A Snapshot of Knowledge about Oral Cancer in Italy: A 505 Person Survey


Abstract
:1. Introduction
2. Materials and Methods
- (1)
- Do you have family members/acquaintances diagnosed with oral cancer? Yes or no
- (2)
- Do you have relatives in dental or medical fields? Yes or no
- (3)
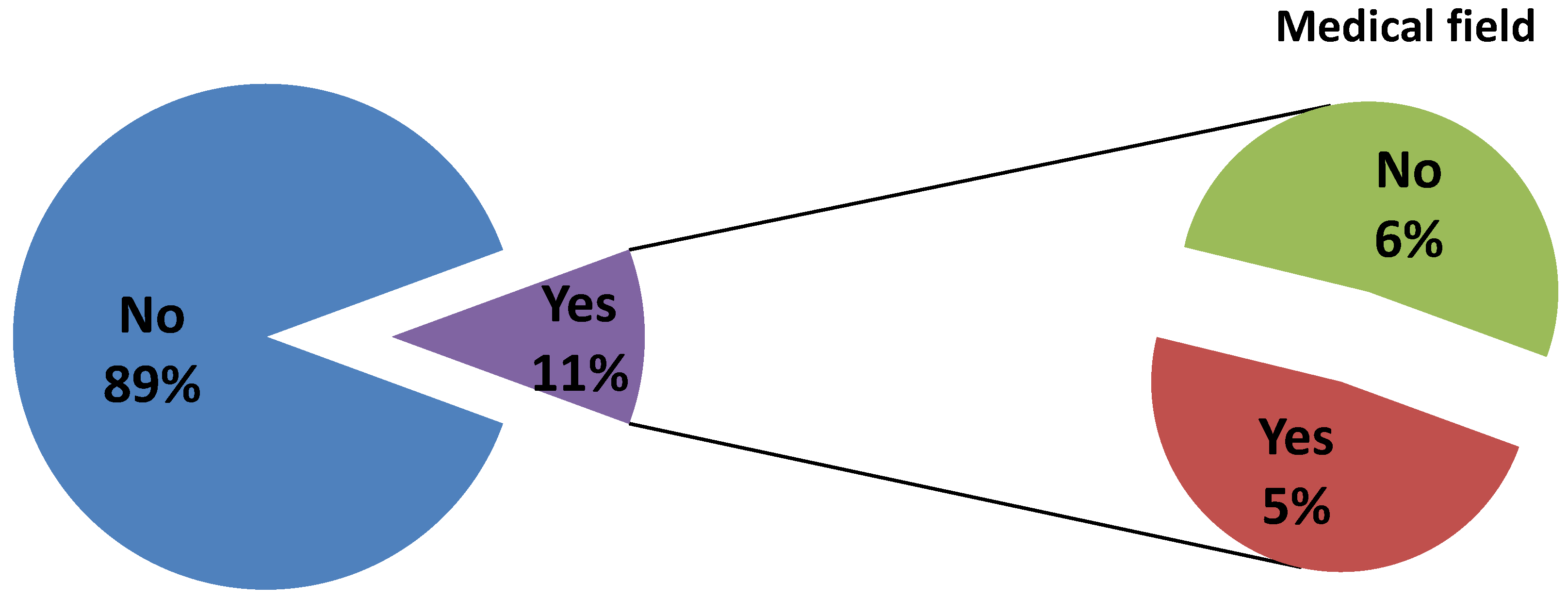
- Are you belonging to medical/dental field? Yes or no
- (4)
- Do you know the existence of cancer of the mouth and lips? Yes or no
- (5)
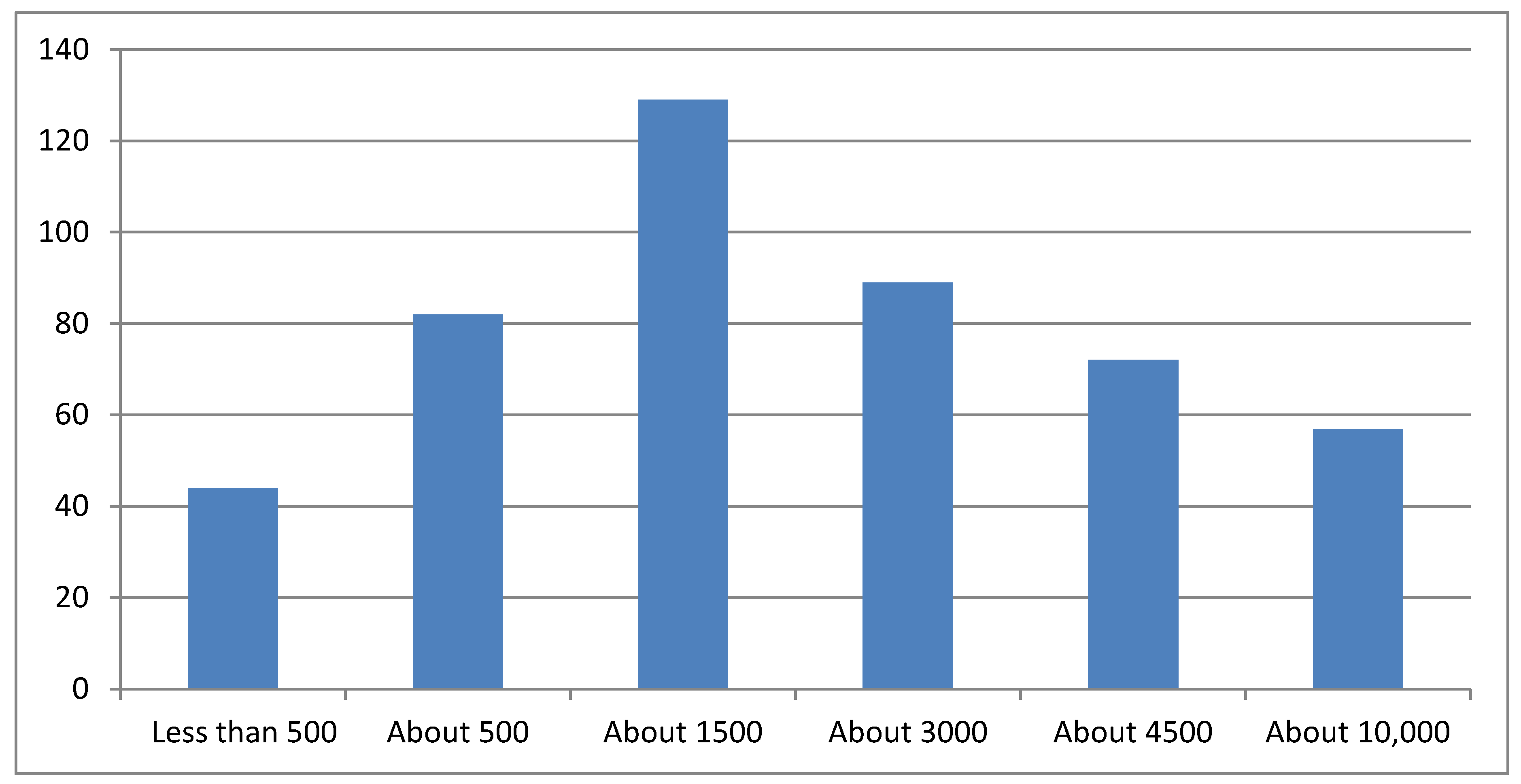
- As far as you are aware, how many cases of oral cancer are registered in Italy every year?
