FODMAP Intake in Spanish Population: Open Approach for Risk Assessment

 , , , , , , and
, , , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Sample and Design
2.2. Dietary Assessment
2.3. Total Fructan Analysis
2.4. Determination of FODMAP Daily Intake
2.5. Determination of the Contribution of Main Risky Foods to Fiber and Micronutrient Daily Intake
2.6. Statistics
3. Results
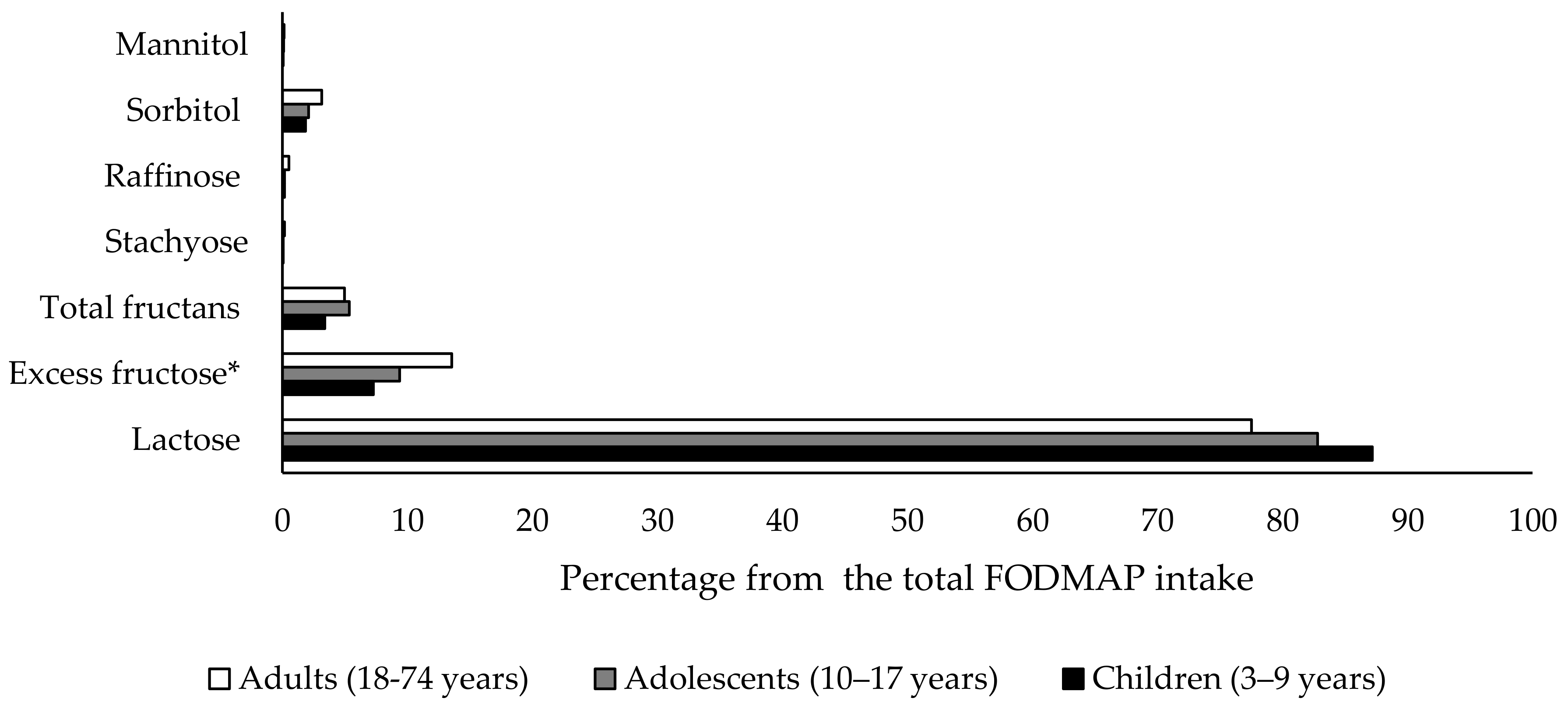
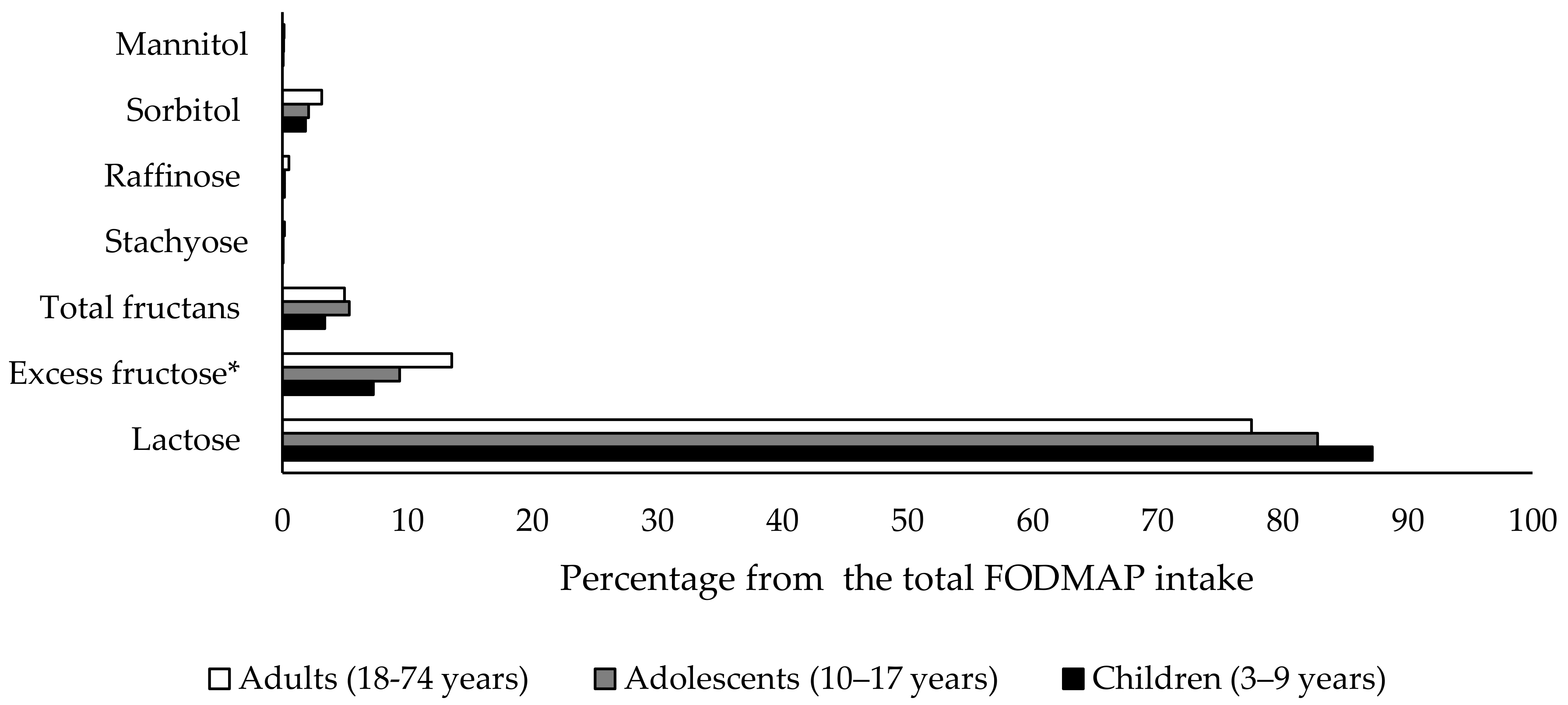
3.1. FODMAP Consumption of Spanish Children, Adolescents and Adult Population
3.2. FODMAP-Risky Foods among Spanish Children, Adolescents and Adult Population
3.3. Fiber and Micronutrients’ Potential Deficiency Risk in a Low-FODMAP Diet Approximation
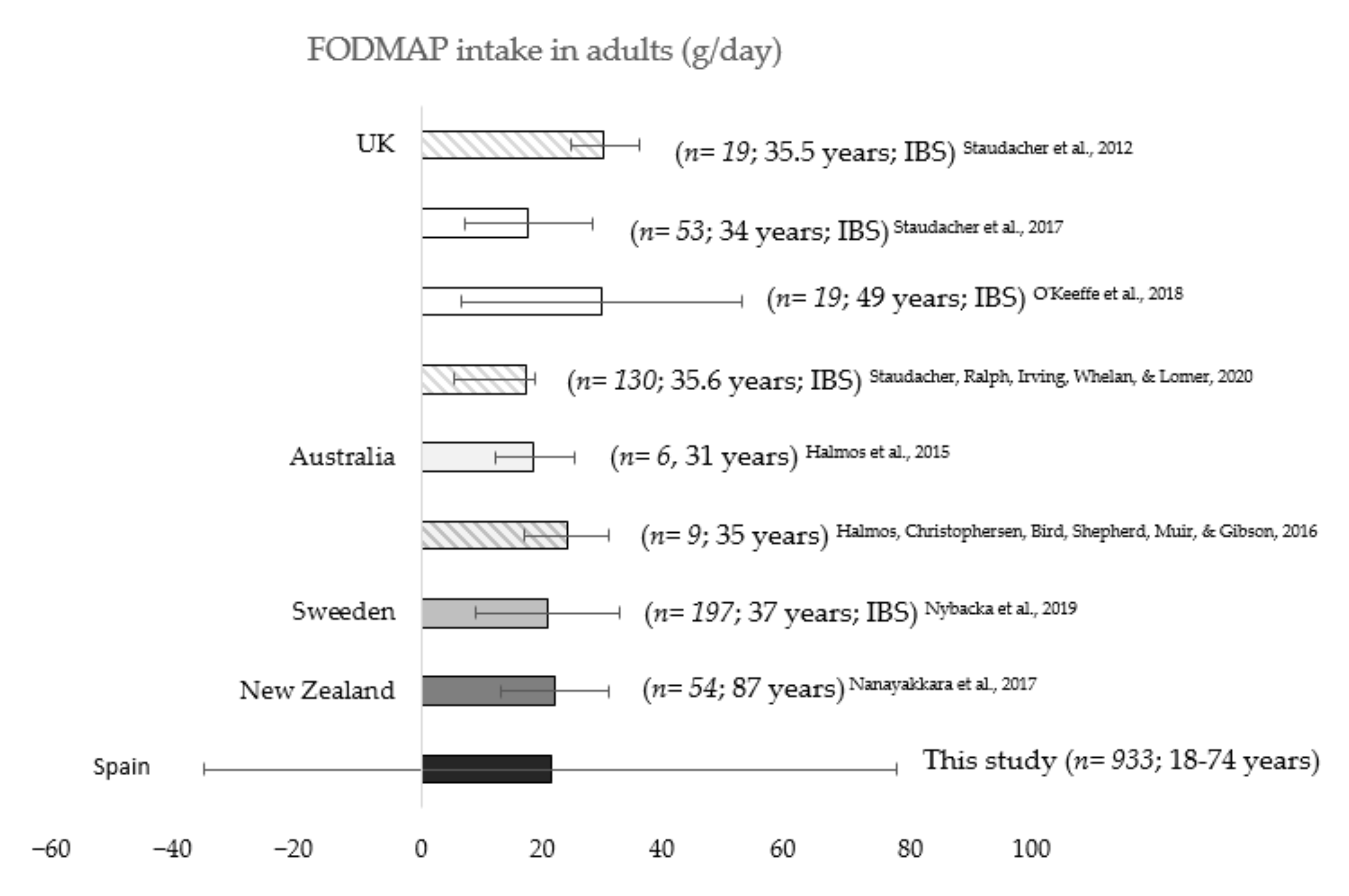
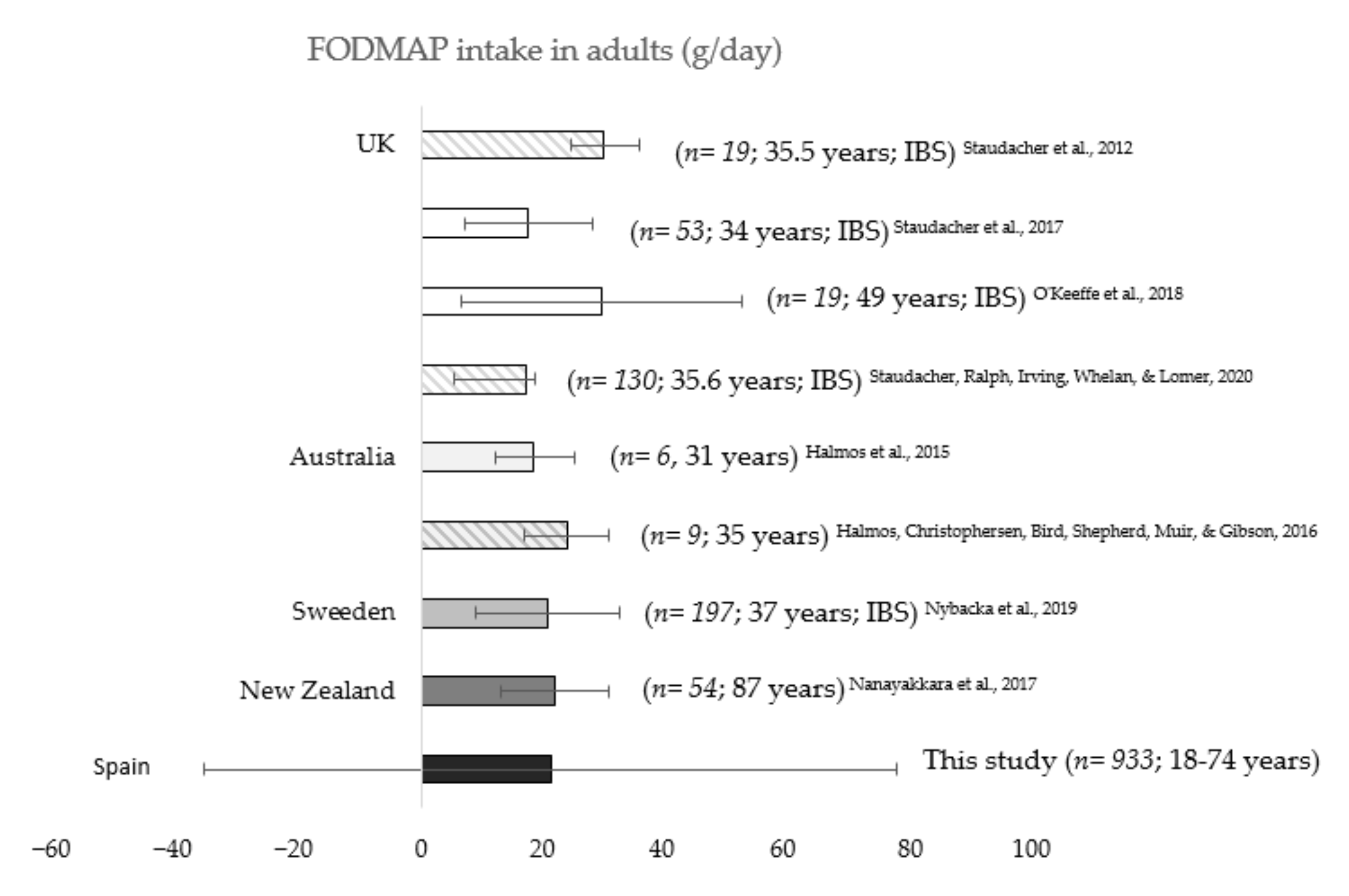
3.4. Total FODMAP Consumption in Other Countries
