Perceived Severity and Susceptibility towards Leptospirosis Infection in Malaysia

 , , , , and
, , , , and 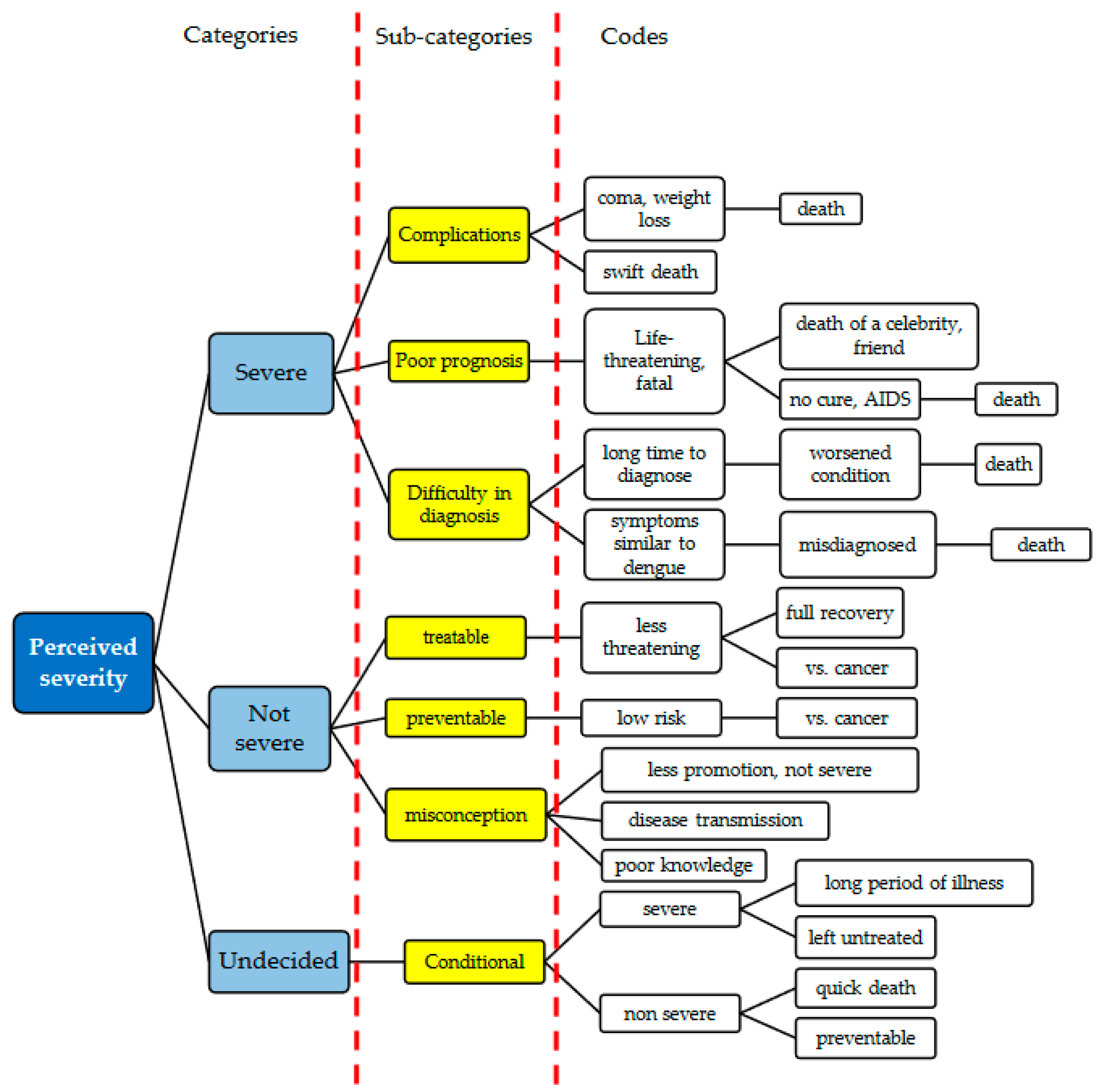{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings
2.2. Study Design
2.3. Study Sample
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Perceived Severity of Leptospirosis
“It is severe because people could die from it. It leads to death, so it is just as dangerous as AIDS. The rat urine disease is categorized as one of the dangerous diseases. The father of my office mate; Linda, died from this disease within a week” (urban)
“This disease can lead to death or comatose. I have seen a patient at the hospital who went from being overweight to extremely skinny” (rural)
“The death of an artist from leptospirosis went viral once. It is indeed dangerous” (urban)
“It takes a very long time to confirm whether it is leptospirosis. One must go to the hospital for a blood test, then monitor the progress, watch for symptoms at home, and wait for the laboratory results. The detection occurs quite late, and meanwhile, patient health worsens. So yes, it can lead to death” (urban)
“I give a score of 2 because we know how to prevent it and thus can be more careful about it” (urban)
“I give it a score of 5. Leptospirosis is 80% treatable” (urban)
“I give it a score of 5. It is not that dangerous. I mean, compared to cancer, it is not that serious” (urban)
“It is not like cancer that can suddenly appear in our body without us knowing if or when we will get it. But leptospirosis can be prevented right from the beginning” (urban)
“If it is not dangerous, there would not be any campaigns to remind the public. However, if it is dangerous, campaigns would be in place. The Ministry of Health does not seem to highlight leptospirosis much” (rural)
“I think leptospirosis is the most dangerous disease because people can die from it and because the parasite comes from the mosquitoes that are present everywhere (in the bushes, woods, and house). It can bite animals like rats that can bite us, humans. So, if we get a fever, we might have leptospirosis” (urban)
“My score on the fear scale is 5. I cannot give a ten because I do not know much about the disease [laugh]” (rural)
“If a person dies straight away, then it is not dangerous. But if a person remains ill for a long time, it is scarier” (rural)
