Health Technology Assessment Report on Vagus Nerve Stimulation in Drug-Resistant Epilepsy

 , , ,
, , ,
Abstract
:1. Background
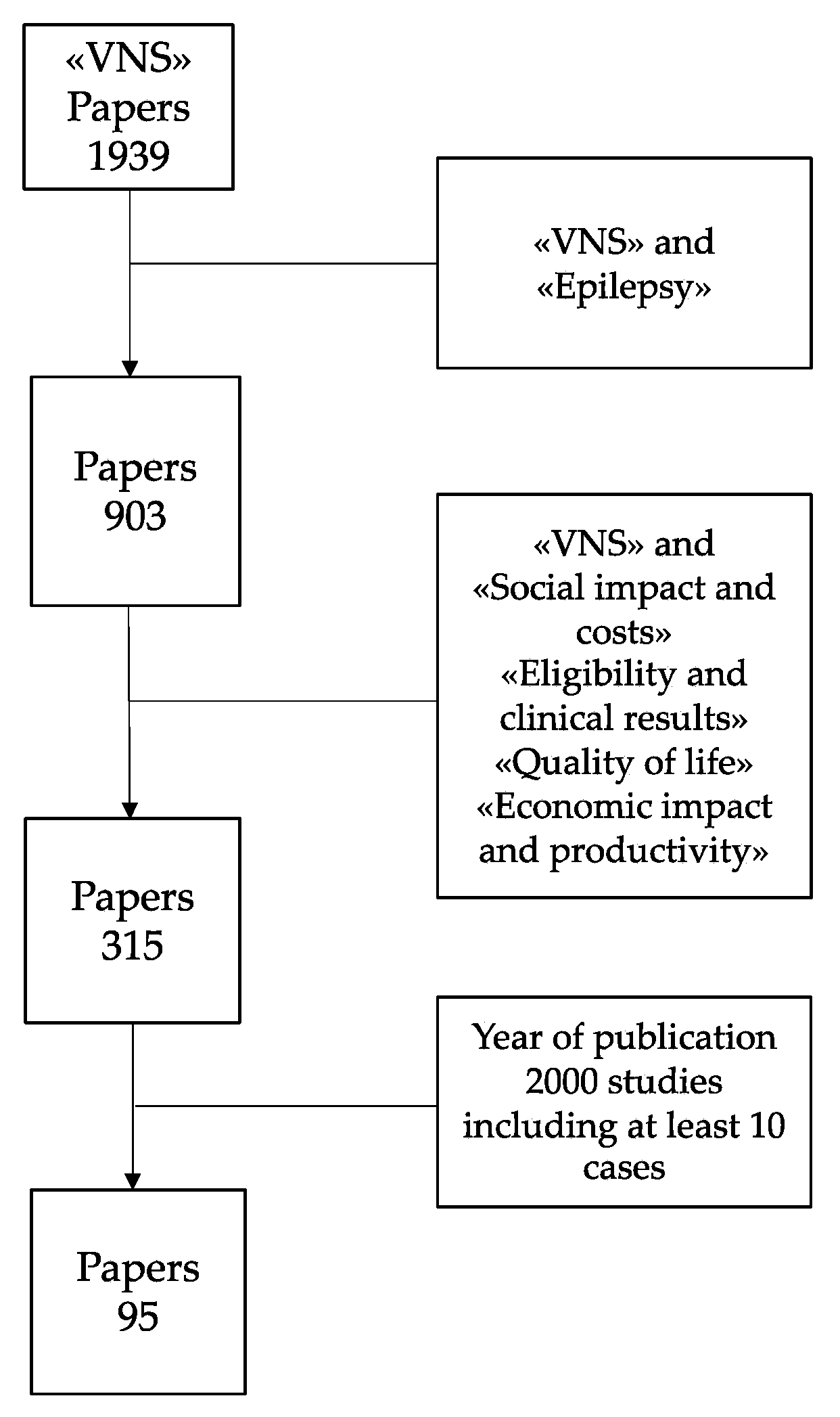
2. Methods
3. Results and Discussion
3.1. Social Impact and Costs of the Disease
3.2. VNS Eligibility and Clinical Results
3.3. Quality of Life (QoL), Quality Adjusted Life Years (QALY) and Health-Related Quality of Life (HRQOL) after VNS
3.4. Economic Impact and Productivity Regained after VNS
3.5. Costs of VNS
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AAN | American Academy of Neurology |
| ASDs | Antiseizure drugs |
| BMP | Best medical practice |
| DRG | Diagnosis-related group |
| EPC | Epilepsia Partialis Continua |
| FDA | Food & Drug Administration |
| GDP | Gross Domestic Product |
| HTA | Health Technology Assessment |
| HRQOL | health-related quality of life |
| ICU | Intensive Care Unit |
| ILAE | International League Against Epilepsy |
| LGS | Lennox Gastaut Syndrome |
| LICE | Lega Italiana Contro l’Epilessia |
| NICE | National Institute for Clinical Excellence |
| QALY | Quality Adjusted Life Years; QoL: Quality of Life |
| RSE | Resistant Status Epilepticus; |
| SE | Status Epilepticus |
| SUDEP | Sudden Unexpected Death in Epilepsy |
| VAT | Value Added Tax |
| WHO | World Health Organization |
References
- Ali, A. Global health: Epilepsy. Semin. Neurol. 2018, 38, 191–199. [Google Scholar] [CrossRef]
- Pahl, K.; de Boer, H.M. Epilepsy and Rights. In Atlas: Epilepsy Care in the World; WHO: Geneva, Switzerland, 2005; pp. 72–73. [Google Scholar]
- De Boer, H.M.; Mula, M.; Sander, J.W. The global burden and stigma of epilepsy. Epilepsy Behav. 2008, 12, 540–546. [Google Scholar] [CrossRef]
- Tombini, M.; Assenza, G.; Quintiliani, L.; Ricci, L.; Lanzone, J.; De Mojà, R.; Ulivi, M.; Di Lazzaro, V. Epilepsy-associated stigma from the perspective of people with epilepsy and the community in Italy. Epilepsy Behav. 2019, 98, 66–72. [Google Scholar] [CrossRef]
- Marras, C.E.; Canevini, M.P.; Colicchio, G.; Guerrini, R.; Rubboli, G.; Scerrati, M.; Spreafico, R.; Tassi, L.; Lorusso, G.; Tinuper, P.; et al. Health Technology Assessment report on the presurgical evaluation and surgical treatment of drug-resistant epilepsy. Epilepsia 2013, 54, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, S.; Blume, W.T.; Girvin, J.P.; Eliasziw, M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N. Engl. J. Med. 2001, 345, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, A.; Taslimi, S.; Abbasian, A.; Badhiwala, J.H.; Akbar, M.A.; Alotaibi, N.M.; Almenawer, S.A.; Weil, A.G.; Fallah, A.; Carmant, L.; et al. Surgical outcomes for medically intractable epilepsy in low- and middle-income countries: A systematic review and meta-analysis. J. Neurosurg. 2019, 131, 1068–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Téllez-Zenteno, J.F.; Dhar, R.; Wiebe, S. Long-term seizure outcomes following epilepsy surgery: A systematic review and meta-analysis. Brain 2005, 128, 1188–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryvlin, P.; Cross, J.H.; Rheims, S. Epilepsy surgery in children and adults. Lancet Neurol. 2014, 13, 1114–1126. [Google Scholar] [CrossRef]
- Vagus Nerve Stimulation Study Group. A randomized controlled trial of chronic vagus nerve stimulation for treatment of medically intractable seizures. Neurology 1995, 45, 224–230. [Google Scholar] [CrossRef]
- Schachter, S.C.; Saper, C.B. Vagus nerve stimulation. Epilepsia 1998, 39, 677–686. [Google Scholar] [CrossRef]
