Impact of Computed Tomography Scans on the Risk of Thyroid Disease in Minor Head Injury Patients: A Population-Based Retrospective Cohort Study

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Data Source
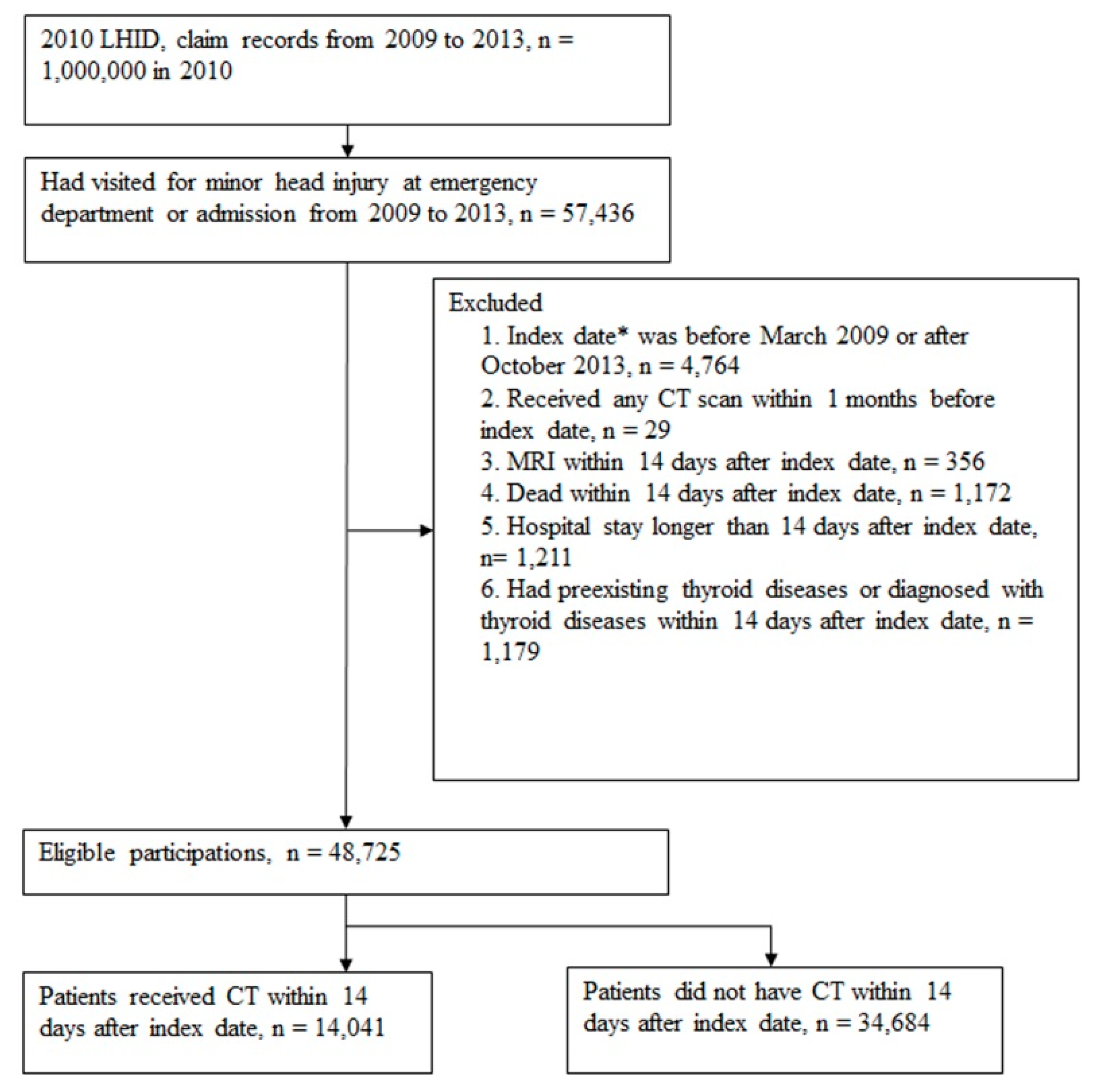
2.2. Identification of Study Patients
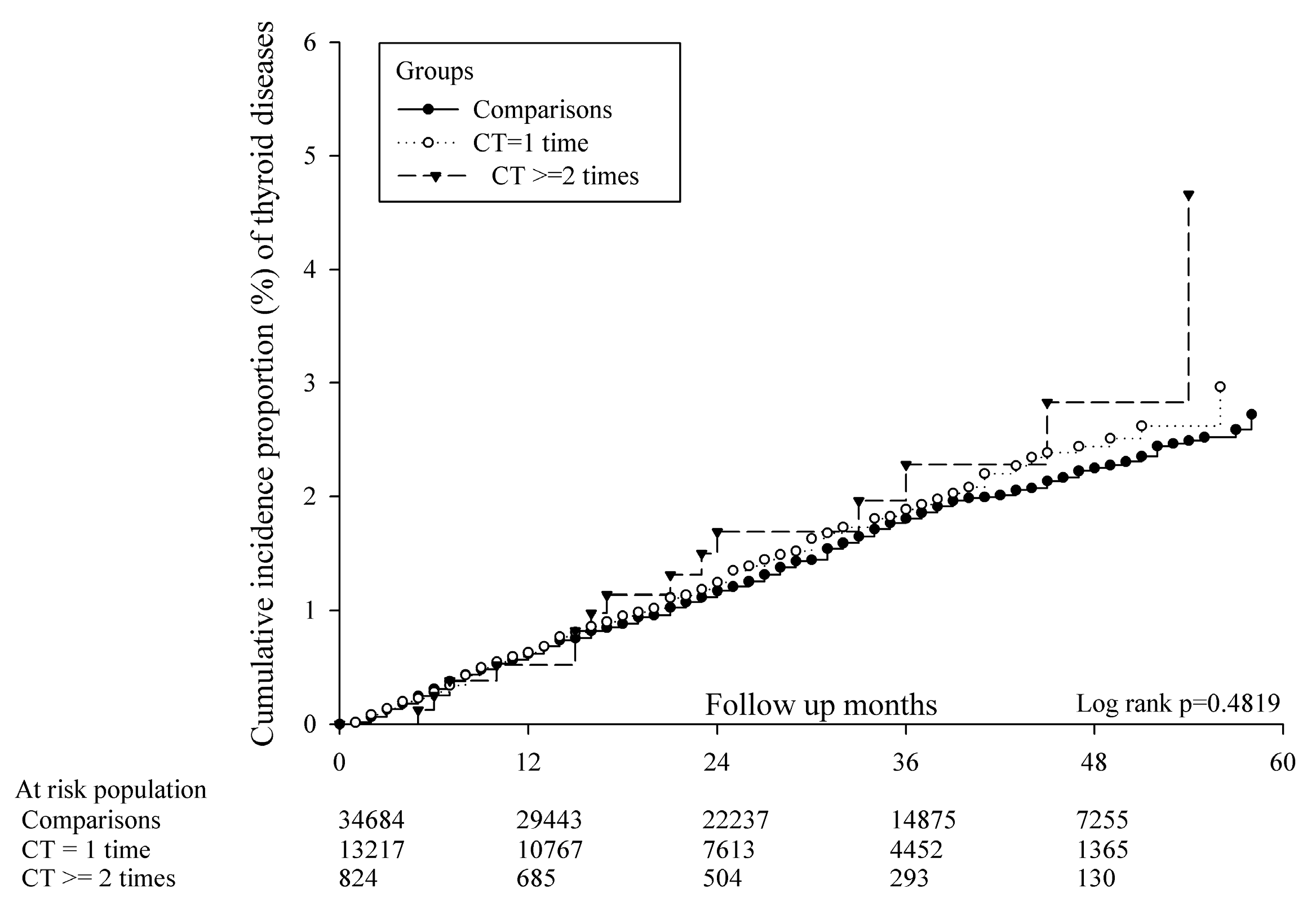
2.3. Study Events and Follow-Up
2.4. Study Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Subjects
3.2. Risk of Thyroid Diseases on Different Comorbidities and Other Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Taylor, C.A.; Bell, J.M.; Breiding, M.J.; Xu, L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths—United states, 2007 and 2013. MMWR Surveill. Summ. 2017, 66, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Hsu, I.L.; Li, C.Y.; Chu, D.C.; Chien, L.C. An epidemiological analysis of head injuries in taiwan. Int. J. Environ. Res. Public Health 2018, 15, 2457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.; Clement, C.; Lesiuk, H.; Laupacis, A.; McKnight, R.D.; Verbeek, R.; Brison, R.; Cass, D.; et al. The canadian ct head rule for patients with minor head injury. Lancet 2001, 357, 1391–1396. [Google Scholar] [PubMed]
- Haydel, M.J.; Preston, C.A.; Mills, T.J.; Luber, S.; Blaudeau, E.; DeBlieux, P.M. Indications for computed tomography in patients with minor head injury. N. Engl. J. Med. 2000, 343, 100–105. [Google Scholar] [PubMed] [Green Version]
- Mower, W.R.; Hoffman, J.R.; Herbert, M.; Wolfson, A.B.; Pollack, C.V., Jr.; Zucker, M.I. Developing a decision instrument to guide computed tomographic imaging of blunt head injury patients. J. Trauma. 2005, 59, 954–959. [Google Scholar] [CrossRef] [Green Version]
- Ron, E.; Brenner, A. Non-malignant thyroid diseases after a wide range of radiation exposures. Radiat. Res. 2010, 174, 877–888. [Google Scholar] [CrossRef] [Green Version]