“I give a score of 5–6 if it is preventable. But if one does not seek any treatment for it, then I give it a 10 in terms of severity” (urban)
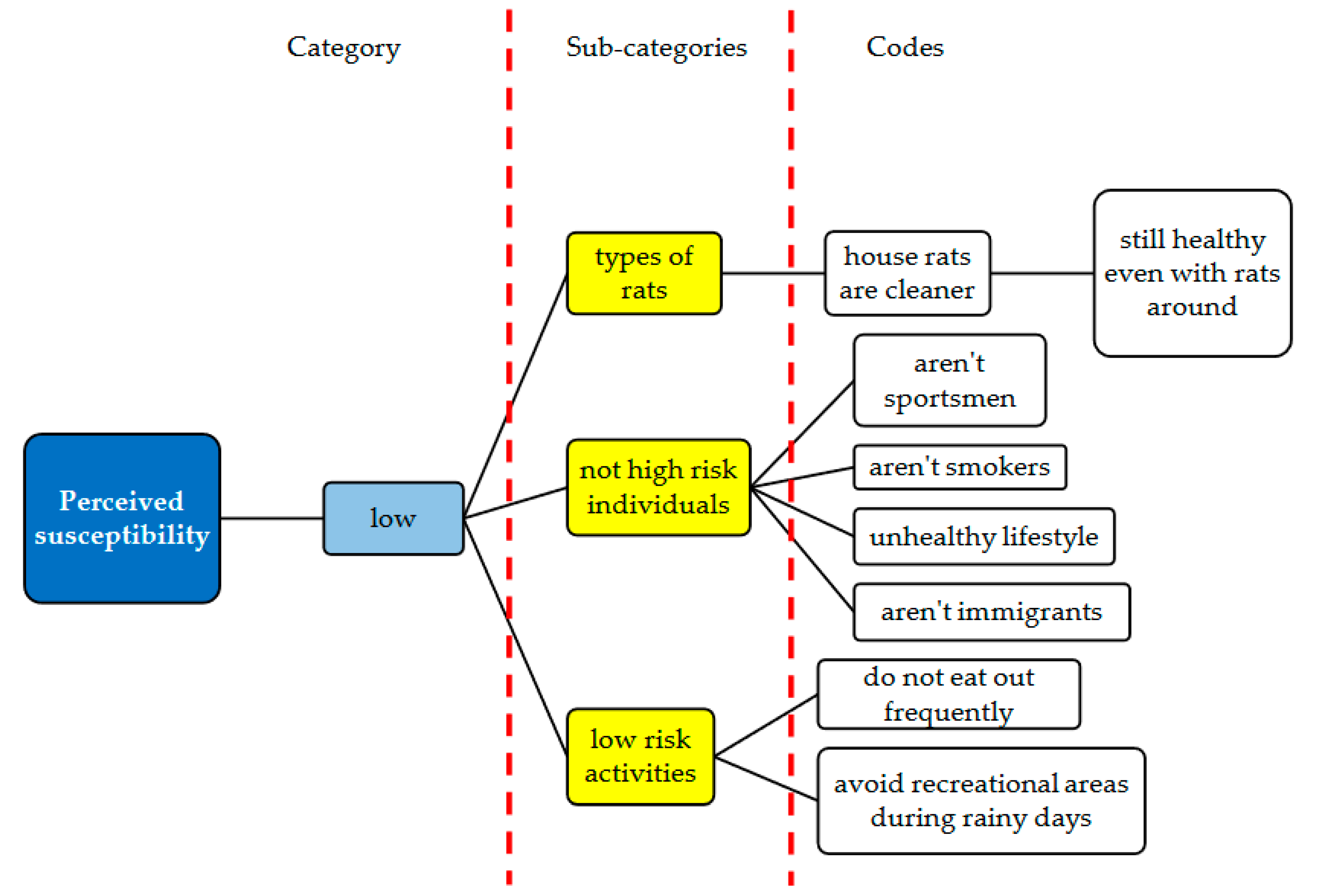
3.2. Perceived Susceptibility towards Leptospirosis
“The disease is only present in the marketplace. I have rats in my house that urinate everywhere; however, it has been three years, and I’m still fine, which means that the urine of house rats has no germs and is not dangerous” (rural)
“To my knowledge, sports enthusiasts were the ones commonly infected by this disease” (urban)
“In my opinion, people who are at risk of this disease are those who practiced unhealthy lifestyle such as smoking and preferred to eat outside where food hygiene is not guaranteed. We must also be careful with the selection of the recreational areas that we visited to prevent exposure to infection. Pay attention to the media and should be aware of the places and avoid going to these places especially when it rains” (rural)
“I believe that the immigrants are more prone to leptospirosis infection because they eat and simply throw away their food waste; this can lead to rat infestation” (urban)
“I regularly wash my hands, but the garbage disposal is poorly managed, and there are house pests everywhere. The children, they love to play in water puddles when it rains. All these are very risky, and we are all at risk” (urban)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rosenstock, I.M. The Health Belief Model and preventive health behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and HEALTH Education: Theory, Research, and Practice; John Wiley & Sons: San Francisco, CA, USA, 2008. [Google Scholar]
- Champion, V.; Skinner, C. The Health Belief Model. In Health Behavior and Health Education: Theory, Research, and Practice; John Wiley & Sons: San Francisco, CA, USA, 2008; Chapter 3. [Google Scholar]
- Paige, S.R.; Bonnar, K.K.; Black, D.R.; Coster, D.C. Risk factor knowledge, perceived threat, and protective health behaviors: Implications for type 2 diabetes control in rural communities. Diabetes Educ. 2018, 44, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Soelar, S.A.; Mohd, S.M.; Hussin, N.; Cheah, W.K.; Verasahib, K.; Goh, P.P. Leptospirosis incidence and mortality in Malaysia. Southeast Asian J. Trop. Med. Public Health 2016, 47, 434. [Google Scholar] [PubMed]
