The Impact of a Gradual Healthier Assortment among Vocational Schools Participating in a School Canteen Programme: Evidence from Sales and Student Survey Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Context
2.2. Study Design and Procedures
2.3. Manipulation Check: Canteen Scan
2.4. Student Survey
2.5. Measures
2.5.1. Cash Register Data
2.5.2. Student Satisfaction
2.5.3. Customer Patronage
2.6. Data Analysis
3. Results
3.1. Descriptives
3.1.1. Canteen Choice Characteristics
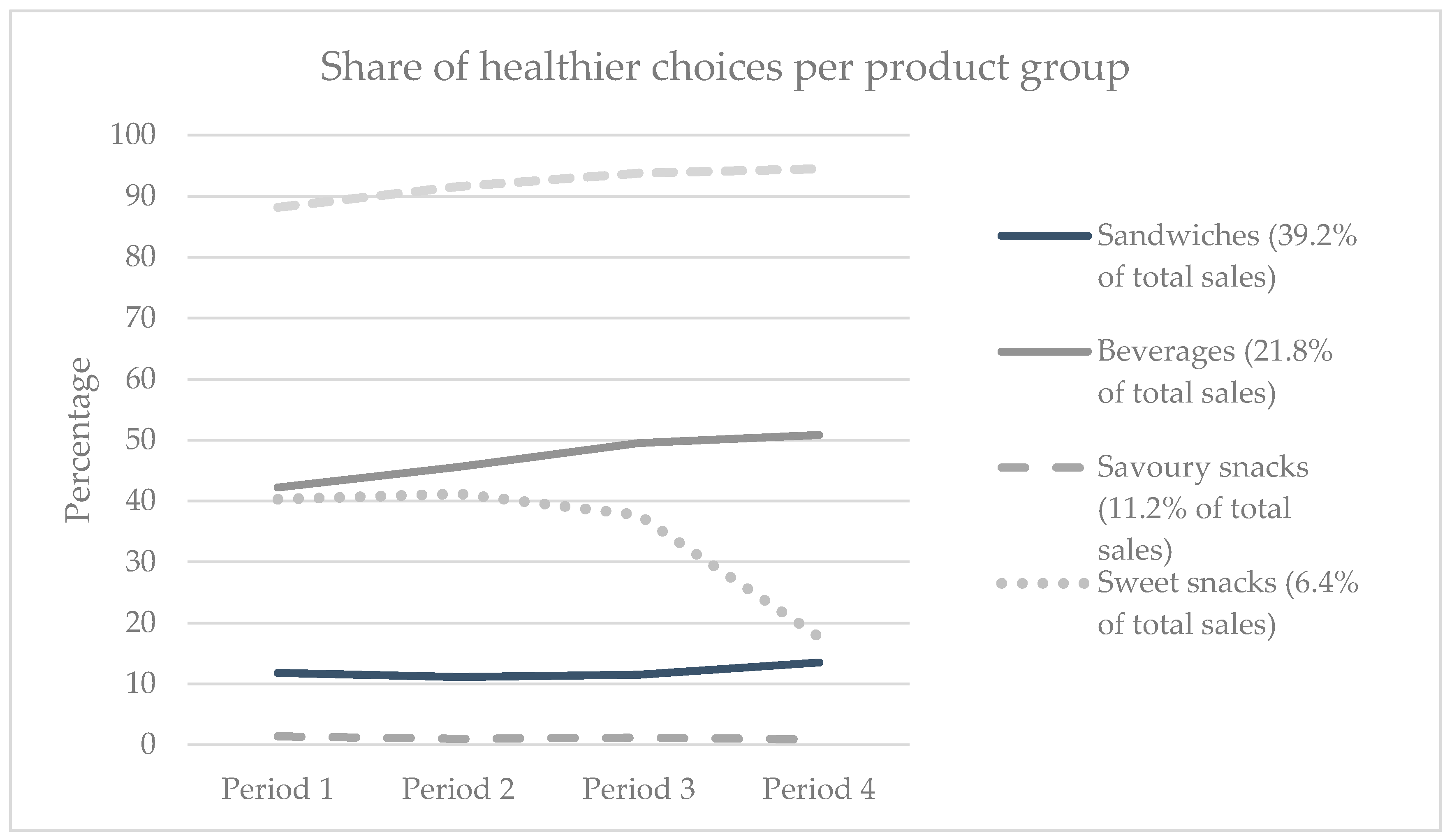
3.1.2. Differences between Product Groups
3.1.3. Spending and Share of Healthier Products per Transaction