- Albi, E.; Cataldi, S.; Lazzarini, A.; Codini, M.; Beccari, T.; Ambesi-Impiombato, F.S.; Curcio, F. Radiation and thyroid cancer. Int. J. Mol. Sci. 2017, 18, 911. [Google Scholar] [CrossRef]
- Nagayama, Y. Radiation-related thyroid autoimmunity and dysfunction. J. Radiat. Res. 2018, 59, ii98–ii107. [Google Scholar]
- Woolf, P.D.; Lee, L.A.; Hamill, R.W.; McDonald, J.V. Thyroid test abnormalities in traumatic brain injury: Correlation with neurologic impairment and sympathetic nervous system activation. Am. J. Med. 1988, 84, 201–208. [Google Scholar] [CrossRef]
- Yang, W.H.; Chen, P.C.; Wang, T.C.; Kuo, T.Y.; Cheng, C.Y.; Yang, Y.H. Endocrine dysfunction following traumatic brain injury: A 5-year follow-up nationwide-based study. Sci. Rep. 2016, 6, 32987. [Google Scholar] [CrossRef]
- Li, M.; Sirko, S. Traumatic brain injury: At the crossroads of neuropathology and common metabolic endocrinopathies. J. Clin. Med. 2018, 7, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitek, V.; Shatney, C.H. Thyroid hormone alterations in patients with shock and injury. Injury 1987, 18, 336–341. [Google Scholar] [CrossRef]
- Haugen, B.R. Drugs that suppress tsh or cause central hypothyroidism. Best Pract. Res. Clin. Endocrinol. Metab. 2009, 23, 793–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hifumi, T.; Okada, I.; Kiriu, N.; Hasegawa, E.; Ogasawara, T.; Kato, H.; Koido, Y.; Inoue, J.; Abe, Y.; Kawakita, K.; et al. Thyroid hormone alterations in trauma patients requiring massive transfusion: An observational study. World J. Emerg. Med. 2014, 5, 270–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrimpton, P.C.; Wall, B.F.; Hart, D. Diagnostic medical exposures in the u.K. Appl. Radiat. Isot. 1999, 50, 261–269. [Google Scholar] [CrossRef]
- McCrohan, J.L.; Patterson, J.F.; Gagne, R.M.; Goldstein, H.A. Average radiation doses in a standard head examination for 250 ct systems. Radiology 1987, 163, 263–268. [Google Scholar] [CrossRef]
