Development and Validation of a Rating Scale of Pain Expression during Childbirth (ESVADOPA)

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Development of the Scale
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Reliability
3.2. Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bergh, I.; Söderlund, T.; Vinterskog, L.; Mårtensson, L. Reliability and validity of the acceptance symptom assessment scale in assessing labour pain. Midwifery 2012, 28, e684–e688. [Google Scholar] [CrossRef] [PubMed]
- Gibbins, J.; Thomson, A.M. Women’s expectations and experiences of childbirth. Midwifery 2001, 17, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Thomson, G.; Feeley, C.; Moran, V.H.; Downe, S.; Oladapo, O.T. Women’s experiences of pharmacological and non-pharmacological pain relief methods for labour and childbirth: A qualitative systematic review. Reprod. Health 2019, 16, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacassie, Q.H. Dolor y Embarazo. Rev. Méd. Clín. Condes 2014, 25, 641–650. [Google Scholar] [CrossRef] [Green Version]
- Demšar, K.; Svetina, M.; Verdenik, I.; Tul, N.; Blickstein, I.; Velikonja, V.G. Tokophobia (fear of childbirth): Prevalence and risk factors. J. Périnat. Med. 2018, 46, 151–154. [Google Scholar] [CrossRef]
- Margarita, A.M.; Jiménez, Y.Y.T.; Ávila, J.F.P. El proceso de parto cultural, una necesidad. Cult. Cuid. 2018, 15, 23–37. [Google Scholar] [CrossRef] [Green Version]
- Cadenas, M.D.M.S.; Del Pino, F.J.P. Variabilidad en la vivencia del parto y su implicación en los cuidados de enfermería. Cult. Cuid. 2018, 22, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Taheri, M.; Takian, A.; Taghizadeh, Z.; Jafari, N.; Sarafraz, N. Creating a positive perception of childbirth experience: Systematic review and meta-analysis of prenatal and intrapartum interventions. Reprod. Health 2018, 15, 73. [Google Scholar] [CrossRef]
- Mallén-Pérez, L.; Juvé-Udina, E.; Roé-Justiniano, M.T. Domènech-Farrarons, Matronas Prof. In A Dolor de Parto: Análisis Del Concepto; Ediciones Mayo, S.A.: Barcelona, Spain, 2015. [Google Scholar]
- Ternström, E.; Hildingsson, I.; Haines, H.; Rubertsson, C. Higher prevalence of childbirth related fear in foreign born pregnant women—Findings from a community sample in Sweden. Midwifery 2015, 31, 445–450. [Google Scholar] [CrossRef]
- Molina-Fernández, I.; Rubio-Rico, L.; Roca-Biosca, A.; Jimenez-Herrera, M.; Flor-López, M.; Sirgo, A. Análisis de las emociones negativas generadas ante el dolor de parto, en mujeres atendidas en un hospital público de Tarragona. MUSAS 2016, 1, 52–63. [Google Scholar] [CrossRef]
- O’Connell, M.A.; Khashan, A.S.; Leahy-Warren, P. Women’s experiences of interventions for fear of childbirth in the perinatal period: A meta-synthesis of qualitative research evidence. Women Birth 2020. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, V.M.; Nazarzadeh, M.; Jahanfar, S. Interventions for reducing fear of childbirth: A systematic review and meta-analysis of clinical trials. Women Birth 2018, 31, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Teles, L.M.R.; Américo, C.F.; Oriá, M.O.B.; Vasconcelos, C.T.M.; Brüggemann, O.M.; Damasceno, A.K.D.C. Efficacy of an educational manual for childbirth companions: Pilot study of a randomized clinical trial. Rev. Lat. -Am. Enferm. 2018, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, L.E.; Whitburn, L.; Davey, M.-A.; Small, R. Assessment of pain associated with childbirth: Women׳s perspectives, preferences and solutions. Midwifery 2015, 31, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Sen, G.; Reddy, B.; Iyer, A.; Heidari, S. Addressing disrespect and abuse during childbirth in facilities. Reprod. Health Matters 2018, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Escalas de Evaluación de Dolor y Protocolo de Analgesia en Terapia Intensiva. Available online: https://www.sati.org.ar/files/kinesio/monos/MONOGRAFIA%20Dolor%20-%20Clarett.pdf. (accessed on 7 August 2020).