- Stull, J.W.; Peregrine, A.S.; Sargeant, J.M.; Weese, J.S. Household knowledge, attitudes and practices related to pet contact and associated zoonoses in Ontario, Canada. BMC Public Health 2012, 12, 553. [Google Scholar] [CrossRef] [Green Version]
- Abdullah, N.M.; Zahiruddin, W.; Nazri, M.; Sukeri, S.; Idris, Z.; Arifin, W.N.; Nozmi, N.; Saudi, S.N.S.; Samsudin, S.; Zainudin, A.-W. Leptospirosis and its prevention: Knowledge, attitude and practice of urban community in Selangor, Malaysia. BMC Public Health 2019, 19, 628. [Google Scholar] [CrossRef] [Green Version]
- Nozmi, N.; Samsudin, S.; Sukeri, S.; Nazri, M.S.; Zahiruddin, W.M.; Idris, Z.; Arifin, W.; Idris, N.; Saudi, S.; Abdullah, N. Low levels of Knowledge, attitudes and preventive practices on leptospirosis among a rural Community in Hulu Langat District, Selangor, Malaysia. Int. J. Environ. Res. Public Health 2018, 15, 693. [Google Scholar] [CrossRef] [Green Version]
- Latimaha, R.; Bahari, Z.; Ismail, N.A. Factors Influencing the Basic Needs Budget Among the Middle Income Earners in Selected Major Cities in Malaysia (Faktor-faktor yang Mempengaruhi Belanjawan Keperluan Asas dalam kalangan Kumpulan Berpendapatan Menengah di Bandar Utama Terpilih Malaysia). J. Ekon. Malays. 2018, 52, 29–40. [Google Scholar]
- Sakinah, S.; Suhailah, S.; Jamaluddin, T.; Norbaya, S.; Malina, O. Seroprevalence of leptospiral antibodies and knowledge, attitude and practices of leptospirosis to non-high risk group in Selangor. Int. J. Public Health Clin. Sci. 2015, 2, 92–104. [Google Scholar]
- Rahim, S.; Aziah, B.; Nazri, M.; Azwany, Y.; Habsah, H. Town service workers’ knowledge, attitude and practice towards Leptospirosis. Brunei Darussalam J. Health 2012, 5, 1–12. [Google Scholar]
- Azfar, Z.; Nazri, M.; Rusli, M.; Maizurah, O.; Zahiruddin, W.; Azwany, N.; Nabilah, I.; Asma, S.; Aziah, B. Knowledge, attitude and practice about leptospirosis prevention among town service workers in northeastern Malaysia: A cross-sectional study. J. Prev. Med. Hyg. 2018, 59, E92. [Google Scholar]
- Sukeri, S.; Idris, Z.; Zahiruddin, W.M.; Shafei, N.M.; Idris, N.; Hamat, R.A.; Jamaluddin, T.Z.T.; Osman, M.; Wahab, Z.A.; Daud, A. A qualitative exploration of the misconceptions, knowledge gaps and constructs of leptospirosis among rural and urban communities in Malaysia. PLoS ONE 2018, 13, e0200871. [Google Scholar] [CrossRef] [PubMed]