- (a)
- Fewer than 500
- (b)
- About 500
- (c)
- About 1500
- (d)
- About 3000
- (e)
- About 4500
- (f)
- About 6000
- (g)
- More than 10,000
- (6)
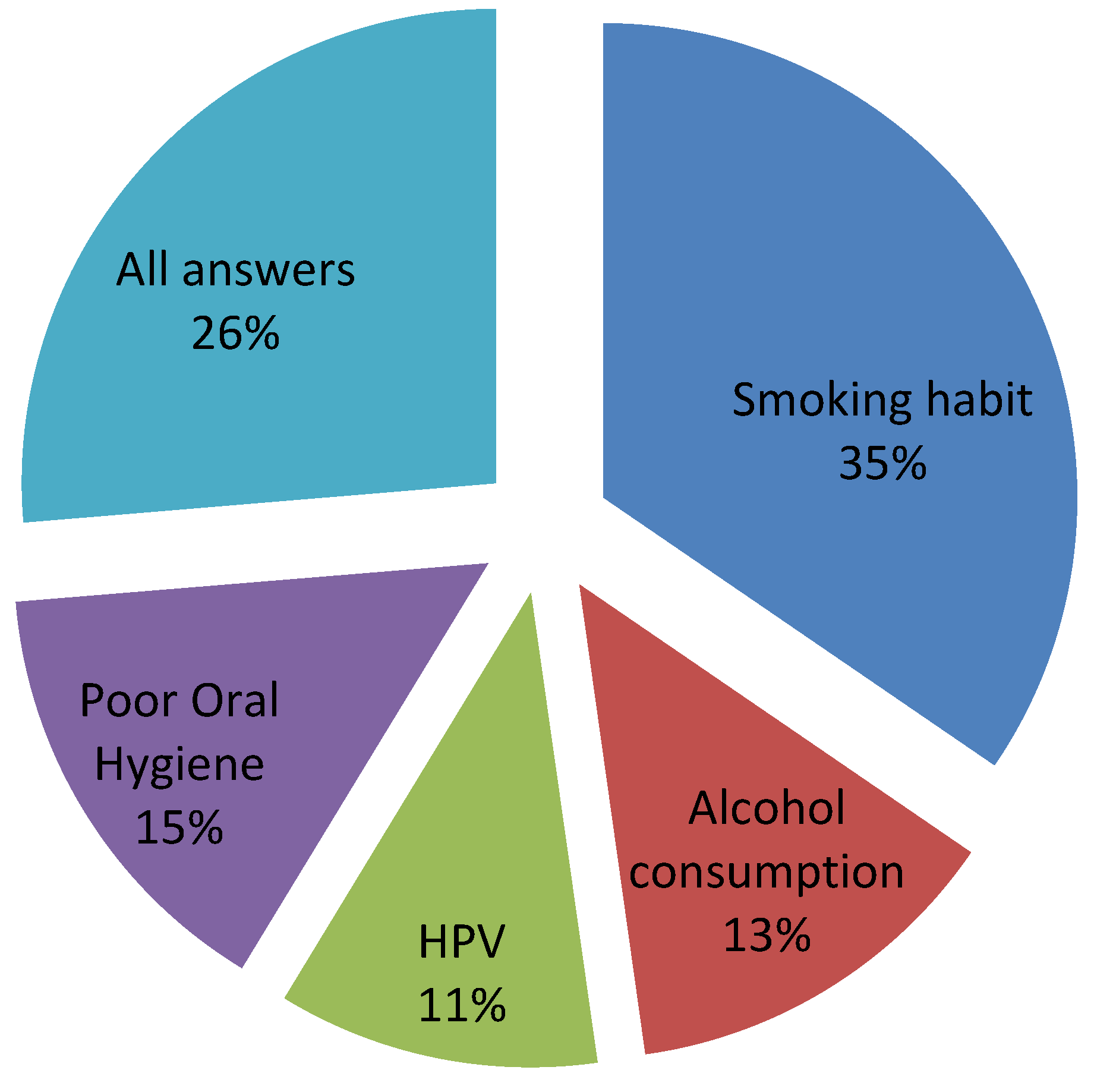
- Which of these factors are related to an increased risk of oral cancer?