- Herrero, M.T.V.; Bueno, S.D.; Moyá, F.B.; De La Torre, M.V.R.I.; García, L.C. Valoración del dolor. Revisión Comparativa de Escalas y Cuestionarios. Rev. Soc. Esp. Dolor 2018, 5, 228–236. [Google Scholar] [CrossRef]
- Carvalho, B.; Mhyre, J.M. Moving beyond the 0–10 scale for labor pain measurement. Anesth. Analg. 2016, 123, 1351–1353. [Google Scholar] [CrossRef]
- Wewers, M.E.; Lowe, N.K. A critical review of visual analogue scales in the measurement of clinical phenomena. Res. Nurs. Health 1990, 13, 227–236. [Google Scholar] [CrossRef]
- Dick, J.A.; Newport, A.; Pattison, D.; Sun, W.; Kenaszchuk, C.; Dennis, C.-L. Development, psychometric assessment, and predictive validity of the comprehensive breastfeeding knowledge scale. Midwifery 2020, 83, 102642. [Google Scholar] [CrossRef]
- Marco, I.L.; Muñoz, M.S.; Ruiz, T.F.; Sánchez, A.L.; Pérez, A.R.; Santos, I.M. Validación de la Escala de Conductas Indicadoras de Dolor para valorar el dolor en pacientes críticos, no comunicativos y sometidos a ventilación mecánica: Resultados del proyecto ESCID. Enferm. Intensiva 2011, 22, 3–12. [Google Scholar] [CrossRef]
- Marques, G.M.; Nascimento, D.Z.D.; Trevisol, D.J.; Iser, B.P. Instruments measuring pregnant women’s expectations of labor and childbirth: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Boil. 2020, 246, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, S.; Chambers, C.T.; Rosen, N.O. Expression of pain behaviors and perceived partner responses in individuals with chronic pain. Clin. J. Pain 2018, 34, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Pardo, C.; Muñoz, T.; Chamorro, C. Monitorización del dolor. Recomendaciones del grupo de trabajo de analgesia y sedación de la SEMICYUC. Med. Intensiva 2006, 30, 379–385. [Google Scholar] [CrossRef]
- Goberna-Tricas, J.; Biurrun-Garrido, A. El alivio del dolor en el parto. Empoderamiento y vulnerabilidad de las mujeres en la toma de decisiones. Estudio cualitativo. MUSAS 2020, 5, 79–97. [Google Scholar] [CrossRef] [Green Version]
- Junge, C.; Von Soest, T.; Weidner, K.; Seidler, A.; Eberhard-Gran, M.; Garthus-Niegel, S. Labor pain in women with and without severe fear of childbirth: A population-based, longitudinal study. Birth 2018, 45, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, C.; Hessman, E.; Sjöblom, H.; Dencker, A.; Jangsten, E.; Mollberg, M.; Patel, H.; Lundin, C.S.; Wigert, H.; Begley, C.M. Definitions, measurements and prevalence of fear of childbirth: A systematic review. BMC Pregnancy Childbirth 2018, 18, 28. [Google Scholar] [CrossRef]
- Oviedo, H.C.; Campo-Arias, A. Aproximación al uso del coeficiente alfa de Cronbach. Rev. Colomb. Psiq. 2005, 34, 572–580. [Google Scholar]
- Penfield, R.D.; Giacobbi, J.P.R. Applying a score confidence interval to Aiken’s item content-relevance index. Meas. Phys. Educ. Exerc. Sci. 2004, 8, 213–225. [Google Scholar] [CrossRef]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernández, A.; Tomás, I. El análisis factorial exploratorio de los ítems: Una guía práctica, revisada y actualizada. An. Psicol. 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- Lacave-Rodero, C.; Molina-Díaz, A.I.; Fernández-Guerrero, M.; Redondo-Duque, M.A. Análisis de la fiabilidad y validez de un cuestionario docente. ReVisión 2016, 9, 136–143. [Google Scholar]