3.1.4. Student Survey
3.2. Hypotheses Testing
3.2.1. Hypothesis 1: Increased Presence of Healthier Products Leads to Increased Sales of Healthier Products
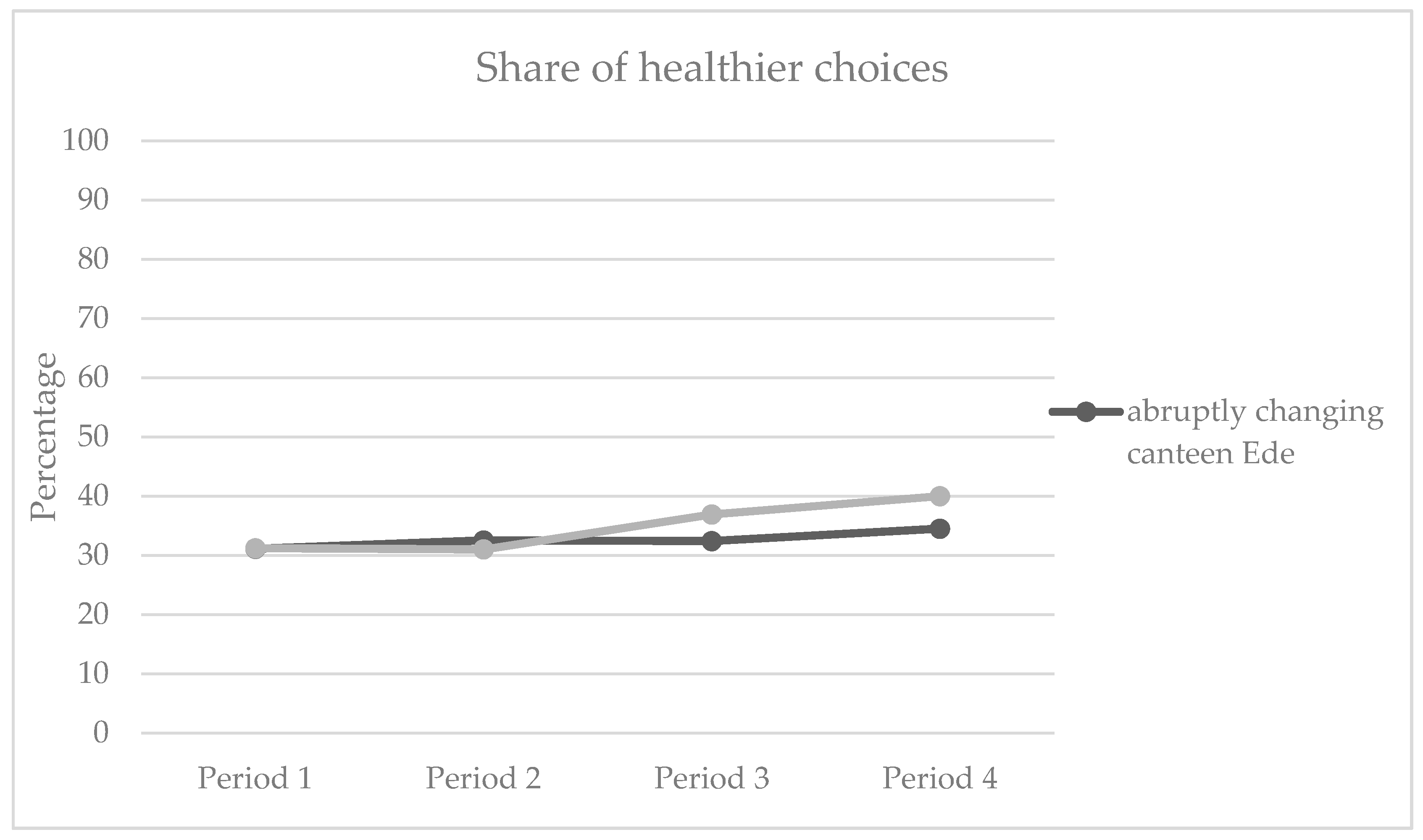
3.2.2. Hypothesis 2: Gradual Increase in Healthier Products Leads to Healthier Choices Than an Abrupt Increase
3.3. Additional Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van Rossum, C.T.; Fransen, H.P.; Verkaik-Kloosterman, J.; Buurma-Rethans, E.J.; Ocke, M.C. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years; RIVM Report 350050006; National Institute for Public Health and the Environment: Bilthoven, The Netherlands, 2011.