- (a)
- Smoking habit
- (b)
- Alcohol consumption
- (c)
- Papilloma virus
- (d)
- Poor hygiene
- (e)
- All previous answers
- (7)
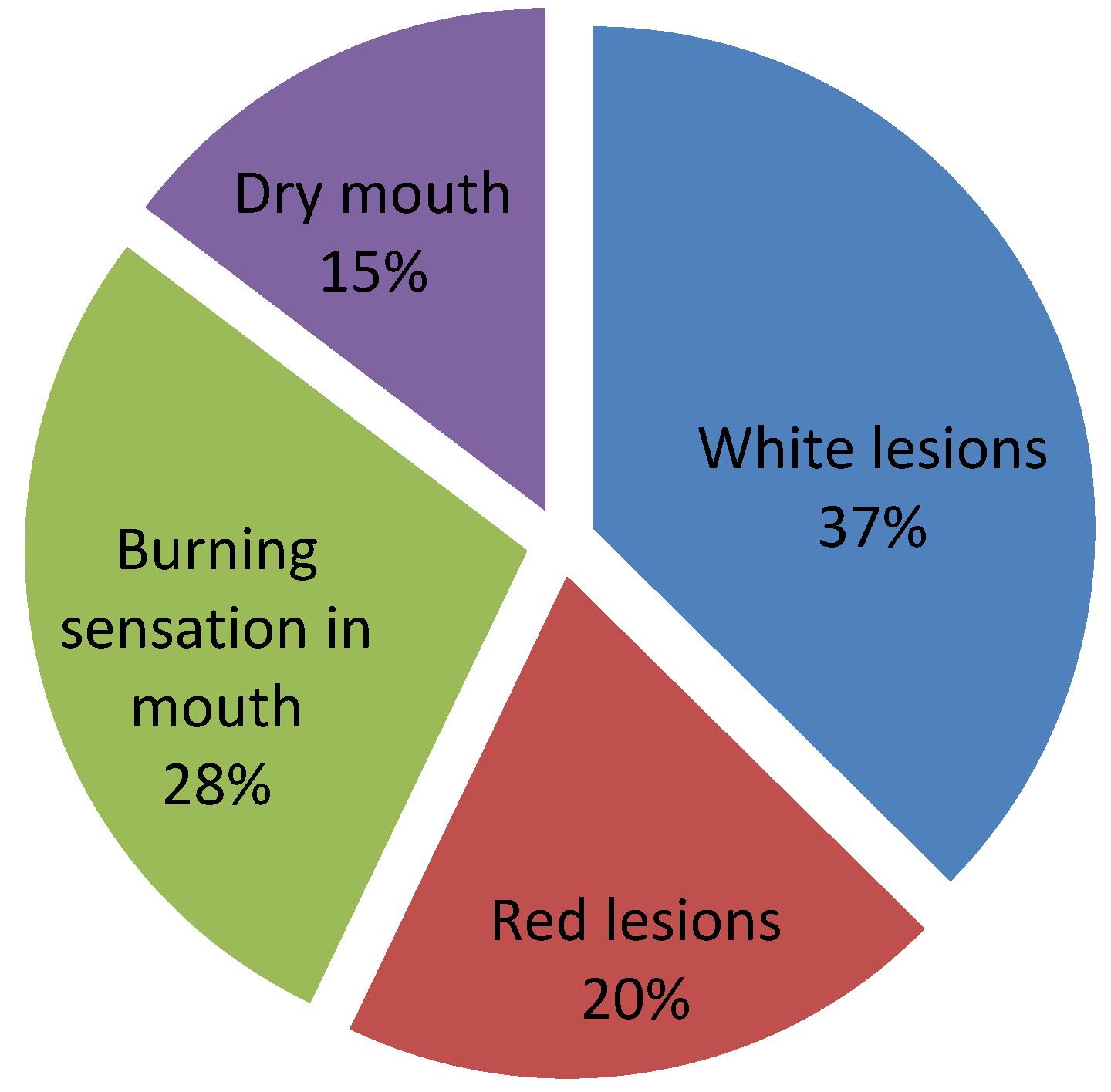
- Which of these features can be initial presentations of oral carcinoma?
- (a)
- White plaque
- (b)
- Reddish plaque
- (c)
- Spreading burning sensation in the mouth
- (d)
- Dry mouth