- Lin, Z.; Yang, Z.; He, B.; Wang, D.; Gao, X.; Tam, S.Y.; Wu, V.W.C. Pattern of radiation-induced thyroid gland changes in nasopharyngeal carcinoma patients in 48 months after radiotherapy. PLoS ONE 2018, 13, e0200310. [Google Scholar] [CrossRef]
- Mazonakis, M.; Tzedakis, A.; Damilakis, J.; Gourtsoyiannis, N. Thyroid dose from common head and neck ct examinations in children: Is there an excess risk for thyroid cancer induction? Eur. Radiol. 2007, 17, 1352–1357. [Google Scholar] [CrossRef]
- Tipnis, S.V.; Spampinato, M.V.; Hungerford, J.; Huda, W. Thyroid doses and risks to adult patients undergoing neck ct examinations. Am. J. Roentgenol. 2015, 204, 1064–1068. [Google Scholar] [CrossRef]
- Gul, N.; Uzum, A.K.; Selcukbiricik, O.S.; Yegen, G.; Tanakol, R.; Aral, F. Prevalence of papillary thyroid cancer in subacute thyroiditis patients may be higher than it is presumed: Retrospective analysis of 137 patients. Radiol. Oncol. 2018, 52, 257–262. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-K.; Lin, C.-L.; Chang, Y.-J.; Cheng, F.T.-F.; Peng, C.-L.; Sung, F.-C.; Cheng, Y.-H.; Kao, C.-H. Cancer risk in patients with graves’ disease: A nationwide cohort study. Thyroid 2013, 23, 879–884. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.K.; Lin, C.L.; Cheng, F.T.F.; Sung, F.C.; Kao, C.H. Cancer risk in patients with hashimoto’s thyroiditis: A nationwide cohort study. Br. J. Cancer 2013, 109, 2496–2501. [Google Scholar] [CrossRef] [Green Version]
- Hopper, K.D. Orbital, thyroid, and breast superficial radiation shielding for patients undergoing diagnostic ct. Semin. Ultrasound. CT MR 2002, 23, 423–427. [Google Scholar] [CrossRef]
- Abuzaid, M.M.; Elshami, W.; Haneef, C.; Alyafei, S. Thyroid shield during brain ct scan: Dose reduction and image quality evaluation. Imaging Med. 2017, 9, 45–48. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Comparison Group n = 34,684 | CT Scan Group n = 14,041 | p Value |
|---|---|---|---|
| Age | <0.0001 | ||