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Giorgio, R.; Volta, U.; Gibson, P.R. Sensitivity to wheat, gluten and FODMAPs in IBS: Facts or fiction? Gut 2016, 65, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, H.M. Nutritional, microbiological and psychosocial implications of the low FODMAP diet. J. Gastroenterol. Hepatol. 2017, 32, 16–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, S.R.; Lindsay, J.O.; Fromentin, S.; Stagg, A.J.; McCarthy, N.E.; Galleron, N.; Ibraim, S.B.; Roume, H.; Levenez, F.; Pons, N.; et al. Effects of low FODMAP diet on symptoms, fecal microbiome, and markers of inflammation in patients with quiescent inflammatory bowel disease in a randomized trial. Gastroenterology 2020, 158, 176–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrett, J.S.; Gearry, R.B.; Muir, J.G.; Irving, P.M.; Rose, R.; Rosella, O.; Haines, M.L.; Shepherd, S.J.; Gibson, P.R. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment. Pharmacol. Ther. 2010, 31, 874–882. [Google Scholar] [CrossRef]
- Van Tilburg, M.A.; Felix, C.T. Diet and functional abdominal pain in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Skodje, G.I.; Minelle, I.H.; Rolfsen, K.L.; Iacovou, M.; Lundin, K.E.A.; Veierød, M.B.; Henriksen, C. Dietary and symptom assessment in adults with self-reported non-coeliac gluten sensitivity. Clin. Nutr. ESPEN 2019, 31, 88–94. [Google Scholar] [CrossRef]
- Halmos, E.P.; Christophersen, C.T.; Bird, A.R.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. Diets that differ in their FODMAP content alter the colonic luminal microenvironment. Gut 2015, 64, 93–100. [Google Scholar] [CrossRef]
- Whelan, K.; Martin, L.D.; Staudacher, H.M.; Lomer, M.C.E. The low FODMAP diet in the management of irritable bowel syndrome: An evidence-based review of FODMAP restriction, reintroduction and personalisation in clinical practice. J. Hum. Nutr. Diet. 2018, 31, 239–255. [Google Scholar] [CrossRef] [Green Version]
- Hill, P.; Muir, J.G.; Gibson, P.R. Controversies and recent developments of the low-FODMAP diet. Gastroenterol. Hepatol. 2017, 13, 36–45. [Google Scholar]
- Castro, M.L.B.; Arnal, I.R.; Romero, R.G.; Martínez, G.R.; Sainz, E.U. Implementationof a low FODMAP dietforfunctional abdominal pain. An. Pediatr. 2019, 90, 180–186. [Google Scholar] [CrossRef]
- Chitkara, D.K.; Rawat, D.J.; Talley, N.J. The epidemiology of childhood recurrent abdominal pain in Western countries: A systematic review. Am. J. Gastroenterol. 2005, 100, 1868–1875. [Google Scholar] [CrossRef] [PubMed]
- Chumpitazi, B.P.; Cope, J.L.; Hollister, E.B.; Tsai, C.M.; McMeans, A.R.; Luna, R.A.; Versalovic, J.; Shulman, R.J. Randomised clinical trial: Gut microbiome biomarkers are associated with clinical response to a low FODMAP diet in children with the irritable bowel syndrome. Aliment. Pharmacol. Ther. 2015, 42, 418–427. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. The EFSA Comprehensive European Food Consumption Database. Available online: https://www.efsa.europa.eu/en/food-consumption/comprehensive-database (accessed on 14 July 2020).
