Flow-Mediated Dilation in Healthy Young Individuals Is Impaired after a Single Resistance Exercise Session

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. Resistance Exercise Protocol
2.4. Flow-Mediated Dilation Assessment
2.5. Statistical Analysis
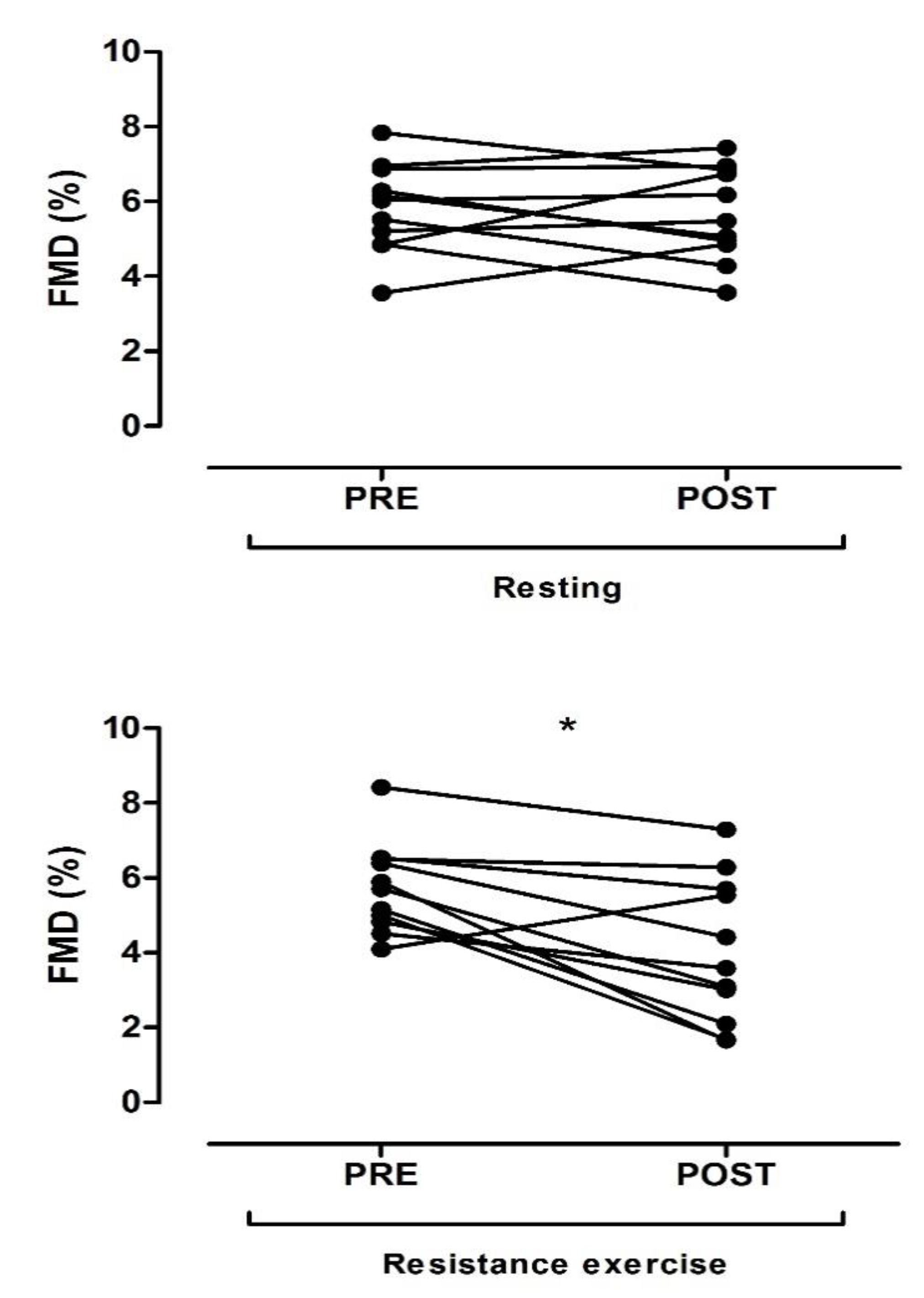
3. Results
4. Discussion
Experimental Consideration
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Green, D.J.; Jones, H.; Thijssen, D.; Cable, N.T.; Atkinson, G. Flow-mediated dilation and cardiovascular event prediction: Does nitric oxide matter? Hypertension 2011, 57, 363–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLay, K.M.; Fontana, F.Y.; Nederveen, J.P.; Guida, F.F.; Paterson, D.H.; Pogliaghi, S.; Murias, J.M. Vascular responsiveness determined by near-infrared spectroscopy measures of oxygen saturation. Exp. Physiol. 2016, 101, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Dawson, E.A.; Groenewoud, H.M.; Jones, H.; Thijssen, D.H. Is flow-mediated dilation nitric oxide mediated? A meta-analysis. Hypertension 2014, 63, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Green, D.J.; Walsh, J.H.; Maiorana, A.; Best, M.J.; Taylor, R.R.; O’Driscoll, J.G. Exercise-induced improvement in endothelial dysfunction is not mediated by changes in CV risk factors: Pooled analysis of diverse patient populations. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H2679–H2687. [Google Scholar] [CrossRef] [Green Version]
- MacDougall, J.D.; Tuxen, D.; Sale, D.G.; Moroz, J.R.; Sutton, J.R. Arterial blood pressure response to heavy resistance exercise. J. Appl. Physiol. 1985, 58, 785–790. [Google Scholar] [CrossRef] [Green Version]
- Tinken, T.M.; Thijssen, D.H.; Hopkins, N.; Dawson, E.A.; Cable, N.T.; Green, D.J. Shear stress mediates endothelial adaptations to exercise training in humans. Hypertension 2010, 55, 312–318. [Google Scholar] [CrossRef] [Green Version]
- Green, D.J.; Rowley, N.; Spence, A.; Carter, H.; Whyte, G.; George, K.; Naylor, L.H.; Cable, N.T.; Dawson, E.A.; JThijssen, D.H. Why isn’t flow-mediated dilation enhanced in athletes? Med. Sci. Sports Exerc. 2013, 2013. 45, 75–82. [Google Scholar] [CrossRef]
- Dawson, E.A.; Green, D.J.; Cable, N.T.; Thijssen, D.H.J. Effects of acute exercise on flow-mediated dilatation in healthy humans. J. Appl. Physiol. 2013, 115, 1589–1598. [Google Scholar] [CrossRef]
- Pedralli, M.L.; Marschner, R.A.; Kollet, D.P.; Neto, S.G.; Eibel, B.; Tanaka, H.; Lehnen, A.M. Different exercise training modalities produce similar endothelial function improvements in individuals with prehypertension or hypertension: A randomized clinical trial Exercise, endothelium and blood pressure. Sci. Rep. 2020, 10, 7628. [Google Scholar] [CrossRef] [PubMed]
