Meeting the Global NCD Target of at Least 10% Relative Reduction in the Harmful Use of Alcohol: Is the WHO European Region on Track?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
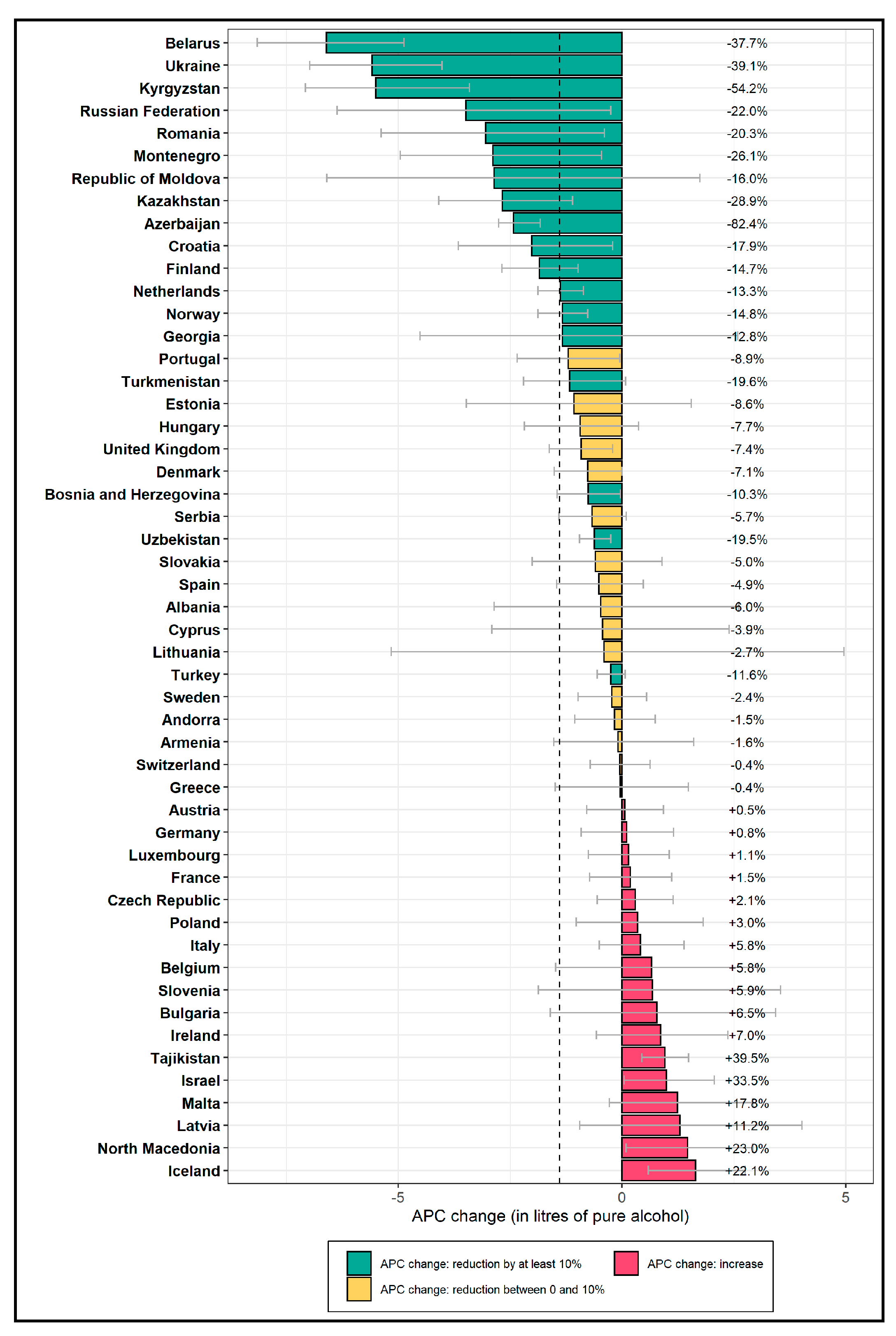
3.1. Total Alcohol Per Capita Consumption
3.2. Heavy Episodic Drinking
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Radovac, I.; Loyola, E.; Breda, J.; Farrington, J.; Gaela, G. Monitoring Noncommunicable Disease Commitments in Europe Theme in Focus: Progress Monitor Indicators. Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/351518/Monitoring-NCD.pdf?ua=1 (accessed on 1 November 2018).