- Cordón, J.R. Analyzing V Aiken’s Content Validity Using Score Method with Spreadsheets; Universidad de Cádiz: Cádiz, España, 2015. [Google Scholar]
- Aiken, L.R. Content validity and reliability of single items or questionnaires. Educ. Psychol. Meas. 1980, 40, 955–959. [Google Scholar] [CrossRef]
- Pérez-Escoda, N.; Bisquerra, R.; Filella, G.; Soldevila-Benet, A. Construction of the emotional development questionnaire for adults (QDE-A). Rev. Esp. Orientac. Psicopedag. 2010, 21, 367–379. [Google Scholar]
- González-Escalada, J.R.; Camba, A.; Muriel, C.; Rodríguez, M.; Contreras, D.; de Barutell, C. Validación del índice de Lattinen para la evaluación del paciente con dolor crónico. Rev. Soc. Esp. Dolor 2012, 19, 181–188. [Google Scholar]
- Cortés-Reyes, É.; Rubio-Romero, J.A.; Gaitán-Duarte, H. Métodos estadísticos de evaluación de la concordancia y la reproducibilidad de pruebas diagnósticas. Rev. Colomb. Obstet. Ginecol. 2010, 61, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Angle, P.; Kurtz-Landy, C.; Djordjevic, J.; Barrett, J.; Kibbe, A.; Sriparamananthan, S.; Lee, Y.; Hamata, L.; Kiss, A. The Angle Labor Pain Questionnaire. Clin. J. Pain 2017, 33, 132–141. [Google Scholar] [CrossRef]
- Carvajal, A.; Centeno, C.; Watson, R.; Martinez, M.; Rubiales, A.S. ¿Cómo validar un instrumento de medida de la salud? An. Sist. Sanit. Navar. 2011, 34, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Luján-Tangarife, J.A.; Cardona-Arias, J.A. Construcción y validación de escalas de medición en salud: Revisión de propiedades psicométricas. Arch. Med. 2015, 11, 1. [Google Scholar] [CrossRef]
- Pedrosa, I.; Suárez-Álvarez, J.; García-Cueto, E. Evidencias sobre la Validez de Contenido: Avances Teóricos y Métodos para su Estimación. Acción Psicol. 2014, 10, 3. [Google Scholar] [CrossRef]
- Fernández-Gómez, E.; Martín-Salvador, A.; Luque-Vara, T.; Sánchez-Ojeda, M.A.; Navarro-Prado, S.; Enrique-Mirón, C. Content validation through expert judgement of an instrument on the nutritional knowledge, beliefs, and habits of pregnant women. Nutrition 2020, 12, 1136. [Google Scholar] [CrossRef]
- Urrutia, M.; Barrios, S.; Gutiérrez, M.; Mayorga, M. Métodos óptimos para determinar validez de contenido. Educ. Méd. Super. 2014, 28, 547–558. [Google Scholar]
- Varela-Ruiz, M.; Díaz-Bravo, V.; García-Durán, R. Descripción y usos del método Delphi en investigaciones del área de la salud. Metodol. Investig. Educ. Méd. 2012, 1, 90–95. [Google Scholar]
- Garcia-Martin, A.; Antúnez, A.; Ibáñez, S.J. Análisis del proceso formativo en jugadores expertos: Validación de instrumento / Analysis of expert players’ training process: Validation of tools. Rev. Int. Med. Cienc. Act. Fís. Deporte 2016, 61, 157–182. [Google Scholar] [CrossRef] [Green Version]