- Ben-Menachem, E.; Manon-Espaillat, R.; Ristanovic, R.; Wilder, B.J.; Stefan, H.; Mirza, W.; Tarver, W.B.; Wernicke, J.F.; First International Vagus Nerve Stimulation Study Group. Vagus Nerve Stimulation for Treatment of Partial Seizures: 1. A controlled study of effect on seizures. Epilepsia 1994, 35, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, R.E.; Uthman, B.M.; Augustinsson, L.E.; Upton, A.R.M.; Naritoku, D.; Willis, J.; Treig, T.; Barolat, G.; Wernicke, J.F.; First International Vagus Nerve Stimulation Study Group. Vagus Nerve Stimulation for Treatment of Partial Seizures: 2. Safety, Side Effects, and Tolerability. Epilepsia 1994, 35, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.V.; Torkelson, R.; Dowler, I.; Simon, S.; Hudson, S. Vagal Nerve Stimulation in Refractory Epilepsy. Arch. Pediatr. Adolesc. Med. 2003, 157, 560–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abubakr, A.; Wambacq, I. Long-term outcome of vagus nerve stimulation therapy in patients with refractory epilepsy. J. Clin. Neurosci. 2008, 15, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Panebianco, M.; Zavanone, C.; Dupont, S.; Restivo, D.; Pavone, A. Vagus nerve stimulation therapy in partial epilepsy: A review. Acta Neurol. Belg. 2016, 116, 241–248. [Google Scholar] [CrossRef]
- Panebianco, M.; Rigby, A.; Weston, J.; Marson, A.G. Vagus nerve stimulation for partial seizures. Cochrane Database Syst. Rev. 2015, 2015, CD002896. [Google Scholar] [CrossRef]
- Wheless, J.W.; Gienapp, A.J.; Ryvlin, P. Vagus nerve stimulation (VNS) therapy update. Epilepsy Behav. 2018, 88, 2–10. [Google Scholar] [CrossRef]
- González, H.; Yengo-Kahn, A.M.; Englot, D.J. Vagus Nerve Stimulation for the Treatment of Epilepsy. Neurosurg. Clin. N. Am. 2019, 30, 219–230. [Google Scholar] [CrossRef]
- Fan, J.; Shan, W.; Wu, J.; Wang, Q. Research progress of vagus nerve stimulation in the treatment of epilepsy. CNS Neurosci. Ther. 2019, 25, 1222–1228. [Google Scholar] [CrossRef]
- Shahwan, A.; Bailey, C.; Maxiner, W.; Harvey, A.S. Vagus nerve stimulation for refractory epilepsy in children: More to VNS than seizure frequency reduction. Epilepsia 2009, 50, 1220–1228. [Google Scholar] [CrossRef]
- Kopciuch, D.; Barciszewska, A.-M.; Fliciński, J.; Zaprutko, T.; Kus, K.; Steinborn, B.; Nowakowska, E. Analysis of pharmacotherapy regimen and costs in patients with drug-resistant epilepsy following vagus nerve stimulation therapy: A single-center study (Poland). Acta Neurol. Belg. 2019, 120, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Kopciuch, D.; Barciszewska, A.-M.; Fliciński, J.; Paczkowska, A.; Winczewska-Wiktor, A.; Jankowski, R.; Steinborn, B.; Nowakowska, E. Economic and clinical evaluation of vagus nerve stimulation therapy. Acta Neurol. Scand. 2019, 140, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Cukiert, A. Vagus Nerve Stimulation for Epilepsy: An Evidence-Based Approach. Prog. Neurol. Surg. 2015, 29, 39–52. [Google Scholar] [PubMed]
- Cicchetti, A.P. Presente e Futuro dell’Health Technology Assessment. Care 2009, 2, 21–23. [Google Scholar]
- Fattore, G.; Cavallo, M.C.; Tarricone, R. Lo sviluppo del Health Technology Assessment in Italia: Contenuti, approcci e riferimenti internazionali. Rapporto OASI 2008, 4, 151–178. [Google Scholar]
- Goodman, C.S. HTA 101: Introduction to Health Technology Assessment; Bethesda, M.D., Ed.; National Library of Medicine: Bethesda, MD, USA, 2014. Available online: https://www.nlm.nih.gov/nichsr/hta101/HTA_101_FINAL_7-23-14.pdf (accessed on 1 July 2020).