- (8)
- Do you know how to self-inspect your mouth? Yes or no
- (9)
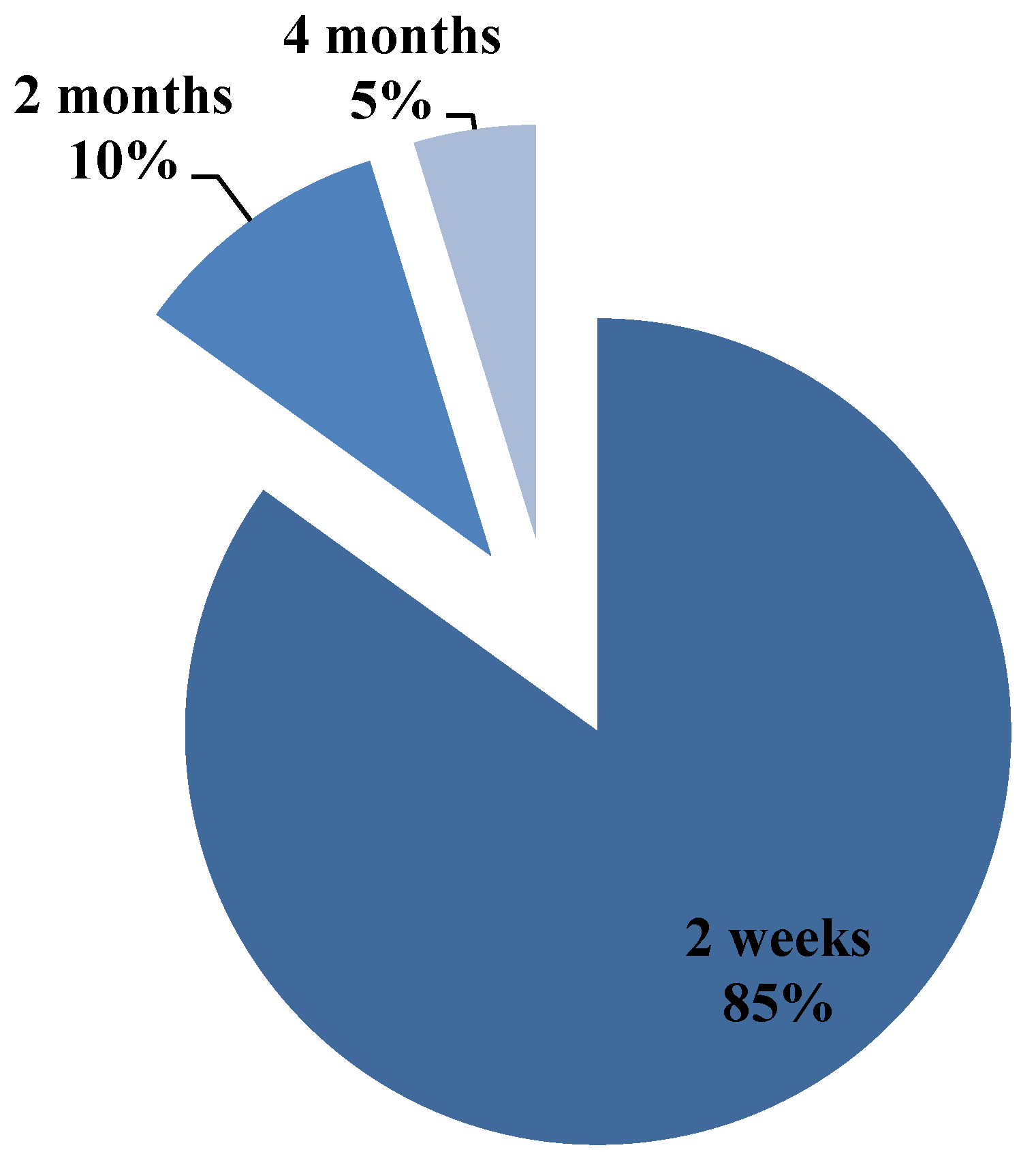
- If you notice an ulcer on your tongue, how long would you wait before seeking medical attention?
- (a)
- 2 weeks
- (b)
- 2 months
- (c)
- 4 months
- (10)
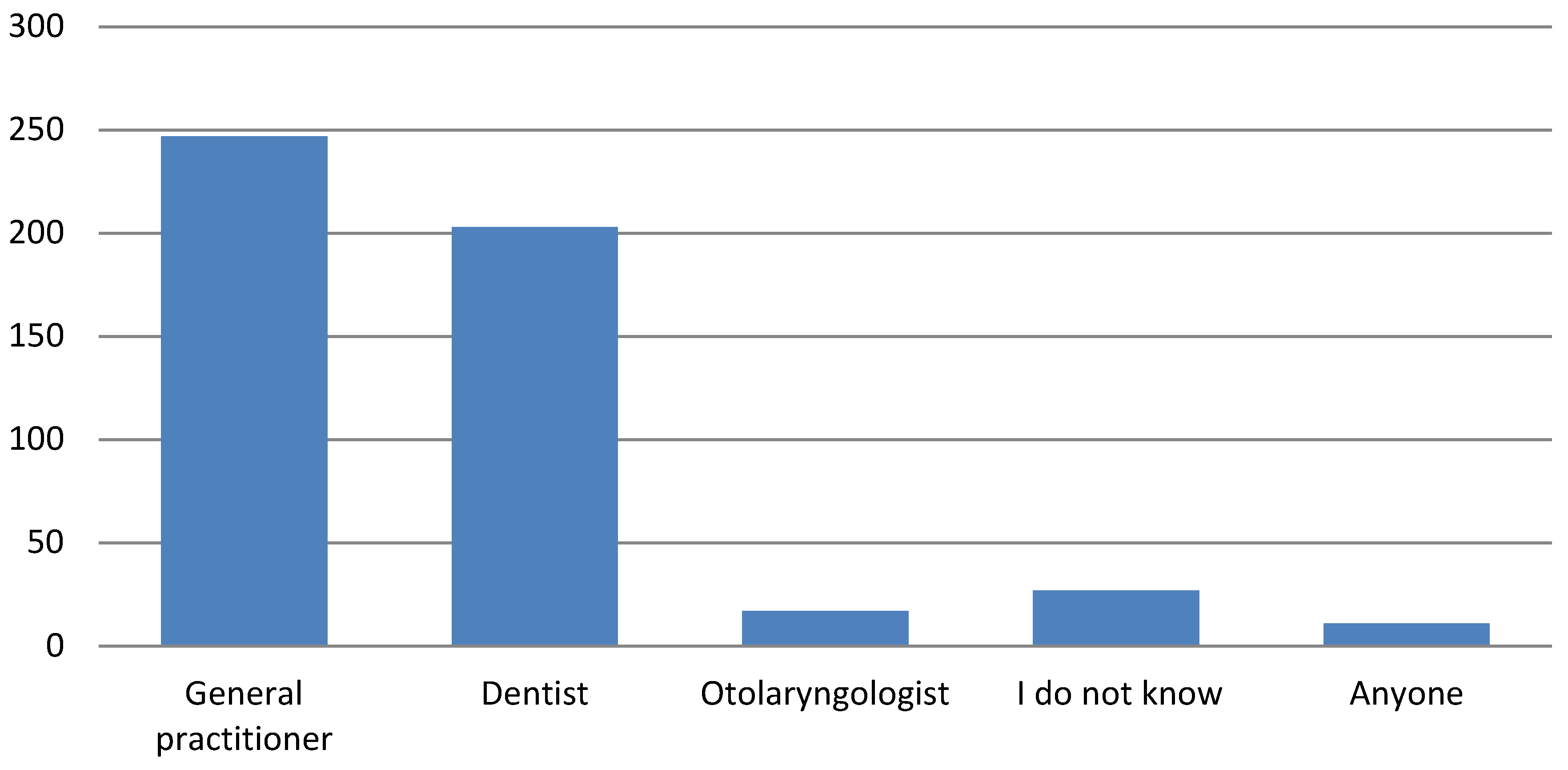
- Whom would you seek out to check it?