- Rehm, J.; Gmel, G.E.; Gmel, G.; Hasan, O.S.M.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.V.; et al. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [Green Version]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef] [PubMed]
- Shield, K.D.; Soerjomataram, I.; Rehm, J. Alcohol Use and Breast Cancer: A Critical Review. Alcohol Clin. Exp. Res. 2016, 40, 1166–1181. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Rehm, J. The cardioprotective association of average alcohol consumption and ischaemic heart disease: A systematic review and meta-analysis. Addiction 2012, 107, 1246–1260. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Rehm, J. Chronic heavy drinking and ischaemic heart disease: A systematic review and meta-analysis. Open Heart 2014, 1, e000135. [Google Scholar] [CrossRef] [Green Version]
- Rehm, J.; Roerecke, M. Cardiovascular effects of alcohol consumption. Trends Cardiovasc. Med. 2017, 27, 534–538. [Google Scholar] [CrossRef]
- World Health Organization. Status Report on Alcohol Consumption, Harm and Policy Responses in 30 European Countries 2019; WHO European Office for the Prevention and Control of Noncommunicable Diseases: Moscow, Russia, 2019. [Google Scholar]
- United Nations Transforming Our World: The 2030 Agenda for Sustainable Development. Available online: https://sustainabledevelopment.un.org/ (accessed on 10 October 2018).
- World Health Organization Thirteenth General Programme of Work 2019−2023. Available online: https://www.who.int/about/what-we-do/thirteenth-general-programme-of-work-2019---2023 (accessed on 10 March 2020).
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization (WHO). NCD Global Monitoring Framework. Available online: https://www.who.int/nmh/global_monitoring_framework/en/ (accessed on 3 March 2020).
- Probst, C.; Fleischmann, A.; Gmel, G.; Poznyak, V.; Rekve, D.; Riley, L.; Rylett, M.A.; Shield, K.; Rehm, J. The Global Proportion and Volume of Unrecorded Alcohol in 2015. J. Glob. Health 2019, 9, 010421. [Google Scholar] [CrossRef]
- Probst, C.; Manthey, J.; Merey, A.; Rylett, M.; Rehm, J. Unrecorded alcohol use: A global modelling study based on nominal group assessments and survey data. Addiction 2018, 113, 1231–1241. [Google Scholar] [CrossRef]
- Manthey, J.; Rylett, M.A.; Hasan, O.S.M.; Probst, C.; Rehm, J. Alcohol exposure between 1990 and 2017 and forecasts until 2030: A global modelling study. Lancet 2019, 393, 2493–2502. [Google Scholar] [CrossRef]
- World Health Organization Global Information System on Alcohol and Health. Available online: http://apps.who.int/gho/data/node.main.GISAH (accessed on 3 February 2020).
- Shield, K.; Rylett, M.; Rehm, J. Public Health Successes and Missed Opportunities—Trends in Alcohol Consumption and Attributable Mortality in the WHO European Region, 1990–2014; World Health Organization: Copenhagen, Denmark, 2016; pp. 1–63. [Google Scholar]
- Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat World Population Prospects: The 2017 Revision, Key Findings and Advance Tables, July 2017 ed. Available online: http://esa.un.org/unpd/wpp/index.htm (accessed on 01 March 2020).