- Lopatriello, S.; Berto, P.; Canevini, M.B.; Colicchio, G.; Rubboli, G.; Spreafico, R.; Tassi, L.; Tinuper, P. La Gestione Delle Epilessie Farmacoresistenti. Hta Report. LICE. 2010. Available online: http://www.lice.it/pdf/report_HTA_old.pdf (accessed on 1 July 2020).
- Jacoby, A.; Austin, J.K. Social stigma for adults and children with epilepsy. Epilepsia 2007, 48, 6–9. [Google Scholar] [CrossRef] [Green Version]
- Camfield, C.S.; Camfield, P.R. Long-term social outcomes for children with epilepsy. Epilepsia 2007, 48, 3–5. [Google Scholar] [CrossRef]
- Bajaj, J.; Tripathi, M.; Dwivedi, R.; Sapra, S.; Gulati, S.; Garg, A.; Tripathi, M.; Bal, C.S.; Chandra, S.P. Does surgery help in reducing stigma associated with drug refractory epilepsy in children? Epilepsy Behav. 2018, 80, 197–201. [Google Scholar] [CrossRef]
- Pugliatti, M.; Beghi, E.; Forsgren, L.; Ekman, M.; Sobocki, P. Estimating the Cost of Epilepsy in Europe: A Review with Economic Modeling. Epilepsia 2007, 48, 2224–2233. [Google Scholar] [CrossRef]
- Argumosa, A.; Herranz, J.L. Childhood epilepsy: A critical review of cost-of-illness studies. Epileptic Disord. 2004, 6, 31–40. [Google Scholar]
- Wijnen, B.; Schat, S.L.; De Kinderen, R.J.; Colon, A.; Ossenblok, P.P.; Evers, S.M.A.A. Burden of disease of people with epilepsy during an optimized diagnostic trajectory: Costs and quality of life. Epilepsy Res. 2018, 146, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Berto, P.; Tinuper, P.; Viaggi, S. Cost-of-Illness of Epilepsy in Italy. PharmacoEconomics 2000, 17, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Ekman, M.; Forsgren, L. Economic evidence in epilepsy: A review. Eur. J. Health Econ. 2004, 5, s36–s42. [Google Scholar] [CrossRef]
- De Kinderen, R.J.; Postulart, D.; Aldenkamp, A.P.; Evers, S.M.A.A.; Lambrechts, D.A.; De Louw, A.; Majoie, M.; Grutters, J.P. Cost-effectiveness of the ketogenic diet and vagus nerve stimulation for the treatment of children with intractable epilepsy. Epilepsy Res. 2015, 110, 119–131. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, H.D.; Lee, J.S.; Heo, K.; Kim, D.S.; Kang, H.-C. Long-term prognosis of patients with Lennox–Gastaut syndrome in recent decades. Epilepsy Res. 2015, 110, 10–19. [Google Scholar] [CrossRef]
- Healy, S.; Lang, J.; Naude, J.T.W.; Gibbon, F.; Leach, P. Vagal nerve stimulation in children under 12 years old with medically intractable epilepsy. Childs Nerv. Syst. 2013, 29, 2095–2099. [Google Scholar] [CrossRef]
- Morris, G.L.; Gloss, D.; Buchhalter, J.; Mack, K.J.; Nickels, K.; Harden, C. Evidence-based guideline update: Vagus nerve stimulation for the treatment of epilepsy: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2013, 81, 1453–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHugh, J.C.; Singh, H.W.; Phillips, J.; Murphy, K.; Doherty, C.P.; Delanty, N. Outcome Measurement after Vagal Nerve Stimulation Therapy: Proposal of a New Classification. Epilepsia 2007, 48, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Parain, D.; Penniello, M.J.; Berquen, P.; Delangre, T.; Billard, C.; Murphy, J.V. Vagal nerve stimulation in tuberous sclerosis complex patients. Pediatr. Neurol. 2001, 25, 213–216. [Google Scholar] [CrossRef]
- Janszky, J.; Hoppe, M.; Behne, F.; Tuxhorn, I.; Pannek, H.W.; Ebner, A. Vagus nerve stimulation: Predictors of seizure freedom. J. Neurol. Neurosurg. Psychiatry 2005, 76, 384–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terra-Bustamante, V.C.; Machado, H.R.; Oliveira, R.D.S.; Serafini, L.N.; Souza-Oliveira, C.; Escorsi-Rosset, S.; Yacubian, E.M.T.; Naffah-Mazzacoratti, M.; Scorza, C.A.; A Cavalheiro, E.; et al. Rasmussen encephalitis: Long-term outcome after surgery. Child’s Nerv. Syst. 2009, 25, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Klinkenberg, S.; Aalbers, M.; Vles, J.S.H.; Cornips, E.; Rijkers, K.; Leenen, L.; Kessels, F.G.H.; Aldenkamp, A.P.; Majoie, M. Vagus nerve stimulation in children with intractable epilepsy: A randomized controlled trial. Dev. Med. Child Neurol. 2012, 54, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Englot, D.J.; Chang, E.F.; Auguste, K.I. Vagus nerve stimulation for epilepsy: A meta-analysis of efficacy and predictors of response. J. Neurosurg. 2011, 115, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- Englot, D.J.; Chang, E.F.; Auguste, K.I. Efficacy of Vagus Nerve Stimulation for Epilepsy by Patient Age, Epilepsy Duration, and Seizure Type. Neurosurg. Clin. N. Am. 2011, 22, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Kavčič, A.; Kajdič, N.; Primec, Z.R.; Krajnc, N.; Žgur, T. Efficacy and tolerability of vagus nerve stimulation therapy (VNS) in Slovenian epilepsy patients: Younger age and shorter duration of epilepsy might result in better outcome. Acta Clin. Croat. 2019, 58, 255–264. [Google Scholar] [CrossRef]