- (a)
- General practitioner
- (b)
- Dentist
- (c)
- Otolaryngologist
- (d)
- Anyone
- (e)
- I do not know
- (11)
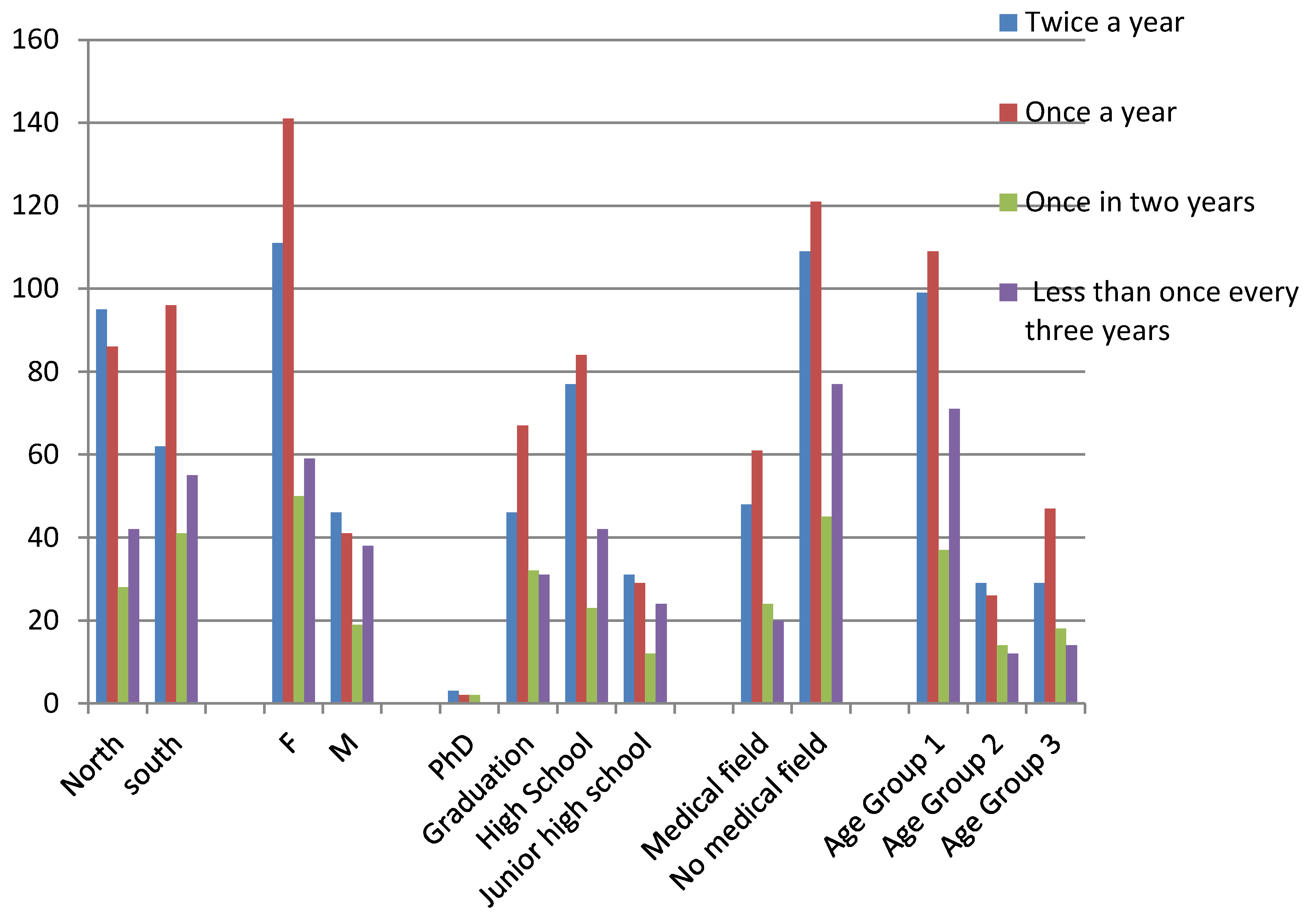
- How often do you visit the dentist?
- (a)
- Twice a year
- (b)
- Once a year
- (c)
- Once in two years
- (d)
- Less than once every three years
Ethical Considerations
3. Statistical Analysis
- Demographic data of population
- Knowledge about incidence of oral cancer in Italy
- existence of oral and lip cancers,
- risk factors,
- features of oral cancer lesions,
- habits of self-inspection,
- waiting time before seeking medical attention,
- professional reference figures,
- habits of routine dental visits.