- Ahmad, O.B.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J.; Lozano, R.; Inoue, M. Age Standardization of Rates: A New WHO Standard; World Health Organization: Geneva, Switzerland, 2001; pp. 1–14. [Google Scholar]
- Babor, T.F. Public health science and the global strategy on alcohol. Bull. World Health 2010, 88, 643. [Google Scholar] [CrossRef]
- Chisholm, D.; Moro, D.; Bertram, M.; Pretorius, C.; Gmel, G.; Shield, K.; Rehm, J. Are the “Best Buys” for alcohol control still valid? An update on the comparative cost-effectiveness of alcohol control strategies at the global level. J. Stud. Alcohol Drugs 2018, 79, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.; Caetano, R.; Casswell, S.; Edwards, G.; Giesbrecht, N.; Graham, K.; Grube, J.; Hill, L.; Holder, H.; Homel, R.; et al. Alcohol: No Ordinary Commodity: Research and Public Policy, 2nd ed.; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- World Health Organization. WHO Launches SAFER, a New Alcohol Control Initiative. Available online: https://www.who.int/substance_abuse/safer/en/ (accessed on 15 April 2020).
- World Health Organization. ‘Best Buys’ and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases. Available online: https://www.who.int/ncds/management/WHO_Appendix_BestBuys_LS.pdf (accessed on 02 March 2020).
- Neufeld, M.; Rehm, J. Alcohol consumption and mortality in Russia since 2000: are there any changes following the alcohol policy changes starting in 2006? Alcohol Alcohol. 2013, 48, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Khaltourina, D.; Korotayev, A. Effects of Specific Alcohol Control Policy Measures on Alcohol-Related Mortality in Russia from 1998 to 2013. Alcohol Alcohol. 2015, 50, 588–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Alcohol Policy Impact Case Study. The Effects of Alcohol Control Measures on Mortality and Life Expectancy in the Russian Federation; WHO Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Neufeld, M.; Ferreira-Borges, C.; Gil, A.; Manthey, J.; Rehm, J. Alcohol policy has saved lives in the Russian Federation. Int. J. Drug Policy. in press.
- World Health Organization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. World Health Statistics 2017: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Orro, E.; Martens, K.; Lepane, L.; Josing, M.; Reinam, M. Alcohol Market, Consumption and Harms in Estonia; Health Development Institute: Tallin, Estonia, 2017. [Google Scholar]
- Stoppel, R. Alcohol availability and alcohol-attributable mortality: Evidence from administrative data. In Annual Conference 2019: 30 Years after the Fall of the Berlin Wall - Democracy and Market Economy; Verein für Socialpolitik/German Economic Association: Leipzig, Germany, 2019. [Google Scholar]
- Grigoriev, P.; Bobrova, A. Alcohol control policies and mortality trends in Belarus. Drug Alcohol Rev. 2020. early view. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Manthey, J.; Lange, S.; Badaras, R.; Zurlyte, I.; Passmore, J.; Breda, J.; Ferreira-Borges, C.; Štelemėkas, M. Alcohol control policy and changes in alcohol-related traffic harm. Addiction 2020, 115, 655–665. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Action Plan on Youth Drinking and on Heavy Episodic Drinking (Binge Drinking) (2014–2016). Progress Evaluation Report; WHO Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Angus, C.; Holmes, J.; Meier, P.S. Comparing alcohol taxation throughout the European Union. Addiction 2019, 114, 1489–1494. [Google Scholar] [CrossRef] [Green Version]
- Directorate-General for Agriculture and Rural Development Wine CMO–Overview 2009-23. Available online: https://ec.europa.eu/info/sites/info/files/food-farming-fisheries/farming/documents/wine-2009-2023-overview_en.pdf (accessed on 03 February 2020).