- Chrastina, J.; Novák, Z.; Zeman, T.; Kocvarova, J.; Pail, M.; Doležalová, I.; Jarkovsky, J.; Brázdil, M. Single-center long-term results of vagus nerve stimulation for epilepsy: A 10–17 year follow-up study. Seizure 2018, 59, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Kuba, R.; Brázdil, M.; Kalina, M.; Procházka, T.; Hovorka, J.; Nežádal, T.; Hadac, J.; Brožová, K.; Sebroňová, V.; Komarek, V.; et al. Vagus nerve stimulation: Longitudinal follow-up of patients treated for 5 years. Seizure 2009, 18, 269–274. [Google Scholar] [CrossRef]
- Vonck, K.; Thadani, V.; Gilbert, K.; Dedeurwaerdere, S.; De Groote, L.; De Herdt, V.; Goossens, L.; Gossiaux, F.; Achten, E.; Thiery, E.; et al. Vagus nerve stimulation for refractory epilepsy: A transatlantic experience. J. Clin. Neurophysiol. 2004, 21, 283–289. [Google Scholar] [CrossRef]
- De Herdt, V.; Boon, P.; Ceulemans, B.; Hauman, H.; Lagae, L.; Legros, B.; Sadzot, B.; Van Bogaert, P.; Van Rijckevorsel, K.; Verhelst, H.; et al. Vagus nerve stimulation for refractory epilepsy: A Belgian multicenter study. Eur. J. Paediatr. Neurol. 2007, 11, 261–269. [Google Scholar] [CrossRef]
- Rossignol, E.; Lortie, A.; Thomas, T.; Bouthiller, A.; Scavarda, D.; Mercier, C.; Carmant, L. Vagus nerve stimulation in pediatric epileptic syndromes. Seizure 2009, 18, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Patwardhan, R.V.; Stong, B.; Bebin, E.M.; Mathisen, J.; A Grabb, P. Efficacy of vagal nerve stimulation in children with medically refractory epilepsy. Neurosurgery 2000, 47, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Nakken, K.O.; Henriksen, O.; Røste, G.K.; Lossius, R. Vagal nerve stimulation—The Norwegian experience. Seizure 2003, 12, 37–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardesch, J.; Buschman, H.; Wagener-Schimmel, L.; Van Der Aa, H.; Hageman, G. Vagus nerve stimulation for medically refractory epilepsy: A long-term follow-up study. Seizure 2007, 16, 579–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terra, V.C.; Furlanetti, L.L.; Nunes, A.A.; Thome, U.; Nisyiama, M.A.; Sakamoto, A.C.; Machado, H.R. Vagus nerve stimulation in pediatric patients: Is it really worthwhile? Epilepsy Behav. 2014, 31, 329–333. [Google Scholar] [CrossRef]
- Fernandez, L.; Gedela, S.; Tamber, M.; Sogawa, Y. Vagus nerve stimulation in children less than 3 years with medically intractable epilepsy. Epilepsy Res. 2015, 112, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Orosz, I.; McCormick, D.; Zamponi, N.; Varadkar, S.; Feucht, M.; Parain, D.; Griens, R.; Vallée, L.; Boon, P.; Rittey, C.; et al. Vagus nerve stimulation for drug-resistant epilepsy: A European long-term study up to 24 months in 347 children. Epilepsia 2014, 55, 1576–1584. [Google Scholar] [CrossRef]
- Kabir, S.M.R.; Rajaraman, C.; Rittey, C.; Zaki, H.S.; Kemeny, A.A.; McMullan, J. Vagus nerve stimulation in children with intractable epilepsy: Indications, complications and outcome. Childs Nerv. Syst. 2009, 25, 1097–1100. [Google Scholar] [CrossRef]
- Alexopoulos, A.V.; Kotagal, P.; Loddenkemper, T.; Hammel, J.; Bingaman, W.E. Long-term results with vagus nerve stimulation in children with pharmacoresistant epilepsy. Seizure 2006, 15, 491–503. [Google Scholar] [CrossRef] [Green Version]
- Colicchio, G.; Policicchio, D.; Barbati, G.; Cesaroni, E.; Fuggetta, F.; Meglio, M.; Papacci, F.; Rychlicki, F.; Scerrati, M.; Zamponi, N. Vagal nerve stimulation for drug-resistant epilepsies in different age, aetiology and duration. Childs Nerv. Syst. 2010, 26, 811–819. [Google Scholar] [CrossRef]
- Kocvarova, J.; Novák, Z.; Doležalová, I.; Svoboda, M.; Brázdil, M.; Chrastina, J. Older Age and Longer Epilepsy Duration Do Not Predict Worse Seizure Reduction Outcome after Vagus Nerve Stimulation. J. Neurol. Surg. Part A Central Eur. Neurosurg. 2017, 79, 152–158. [Google Scholar] [CrossRef]
- Renfroe, J.B.; Wheless, J.W. Earlier use of adjunctive vagus nerve stimulation therapy for refractory epilepsy. Neurology 2002, 59. [Google Scholar] [CrossRef] [PubMed]
- LaBar, D. Vagus nerve stimulation for 1 year in 269 patients on unchanged antiepileptic drugs. Seizure 2004, 13, 392–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.-J.; Tan, G.; Zhu, L.-N.; Chen, D.; Xu, D.; Chu, S.-S.; Liu, L. Predictors of seizure reduction outcome after vagus nerve stimulation in drug-resistant epilepsy. Seizure 2019, 66, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helmers, S.L.; Griesemer, D.A.; Dean, J.C.; Sanchez, J.D.; LaBar, D.; Murphy, J.V.; Bettis, D.; Park, Y.D.; Shuman, R.M.; Morris, G.L. Observations on the Use of Vagus Nerve Stimulation Earlier in the Course of Pharmacoresistant Epilepsy: Patients With Seizures for Six Years or Less. Neurology 2003, 9, 160–164. [Google Scholar] [CrossRef]
- Ghaemi, K.; Elsharkawy, A.E.; Schulz, R.; Hoppe, M.; Polster, T.; Pannek, H.; Ebner, A. Vagus nerve stimulation: Outcome and predictors of seizure freedom in long-term follow-up. Seizure 2010, 19, 264–268. [Google Scholar] [CrossRef] [Green Version]
