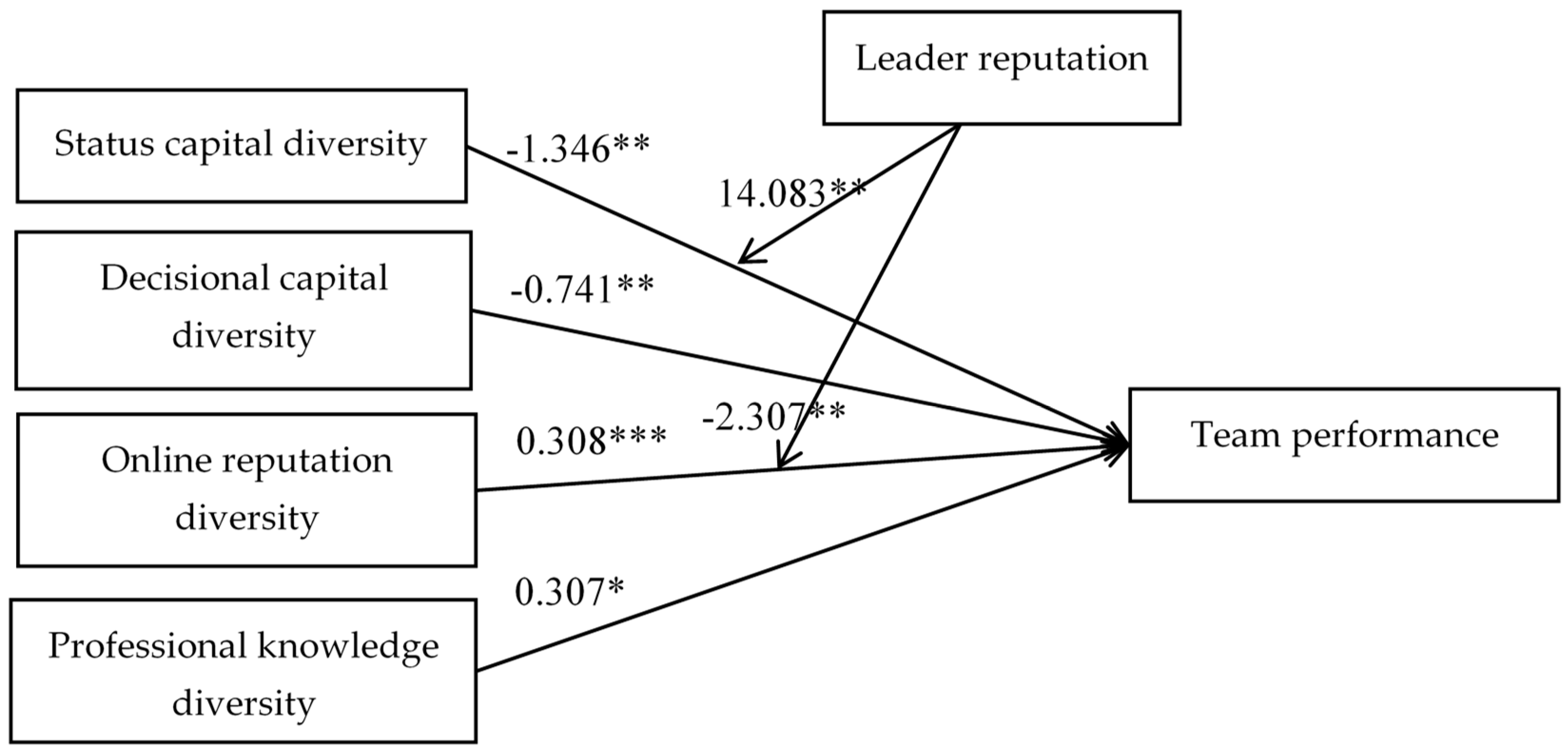
| Status capital diversity | −0.776 * | −1.23 ** | −0.786 * | −0.742 * | −0.774 * | −1.346 ** | |
| (−2.125) | (−2.929) | (−2.151) | (−2.027) | (−2.116) | (−3.189) | ||
| Decisional capital diversity | −0.679 *** | −0.677 *** | −0.715 *** | −0.683 *** | −0.679 *** | −0.741 *** | |
| (−9.459) | (−9.443) | (−9.114) | (−9.513) | (−9.438) | (−9.348) | ||
| Online reputation diversity | 0.249 ** | 0.239 ** | 0.243 ** | 0.295 ** | 0.248 ** | 0.308 *** | |
| (2.904) | (2.795) | (2.83) | (3.257) | (2.892) | (3.389) | ||
| Professional knowledge diversity | 0.292 * | 0.273 * | 0.285 * | 0.301 ** | 0.303 * | 0.307 * | |
| (2.509) | (2.341) | (2.445) | (2.587) | (2.239) | (2.274) | ||
| Interactions | |||||||
| Leader reputation * Status capital diversity | 10.22 * | 14.083 ** | |||||
| (2.182) | (2.832) | ||||||
| Leader reputation * Decisional capital diversity | 1.233 | 2.009 | |||||
| (1.137) | (1.774) | ||||||
| Leader reputation * Online reputation diversity | −1.264 * | −2.307 ** | |||||
| (−2.016) | (−2.62) | ||||||
| Leader reputation * Professional knowledge diversity | −0.18 | −0.6 | |||||
| (−0.158) | (−0.508) | ||||||
| R2 | 0.32 | 0.361 | 0.363 | 0.362 | 0.362 | 0.361 | 0.367 |
| F | 122.452 *** | 87.976 *** | 80.604 *** | 80.111 *** | 80.277 *** | 79.930 *** | 64.165 *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Chen, M.; Li, J.; Ma, L. How to Manage Diversity and Enhance Team Performance: Evidence from Online Doctor Teams in China. Int. J. Environ. Res. Public Health 2020, 17, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010048
Liu X, Chen M, Li J, Ma L. How to Manage Diversity and Enhance Team Performance: Evidence from Online Doctor Teams in China. International Journal of Environmental Research and Public Health. 2020; 17(1):48. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010048
Chicago/Turabian StyleLiu, Xuan, Meimei Chen, Jia Li, and Ling Ma. 2020. "How to Manage Diversity and Enhance Team Performance: Evidence from Online Doctor Teams in China" International Journal of Environmental Research and Public Health 17, no. 1: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010048