| 0–18 | 9479 (27.33%) | 2075 (14.78%) | |
| 19–45 | 14,214 (40.98%) | 4831 (34.41%) | |
| 46–65 | 6983 (20.13%) | 3477 (24.76%) | |
| >65 | 4008 (11.56%) | 3658 (26.05%) | |
| Sex | 0.0291 | ||
| Female | 15,529 (44.77%) | 6439 (45.86%) | |
| Male | 19,155 (55.23%) | 7602 (54.14%) | |
| Co-morbidities | |||
| Diabetes mellitus | 2320 (6.69%) | 1864 (13.28%) | <0.0001 |
| Hypertension | 4775 (13.77%) | 3729 (26.56%) | <0.0001 |
| COPD ** | 3335 (9.62%) | 1797 (12.80%) | <0.0001 |
| Coronary artery disease | 1462 (4.22%) | 1282 (9.13%) | <0.0001 |
| Cancer | 669 (1.93%) | 498 (3.55%) | <0.0001 |
| Hospital stays (days) within 1 month | <0.0001 | ||
| 0 | 31,292 (90.22%) | 9638 (68.64%) | |
| 1–7 | 2727 (7.86%) | 3364 (23.96%) | |
| 8–14 | 665 (1.92%) | 1039 (7.40%) | |
| Frequency of CT scan within 14 days | - | ||
| 1 | 0 (0%) | 13,217 (94.13%) | |
| ≥2 | 0 (0%) | 824 (5.87%) | |
| Frequency of CT scan within 2 months | - | ||
| 1 | 5 (0.01%) | 13,112 (93.38%) | |
| ≥2 | 0 (0%) | 929 (6.62%) | |
| Mortality within 6 months | 307 (0.89%) | 219 (1.56%) | <0.0001 |
| Follow-Up Person-Months | Case of Thyroid Diseases | Incidence Rate *(95% CI) | IRR | |
|---|---|---|---|---|
| Comparison group | 1,076,856 | 539 | 0.50 (0.46–0.54) | 1 |
| CT scan group | 386,042 | 213 | 0.55 (0.48–0.63) | 1.10 (0.94–1.29) |
| 1 time | 362,352 | 198 | 0.55 (0.48–0.63) | 1.10 (0.94–1.29) |
| ≥2 times | 23,690 | 15 | 0.63 (0.38–1.05) | 1.09 (0.93–1.28) |
| Variable | aHR | 95% CI | p-Value |
|---|---|---|---|
| CT exposure | |||
| Comparisons | Reference | - | - |
| 1 time | 0.933 | 0.787–1.107 | 0.4286 |
| ≥2 times | 1.053 | 0.618–1.794 | 0.8496 |
| Age | |||
| 0–18 | Reference | - | - |
| 19–45 | 0.666 | 0.534–0.829 | 0.0003 |
| 46–65 | 1.096 | 0.902–1.331 | 0.3567 |
| <65 | 1.065 | 0.830–1.367 | 0.6187 |
| Sex | |||
| Female | Reference | - | - |
| Male | 0.383 | 0.327–0.447 | <0.0001 |
| Co-morbidities | |||
| Diabetes mellitus | 1.246 | 0.975–1.593 | 0.0789 |