- Anderson, P.; de Bruijn, A.; Angus, K.; Gordon, R.; Hastings, G. Impact of alcohol advertising and media exposure on adolescent alcohol use: A systematic review of longitudinal studies. Alcohol Alcohol. 2009, 44, 229–243. [Google Scholar] [CrossRef] [Green Version]
- Probst, C.; Manthey, J.; Rehm, J. Understanding the prevalence of lifetime abstinence from alcohol: An ecological study. Drug Alcohol Depend 2017, 178, 126–129. [Google Scholar] [CrossRef]
- Shield, K.D.; Rehm, M.; Patra, J.; Sornpaisarn, B.; Rehm, J. Global and Country Specific Adult per capita Consumption of Alcohol. Sucht 2011, 57, 99–117. [Google Scholar] [CrossRef]
- Ettner, S.L. Measuring the human cost of a weak economy: Does unemployment lead to alcohol abuse? Soc. Sci. Med. 1997, 44, 251–260. [Google Scholar] [CrossRef]
- Dee, T.S. Alcohol abuse and economic conditions: Evidence from repeated cross-sections of individual-level data. Health Econ. 2001, 10, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Pacula, R.L. Substance use and recessions: What can be learned from economic analyses of alcohol? Int. J. Drug Policy 2011, 22, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Lai, T.; Habicht, J. Decline in Alcohol Consumption in Estonia: Combined Effects of Strengthened Alcohol Policy and Economic Downturn. Alcohol Alcohol. 2011, 46, 200–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehm, J.; Manthey, J.; Shield, K.D.; Ferreira-Borges, C. Trends in substance use and in the attributable burden of disease and mortality in the WHO European Region, 2010–2016. Eur. J.Public Health 2019, 29, 723–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, A.; Anderson, P.; Jané-Llopis, E.; Manthey, J.; Kaner, E.; Rehm, J. Immediate impact of minimum unit pricing on alcohol purchases in Scotland: controlled interrupted time series analysis for 2015-18. BMJ 2019, 366, l5274. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Country Groups | Countries |
|---|---|
| EU-28 | Austria, Belgium, Bulgaria, Croatia, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden, United Kingdom |
| Central–Eastern EU | Bulgaria, Croatia, Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia, Slovenia |
| Central–Western EU | Austria, Belgium, Denmark, Germany, Netherlands, Switzerland |
| Eastern WHO EUR | Belarus, Republic of Moldova, Russian Federation, Ukraine |
| Mediterranean | Cyprus, France, Greece, Israel, Italy, Malta, Portugal, Spain, Turkey |
| South–Eastern WHO EUR | Armenia, Azerbaijan, Georgia, Kazakhstan, Kyrgyzstan, Tajikistan, Turkey, Turkmenistan, Uzbekistan |