- European Food Safety Authority. General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA J. 2009, 7, 1435. [Google Scholar] [CrossRef]
- Suarez, V.M.; Mañas, J.R.; Fernández, R.S.; de Dios, T.R. Spanish national dietary survey on children and adolescents. EFSA Supporting Publ. 2015, 12, 900E. [Google Scholar] [CrossRef] [Green Version]
- Marcos, S.V.; Rubio, M.J.; Sanchidrián, F.R.; de Robledo, D. Spanish national dietary survey in adults, elderly and pregnant women. EFSA Supporting Publ. 2016, 13, 1053E. [Google Scholar] [CrossRef] [Green Version]
- Varney, J.; Barrett, J.; Scarlata, K.; Catsos, P.; Gibson, P.R.; Muir, J.G. FODMAPs: Food composition, defining cutoff values and international application. J. Gastroenterol. Hepatol. 2017, 32, 53–61. [Google Scholar] [CrossRef]
- Food Standards Australia New Zealand. Australian Food Composition Database—Release 1. Canberra: FSANZ. Available online: www.foodstandards.gov.au (accessed on 14 July 2020).
- Lasa, A.; Larretxi, I.; Simón, E.; Churruca, I.; Navarro, V.; Martínez, O.; Bustamante, M.; Miranda, J. New software for gluten-free diet evaluation and nutritional education. Nutrients 2019, 11, 2505. [Google Scholar] [CrossRef] [Green Version]
- Muir, J.G.; Shepherd, S.J.; Rosella, O.; Rose, R.; Barrett, J.S.; Gibson, P.R. Fructan and free fructose content of common Australian vegetables and fruit. J. Agric. Food Chem. 2007, 55, 6619–6627. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Rosella, O.; Rose, R.; Liels, K.; Barrett, J.S.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. Quantification of fructans, galacto-oligosacharides and other short-chain carbohydrates in processed grains and cereals. J. Hum. Nutr. Diet. 2011, 24, 154–176. [Google Scholar] [CrossRef]
- Halmos, E.P.; Christophersen, C.T.; Bird, A.R.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Consistent prebiotic effect on gut microbiota with altered fodmap intake in patients with crohn’s disease: A randomised, controlled cross-over trial of well-defined diets. Clin. Transl. Gastroenterol. 2016, 7, e164. [Google Scholar] [CrossRef]
- Nybacka, S.; Störsrud, S.; Liljebo, T.; Le Nevé, B.; Törnblom, H.; Simrén, M.; Winkvist, A. Within-and between-subject variation in dietary intake of fermentable oligo-, DI-, monosaccharides, and polyols among patients with irritable bowel syndrome. Curr. Dev. Nutr. 2019, 3. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, H.M.; Lomer, M.C.; Anderson, J.L.; Barrett, J.S.; Muir, J.G.; Irving, P.M.; Whelan, K. Fermentable carbohydrate restriction reduces luminal bifidobacteria and gastrointestinal symptoms in patients with irritable bowel syndrome. J. Nutr. 2012, 142, 1510–1518. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, M.; Jansen, C.; Martin, L.; Williams, M.; Seamark, L.; Staudacher, H.M.; Irving, P.M.; Whelan, K.; Lomer, M.C. Long-term impact of the low-FODMAP diet on gastrointestinal symptoms, dietary intake, patient acceptability, and healthcare utilization in irritable bowel syndrome. Neurogastroenterol. Motil. 2018, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staudacher, H.M.; Lomer, M.C.E.; Farquharson, F.M.; Louis, P.; Fava, F.; Franciosi, E.; Scholz, M.; Tuohy, K.M.; Lindsay, J.O.; Irving, P.M.; et al. A diet low in FODMAPs reduces symptoms in patients with irritable bowel syndrome and a probiotic restores bifidobacterium species: A randomized controlled trial. Gastroenterology 2017, 153, 936–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staudacher, H.M.; Ralph, F.S.E.; Irving, P.M.; Whelan, K.; Lomer, M.C.E. Nutrient Intake, Diet Quality, and Diet Diversity in Irritable Bowel Syndrome and the Impact of the Low FODMAP Diet. J. Acad. Nutr. Diet. 2020, 120, 535–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepherd, S.J.; Lomer, M.C.; Gibson, P.R. Short-chain carbohydrates and functional gastrointestinal disorders. Am. J. Gastroenterol. 2013, 108, 707–717. [Google Scholar] [CrossRef]