4. Results
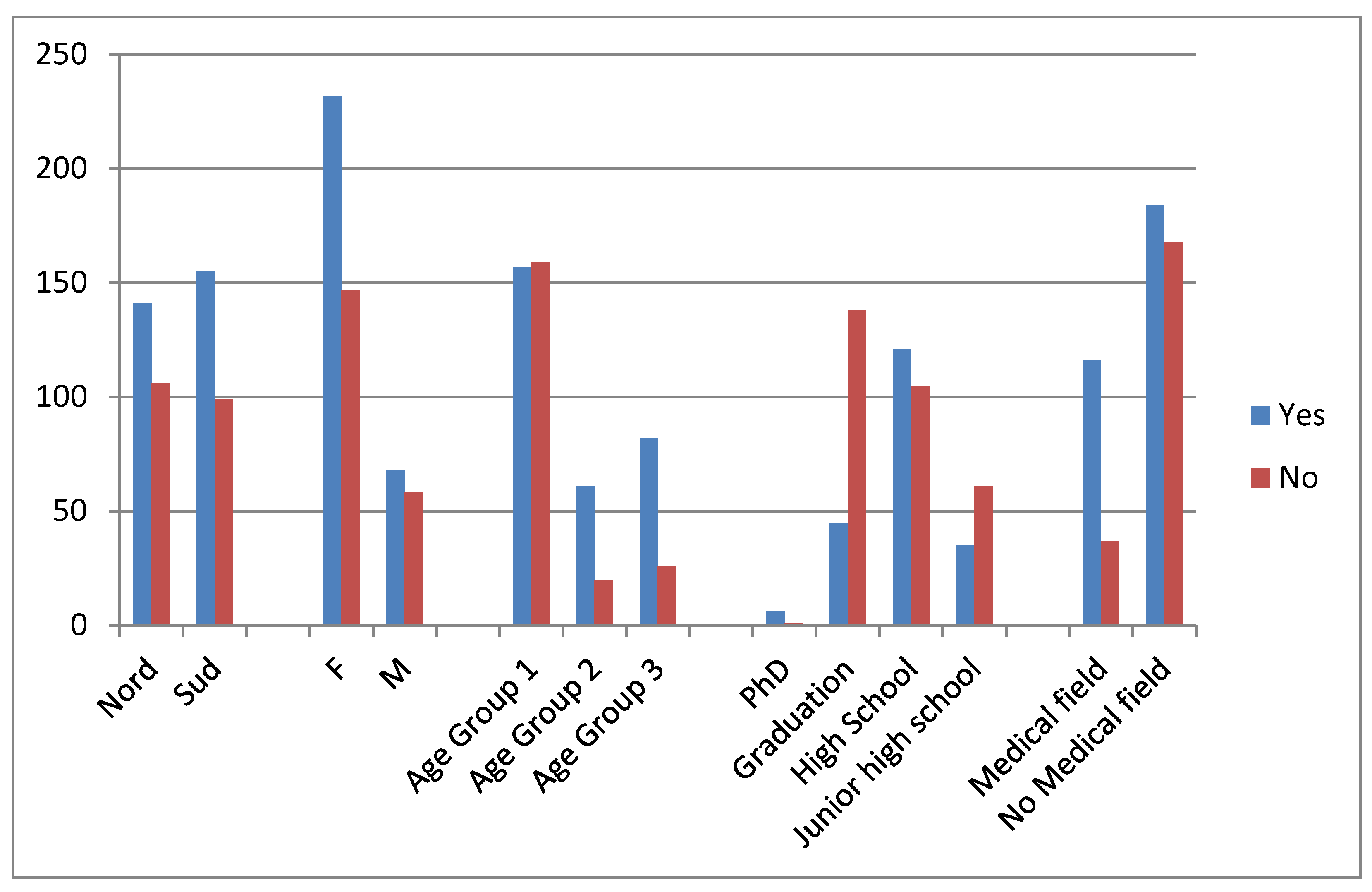
4.1. Demographic Data of Population
4.2. Existence of Oral and Lip Cancers
4.3. Knowledge about Incidence of Oral Cancer in Italy
4.4. Risk Factors
4.5. Features of Oral Cancer Lesions
4.6. Habits of Self-Inspection
4.7. Time Waited before Seeking Medical Attention
4.8. Professional Reference Figures
4.9. Habits of Routine Dental Visits
5. Discussion
6. Future Outlook
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rivera, C. Essentials of oral cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884–11894. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Choudhari, S.K.; Chaudhary, M.; Gadbail, A.R.; Sharma, A.; Tekade, S. Oxidative and antioxidative mechanisms in oral cancer and precancer: A review. Oral Oncol. 2014, 50, 10–18. [Google Scholar] [CrossRef]
- Reidy, J.; McHugh, E.; Stassen, L.F.A. A review of the relationship between alcohol and oral cancer. Surgeon 2011, 9, 278–283. [Google Scholar] [CrossRef]
- Termine, N.; Panzarella, V.; Falaschini, S.; Russo, A.; Matranga, D.; Lo Muzio, L.; Campisi, G. HPV in oral squamous cell carcinoma vs head and neck squamous cell carcinoma biopsies: A meta-analysis (1988–2007). Ann. Oncol. 2008, 19, 1681–1690. [Google Scholar] [CrossRef]
- Yete, S.; D’Souza, W.; Saranath, D. High-Risk Human Papillomavirus in Oral Cancer: Clinical Implications. Oncology 2018, 94, 133–141. [Google Scholar] [CrossRef]
- Gupta, B.; Bray, F.; Kumar, N.; Johnson, N.W. Associations between oral hygiene habits, diet, tobacco and alcohol and risk of oral cancer: A case–control study from India. Cancer Epidemiol. 2017, 51, 7–14. [Google Scholar] [CrossRef]
- Singhvi, H.R.; Malik, A.; Chaturvedi, P. The role of chronic mucosal trauma in oral cancer: A review of literature. Indian J. Med. Paediatr. Oncol. 2017, 38, 44–50. [Google Scholar]
- Jitender, S.; Sarika, G.; Varada, H.R.; Omprakash, Y.; Mohsin, K. Screening for oral cancer. J. Exp. Ther. Oncol. 2016, 11, 303–307. [Google Scholar]
- Güneri, P.; Epstein, J.B. Late stage diagnosis of oral cancer: Components and possible solutions. Oral Oncol. 2014, 50, 1131–1136. [Google Scholar] [CrossRef]
- Richards, D. Patient delay in reporting oral cancer is poorly understood. Evid.-Based Dent. 2007, 8, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Archilla, A. Diagnostic Delay in Oral Cancer, 2017. Available online: https://scientonline.org/abstract/21675/Diagnostic-Delay-in-Oral-Cancer (accessed on 1 July 2020).