- Hyrkäs, K.; Appelqvist-Schmidlechner, K.; Oksa, L. Validating an instrument for clinical supervision using an expert panel. Int. J. Nurs. Stud. 2003, 40, 619–625. [Google Scholar] [CrossRef]
- Jiménez, J.; Salazar, W.; Morera, M. Diseño y validación de un instrumento para la evaluación de patrones básicos de movimiento. Eur. J. Hum. Mov. 2013, 31, 87–97. [Google Scholar]
- Juárez-Hernández, L.G.; Tobón, S. Análisis de los elementos implícitos en la validación de contenido de un instrumento de investigación. Rev. Espac. 2018, 39, 23. [Google Scholar]
- Ferrer-Peña, R.; Gil-Martínez, A.; Pardo-Montero, J.; Jiménez-Penick, V.; Izquierdo, T.G.; La Touche, R. Adaptation and validation of the Spanish version of the graded chronic pain scale. Reumatol. Clín. (Engl. Ed.) 2016, 12, 130–138. [Google Scholar] [CrossRef]
- Carrasco, J.A.P.; Rodríguez-Bouza, M.; Casal-Sánchez, M.-D.-M.; De-La-Fuente-Rodríguez, J.-M.; Puerta-Córdoba, A.; Rodríguez-Ruiz, H.-J.; Sánchez-Almagro, C.-P.; Failde, I. Development and validation of a safety scale perceived by the witness of prehospital emergency care. J. Patient Saf. 2019, 1–7. [Google Scholar] [CrossRef]
- Francesco, S.; Melania, L.; Lucrezia, B.; Antonella, G.; Concetta, I.; Giulia, V.; Giovanna, A.; Leopoldo, S. A first contribution to the validation of the Italian version of the behavioral pain scale in sedated, intubated, and mechanically ventilated paediatric patients. Acta Bio-Med. Atenei Parm. 2018, 89, 19–24. [Google Scholar] [CrossRef]


{kind=link}
| Item | Sub-Item: Score/Meaning | References | Articles |
|---|---|---|---|
| FACIAL MUSCLES (FM) | 0. Relaxed during the entire contraction. 1. Relaxed with slight facial tightening during most of the contraction. 2. Frowning/grimacing/clenched teeth only during the peak of contraction. 3. Frowning/grimacing/clenched teeth during the entire contraction. | [3,19,21,22,23,24,25] |
|
| BODY RESPONSE (BR) | 0. Relaxed during the entire contraction. 1. Relaxed with slight contraction of hands, arms, and/or toes and legs during most of the contraction. 2. Increased: flexion of the fingers, arms, and/or toes and legs during the peak of contraction. 3. Increased: flexion of fingers, arms, and/or legs during the entire contraction. | [3,21,23,24,25] |
|
| VERBAL RESPONSE (VR) | 0. In silence or fluid conversation during the entire contraction. 1. Mild moans and sobs during most of the contraction. 2. Shouts, complains, grunts, and sobs at the peak of contraction. 3. Shouts, complains, grunts, and sobs during the entire contraction. | [3,21,23,24,25] |
|
| RESTLESSNESS (R) | 0. Calm, relaxed, normal movements during the entire contraction. 1. Calm, relaxed, slight movements indicating restlessness during most of the contraction. 2. Occasional movements indicating restlessness and/or changes in position at the peak of contraction. 3. Continuous movements indicating restlessness and/or changes in position during the entire contraction. | [3,8,21,23,25,26,27] |
|