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in children’s and adolescents’ body mass index, underweight, overweight and obesity, in comparison with adults, from 1975 to 2016: A pooled analysis of 2,416 population-based measurement studies with 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar]
- Story, M.; Nanney, M.S.; Schwartz, M.B. Schools and obesity prevention: Creating school environments and policies to promote healthy eating and physical activity. Milbank Q. 2009, 87, 71–100. [Google Scholar] [CrossRef] [PubMed]
- Barnes, C. Mediating good food and moments of possibility with Jamie Oliver: Problematising celebrity chefs as talking labels. Geoforum 2017, 84, 169–178. [Google Scholar] [CrossRef]
- Driessen, C.E.; Cameron, A.J.; Thornton, L.E.; Lai, S.K.; Barnett, L.M. Effect of changes to the school food environment on eating behaviours and/or body weight in children: A systematic review. Obes. Rev. 2014, 15, 968–982. [Google Scholar] [CrossRef] [PubMed]
- Terry-McElrath, Y.M.; O’Malley, P.M.; Johnston, L.D. Foods and beverages offered in US public secondary schools through the National School Lunch Program from 2011–2013: Early evidence of improved nutrition and reduced disparities. Prev. Med. 2015, 78, 52–58. [Google Scholar] [CrossRef]
- Cullen, K.W.; Watson, K.; Zakeri, I.; Ralston, K. Exploring changes in middle-school student lunch consumption after local school food service policy modifications. Public Health Nutr. 2006, 9, 814–820. [Google Scholar] [CrossRef] [Green Version]
- Moore, L.; Tapper, K. The impact of school fruit tuck shops and school food policies on children’s fruit consumption: A cluster randomised trial of schools in deprived areas. J. Epidemiol. Community Health 2008, 62, 926–931. [Google Scholar] [CrossRef]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Penalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef]
- Marcano-Olivier, M.I.; Horne, P.J.; Viktor, S.; Erjavec, M. Using nudges to promote healthy food choices in the school dining room: A systematic review of previous investigations. J. Sch. Health 2020, 90, 143–157. [Google Scholar] [CrossRef]
- Devi, A.; Surender, R.; Rayner, M. Improving the food environment in UK schools: Policy opportunities and challenges. J. Public Health Policy 2010, 31, 212–226. [Google Scholar] [CrossRef]
- Williams, J.; Scarborough, P.; Matthews, A.; Cowburn, G.; Foster, C.; Roberts, N.; Rayner, M. A systematic review of the influence of the retail food environment around schools on obesity-related outcomes. Obes. Rev. 2014, 15, 359–374. [Google Scholar] [CrossRef] [PubMed]
- Welker, E.; Lott, M.; Story, M. The school food environment and obesity prevention: Progress over the last decade. Curr. Obes. Rep. 2016, 5, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Veldhuis, L.; Mensink, F.; Wolvers, D. Guidelines for Healthier Canteens. Fact Sheet; Netherlands Nutrition Centre: The Hague, The Netherlands, 2017. [Google Scholar]
- Thaler, R.H.; Sunstein, C.R. Nudge: Improving Decisions about Health, Wealth, and Happiness; Penguin Books: New York, NY, USA, 2009. [Google Scholar]
- van Kleef, E.; van den Broek, O.; van Trijp, H.C. Exploiting the spur of the moment to enhance healthy consumption: Verbal prompting to increase fruit choices in a self-service restaurant. Appl. Psychol. Health Well-Being 2015, 7, 149–166. [Google Scholar] [CrossRef] [PubMed]