- Panzarella, V.; Pizzo, G.; Calvino, F.; Compilato, D.; Colella, G.; Campisi, G. Diagnostic delay in oral squamous cell carcinoma: The role of cognitive and psychological variables. Int. J. Oral Sci. 2014, 6, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi. J. Anaesth. 2017, 11 (Suppl. 1), S80–S89. [Google Scholar] [CrossRef]
- Monteiro, L.S.; Salazar, F.; Pacheco, J.; Warnakulasuriya, S. Oral cancer awareness and knowledge in the city of valongo, portugal. Int. J. Dent. 2012, 2012, 376838. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.M.; Cushen, S.; Schellekens, H.; Bhuachalla, E.N.; Burns, L.; Kenny, U.; Power, D.G. Poor awareness of risk factors for cancer in Irish adults: Results of a large survey and review of the literature. Oncologist 2015, 20, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa, A.; Kreimer, A.R.; Pasi, M.; Polimeni, A.; Cicciù, D.; Strohmenger, L.; Gherlone, E.; Abati, S. Oral cancer knowledge: A survey administered to patients in dental departments at large Italian hospitals. J. Cancer Educ. 2011, 26, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Nocini, R.; Lippi, G.; Mattiuzzi, C. The worldwide burden of smoking-related oral cancer deaths. Clin. Exp. Dent. Res. 2020, 6, 161–164. [Google Scholar] [CrossRef]
- Zotti, F.; Nocini, R.; Capocasale, G.; Fior, A.; Peretti, M.; Albanese, M. Malignant transformation evidences of Oral Lichen Planus: When the time is of the essence. Oral Oncol. 2020, 104, 104594. [Google Scholar] [CrossRef]
- Ganesh, D.; Sreenivasan, P.; Öhman, J.; Wallström, M.; Braz-Silva, P.H.; Giglio, D.; Kjeller, G.; Hasséus, B. Potentially malignant oral disorders and cancer transformation. Anticancer. Res. 2018, 38, 3223–3229. [Google Scholar] [CrossRef] [Green Version]
- Asad, S. Anti-Smoking Measures Implemented by Educational Institutions and the Prohibition of Smoking and Protection of Non-Smokers Health Ordinance, 2002. J. Pak. Med. Assoc. 2019, 69, 1700–1704. [Google Scholar] [CrossRef]
- Schliemann, D.; Su, T.T.; Paramasivam, D.; Somasundaram, S.; Tamin, N.S.B.I.; Dahlui, M.; Loh, S.Y.; Donnelly, M. The systematic cultural adaptation of a UK public health cancer awareness raising programme for Malaysia: The Be Cancer Alert Campaign. Transl. Behav. Med. 2019, 9, 1087–1099. [Google Scholar] [CrossRef] [PubMed]
- Rahman, B.; Hawas, N.; Rahman, M.M.; Rabah, A.F.; Al Kawas, S. Assessing dental students’ knowledge of oral cancer in the United Arab Emirates. Int. Dent. J. 2013, 63, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Azimi, S.; Ghorbani, Z.; Tennant, M.; Kruger, E.; Safiaghdam, H.; Rafieian, N. Population Survey of Knowledge about Oral Cancer and Related Factors in the Capital of Iran. J. Cancer Educ. 2019, 34, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Hertrampf, K.; Wenz, H.J.; Koller, M.; Wiltfang, J. Public awareness about prevention and early detection of oral cancer: A population-based study in Northern Germany. J. Cranio-Maxillofac. Surg. 2012, 40, e82–e86. [Google Scholar] [CrossRef]
- Peker, I.; Alkurt, M.T. Public awareness level of oral cancer in a group of dental patients. J. Contemp. Dent. Pract. 2010, 11, 49–56. [Google Scholar] [CrossRef]
- Tadbir, A.A.; Ebrahimi, H.; Pourshahidi, S.; Zeraatkar, M. Evaluation of levels of knowledge about etiology and symptoms of oral cancer in Southern Iran. Asian Pac. J. Cancer Prev. 2013, 14, 2217–2220. [Google Scholar] [CrossRef] [Green Version]
- Pakfetrat, A.; Falaki, F.; Esmaily, H.O.; Shabestari, S. Oral cancer knowledge among patients referred to Mashhad Dental School, Iran. Arch. Iran. Med. 2010, 13, 543–548. [Google Scholar]
- Cossellu, G.; Fedele, L.; Badaoui, B.; Angiero, F.; Farronato, G.; Monti, E.; Liverani, C.A.; Gorni, C.; Botti, S. Prevalence and concordance of oral and genital HPV in women positive for cervical HPV infection and in their sexual stable partners: An Italian screening study. PLoS ONE 2018, 13, e0205574. [Google Scholar] [CrossRef]
- Brondani, M.A.; Siqueira, A.B.; Alves, C.M.C. Exploring lay public and dental professional knowledge around HPV transmission via oral sex and oral cancer development. BMC Public Health 2019, 19, 1529. [Google Scholar] [CrossRef]
- Reddy, B.S.; Doshi, D.; Reddy, M.P.; Kulkarni, S.; Gaffar, A.; Reddy, V.R. Oral cancer awareness and knowledge among dental patients in South India. J. Cranio-Maxillofac. Surg. 2012, 40, 521–524. [Google Scholar] [CrossRef]
- Al-Maweri, S.A.; Al-Soneidar, W.A.; Dhaifullah, E.; Halboub, E.S.; Tarakji, B. Oral Cancer: Awareness and Knowledge Among Dental Patients in Riyadh. J. Cancer Educ. 2017, 32, 308–313. [Google Scholar] [CrossRef]
- Al-Maweri, S.A.; Addas, A.; Tarakji, B.; Abbas, A.; Al-Shamiri, H.M.; Alaizari, N.A.; Shugaa-Addin, B. Public awareness and knowledge of oral cancer in Yemen. Asian Pac. J. Cancer Prev. 2014, 15, 10861–10865. [Google Scholar] [CrossRef] [Green Version]
- Hassona, Y.; Sawair, F.; Matarweh, D.; Abdalhamid, A.; Thweib, D.; Scully, C. Oral Cancer Early Detection: What Do Patients Need To Know? J. Cancer Educ. 2018, 33, 865–869. [Google Scholar] [CrossRef]
- Holmstrup, P. Oral erythroplakia—What is it? Oral Dis. 2018, 24, 138–143. [Google Scholar] [CrossRef]