| Hypertension | 1.102 | 0.878–1.384 | 0.4027 |
| COPD | 1.511 | 1.216–1.877 | 0.0002 |
| Coronary artery disease | 1.168 | 0.869–1.569 | 0.3029 |
| Cancer | 1.716 | 1.187–2.480 | 0.0041 |
| Hospital stays (days) within 1 month | |||
| 0 | Reference | - | - |
| 1–7 | 1.000 | 0.802–1.245 | 0.9973 |
| 8–14 | 1.365 | 0.977–1.907 | 0.0679 |
| aHR (95% C.I.) | |||
|---|---|---|---|
| CT Exposure | |||
| Diagnosis | Comparisons | 1 time | ≥2 times |
| Thyroid disease (ICD-9 240–246) | Reference | 0.933 (0.787–1.107) | 1.053 (0.618–1.794) |
| Simple and unspecified, nontoxic nodular goiter (ICD-9 240–241) | Reference | 0.928 (0.698–1.235) | 0.769 (0.241–2.457) |
| Thyrotoxicosis with or without goiter (ICD-9 242) | Reference | 0.850 (0.603–1.200) | 0.755 (0.232–2.457) |
| Acquired hypothyroidism, thyroiditis (ICD-9 244, 245) | Reference | 1.104 (0.758–1.608) | 1.796 (0.699–4.619) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsao, S.-L.; Chen, Y.-Y.; Yeh, L.-T.; Huang, J.-Y.; Li, W.-T.; Yang, S.-F.; Yeh, C.-B. Impact of Computed Tomography Scans on the Risk of Thyroid Disease in Minor Head Injury Patients: A Population-Based Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 3873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113873
Tsao S-L, Chen Y-Y, Yeh L-T, Huang J-Y, Li W-T, Yang S-F, Yeh C-B. Impact of Computed Tomography Scans on the Risk of Thyroid Disease in Minor Head Injury Patients: A Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(11):3873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113873
Chicago/Turabian StyleTsao, Shao-Lun, Yin-Yang Chen, Liang-Tsai Yeh, Jing-Yang Huang, Wen-Tyng Li, Shun-Fa Yang, and Chao-Bin Yeh. 2020. "Impact of Computed Tomography Scans on the Risk of Thyroid Disease in Minor Head Injury Patients: A Population-Based Retrospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 11: 3873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113873