- Curhan, R.C. The effects of merchandising and temporary promotional activities on the sales of fresh fruits and vegetables in supermarkets. J. Mark. Res. 1974, 11, 286–294. [Google Scholar] [CrossRef]
- French, S.A.; Hannan, P.J.; Harnack, L.J.; Mitchell, N.R.; Toomey, T.L.; Gerlach, A. Pricing and availability intervention in vending machines at four bus garages. J. Occup. Environ. Med. 2010, 52 (Suppl. 1), S29. [Google Scholar] [CrossRef] [Green Version]
- Bos, C.; van der Lans, I.A.; van Kleef, E.; van Trijp, H.C. Promoting healthy choices from vending machines: Effectiveness and consumer evaluations of four types of interventions. Food Policy 2018, 79, 247–255. [Google Scholar] [CrossRef]
- Lombardini, C.; Lankoski, L. Forced choice restriction in promoting sustainable food consumption: Intended and unintended effects of the mandatory vegetarian day in Helsinki schools. J. Consum. Policy 2013, 36, 159–178. [Google Scholar] [CrossRef]
- Bassett, R.; Chapman, G.E.; Beagan, B.L. Autonomy and control: The co-construction of adolescent food choice. Appetite 2008, 50, 325–332. [Google Scholar] [CrossRef]
- Fletcher, A.; Jamal, F.; Fitzgerald-Yau, N.; Bonell, C. ‘We’ve got some underground business selling junk food’: Qualitative evidence of the unintended effects of English school food policies. Sociology 2014, 48, 500–517. [Google Scholar] [CrossRef]
- McDougal, B. Health Nazis Losing Obesity War as Pies Return to School Canteens. 2017. Available online: http://www.dailytelegraph.com.au/health-nazis-losing-obesity-war-as-pies-return-to-school-canteens/story-e6freuy9-1225734745940 (accessed on 20 December 2019).
- Drewnowski, A. Obesity, diets, and social inequalities. Nutr. Rev. 2009, 67 (Suppl. 1), S36–S39. [Google Scholar] [CrossRef]
- Boer, J.; Buurma-Rethans, E.; Hendriksen, M.; van Kranen, H.; Milder, I.; Ocke, M.; Verkaik-Kloosterman, J.; van Raaij, J. Health Aspects of the Dutch Diet: Background Report to What Is on Our Plate? Safe, Healthy and Sustainable Diets in The Netherlands; RIVM Report 2016-0197; National Institute for Public Health and the Environment: Bilthoven, The Netherlands, 2017.
- Health Council of the Netherlands. Guidelines for a Healthy Diet 2006; Health Council of the Netherlands: The Hague, The Netherlands, 2006.
- Evenhuis, I.; Wezenbeek, N.; Vyth, E.; Veldhuis, L.; Poelman, M.; Wolvers, D.; Seidell, J.C.; Renders, C.M. Development of the ‘Canteen Scan’: An online tool to monitor implementation of healthy canteen guidelines. BMC Public Health 2018, 18, 1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velema, E.; Vyth, E.L.; Hoekstra, T.; Steenhuis, I.H. Nudging and social marketing techniques encourage employees to make healthier food choices: A randomized controlled trial in 30 worksite cafeterias in The Netherlands. Am. J. Clin. Nutr. 2018, 107, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Pechey, R.; Cartwright, E.; Pilling, M.; Hollands, G.J.; Vasiljevic, M.; Jebb, S.A.; Marteau, T.M. Impact of increasing the proportion of healthier foods available on energy purchased in worksite cafeterias: A stepped wedge randomized controlled pilot trial. Appetite 2019, 133, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Van Kleef, E.; Seijdell, K.; Vingerhoeds, M.H.; de Wijk, R.A.; van Trijp, H.C. The effect of a default-based nudge on the choice of whole wheat bread. Appetite 2018, 121, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.J.; Dallas, S.K.; Harding, M.; Fitzsimons, G.J. The sales impact of featuring healthy foods, indulgent foods, or both: Finding from a large-scale field study. J. Assoc. Consum. Res. 2018, 3, 346–363. [Google Scholar] [CrossRef]