- Capocasale, G.; Panzarella, V.; Tozzo, P.; Mauceri, R.; Rodolico, V.; Lauritano, D.; Campisi, G. Oral verruciform xanthoma and erythroplakia associated with chronic graft-versus-host disease: A rare case report and review of the literature. BMC Res. Notes 2017, 10, 631. [Google Scholar] [CrossRef] [Green Version]
- Elango, K.J.; Anandkrishnan, N.; Suresh, A.; Iyer, S.K.; Ramaiyer, S.K.; Kuriakose, M.A. Mouth self-examination to improve oral cancer awareness and early detection in a high-risk population. Oral Oncol. 2011, 47, 620–624. [Google Scholar] [CrossRef]
- Walvekar, S.S.; Mohite, V.R.; Mohite, R.V.; Kakade, S.V. Effectiveness of self-instructional module on awareness on screening regarding breast cancer with Intelligent Breast Examination among primary schoolteachers in Karad. J. Cancer Res. Ther. 2020, 16, 139–143. [Google Scholar] [CrossRef]
- Robinson, J.K.; Perez, M.; Abou-El-Seoud, D.; Kim, K.; Brown, Z.; Liko-Hazizi, E.; Friedewald, S.M.; Kwasny, M.; Spring, B. Targeted Melanoma Screening: Risk Self-Assessment and Skin Self-Examination Education Delivered During Mammography of Women. JNCI Cancer Spectr. 2019, 3, pkz047. [Google Scholar] [CrossRef]
- Brenner, J.S.; Hergenroeder, A.C.; Kozinetz, C.A.; Kelder, S.H. Teaching testicular self-examination: Education and practices in pediatric residents. Pediatrics 2003, 111, e239–e244. [Google Scholar] [CrossRef] [Green Version]
- Hurkmans, E.; Matthys, C.; Bogaerts, A.; Scheys, L.; Devloo, K.; Seghers, J. Face-to-Face Versus Mobile Versus Blended Weight Loss Program: Randomized Clinical Trial. JMIR mHealth uHealth 2018, 6, e14. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, L.S.; Warnakulasuriya, S.; Cadilhe, S.; Sousa, D.; Trancoso, P.F.; Antunes, L.; Salazar, F.; Pacheco, J.J. Oral cancer awareness and knowledge among residents in the Oporto city, Portugal. J. Investig. Clin. Dent. 2016, 7, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Zotti, F.; Zotti, R.; Albanese, M.; Nocini, P.F.; Paganelli, C. Implementing post-orthodontic compliance among adolescents wearing removable retainers through whatsapp: A pilot study. Patient Prefer Adherence 2019, 13, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Zotti, F.; Pietrobelli, A.; Malchiodi, L.; Nocini, P.F.; Albanese, M. Apps for oral hygiene in children 4 to 7 years: Fun and effectiveness. J. Clin. Exp. Dent. 2019, 11, e795–e801. [Google Scholar] [CrossRef] [PubMed]
- Capocasale, G.; Perno, G.; Nocini, R.; Albanese, M.; Zotti, F. Role of telemedicine and smartphone for distant patient management in dentistry: The new way of triage. J. Int. Soc. Prev. Community Dent. 2020, 10, 376–378. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Existence of Knowledge | Risk Factors | Signs and Symptoms | Self-Inspection | Referral | Waiting Time | Scheduled Visits | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Smoking | Alcohol | Poor oral Hygiene | HPV | All Risk Factors | White Plaque | Red Plaque | Burning Sensation in Mouth | Dry Mouth | ||||||
| Sex | 0 | 0.844 | 0.463 | 0.014 | 0.102 | 0.903 | 0.27 | 0.707 | 0.415 | 0.706 | 0.119 | 0.581 | 0.384 | 0.034 |
| Age | 0 | 0.229 | 0.341 | 0.002 | 0.137 | 0.759 | 0.465 | 0.192 | 0.487 | 0.472 | 0.561 | 0.109 | 0.007 | 0.103 |
| North/South | 0.456 | 0.825 | 0.101 | 0.41 | 0.506 | 0.266 | 0.019 | 0.315 | 0.267 | 0.459 | 0.741 | 0.206 | 0.163 | 0.009 |
| Educational Attainment | 0 | 0.712 | 0.816 | 0.012 | 0.568 | 0.428 | 0.308 | 0.535 | 0.43 | 0.877 | 0.403 | 0.192 | 0.86 | 0.169 |
| Medical Relationship | 0 | 0.914 | 0.003 | 0.539 | 0.7 | 0.227 | 0.816 | 0.11 | 0.513 | 0.196 | 0.002 | 0.104 | 0.647 | 0.119 |
| Family OSCC | 0 | 0.945 | 0.478 | 0.031 | 0.22 | 0.909 | 0.912 | 0.608 | 0.51 | 0.754 | 0.119 | 0.07 | 0.936 | 0.081 |
| Gender | M | 144 | 28.51% |
| F | 361 | 71.49% | |
| Age | Group 1 | 316 | 71.48% |
| Group 2 | 81 | 16.03% | |
| Group 3 | 108 | 21.38% | |
| Provenance | North | 251 | 49.70% |
| South | 254 | 50.29% | |
| Educational Attainment | Junior high school | 101 | 20% |
| High school | 217 | 44.75% | |
| Graduate degree | 180 | 36.23% | |
| PhD | 7 | 1.38% | |
| Relatives with OSCC Diagnosis | Yes | 24 | 4.75%% |
| No | 481% | 95.24% | |
| Medical Relationship | Yes | 153 | 30.29% |
| No | 352 | 69.72% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nocini, R.; Capocasale, G.; Marchioni, D.; Zotti, F. A Snapshot of Knowledge about Oral Cancer in Italy: A 505 Person Survey. Int. J. Environ. Res. Public Health 2020, 17, 4889. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134889
Nocini R, Capocasale G, Marchioni D, Zotti F. A Snapshot of Knowledge about Oral Cancer in Italy: A 505 Person Survey. International Journal of Environmental Research and Public Health. 2020; 17(13):4889. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134889
Chicago/Turabian StyleNocini, Riccardo, Giorgia Capocasale, Daniele Marchioni, and Francesca Zotti. 2020. "A Snapshot of Knowledge about Oral Cancer in Italy: A 505 Person Survey" International Journal of Environmental Research and Public Health 17, no. 13: 4889. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134889