- Olson, T.P.; Dengel, D.R.; Leon, A.S.; Schmitz, K.H. Moderate resistance training and vascular health in overweight women. Med. Sci. Sports Exerc. 2006, 38, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Cosio-Lima, L.M.; Thompson, P.D.; Reynolds, K.L.; Headley, S.A.; Winter, C.R.; Manos, T.; Lagasse, M.A.; Todorovich, J.R.; Germain, M. The acute effect of aerobic exercise on brachial artery endothelial function in renal transplant recipients. Prev. Cardiol. 2006, 9, 211–214. [Google Scholar] [CrossRef] [Green Version]
- Varady, K.A.; Bhutani, S.; Church, E.C.; Phillips, S.A. Adipokine responses to acute resistance exercise in trained and untrained men. Med. Sci. Sports Exerc. 2010, 42, 456–462. [Google Scholar] [CrossRef]
- Phillips, S.A.; Das, E.; Wang, J.; Pritchard, K.; Gutterman, D.D. Resistance and aerobic exercise protects against acute endothelial impairment induced by a single exposure to hypertension during exertion. J. Appl. Physiol. 2011, 110, 1013–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvestro, A.; Scopacasa, F.; Oliva, G.; de Cristofaro, T.; Luliano, L.; Brevetti, G. Vitamin C prevents endothelial dysfunction induced by acute exercise in patients with intermittent claudication. Atherosclerosis 2002, 165, 277–283. [Google Scholar] [CrossRef]
- Gonzales, J.U.; Thompson, B.C.; Thistlethwaite, J.R.; Scheuermann, B.W. Association between exercise hemodynamics and changes in local vascular function following acute exercise. Appl. Physiol. Nutr. Metab. 2011, 36, 137–144. [Google Scholar] [CrossRef]
- Sugiura, Y.; Hatanaka, Y.; Arai, T.; Sakurai, H.; Kanada, Y. Estimations of one repetition maximum and isometric peak torque in knee extension based on the relationship between force and velocity. J. Strength Cond. Res. 2016, 30, 980–988. [Google Scholar] [CrossRef]
- Oliveira, G.V.; Volino-Souza, M.; Leitão, R.; Pinheiro, V.; Alvares, T.S. Is flow-mediated dilatation associated with near-infrared spectroscopy-derived magnitude of muscle O2 desaturation in healthy young and individuals at risk for cardiovascular disease? Microvasc. Res. 2020, 129, 103967. [Google Scholar] [CrossRef]
- Buchanan, C.E.; Kadlec, A.O.; Hoch, A.Z.; Gutterman, D.D.; Durand, M.J. Hypertension during weight lifting reduces flow-mediated dilation in nonathletes. Med. Sci. Sports Exerc. 2017, 49, 669–675. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.; Masuhara, M.; Ikuta, K. Relationship between plasma endothelin-1 concentration and cardiovascular responses during high-intensity eccentric and concentric exercise. Clin. Physiol. Funct. Imaging 2008, 28, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Bilfinger, T.V.; Stefano, G.B. Human aortocoronary grafts and nitric oxide release: Relationship to pulsatile pressure. Ann. Thorac. Surg. 2000, 69, 480–485. [Google Scholar] [CrossRef]