- Marras, C.E.; Chiesa, V.; De Benedictis, A.; Franzini, A.; Rizzi, M.; Villani, F.; Ragona, F.; Tassi, L.; Vignoli, A.; Freri, E.; et al. Vagus nerve stimulation in refractory epilepsy: New indications and outcome assessment. Epilepsy Behav. 2013, 28, 374–378. [Google Scholar] [CrossRef]
- Casazza, M.; Avanzini, G.; Ferroli, P.; Villani, F.; Raggi, A. Vagal nerve stimulation: Relationship between outcome and electroclinical seizure pattern. Seizure 2006, 15, 198–207. [Google Scholar] [CrossRef] [Green Version]
- Alsaadi, T.M.; Laxer, K.D.; Barbaro, N.M.; Marks, W.J.; Garcia, P.A. Vagus nerve stimulation for the treatment of bilateral independent temporal lobe epilepsy. Epilepsia 2001, 42, 954–956. [Google Scholar] [CrossRef] [Green Version]
- Kuba, R.; Brázdil, M.; Novák, Z.; Chrastina, J.; Rektor, I. Effect of vagal nerve stimulation on patients with bitemporal epilepsy. Eur. J. Neurol. 2003, 10, 91–94. [Google Scholar] [CrossRef]
- Hilderink, J.; Tjepkema-Cloostermans, M.C.; Geertsema, A.; Glastra-Zwiers, J.; De Vos, C.C. Predicting success of vagus nerve stimulation (VNS) from EEG symmetry. Seizure 2017, 48, 69–73. [Google Scholar] [CrossRef] [Green Version]
- De Vos, C.; Melching, L.; Van Schoonhoven, J.; Ardesch, J.; De Weerd, A.; Van Lambalgen, H.; Van Putten, M.J. Predicting success of vagus nerve stimulation (VNS) from interictal EEG. Seizure 2011, 20, 541–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolston, J.D.; Englot, D.J.; Wang, R.D.; Garcia, P.A.; Chang, E.F. Corpus callosotomy versus vagus nerve stimulation for atonic seizures and drop attacks: A systematic review. Epilepsy Behav. 2015, 51, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cukiert, A.; Cukiert, C.M.; Burattini, J.A.; Lima, A.M.; Forster, C.R.; Baise, C.; Argentoni-Baldochi, M. Long-term outcome after callosotomy or vagus nerve stimulation in consecutive prospective cohorts of children with Lennox–Gastaut or Lennox-like syndrome and non-specific MRI findings. Seizure 2013, 22, 396–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillamón, E.; Miró, J.; Gutiérrez, A.; Conde, R.; Falip, M.; Jaraba, S.; Plans, G.; Garcés, M.; Villanueva, V. Combination of Corpus Callosotomy and Vagus Nerve Stimulation in the Treatment of Refractory Epilepsy. Eur. Neurol. 2013, 71, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Kossoff, E.H.; Shields, W.D. Nonpharmacologic care for patients with Lennox-Gastaut syndrome: Ketogenic diets and vagus nerve stimulation. Epilepsia 2014, 55, 29–33. [Google Scholar] [CrossRef]
- Ben-Menachem, E.; Hellström, K.; Waldton, C.; Augustinsson, L.E. Evaluation of refractory epilepsy treated with vagus nerve stimulation for up to 5 years. Neurology 1999, 52, 1265. [Google Scholar] [CrossRef]
- Frost, M.; Gates, J.; Helmers, S.L.; Wheless, J.W.; Levisohn, P.; Tardo, C.; Conry, J.A. Vagus nerve stimulation in children with refractory seizures associated with Lennox-Gastaut syndrome. Epilepsia 2001, 42, 1148–1152. [Google Scholar] [CrossRef] [Green Version]
- Lundgren, J.; Amark, P.; Blennow, G.; Stromblad, L.G.; Wallstedt, L. Vagus nerve stimulation in 16 children with refractory epilepsy. Epilepsia 1998, 39, 809–813. [Google Scholar] [CrossRef]
- De Benedictis, A.; Freri, E.; Rizzi, M.; Franzini, A.; Ragona, F.; Specchio, N.; Rebessi, E.; Casazza, M.; Granata, T.; Marras, C.E. Vagus nerve stimulation for drug-resistant Epilepsia Partialis Continua: Report of four cases. Epilepsy Res. 2013, 107, 163–171. [Google Scholar] [CrossRef]
- Dibué-Adjei, M.; Brigo, F.; Yamamoto, T.; Vonck, K.; Trinka, E. Vagus nerve stimulation in refractory and super-refractory status epilepticus—A systematic review. Brain Stimul. 2019, 12, 1101–1110. [Google Scholar] [CrossRef] [Green Version]
- Annegers, J.F.; Coan, S.P.; Hauser, W.A.; Leestma, J. Epilepsy, vagal nerve stimulation by the NCP system, all-cause mortality, and sudden, unexpected, unexplained death. Epilepsia 2000, 41, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Kotagal, P. Neurostimulation: Vagus Nerve Stimulation and Beyond. Semin. Pediatr. Neurol. 2011, 18, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Terra, V.C.; Nisyiama, M.A.; Abrão, J.; Sakamoto, A.C.; Machado, H.R.; Arida, R.M.; A Cavalheiro, E.; Scorza, F.A. Epileptologists probe vagus nerve stimulation in children with refractory epilepsy: A promise against sudden unexpected death in epilepsy. Arq. Neuro-Psiquiatria 2012, 70, 953–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granbichler, C.A.; Nashef, L.; Selway, R.; E Polkey, C. Mortality and SUDEP in epilepsy patients treated with vagus nerve stimulation. Epilepsia 2015, 56, 291–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomson, T.; Sveinsson, O.; Carlsson, S.; Andersson, T. Evolution over time of SUDEP incidence: A nationwide population-based cohort study. Epilepsia 2018, 59, e120–e124. [Google Scholar] [CrossRef] [Green Version]
- Ryvlin, P.; So, E.; Gordon, C.M.; Hesdorffer, D.C.; Sperling, M.R.; Devinsky, O.; Bunker, M.T.; Olin, B.; Friedman, D. Long-term surveillance of SUDEP in drug-resistant epilepsy patients treated with VNS therapy. Epilepsia 2018, 59, 562–572. [Google Scholar] [CrossRef]