- Molineri, A.I.; Signorini, M.L.; Tarabla, H.D. Knowledge of zoonoses transmission routes and of the species concerned among rural workers. Rev. Argent. Microbiol. 2013, 46, 7–13. [Google Scholar]
- Iriyama, S.; Nakahara, S.; Jimba, M.; Ichikawa, M.; Wakai, S. AIDS health beliefs and intention for sexual abstinence among male adolescent students in Kathmandu, Nepal: A test of perceived severity and susceptibility. Public Health 2007, 121, 64–72. [Google Scholar] [CrossRef]
- Sharifabad, M.; Rouhani Tonekaboni, N. Perceived severity and susceptibility of diabetes complications and its relation to self-care behaviors among diabetic patients. Armaghane Danesh 2007, 12, 59–68. [Google Scholar]
- van der Snoek, E.M.; de Wit, J.B.; Götz, H.M.; Mulder, P.G.; Neumann, M.H.; van der Meijden, W.I. Incidence of sexually transmitted diseases and HIV infection in men who have sex with men related to knowledge, perceived susceptibility, and perceived severity of sexually transmitted diseases and HIV infection: Dutch MSM–cohort study. Sex. Transm. Dis. 2006, 33, 193–198. [Google Scholar] [CrossRef]
- Daniel, M.; Messer, L.C. Perceptions of disease severity and barriers to self-care predict glycemic control in Aboriginal persons with type 2 diabetes mellitus. Chronic Dis. Inj. Can. 2002, 23, 130. [Google Scholar]
- Gracia, E.; García, F.; Lila, M. Public responses to intimate partner violence against women: The influence of perceived severity and personal responsibility. Span. J. Psychol. 2009, 12, 648–656. [Google Scholar] [CrossRef]
- Wahab, Z.A. Epidemiology and current situation of leptospirosis in Malaysia. In Proceedings of the Local Authority Conference on Environmental Health, Labuan, Malaysia, 8–9 September 2015. [Google Scholar]
- Stycos, J.M. A critique of focus group and survey research: The Machismo case. Stud. Fam. Plan. 1981, 12, 450–456. [Google Scholar] [CrossRef]
- Carlsen, B.; Glenton, C. What about N? A methodological study of sample-size reporting in focus group studies. BMC Med. Res. Methodol. 2011, 11, 26. [Google Scholar] [CrossRef] [Green Version]
- Weber, R.P. Basic Content Analysis; Sage: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Morse, J.M. Confusing categories and themes. Qual. Health Res. 2008, 18, 727–728. [Google Scholar] [CrossRef]
- Allwood, P.; Muñoz-Zanzi, C.; Chang, M.; Brown, P.D. Knowledge, perceptions, and environmental risk factors among Jamaican households with a history of leptospirosis. J. Infect. Public Health 2014, 7, 314–322. [Google Scholar] [CrossRef] [Green Version]