- Botti, S.; Broniarczyk, S.; Häubl, G.; Hill, R.; Huang, Y.; Kahn, B.; Kopalle, P.; Lehmann, D.; Urbany, J.; Wansink, B. Choice under restrictions. Mark. Lett. 2008, 19, 183–199. [Google Scholar] [CrossRef]
- Evans, C.E.; Christian, M.S.; Cleghorn, C.L.; Greenwood, D.C.; Cade, J.E. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am. J. Clin. Nutr. 2012, 96, 889–901. [Google Scholar] [CrossRef] [Green Version]
- Van Kleef, E.; Meeuwsen, T.; Rigterink, J.; Van Trijp, H.C.M. Moving towards a 100% healthy assortment in school food environments: Dutch vocational student and school professional perspectives. Br. Food J. 2019, 121, 2052–2066. [Google Scholar] [CrossRef]
- Hawkes, C.; Smith, T.G.; Jewell, J.; Wardle, J.; Hammond, R.A.; Friel, S.; Thow, A.M.; Kain, J. Smart food policies for obesity prevention. Lancet 2015, 385, 2410–2421. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Canteen | Academic Year (September til June) | |||
|---|---|---|---|---|
| Baseline period 1 (about two months) | Experimental period 2 (about two months) | Experimental period 3 (about 3–4 months) | Experimental period 4 (two months) * | |
| Canteen Ede | 60% Healthier Choice products in the assortment | 80% Healthier Choice products in the assortment | 80% Healthier Choice products in the assortment | 80% Healthier Choice products in the assortment |
| Canteen Velp | 60% Healthier Choice products in the assortment | 70% Healthier Choice products in the assortment | 80% Healthier Choice products in the assortment | 80% Healthier Choice products in the assortment |
| Canteen Ede (Fast Change to 80% Healthier Choice Products) | Canteen Velp (Slow Change to 80% Healthier Choice Products) | |||||||
|---|---|---|---|---|---|---|---|---|
| Period 1 (12 September–18 November) | Period 2 (19 November–15 January) | Period 3 (16 January–30 April) | Period 4 (1 May–1 July) | Period 1 (12 September–13 November) | Period 2 (14 November–15 January) | Period 3 (16 January–30 April) | Period 4 (1 May–1 July) | |
| # surveyed participants | 256 | 217 | 249 | 170 | 160 | 180 | 175 | 157 |
| % healthier choices displayed | 60% | 80% | 80% | 80% | 60% | 70% | 80% | 80% |
| Number of weeks open | 8 | 6 | 13 | 5 | 9 | 7 | 13 | 5 |
| Average total number of products sold per week | 4342 | 3720 | 4982 | 2606 | 2011 | 2455 | 1818 | 860 |
| % Healthier Choice products sold of total sales (total number sold) 1 | ||||||||
| Sandwiches | 12.1% (1704/14,122) | 10.8% (978/9083) | 10.5% (2769/26,426) | 12.5% (646/5171) | 11.2% (736/6561) | 11.5% (762/6655) | 14.6% (1200/8226) | 19.6% (284/1446) |
| Beverages | 40.5% (3027/7467) | 46.2% (2188/4740) | 48.1% (6858/14,244) | 46.5% (1399/3010) | 45.2% (1859/4114) | 44.8% (1616/3607) | 59.5% (2956/4967) | 62.4% (693/1110) |
| Savoury snacks | 1.4% (57/4013) | 0.9% (22/2474) | 1.3% (100/7995) | 0.7% (11/1500) | 1.3% (23/1816) | 1.1% (19/1773) | 1.0% (23/2265) | 1.8% (7/399) |
| Sweet snacks | 34.9% (751/2149) | 39.4% (467/1186) | 37.1% (1055/2845) | 15.0% (68/452) | 47.9% (720/1502) | 42.8% (580/1354) | 38.3% (1108/2894) | 21.6% (67/310) |
| Soups | 96.9% (1421/1467) | 94.3% (1164/1235) | 97.3% (3028/3112) | 98.0% (595/607) | 74.3% (681/916) | 88.5% (954/1078) | 87.6% (1529/1746) | 87.4% (263/301) |