- Amar, A.P.; Apuzzo, M.L.; Liu, C.Y. Vagus Nerve Stimulation Therapy After Failed Cranial Surgery for Intractable Epilepsy. Neurosurgery 2008, 62, 1086–1093. [Google Scholar] [CrossRef]
- Ulate-Campos, A.; Cean-Cabrera, L.; Petanas-Argemi, J.; Garcia-Fructuoso, G.; Aparicio, J.; López-Sala, A.; Palacio-Navarro, A.; Mas, M.; Muchart, J.; Rebollo, M.; et al. Resultados de la colocación del estimulador del nervio vago en epilepsia y calidad de vida en un hospital pediátrico. Neurología 2015, 30, 465–471. [Google Scholar] [CrossRef]
- De Faes, G.M.; Moyano, B.S.; Extremera, V.C.; Vinués, B.M.; Fernández, M.G.; Jiménez, M.; Ángeles, P.; Martín, M.B.R.; Ezquiaga, J.G.; Rodríguez, A.D.; et al. Diez años de experiencia con el estimulador del nervio vago en una población pediátrica. Rev. Neurol. 2018, 67, 382. [Google Scholar] [CrossRef]
- Soleman, J.; Stein, M.; Knorr, C.; Datta, A.N.; Constantini, S.; Fried, I.; Guzman, R.; Kramer, U. Improved quality of life and cognition after early vagal nerve stimulator implantation in children. Epilepsy Behav. 2018, 88, 139–145. [Google Scholar] [CrossRef]
- Ryvlin, P.; Gilliam, F.G.; Nguyen, D.K.; Colicchio, G.; Iudice, A.; Tinuper, P.; Zamponi, N.; Aguglia, U.; Wagner, L.; Minotti, L.; et al. The long-term effect of vagus nerve stimulation on quality of life in patients with pharmacoresistant focal epilepsy: The PuLsE (Open Prospective Randomized Long-term Effectiveness) trial. Epilepsia 2014, 55, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Majoie, M.; Berfelo, M.; Aldenkamp, A.; Renier, W.; Kessels, A. Vagus nerve stimulation in patients with catastrophic childhood epilepsy, a 2-year follow-up study. Seizure 2005, 14, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikati, M.A.; Ataya, N.F.; El-Ferezli, J.C.; Baghdadi, T.S.; Turkmani, A.H.; Comair, Y.G.; Kansagra, S.; Najjar, M.W. Quality of life after vagal nerve stimulator insertion. Epileptic Disord. 2009, 11, 067–074. [Google Scholar] [CrossRef] [PubMed]
- Ekmekçi, H.; Kaptan, H. Vagal nerve stimulation has robust effects on neuropsychiatric assessment in resistant epilepsy: A clinical series with clinical experiences. Turk. Neurosurg. 2018, 29, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Englot, D.J.; Hassnain, K.H.; Rolston, J.D.; Harward, S.C.; Sinha, S.R.; Haglund, M.M. Quality-of-life metrics with vagus nerve stimulation for epilepsy from provider survey data. Epilepsy Behav. 2016, 66, 4–9. [Google Scholar] [CrossRef]
- Tsai, J.-D.; Chang, Y.-C.; Lin, L.-C.; Hung, K.-L. The neuropsychological outcome of pediatric patients with refractory epilepsy treated with VNS—A 24-month follow-up in Taiwan. Epilepsy Behav. 2016, 56, 95–98. [Google Scholar] [CrossRef]
- Vonck, K.; Raedt, R.; Naulaerts, J.; De Vogelaere, F.; Thiery, E.; Van Roost, D.; Aldenkamp, A.P.; Miatton, M.; Boon, P. Vagus nerve stimulation, 25 years later! What do we know about the effects on cognition? Neurosci. Biobehav. Rev. 2014, 45, 63–71. [Google Scholar] [CrossRef]
- Sourbron, J.; Klinkenberg, S.; Kessels, A.; Schelhaas, H.J.; Lagae, L.; Majoie, M. Vagus Nerve Stimulation in children: A focus on intellectual disability. Eur. J. Paediatr. Neurol. 2017, 21, 427–440. [Google Scholar] [CrossRef]
- Schevernels, H.; Van Bochove, M.E.; De Taeye, L.; Bombeke, K.; Vonck, K.; Van Roost, D.; De Herdt, V.; Santens, P.; Raedt, R.; Boehler, C.N. The effect of vagus nerve stimulation on response inhibition. Epilepsy Behav. 2016, 64, 171–179. [Google Scholar] [CrossRef]
- DeGiorgio, C.M.; Schachter, S.C.; Handforth, A.; Salinsky, M.; Thompson, J.; Uthman, B.; Reed, R.; Collin, S.; Tecoma, E.; Morris, G.L.; et al. Prospective Long-Term Study of Vagus Nerve Stimulation for the Treatment of Refractory Seizures. Epilepsia 2000, 41, 1195–1200. [Google Scholar] [CrossRef]
- Aburahma, S.K.; Alzoubi, F.Q.; Hammouri, H.; Masri, A. Vagus nerve stimulation therapy in a developing country: A long term follow up study and cost utility analysis. Seizure 2015, 25, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soleman, J.; Knorr, C.; Datta, A.N.; Strozzi, S.; Ramelli, G.P.; Mariani, L.; Guzman, R. Early vagal nerve stimulator implantation in children: Personal experience and review of the literature. Childs Nerv. Syst. 2017, 34, 893–900. [Google Scholar] [CrossRef]