| Population | Drinkers | ||||||
|---|---|---|---|---|---|---|---|
| Country Group | Sex | APC 2010 (95% CI) | APC 2017 (95% CI) | % Change (95% CI) | APC 2010 (95% CI) | APC 2017 (95% CI) | % Change (95% CI) |
| WHO European Region | Female | 5.1 (5.0, 5.2) | 4.3 (4.1, 4.6) | −14.9% (−19.5, −9.6%) | 8.9 (8.7, 9.0) | 7.9 (7.5, 8.4) | −10.6% (−15.4, −5.0%) |
| Male | 17.5 (17.2, 17.8) | 15.4 (14.5, 16.3) | −12.3% (−17.1, −6.8%) | 24.0 (23.6, 24.4) | 21.7 (20.5, 23.0) | −9.9% (−14.9, −4.3%) | |
| Total | 11.2 (11.0, 11.4) | 9.8 (9.3, 10.4) | −12.4% (−17.2, −7.0%) | 17.3 (17.0, 17.6) | 15.7 (14.9, 16.7) | −9.1% (−14.1, −3.4%) | |
| Central–Eastern EU | Female | 5.9 (5.7, 6.1) | 5.6 (4.8, 6.4) | −6.1% (−19.5, 8.6%) | 8.7 (8.4, 9.0) | 8.1 (7.0, 9.4) | −6.3% (−19.7, 8.3%) |
| Male | 19.6 (19.0, 20.3) | 18.7 (16.0, 21.6) | −5.0% (−18.5, 9.9%) | 23.6 (22.8, 24.4) | 22.3 (19.2, 25.8) | −5.4% (−18.8, 9.4%) | |
| Total | 12.6 (12.2, 13.0) | 12.0 (10.3, 13.9) | −4.5% (−18.1, 10.4%) | 16.7 (16.2, 17.2) | 15.9 (13.6, 18.4) | −4.8% (−18.4, 10.0%) | |
| Central–Western EU | Female | 5.8 (5.7, 6.0) | 5.8 (5.3, 6.3) | −1.1% (−9.2, 7.4%) | 8.0 (7.8, 8.1) | 7.7 (7.1, 8.4) | −2.7% (−10.7, 5.6%) |
| Male | 19.0 (18.6, 19.4) | 18.6 (17.1, 20.2) | −1.9% (−10.0, 6.5%) | 21.8 (21.3, 22.3) | 21.2 (19.5, 23.0) | −2.7% (−10.7, 5.6%) | |
| Total | 12.3 (12.0, 12.5) | 12.2 (11.2, 13.2) | −0.8% (−9.0, 7.7%) | 15.3 (15.0, 15.7) | 15.0 (13.8, 16.3) | −2.1% (−10.1, 6.3%) | |
| Eastern WHO EUR | Female | 6.9 (6.6, 7.2) | 4.8 (3.7, 5.9) | −31.3% (−46.1, −14.5%) | 12.3 (11.8, 12.8) | 10.1 (7.9, 12.6) | −17.9% (−35.6, 2.1%) |
| Male | 25.7 (24.6, 26.9) | 19.4 (15.2, 24.1) | −24.8% (−41.1, −6.3%) | 33.9 (32.4, 35.4) | 27.9 (21.9, 34.8) | −17.6% (−35.4, 2.6%) | |
| Total | 15.6 (14.9, 16.3) | 11.5 (9.0, 14.3) | −26.2% (−42.2, −8.1%) | 23.9 (22.9, 25.0) | 20.1 (15.8, 25.1) | −15.8% (−34.0, 4.8%) | |
| EU-28 | Female | 5.4 (5.3, 5.5) | 5.2 (4.7, 5.8) | −3.5% (−13.0, 6.5%) | 7.8 (7.6, 8.0) | 7.5 (6.8, 8.3) | −3.4% (−12.9, 6.7%) |
| Male | 17.9 (17.4, 18.4) | 17.4 (15.7, 19.2) | −2.9% (−12.5, 7.1%) | 21.2 (20.6, 21.8) | 20.6 (18.5, 22.7) | −3.0% (−12.5, 7.1%) | |
| Total | 11.5 (11.2, 11.8) | 11.2 (10.1, 12.4) | −2.4% (−12.0, 7.8%) | 15.0 (14.6, 15.4) | 14.6 (13.2, 16.2) | −2.4% (−12.0, 7.8%) | |
| Mediterranean | Female | 3.6 (3.5, 3.7) | 3.5 (3.1, 3.9) | −3.9% (−13.5, 6.1%) | 7.1 (6.9, 7.3) | 7.1 (6.4, 7.8) | −0.5% (−10.5, 9.9%) |