| Dairy | 36.0% (644/1789) | 30.9% (305/986) | 36.1% (974/2696) | 48.6% (297/611) | 23.3% (375/1609) | 20.7 (206/995) | 20.0 (301/1507) | 27.4 (102/372) |
| Salads | 92.7% (662/714) | 87.8% (332/378) | 94.3% (1185/1256) | 97.6% (327/335) | 92.4% (194/210) | 78.7% (129/164) | 55.6% 2 (50/90) | 100% (44/44) |
| Sauces | 95.7% (1942/2029) | 93.2% (1417/1521) | 99.2% (3845/3877) | 100% (767/767) | 88.1% (922/1047) | 82.4% (842/1022) | 95.9% (1178/1229) | 100% (178/178) |
| Fruits and vegetables | 100% (443/443) | 100% (318/318) | 100% (952/952) | 100% (321/321) | 100% (112/112) | 100% (180/180) | 100% (346/346) | 100% (82/82) |
| Bread—no topping | 23.8% (127/534) | 14.2% (56/394) | 16.2% (218/1344) | 26.4% (66/250) | 9.0% (19/210) | 9.3% (33/356) | 11.3% (41/363) | 0% (0/59) |
| Revenues per transaction | 2.86 (1.58) | 2.70 (1.53) | 3.67 (2.43) | 2.88 (1.54) | 2.74(1.53) | 2.80 (1.84) | 3.20(2.11) | 2.56 (1.31) |
| Products sold per transaction | 1.56 (0.85) | 1.49 (0.81) | 2.01 (1.33) | 1.58 (0.84) | 1.59 (0.91) | 1.61 (1.01) | 1.95 (1.31) | 1.52 (0.79) |
| Characteristic | Ede | Velp | Total Sample |
|---|---|---|---|
| Gender | |||
| Male | 434 | 282 | 716 |
| Female | 458 | 390 | 848 |
| Total | 892 | 672 | 1564 |
| Age (mean, SD) | 18.8 (2.7) | 18.3 (2.1) | 18.6 (2.5) |
| Average number of days present at school | 4.4 (1.1) | 4.5 (0.9) | 4.4 (1.0) |
| Type of education followed | |||
| Business, Economics and Administration | 246 | 175 | 421 |
| Media, ICT, Image & Sound | 294 | 121 | 365 |
| Care and Wellbeing | 148 | 204 | 352 |
| Catering, Tourism, Recreation & Wellness | 60 | 69 | 126 |
| Another type of education | 144 | 103 | 247 |
| Canteen Ede (Fast Change to 80% ‘Healthier Choice’ Products) | Canteen Velp (Slow Change to 80% ‘Healthier Choice’ Products) | |||||||
|---|---|---|---|---|---|---|---|---|
| Period 1 (12 September–18 November) | Period 2 (19 November–15 January) | Period 3 (16 January–30 April) | Period 4 (1 May–1 July) | Period 1 (12 September–13 November) | Period 2 (14 November–15 January) | Period 3 (16 January–30 April) | Period 4 (1 May–1 July) | |
| Cash Register Data | ||||||||
| Relative proportion of Healthier Choice products sold of total sales (%) | 31.1% | 32.5% | 32.4% | 34.5% | 31.2% | 31.0% | 36.9% | 40.0% |
| Relative proportion of Healthier Choice products sold per transaction (%) | 29.9% | 31.0% | 31.0% | 33.1% | 29.7% | 30.2% | 35.5% | 39.7% |
| Student Satisfaction | ||||||||
| I am satisfied about this canteen * | 3.2 (0.9) | 3.2 (0.8) | 3.1 (0.8) | 3.0 (0.8) | 2.9 (0.9) | 3.1 (1.0) | 2.9 (0.8) | 3.0 (0.9) |
| In this canteen you can eat healthily * | 3.4 (0.8) | 3.4 (0.8) | 3.3 (0.8) | 3.2 (0.7) | 3.2 (0.8) | 3.3 (0.8) | 3.2 (0.7) | 3.2 (0.8) |
| I feel free to choose what I like * | 3.6 (0.9) | 3.6 (0.9) | 3.6 (0.9) | 3.4 (0.9) | 3.4 (1.0) | 3.6 (1.0) | 3.3 (0.9) | 3.6 (1.0) |
| Outlet Choice | ||||||||
| Where do you get your lunch? | ||||||||
| Entirely bought at school | 18.8% | 8.3% | 10.4% | 5.9% | 1.9% | 7.2% | 7.4% | 3.2% |
| Partly bought at school | 44.1% | 61.3% | 43.4% | 50.0% | 28.7% | 40.0% | 29.1% | 48.4% |
| Entirely from somewhere else | 37.1% | 30.4% | 46.2% | 44.1% | 69.4% | 52.8% | 63.4% | 48.4% |
| Where do you get your drinks? | ||||||||
| Entirely bought at school | 14.5% | 7.4% | 10.0% | 7.1% | 2.5% | 7.8% | 8.0% | 5.1% |