- Helmers, S.L.; Duh, M.S.; Guérin, A.; Sarda, S.P.; Samuelson, T.M.; Bunker, M.T.; Olin, B.; Jackson, S.D.; Faught, E. Clinical outcomes, quality of life, and costs associated with implantation of vagus nerve stimulation therapy in pediatric patients with drug-resistant epilepsy. Eur. J. Paediatr. Neurol. 2012, 16, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Sherman, E.M.S.; Connolly, M.; Slick, D.J.; Eyrl, K.L.; Steinbok, P.; Farrell, K. Quality of Life and Seizure Outcome After Vagus Nerve Stimulation in Children With Intractable Epilepsy. J. Child Neurol. 2008, 23, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-T.; Chiu, N.-C.; Kuo, Y.-T.; Shen, E.-Y.; Tsai, P.-C.; Ho, C.-S.; Wu, W.-H.; Chen, J.-C.; Wang, C.-Y.; Wang, H.-S.; et al. Parenting stress in parents of children with refractory epilepsy before and after vagus nerve stimulation implantation. Pediatr. Neonatol. 2017, 58, 516–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, S.; Majumdar, A.; Mallick, A.; Patel, J.; Scatchard, R.; Partridge, C.; Lux, A. Caregiver’s perception of epilepsy treatment, quality of life and comorbidities in an international cohort of CDKL5 patients. Hippokratia 2017, 21, 130–135. [Google Scholar]
- You, S.J.; Kang, H.-C.; Kim, H.D.; Ko, T.-S.; Kim, D.-S.; Hwang, Y.S.; Kim, D.S.; Lee, J.-K.; Park, S.K. Vagus Nerve Stimulation in Intractable Childhood Epilepsy: A Korean Multicenter Experience. J. Korean Med. Sci. 2007, 22, 442–445. [Google Scholar] [CrossRef] [Green Version]
- Spindler, P.; Bohlmann, K.; Straub, H.-B.; Vajkoczy, P.; Schneider, U.C. Effects of vagus nerve stimulation on symptoms of depression in patients with difficult-to-treat epilepsy. Seizure 2019, 69, 77–79. [Google Scholar] [CrossRef]
- Chan, A.Y.; Rolston, J.D.; Rao, V.R.; Chang, E.F. Effect of neurostimulation on cognition and mood in refractory epilepsy. Epilepsia Open 2018, 3, 18–29. [Google Scholar] [CrossRef]
- Sun, L.; Peräkylä, J.; Holm, K.; Haapasalo, J.; Lehtimäki, K.; Ogawa, K.H.; Peltola, J.; Hartikainen, K.M. Vagus nerve stimulation improves working memory performance. J. Clin. Exp. Neuropsychol. 2017, 39, 954–964. [Google Scholar] [CrossRef]
- Health Care Authority. Vagal Nerve Stimulation for Epilepsy and Depression; Final Evidence Report; Health Care Authority: Washington, DC, USA, 2020.
- Boon, P.; Vonck, K.; De Reuck, J.; Caemaert, J. Vagus nerve stimulation for refractory epilepsy. Seizure 2001, 10, 448–455. [Google Scholar] [CrossRef]
- Boon, P.; Vonck, K.; Vandekerckhove, T.; D’Have, M.; Nieuwenhuis, L.; Michielsen, G.; Vanbelleghem, H.; Goethals, I.; Caemaert, J.; Calliauw, L.; et al. Vagus nerve stimulation for medically refractory epilepsy; efficacy and cost-benefit analysis. Acta Neurochir. 1999, 141, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Boon, P.; Vonck, K.; D’Have, M.; O’Connor, S.; Vandekerckhove, T.; De Reuck, J. Cost-benefit of vagus nerve stimulation for refractory epilepsy. Acta Neurol. Belg. 1999, 99, 275–280. [Google Scholar] [PubMed]
- Boon, P.; D’Hav, M.; Van Walleghem, P.; Michielsen, G.; Vonck, K.; Caemaert, J.; De Reuck, J.; D’Havé, M. Direct medical costs of refractory epilepsy incurred by three different treatment modalities: A prospective assessment. Epilepsia 2002, 43, 96–102. [Google Scholar] [CrossRef] [Green Version]
- Purser, M.; Mladsi, D.M.; Beckman, A.; Barion, F.; Forsey, J. Expected Budget Impact and Health Outcomes of Expanded Use of Vagus Nerve Stimulation Therapy for Drug-Resistant Epilepsy. Adv. Ther. 2018, 35, 1686–1696. [Google Scholar] [CrossRef]
- Jennum, P.; Sabers, A.; Christensen, J.; Ibsen, R.; Kjellberg, J. Socioeconomic evaluation of vagus stimulation: A controlled national study. Seizure 2016, 42, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Ben-Menachem, E.; Hellström, K.; Verstappen, D. Analysis of direct hospital costs before and 18 months after treatment with vagus nerve stimulation therapy in 43 patients. Neurology 2002, 59, S44–S47. [Google Scholar] [CrossRef]
- Bernstein, A.L.; Barkan, H.; Hess, T. Vagus nerve stimulation therapy for pharmacoresistant epilepsy: Effect on health care utilization. Epilepsy Behav. 2007, 10, 134–137. [Google Scholar] [CrossRef]
- Bodin, E.; Le Moing, A.-G.; Bourel-Ponchel, E.; Querne, L.; Toussaint, P.; Berquin, P. Vagus nerve stimulation in the treatment of drug-resistant epilepsy in 29 children. Eur. J. Paediatr. Neurol. 2016, 20, 346–351. [Google Scholar] [CrossRef]
- Burke, T.; Hughes, D.; Forsey, J.; Bunker, M.; Bhattacharya, D.; Smithson, W.H. A study of the impact of VNS on health care utilisation in England. Seizure 2016, 34, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Kalanithi, P.S.; Arrigo, R.T.; Tran, P.; Gephart, M.H.; Shuer, L.; Fisher, R.; Boakye, M. Rehospitalization and Emergency Department Use Rates Before and After Vagus Nerve Stimulation for Epilepsy: Use of State Databases to Provide Longitudinal Data Across Multiple Clinical Settings. Neuromodulation Technol. Neural Interface 2013, 17, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Helmers, S.L.; Duh, M.S.; Guérin, A.; Sarda, S.P.; Samuelson, T.M.; Bunker, M.T.; Olin, B.D.; Jackson, S.D.; Faught, E. Clinical and economic impact of vagus nerve stimulation therapy in patients with drug-resistant epilepsy. Epilepsy Behav. 2011, 22, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Révész, D.; Rydenhag, B.; Ben-Menachem, E. Complications and safety of vagus nerve stimulation: 25 years of experience at a single center. J. Neurosurg. Pediatr. 2016, 18, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Author (Ref) | Patients Number | Mean/Range Age at Implantation | Mean/Range Follow-Up | Seizure Free % (n) | Responders % (n) of Patients with ≥50% Seizure Reduction |