| ABILITY TO RELAX (AR) | 0. Relaxed and calm throughout the contraction. 1. Relaxes with the touch and/or voice of the companion or health professional. 2. Begins to present difficulties with relaxing with the touch and/or voice of the companion or health professional. 3. Rejects the touch and/or the voice of the companion or health professional. | [3,8,21,23,25,26,27] |
|
| VEGETATIVE SYMPTOMS (VS) | 0. No vegetative symptoms. 1. Sweating and/or nausea. 2. Sweating, nausea, and/or dizziness. 3. Sweating, nausea, vomiting, dizziness, increased blood pressure (BP), tachycardia, and/or dilated pupils. | [5,10,13,23,25,27,28] |
|
| Mean | Standard Deviation | Corrected Total Correlation of Elements (HIc) | Cronbach’s Alpha if the Element Were Eliminated | Component 1 | Component 2 | |
|---|---|---|---|---|---|---|
| FM | 2.15 | 0.621 | 0.593 | 0.738 | 0.257 | |
| BR | 2.22 | 0.599 | 0.562 | 0.746 | 0.296 | |
| VR | 1.82 | 0.819 | 0.681 | 0.710 | 0.293 | |
| R | 2.29 | 0.685 | 0.660 | 0.718 | 0.267 | |
| AR | 1.76 | 0.637 | 0.564 | 0.744 | 0.372 | |
| VS | 1.00 | 0.638 | 0.178 | 0.828 | 0.819 |
| KMO and Bartlett’s Test | ||
|---|---|---|
| KMO Measure of Sampling Adequacy | 0.796 | |
| Bartlett’s sphericity test | Approx. chi-squared | 99.474 |
| df | 15 | |
| Sig. | 0.000 | |
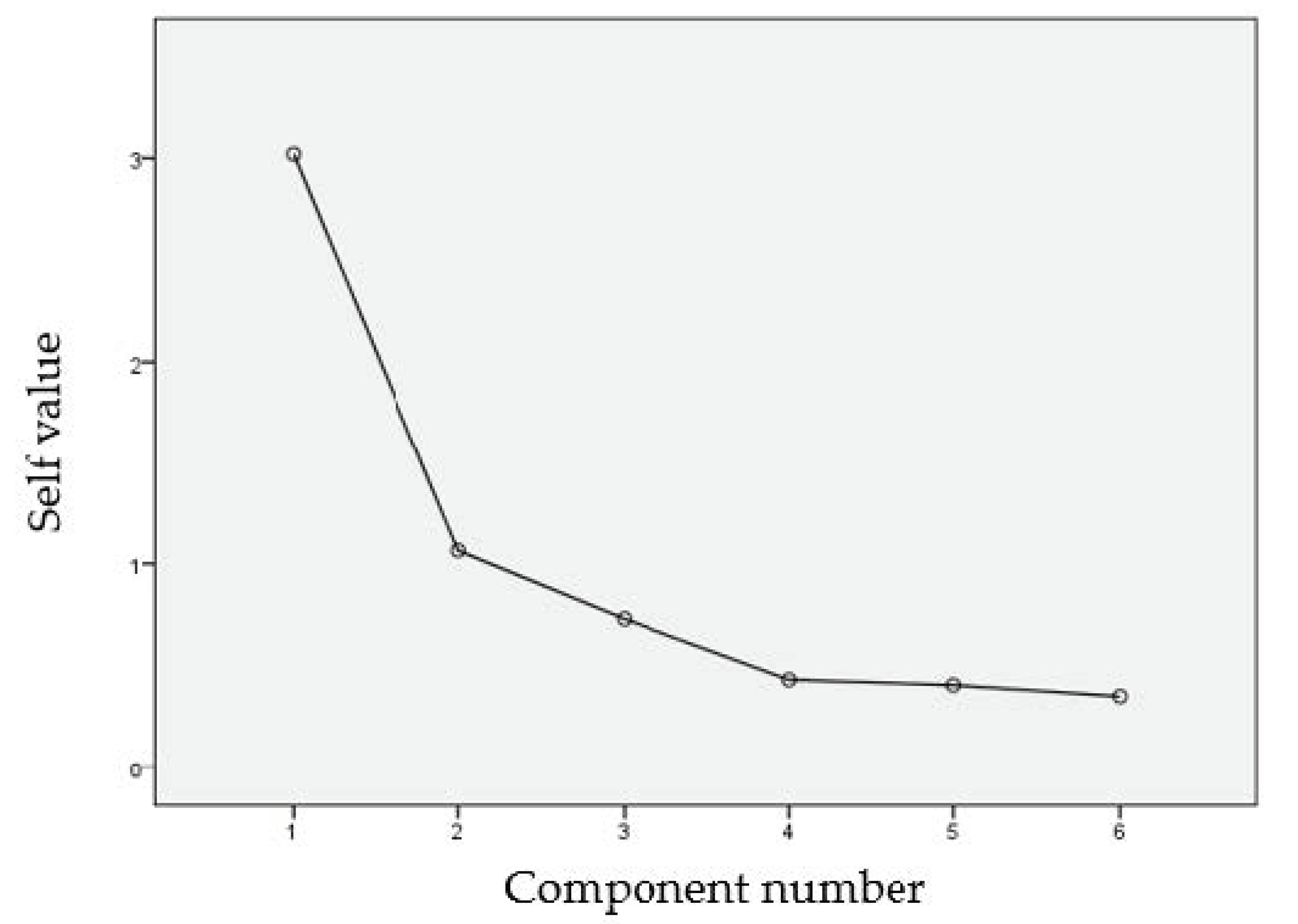
| Component | Initial Eigenvalues | Extraction Sums of Squared Loadings | Rotation Sums of Squared Loadings | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Variance % | Cumulative % | Total | Variance % | Cumulative % | Total | Variance % | Cumulative % | |
| 1 | 3.020 | 50.330 | 50.330 | 3.020 | 50.330 | 50.330 | 2.858 | 47.634 | 47.634 |
| 2 | 1.065 | 17.752 | 68.083 | 1.065 | 17.752 | 68.083 | 1.227 | 20.449 | 68.083 |
| 3 | 0.730 | 12.161 | 80.244 | ||||||
| 4 | 0.431 | 7.186 | 87.431 | ||||||
| 5 | 0.405 | 6.749 | 94.180 | ||||||
| 6 | 0.349 | 5.820 | 100.000 | ||||||
| EVA | ESVADOPA | ||
|---|---|---|---|
| VAS | Pearson correlation | 1 | 0.641 ** |
| Sig. (two-tailed) | 0.000 | ||
| ESVADOPA | Pearson correlation | 0.641 ** | 1 |
| Sig. (two-tailed) | 0.000 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Prado, S.; Sánchez-Ojeda, M.A.; Martín-Salvador, A.; Luque-Vara, T.; Fernández-Gómez, E.; Caro-Morán, E. Development and Validation of a Rating Scale of Pain Expression during Childbirth (ESVADOPA). Int. J. Environ. Res. Public Health 2020, 17, 5826. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165826
Navarro-Prado S, Sánchez-Ojeda MA, Martín-Salvador A, Luque-Vara T, Fernández-Gómez E, Caro-Morán E. Development and Validation of a Rating Scale of Pain Expression during Childbirth (ESVADOPA). International Journal of Environmental Research and Public Health. 2020; 17(16):5826. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165826
Chicago/Turabian StyleNavarro-Prado, Silvia, María Angustias Sánchez-Ojeda, Adelina Martín-Salvador, Trinidad Luque-Vara, Elisabet Fernández-Gómez, and Elena Caro-Morán. 2020. "Development and Validation of a Rating Scale of Pain Expression during Childbirth (ESVADOPA)" International Journal of Environmental Research and Public Health 17, no. 16: 5826. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165826