- Cingolani, A.; Paduano, D.; Vecchiarelli, V.; Demelas, M.; Corrias, P.T.; Casula, L.; Usai, P. Feasibility of low fermentable oligosaccharide, disaccharide, monosaccharide, and polyol diet and its effects on quality of life in an Italian cohort. Nutrients 2020, 12, 716. [Google Scholar] [CrossRef] [Green Version]
- Nanayakkara, W.S.; Gearry, R.B.; Muir, J.G.; O’Brien, L.; Wilkinson, T.J.; Williman, J.A.; Skidmore, P.M.L. Gastrointestinal symptoms and FODMAP intake of aged-care residents from Christchurch, New Zealand. Nutrients 2017, 9, 1083. [Google Scholar] [CrossRef] [Green Version]
- Staudacher, H.M.; Whelan, K. The low FODMAP diet: Recent advances in understanding its mechanisms and efficacy in IBS. Gut 2017, 66, 1517. [Google Scholar] [CrossRef] [Green Version]
- Dionne, J.; Ford, A.C.; Yuan, Y.; Chey, W.D.; Lacy, B.E.; Saito, Y.A.; Quigley, E.M.M.; Moayyedi, P. A systematic review and meta-analysis evaluating the efficacy of a gluten-free diet and a low FODMAPs diet in treating symptoms of irritable bowel syndrome. Am. J. Gastroenterol. 2018, 113, 1290–1300. [Google Scholar] [CrossRef] [Green Version]
- National Statistics Institute. Demographic and Social Characteristics of the Spanish Population. Available online: https://www.ine.es/index.htm (accessed on 14 July 2020).
- Iacovou, M. Adapting the low FODMAP diet to special populations: Infants and children. J. Gastroenterol. Hepatol. 2017, 32, 43–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, N.; Andersen, N.N.; Végh, Z.; Jensen, L.; Ankersen, D.V.; Felding, M.; Simonsen, M.H.; Burisch, J.; Munkholm, P. Ehealth: Low FODMAP diet vs. Lactobacillus rhamnosus GG in irritable bowel syndrome. World J. Gastroenterol. 2014, 20, 16215–16226. [Google Scholar] [CrossRef] [PubMed]
- Roncoroni, L.; Elli, L.; Doneda, L.; Bascuñán, K.A.; Vecchi, M.; Morreale, F.; Scricciolo, A.; Lombardo, V.; Pellegrini, N. A retrospective study on dietary FODMAP intake in celiac patients following a gluten-free diet. Nutrients 2018, 10, 1769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fodor, I.; Man, S.C.; Dumitrascu, D.L. Low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols diet in children. World J. Clin. Cases 2019, 7, 2666–2674. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.R.; Shepherd, S.J. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J. Gastroenterol. Hepatol. 2010, 25, 252–258. [Google Scholar] [CrossRef]
- Hewawasam, S.P.; Iacovou, M.; Muir, J.G.; Gibson, P.R. Dietary practices and FODMAPs in South Asia: Applicability of the low FODMAP diet to patients with irritable bowel syndrome. J. Gastroenterol. Hepatol. 2018, 33, 365–374. [Google Scholar] [CrossRef] [Green Version]
- McMeans, A.R.; King, K.L.; Chumpitazi, B.P. Low FODMAP Dietary Food Lists are Often Discordant. Am. J. Gastroenterol. 2017, 112, 655–656. [Google Scholar] [CrossRef] [Green Version]
- Moshfegh, A.J.; Friday, J.E.; Goldman, J.P.; Ahuja, J.K. Presence of inulin and oligofructose in the diets of Americans. J. Nutr. 1999, 129, 1407S–1411S. [Google Scholar] [CrossRef]
- van Loo, J.; Coussement, P.; de Leenheer, L.; Hoebregs, H.; Smits, G. On the presence of inulin and oligofructose as natural ingredients in the western diet. Crit. Rev. Food Sci. Nutr. 1995, 35, 525–552. [Google Scholar] [CrossRef]