|---|---|---|---|---|---|
| Abubakr [15] | 31 | 14 to 62 years | 4 years | - | 53% (16) |
| Gonzales [19] | 1194 | n.d. | 24–48 months | 8% | 63% |
| Morris [40] | 481 | n.d. | 1–5 years | n.d. | 55% |
| Parain [42] | 10 | 5 to 20 y | 22 months | 0% | 90% |
| Janszky [43] | 47 | 22.7 y | 22 months | 13% | n.d. |
| Klinkenberg [45] | 41 | 4 to 18 y | 10 months | n.d. | 26% |
| Englot [46] | 3321 | n.d. | 3 to 64 months | n.d. | 21 to 50% |
| Englot [47] | 4483 1104 | - | 3 months 24 months | - | 44% 56% |
| Chrastina [49] | 74 | 18–59 years | 10 years | n.d. | 63.6% |
| Kuba [50] | 90 | 36.3 years | 5 years | (5) | (44/85) |
| Vonck [51] | 131 | 32 years | 33 months | 7% | 50% |
| De Herdt [52] | 138 | 30 years | 44 months | 9% (12) | 13% |
| Patwardhan [54] | 38 | 11 months–16 years | 12 moths (10 months–18 months) | n.d. (n 29% >90% reduction) | 68% |
| Nakken [55] | 47 | 34.4 years | 2.7 years | 2% (1 pt) | 32% (15) |
| Fernandez [58] | 15 | 3 years < | 4.3 years (1.4 years–10.2) | 0% | categorical variable reported 33% “improvement” |
| Terra [57] | 36 | up to 18years | 12 months to 4 years | (1 pt) | 55% ≥ 50% seizure reduction |
| Orosz [59] | 347 | 6 months to 17.9 years | 24 months | 8% (17/208) | 43.8% |
| Kabir [60] | 69 | 10.69 years | 6 months to 10 years | 1.4% (1) | 8.7% (6) Engel II 90% (63) Engel III–IV |
| Alexopoulos [61] | 46 | 12 years | 2 years | 10% (5) | 43.5% (20) |
| Colicchio [62] | 135 | 5 months to 64 years | 36 months | 5.1% | 49% |
| Wang [66] | 1061 | 5–60 years | 6 months–12 years | n.d. | 53.53% |
| Ghaemi [68] | 144 | 3 to 65 years | 2 years | (10) | 62% (89) |
| Marras [69] | 35 | 6 to 52 years | 36 months | - | 51% (18) |
| Amar [90] | 921 CS 3822 Non-CS | 28 years 26 years | 24 months 24 months | 5% 8% | 55% 62% |
| Ulate-Campos [91] | 30 | 21 months (1–144) | 6–36 months | n.d. | 50% |
| Moro de Faes [92] | 35 | 3–18 years | 3 months to 2–3 years | n.d. | 43% |
| Soleman [93] | 45 | 133.9 ± 184.5 months | 72.3 ± 39.8 months | n.d. | 49.9% |
| Items | Lazio | Emilia Romagna | Lombardia | National Average |
|---|---|---|---|---|
| Surgery | EUR 3182 | EUR 5168 | EUR 2204 | EUR 3518 |
| VNS device | EUR 21,084 | EUR 21,084 | EUR 21,084 | EUR 21,084 |
| Hospital stay | EUR 1327 | EUR 2293 | EUR 2203 | EUR 1941 |
| Total costs | EUR 25,593 | EUR 28,545 | EUR 25,491 | EUR 26,543 |
| Total costs without device | EUR 4509 | EUR 7461 | EUR 4407 | EUR 5459 |
| Health Resources | Min | Max | National Average |
|---|---|---|---|
| Days of hospitalization/patient (no.) | 3 | 4 | 4 |
| Average duration of surgery (hours) | 1 | 3 | 2 |
| Duration occupancy operating room (hours) | 2 | 5 | 3 |
| Hours of intensive care/patient (no.) | 0 | 0 | 0 |
| Items | Min (EUR) | Max (EUR) | National Average (EUR) |
|---|---|---|---|
| Pre-operative diagnostic tests | 380 | 380 | 380 |
| Surgery | - | - | - |
| Materials | 38 | 80 | 65 |
| Personnel costs | 293 | 931 | 638 |
| Drugs | 189 | 199 | 193 |
| Operating room | 1684 | 3958 | 2622 |
| VNS device | 21,084 | 21,084 | 21,084 |
| Total cost of intervention | 23,288 | 26,252 | 24,602 |
| Total cost of intervention without VNS device | 2204 | 5168 | 3518 |
| Inpatient | - | - | - |
| Hospital stay | 1067 | 1869 | 1572 |
| Inpatient drugs | - | 5 | 3 |
| Personnel costs for inpatient | 233 | 392 | 339 |
| Other (e.g., perfusion) | 27 | 27 | 27 |
| Total cost of inpatient | 1327 | 2293 | 1941 |
| Total cost of VNS implantation stage without pre-operative tests | 24,615 | 28,545 | 26,543 |
| TOTAL COST OF VNS IMPLANT | 24,995 | 28,925 | 26,923 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marras, C.E.; Colicchio, G.; De Palma, L.; De Benedictis, A.; Di Gennaro, G.; Cavaliere, M.; Cesaroni, E.; Consales, A.; Asioli, S.; Caulo, M.; et al. Health Technology Assessment Report on Vagus Nerve Stimulation in Drug-Resistant Epilepsy. Int. J. Environ. Res. Public Health 2020, 17, 6150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176150
Marras CE, Colicchio G, De Palma L, De Benedictis A, Di Gennaro G, Cavaliere M, Cesaroni E, Consales A, Asioli S, Caulo M, et al. Health Technology Assessment Report on Vagus Nerve Stimulation in Drug-Resistant Epilepsy. International Journal of Environmental Research and Public Health. 2020; 17(17):6150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176150
Chicago/Turabian StyleMarras, Carlo Efisio, Gabriella Colicchio, Luca De Palma, Alessandro De Benedictis, Giancarlo Di Gennaro, Marilou Cavaliere, Elisabetta Cesaroni, Alessandro Consales, Sofia Asioli, Massimo Caulo, and et al. 2020. "Health Technology Assessment Report on Vagus Nerve Stimulation in Drug-Resistant Epilepsy" International Journal of Environmental Research and Public Health 17, no. 17: 6150. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176150