- Lamping, K.G.; Dole, W.P. Acute hypertension selectively potentiates constrictor responses of large coronary arteries to serotonin by altering endothelial function in vivo. Circ. Res. 1987, 61, 904–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padilla, J.; Harris, R.A.; Wallace, J.P. Can the measurement of brachial artery flow-mediated dilation be applied to the acute exercise model? Cardiovasc. Ultrasound 2007, 5, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, B.E.; Proffit, M.; Gifford, J.R. Vascular function is related to blood flow during high-intensity, but not low-intensity, knee extension exercise. J. Appl. Physiol. 2020, 128, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Demographics | Mean ± SD |
|---|---|
| Number of participants (female) | 11 (3) |
| Age (years) | 24.36 ± 5.14 |
| Weight (kg) | 76.23 ± 8.10 |
| Height (cm) | 171.27 ± 7.50 |
| BMI (kg/m2) | 26.03 ± 2.74 |
| Biochemistry | |
| Glucose (mg/dL) | 86.28 ± 8.91 |
| Total cholesterol (mg/dL) | 158.18 ± 40.5 |
| LDL cholesterol (mg/dL) | 98.09 ± 47.03 |
| HDL cholesterol (mg/dL) | 38.66 ± 11.81 |
| Triglycerides (mg/dL) | 108.66 ± 39.39 |
| Clinical measures | |
| SBP (mm Hg) | 118.00 ± 11.06 |
| DBP (mm Hg) | 78.27 ± 6.66 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira, G.V.; Mendes Cordeiro, E.; Volino-Souza, M.; Rezende, C.; Conte-Junior, C.A.; Silveira Alvares, T. Flow-Mediated Dilation in Healthy Young Individuals Is Impaired after a Single Resistance Exercise Session. Int. J. Environ. Res. Public Health 2020, 17, 5194. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145194
de Oliveira GV, Mendes Cordeiro E, Volino-Souza M, Rezende C, Conte-Junior CA, Silveira Alvares T. Flow-Mediated Dilation in Healthy Young Individuals Is Impaired after a Single Resistance Exercise Session. International Journal of Environmental Research and Public Health. 2020; 17(14):5194. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145194
Chicago/Turabian Stylede Oliveira, Gustavo Vieira, Elisaldo Mendes Cordeiro, Mônica Volino-Souza, Cristina Rezende, Carlos Adam Conte-Junior, and Thiago Silveira Alvares. 2020. "Flow-Mediated Dilation in Healthy Young Individuals Is Impaired after a Single Resistance Exercise Session" International Journal of Environmental Research and Public Health 17, no. 14: 5194. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145194