| Male | 12.7 (12.4, 13.1) | 12.3 (11.1, 13.7) | −3.2% (−13.2, 7.2%) | 19.5 (19.0, 20.1) | 19.4 (17.4, 21.4) | −0.8% (−11.0, 9.9%) | |
| Total | 8.0 (7.8, 8.3) | 7.8 (7.0, 8.6) | −2.8% (−12.8, 7.6%) | 13.9 (13.5, 14.2) | 13.9 (12.4, 15.3) | 0.1% (−10.2, 10.8%) | |
| South–Eastern WHO EUR | Female | 1.4 (1.3, 1.5) | 1.0 (0.8, 1.3) | −27.6% (−42.9, −9.7%) | 11.0 (10.5, 11.5) | 7.8 (6.1, 9.7) | −29.1% (−44.1, −11.6%) |
| Male | 6.7 (6.4, 7.1) | 5.1 (4.0, 6.2) | −25.0% (−40.1, −7.5%) | 29.3 (27.9, 30.7) | 21.1 (16.8, 26.0) | −28.1% (−42.6, −11.2%) | |
| Total | 3.9 (3.8, 4.1) | 3.0 (2.4, 3.7) | −25.0% (−40.3, −7.2%) | 22.3 (21.2, 23.3) | 16.1 (12.8, 20.0) | −27.5% (−42.3, −10.3%) | |
| Population | Drinkers | ||||||
|---|---|---|---|---|---|---|---|
| Group | Sex | HED 2010 | HED 2017 | % Change | HED 2010 | HED 2017 | % Change |
| WHO European Region | Female | 19.6% (15.8, 23.5%) | 18.4% (15.0, 21.7%) | −6.4% (−23.7, 10.9%) | 34.2% (27.5, 41.0%) | 33.7% (27.5, 39.9%) | −1.6% (−19.8, 16.5%) |
| Male | 41.8% (38.0, 45.6%) | 39.8% (36.1, 43.4%) | −4.8% (−13.6, 4.0%) | 57.3% (52.1, 62.6%) | 56.1% (50.9, 61.3%) | −2.2% (−11.3, 6.8%) | |
| Total | 30.7% (26.9, 34.5%) | 29.1% (25.5, 32.6%) | −5.4% (−16.9, 6.1%) | 47.5% (41.6, 53.4%) | 46.7% (41.0, 52.3%) | −1.7% (−13.7, 10.2%) | |
| Central–Eastern EU | Female | 30.3% (27.5, 33.0%) | 31.7% (28.8, 34.5%) | 4.6% (−4.6, 13.9%) | 44.3% (40.2, 48.3%) | 46.2% (42.1, 50.3%) | 4.3% (−4.9, 13.6%) |
| Male | 57.7% (54.9, 60.4%) | 58.9% (56.2, 61.6%) | 2.0% (−2.6, 6.7%) | 69.3% (66.0, 72.6%) | 70.5% (67.2, 73.7%) | 1.6% (−3.0, 6.3%) | |
| Total | 44.0% (41.2, 46.7%) | 45.3% (42.5, 48.0%) | 2.9% (−3.3, 9.2%) | 58.3% (54.6, 61.9%) | 59.8% (56.1, 63.4%) | 2.6% (−3.7, 8.8%) | |
| Central–Western EU | Female | 19.8% (17.8, 21.8%) | 21.0% (18.9, 23.1%) | 6.0% (−4.7, 16.7%) | 27.0% (24.3, 29.8%) | 28.2% (25.3, 31.0%) | 4.2% (−6.3, 14.7%) |
| Male | 45.1% (42.2, 48.0%) | 46.3% (43.1, 49.4%) | 2.6% (−4.4, 9.6%) | 51.8% (48.4, 55.1%) | 52.7% (49.1, 56.3%) | 1.8% (−5.1, 8.7%) | |
| Total | 32.5% (30.0, 34.9%) | 33.6% (31.0, 36.3%) | 3.6% (−4.5, 11.7%) | 40.6% (37.5, 43.6%) | 41.5% (38.3, 44.8%) | 2.3% (−5.7, 10.3%) | |
| Eastern WHO EUR | Female | 27.9% (17.3, 38.4%) | 23.1% (14.2, 32.1%) | −17.0% (−49.2, 15.3%) | 49.5% (30.8, 68.2%) | 49.1% (30.1, 68.2%) | −0.7% (−39.3, 37.8%) |
| Male | 53.6% (44.9, 62.3%) | 46.7% (38.4, 55.0%) | −12.9% (−28.4, 2.5%) | 70.6% (59.2, 82.0%) | 67.3% (55.4, 79.3%) | −4.6% (−21.6, 12.3%) | |
| Total | 40.7% (31.1, 50.3%) | 34.9% (26.3, 43.5%) | −14.3% (−35.5, 6.9%) | 62.4% (47.7, 77.2%) | 61.0% (45.9, 76.1%) | −2.3% (−26.5, 21.9%) | |