| Partly bought at school | 28.5% | 39.2% | 27.7% | 38.2% | 18.1% | 28.9% | 25.1% | 31.2% |
| Entirely from somewhere else | 57.0% | 53.5% | 62.2% | 54.7% | 79.4% | 63.3% | 66.9% | 63.7% |
| Where do you get your snacks? | ||||||||
| Entirely bought at school | 13.7% | 6.9% | 9.2% | 5.9% | 3.1% | 7.2% | 6.3% | 5.1% |
| Partly bought at school | 31.6% | 26.3% | 26.5% | 34.7% | 18.8% | 32.2% | 22.9% | 31.8% |
| Entirely from somewhere else | 54.7% | 66.8% | 64.3% | 59.4% | 78.1% | 60.6% | 70.9% | 63.1% |
| Unstandardized Intercept B0 | Unstandardized B (Dummy Contrast) | Fit | |
|---|---|---|---|
| Cash register data (H1) | |||
| Ede (60 –> 80% period change) | |||
| Healthy choice | 0.80 | −0.08 * | 31.87 a |
| Velp (60 –> 70% period change) | |||
| Healthy choice | 0.79 | 0.01 | 0.20 a |
| Velp (60 –> 80% period change) | |||
| Healthy choice | 0.79 | −0.28 * | 187.07 a |
| Student satisfaction (additional measure) | |||
| Ede (60 –> 80% period change) | |||
| Satisfaction | 3.05 | 0.10 | 0.02 b |
| Can eat healthily | 3.28 | 0.07 | 0.01 b |
| Free to choose | 3.52 | 0.07 | 0.01 b |
| Velp (60 –> 70% –> 80% period change) | |||
| Satisfaction | 3.05 | −0.04 | 0.02 b |
| Can eat healthily | 3.28 | −0.03 | 0.01 b |
| Free to choose | 3.52 | −0.03 | 0.01 b |
| Customer patronage (additional measure) | |||
| Ede (60 –> 80% period change) | |||
| Lunch (school purchase) | −0.04 | −0.35 * | 7.39 a |
| Drinks (school purchase) | 0.53 | −0.35 * | 6.78 a |
| Snacks (school purchase) | 0.62 | −0.47 * | 11.82 a |
| Velp (60 –> 70% –> 80% period change) | |||
| Lunch (school purchase) | −0.04 | 0.14 * | 7.39 a |
| Drinks (school purchase) | 0.53 | 0.14 * | 6.78 a |
| Snacks (school purchase) | 0.62 | 0.19 * | 11.82 a |
| Unstandardized Intercept B0 | Unstandardized B (Dummy Contrast) | Fit | |
|---|---|---|---|
| Cash register data (H2) | |||
| Healthy choice | 0.68 * | −0.08 * | 0.003 b 31.87 a |
| Student evaluation (additional measure) | |||
| Satisfaction | 3.05 | 0.01 | 0.02 b |
| Can eat healthily | 3.28 | 0.01 | 0.01 b |
| Free to choose | 3.52 | 0.01 | 0.01 b |
| Customer patronage (additional measure) | |||
| Lunch (school purchase) | −0.04 | −0.04 * | 7.39 a |
| Drinks (school purchase) | 0.53 | −0.04 * | 6.78 a |
| Snacks (school purchase) | 0.62 | −0.06 * | 11.82 a |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Kleef, E.; Kremer, F.; van Trijp, H.C.M. The Impact of a Gradual Healthier Assortment among Vocational Schools Participating in a School Canteen Programme: Evidence from Sales and Student Survey Data. Int. J. Environ. Res. Public Health 2020, 17, 4352. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124352
van Kleef E, Kremer F, van Trijp HCM. The Impact of a Gradual Healthier Assortment among Vocational Schools Participating in a School Canteen Programme: Evidence from Sales and Student Survey Data. International Journal of Environmental Research and Public Health. 2020; 17(12):4352. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124352
Chicago/Turabian Stylevan Kleef, Ellen, Florine Kremer, and Hans C. M. van Trijp. 2020. "The Impact of a Gradual Healthier Assortment among Vocational Schools Participating in a School Canteen Programme: Evidence from Sales and Student Survey Data" International Journal of Environmental Research and Public Health 17, no. 12: 4352. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124352