- Ong, D.K.; Mitchell, S.B.; Barrett, J.S.; Shepherd, S.J.; Irving, P.M.; Biesiekierski, J.R.; Smith, S.; Gibson, P.R.; Muir, J.G. Manipulation of dietary short chain carbohydrates alters the pattern of gas production and genesis of symptoms in irritable bowel syndrome. J. Gastroenterol. Hepatol. 2010, 25, 1366–1373. [Google Scholar] [CrossRef]
- Pejcz, E.; Spychaj, R.; Gil, Z. Technological methods for reducing the content of fructan in wheat bread. Foods 2019, 8, 663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedewa, A.; Rao, S.S. Dietary fructose intolerance, fructan intolerance and FODMAPs. Curr. Gastroenterol. Rep. 2014, 16, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catassi, G.; Lionetti, E.; Gatti, S.; Catassi, C. The low FODMAP diet: Many question marks for a catchy acronym. Nutrients 2017, 9, 292. [Google Scholar] [CrossRef] [PubMed]
- Eswaran, S.; Dolan, R.D.; Ball, S.C.; Jackson, K.; Chey, W. The impact of a 4-week low-fodmap and mnice diet on nutrient intake in a sample of us adults with irritable bowel syndrome with diarrhea. J. Acad. Nutr. Diet. 2020, 120, 641–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.J.; Camilleri, M.; Vanner, S.; Tuck, C. Review article: Biological mechanisms for symptom causation by individual FODMAP subgroups—The case for a more personalised approach to dietary restriction. Aliment. Pharmacol. Ther. 2019, 50, 517–529. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FODMAP Intake | Children (3–9 Years) | Adolescents (10–17 Years) | Adults (18–74 Years) | Children vs. Adolescents | Children vs. Adults | Adolescents vs. Adults | |||
|---|---|---|---|---|---|---|---|---|---|
| (g/d) | Mean | SD | Mean | SD | Mean | SD | p Value | p Value | p Value |
| Lactose | 29.1 | 79.4 | 22.6 | 53.9 | 16.6 | 41.6 | 0.06 | <0.001 | 0.01 |
| Excess fructose * | 2.43 | 6.31 | 2.56 | 7.04 | 2.90 | 7.21 | 0.70 | 0.14 | 0.11 |
| Total fructan | 1.13 | 3.95 | 1.46 | 5.09 | 1.06 | 4.29 | 0.15 | 0.72 | 0.08 |
| Stachyose | 0.02 | 0.12 | 0.02 | 0.15 | 0.04 | 0.23 | 0.99 | 0.02 | 0.03 |
| Raffinose | 0.06 | 0.37 | 0.05 | 0.37 | 0.11 | 0.67 | 0.59 | 0.05 | 0.02 |
| Sorbitol | 0.62 | 2.05 | 0.57 | 2.18 | 0.67 | 2.52 | 0.64 | 0.65 | 0.38 |
| Mannitol | 0.02 | 0.15 | 0.03 | 0.24 | 0.03 | 0.17 | 0.33 | 0.19 | 1 |
| Total | 33.4 | 92.3 | 27.3 | 69.0 | 21.4 | 56.7 | 0.14 | <0.01 | 0.06 |
| Position | Food | Lactose Intake (g/d) | Food | Excess Fructose Intake (g/d) * | Food | Total Fructan Intake (g/d) | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| 1st | Whole cow milk | 9.33 | 11.2 | Apple | 1.52 | 3.06 | White bread | 0.14 | 0.16 |
| 2nd | Powdered milk | 6.27 | 31.8 | Pear | 0.33 | 1.01 | Garlic | 0.13 | 0.17 |
| 3rd | Partly skimmed cow milk | 5.75 | 9.54 | White bread | 0.16 | 0.18 | Onion | 0.11 | 0.16 |
| 4th | Plain yogurt | 2.11 | 3.96 | Plain sweet biscuit | 0.06 | 0.14 | Plain sweet biscuit | 0.10 | 0.22 |
| 5th | Flavoured yogurt | 1.76 | 3.17 | Orange juice | 0.05 | 0.22 | Leek | 0.08 | 0.27 |
| 6th | Sponge cake | 0.92 | 4.76 | Tomato | 0.05 | 0.10 | Sponge cake | 0.08 | 0.37 |
| 7th | Skimmed cow milk | 0.81 | 3.65 | Melon | 0.04 | 0.21 | Sandwich bread | 0.08 | 0.20 |
| 8th | Plain skimmed yogurt | 0.57 | 1.45 | Honey | 0.04 | 0.23 | Chocolate biscuits | 0.07 | 0.24 |
| 9th | Egg pudding dessert | 0.53 | 1.58 | Orange | 0.03 | 0.12 | Chocolate sponge cake | 0.02 | 0.16 |
| 10th | Milk chocolate | 0.19 | 0.87 | Strawberry | 0.03 | 0.12 | Corn flakes | 0.02 | 0.11 |
| Position | Food | Lactose Intake (g/d) | Food | Excess Fructose Intake (g/d) * | Food | Total Fructan Intake (g/d) | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| 1st | Whole cow milk | 7.95 | 14.44 | Apple | 1.46 | 3.20 | White bread | 0.25 | 0.24 |