| EU-28 | Female | 20.6% (18.5, 22.6%) | 20.8% (18.8, 22.9%) | 1.3% (−8.6, 11.3%) | 29.7% (26.8, 32.7%) | 30.2% (27.2, 33.1%) | 1.5% (−8.5, 11.4%) |
| Male | 45.7% (42.9, 48.4%) | 45.7% (42.9, 48.5%) | 0.0% (−6.0, 6.1%) | 54.1% (50.9, 57.3%) | 54.1% (50.8, 57.4%) | −0.0% (−6.1, 6.1%) | |
| Total | 33.1% (30.7, 35.5%) | 33.3% (30.9, 35.7%) | 0.4% (−6.8, 7.7%) | 43.3% (40.2, 46.4%) | 43.5% (40.3, 46.6%) | 0.5% (−6.8, 7.8%) | |
| Mediterranean | Female | 12.4% (11.1, 13.7%) | 11.8% (10.5, 13.1%) | −4.6% (−14.9, 5.7%) | 24.2% (21.7, 26.8%) | 23.9% (21.4, 26.5%) | −1.2% (−11.9, 9.4%) |
| Male | 31.0% (28.9, 33.2%) | 29.9% (27.8, 32.1%) | −3.6% (−10.6, 3.3%) | 47.5% (44.2, 50.9%) | 47.0% (43.6, 50.3%) | −1.2% (−8.3, 5.9%) | |
| Total | 21.7% (20.0, 23.4%) | 20.9% (19.2, 22.6%) | −3.8% (−11.7, 4.1%) | 37.5% (34.5, 40.5%) | 37.1% (34.1, 40.1%) | −1.0% (−9.1, 7.2%) | |
| South–Eastern WHO EUR | Female | 3.9% (3.4, 4.3%) | 3.9% (3.4, 4.3%) | −0.3% (−12.4, 11.7%) | 30.4% (26.9, 33.9%) | 29.6% (26.0, 33.2%) | −2.5% (−14.2, 9.3%) |
| Male | 11.5% (10.5, 12.5%) | 11.5% (10.4, 12.5%) | −0.5% (−9.9, 8.9%) | 50.1% (45.7, 54.6%) | 47.8% (43.3, 52.4%) | −4.6% (−13.6, 4.5%) | |
| Total | 7.7% (7.0, 8.5%) | 7.7% (6.9, 8.5%) | −0.2% (−10.2, 9.8%) | 43.6% (39.5, 47.8%) | 42.1% (37.8, 46.3%) | −3.6% (−13.3, 6.1%) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Probst, C.; Manthey, J.; Neufeld, M.; Rehm, J.; Breda, J.; Rakovac, I.; Ferreira-Borges, C. Meeting the Global NCD Target of at Least 10% Relative Reduction in the Harmful Use of Alcohol: Is the WHO European Region on Track? Int. J. Environ. Res. Public Health 2020, 17, 3423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103423
Probst C, Manthey J, Neufeld M, Rehm J, Breda J, Rakovac I, Ferreira-Borges C. Meeting the Global NCD Target of at Least 10% Relative Reduction in the Harmful Use of Alcohol: Is the WHO European Region on Track? International Journal of Environmental Research and Public Health. 2020; 17(10):3423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103423
Chicago/Turabian StyleProbst, Charlotte, Jakob Manthey, Maria Neufeld, Jürgen Rehm, João Breda, Ivo Rakovac, and Carina Ferreira-Borges. 2020. "Meeting the Global NCD Target of at Least 10% Relative Reduction in the Harmful Use of Alcohol: Is the WHO European Region on Track?" International Journal of Environmental Research and Public Health 17, no. 10: 3423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103423