| 2nd | Partly skimmed cow milk | 7.20 | 11.19 | Pear | 0.28 | 1.02 | Onion | 0.15 | 0.24 |
| 3rd | Plain yogurt | 1.94 | 4.01 | White bread | 0.27 | 0.27 | Garlic | 0.14 | 0.24 |
| 4th | Skimmed cow milk | 1.93 | 5.92 | Tomato | 0.08 | 0.16 | Sponge cake | 0.10 | 0.40 |
| 5th | Flavoured yogurt | 1.30 | 2.92 | Orange juice | 0.06 | 0.27 | Leak | 0.09 | 0.38 |
| 6th | Egg pudding dessert | 0.56 | 1.68 | Orange | 0.05 | 0.14 | Plain sweet biscuit | 0.08 | 0.20 |
| 7th | Skimmed yogurt | 0.40 | 1.24 | Plain sweet biscuit | 0.05 | 0.13 | Sandwich bread | 0.08 | 0.25 |
| 8th | Powdered milk | 0.33 | 8.19 | Honey | 0.04 | 0.25 | Chocolate biscuits | 0.06 | 0.25 |
| 9th | Flavoured skimmed yogurt | 0.11 | 0.75 | Strawberry | 0.04 | 0.15 | Pasta | 0.06 | 0.12 |
| 10th | Chocolate and hazelnut spread | 0.11 | 0.52 | Melon | 0.04 | 0.21 | Chocolate sponge cake | 0.03 | 0.20 |
| Position | Food | Lactose Intake (g/d) | Food | Excess Fructose Intake (g/d) * | Food | Total Fructan Intake (g/d) | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| 1st | Partly skimmed cow milk | 4.87 | 8.69 | Apple | 1.78 | 3.20 | White bread | 0.17 | 0.00 |
| 2nd | Skimmed cow milk | 3.88 | 7.07 | Pear | 0.31 | 1.03 | Onion | 0.16 | 0.27 |
| 3rd | Whole cow milk | 3.57 | 7.16 | White bread | 0.19 | 0.00 | Garlic | 0.14 | 0.60 |
| 4th | Plain yogurt | 1.09 | 2.80 | Tomato | 0.12 | 0.19 | Sponge cake | 0.08 | 0.37 |
| 5th | Plain skimmed yogurt | 0.90 | 2.11 | Honey | 0.07 | 0.31 | Leak | 0.08 | 0.38 |
| 6th | Flavoured yogurt | 0.42 | 1.87 | Orange | 0.07 | 0.15 | Sandwich bread | 0.06 | 0.20 |
| 7th | Sponge cake | 0.32 | 1.40 | Melon | 0.05 | 0.19 | Plain sweet biscuit | 0.05 | 0.14 |
| 8th | Egg pudding dessert | 0.31 | 1.26 | Sweet white wine | 0.03 | 0.36 | Peach | 0.04 | 0.19 |
| 9th | Flavoured skimmed yogurt | 0.28 | 1.18 | Tangerine | 0.03 | 0.10 | Watermelon | 0.02 | 0.07 |
| 10th | Ice-cream | 0.12 | 0.64 | Kiwi fruit | 0.03 | 0.14 | Melon | 0.02 | 0.06 |
| Percentage of Diet Contribution | Children (3–9 Years) | Adolescents (10–17 Years) | Adults (18–74 Years) |
|---|---|---|---|
| Fiber | −55 | −47 | −55 |
| Vitamin A | −32 | −25 | −36 |
| Vitamin C | −46 | −39 | −46 |
| Vitamin D | −14 | −9 | −5 |
| Riboflavin | −52 | −41 | −50 |
| Thiamin | −37 | −61 | −36 |
| Calcium | −72 | −59 | −68 |
| Magnesium | −44 | −38 | −41 |
| Zinc | −33 | −29 | −38 |
| Phosphorus | −45 | −39 | −43 |
| Iron | −33 | −21 | −38 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, J.; Vázquez-Polo, M.; Pérez-Junkera, G.; Fernández-Gil, M.d.P.; Bustamante, M.Á.; Navarro, V.; Simón, E.; Martínez, O. FODMAP Intake in Spanish Population: Open Approach for Risk Assessment. Int. J. Environ. Res. Public Health 2020, 17, 5882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165882
Miranda J, Vázquez-Polo M, Pérez-Junkera G, Fernández-Gil MdP, Bustamante MÁ, Navarro V, Simón E, Martínez O. FODMAP Intake in Spanish Population: Open Approach for Risk Assessment. International Journal of Environmental Research and Public Health. 2020; 17(16):5882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165882
Chicago/Turabian StyleMiranda, Jonatan, Maialen Vázquez-Polo, Gesala Pérez-Junkera, María del Pilar Fernández-Gil, María Ángeles Bustamante, Virginia Navarro, Edurne Simón, and Olaia Martínez. 2020. "FODMAP Intake in Spanish Population: Open Approach for Risk Assessment" International Journal of Environmental Research and Public Health 17, no. 16: 5882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165882