- Della, L.J. Exploring diabetes beliefs in at-risk Appalachia. J. Rural Health 2011, 27, 3–12. [Google Scholar] [CrossRef]
- Kasperson, J.X.; Kasperson, R.E.; Pidgeon, N.; Slovic, P. The Social Amplification of Risk: Assessing Fifteen Years of Research and Theory, 1st ed.; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Berry, T.R.; Wharf-Higgins, J.; Naylor, P.J. SARS wars: An examination of the quantity and construction of health iInformation in the news media. Health Commun. 2007, 21, 35–44. [Google Scholar] [CrossRef]
- Young, M.E.; Norman, G.R.; Humphreys, K.R. Medicine in the popular press: The influence of the media on perceptions of disease. PLoS ONE 2008, 3, e3552. [Google Scholar] [CrossRef]
- Frost, K.; Frank, E.; Maibach, E. Relative risk in the news media: A quantification of misrepresentation. Am. J. Public Health 1997, 87, 842–845. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia. Malaysia Dengue Incidence Rate and Case Fatality Rate for Year 2000–2016. Available online: http://idengue.remotesensing.gov.my/idengue/content/statistik.pdf (accessed on 18 May 2017).
- Petrie, K.; Weinman, J. Why illness perceptions matter. Clin. Med. 2006, 6, 536–539. [Google Scholar] [CrossRef]
- Kasmaei, P.; Amin Shokravi, F.; Hidarnia, A.; Hajizadeh, E.; Atrkar-Roushan, Z.; Karimzadeh Shirazi, K.; Montazeri, A. Brushing behavior among young adolescents: Does perceived severity matter. BMC Public Health 2014, 14, 8. [Google Scholar] [CrossRef] [Green Version]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Bond, L.; Nolan, T. Making sense of perceptions of risk of diseases and vaccinations: A qualitative study combining models of health beliefs, decision-making and risk perception. BMC Public Health 2011, 11, 943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosca, L.; Ferris, A.; Fabunmi, R.; Robertson, R.M. Tracking women’s awareness of heart disease: An American Heart Association national study. Circulation 2004, 109, 573–579. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, S.; Ainsworth, B.E.; LaMonte, M.J.; DuBose, K.D. Worry regarding major diseases among older African-American, Native-American, and Caucasian women. Women Health 2002, 36, 83–99. [Google Scholar] [CrossRef] [PubMed]
- DiLorenzo, T.A.; Schnur, J.; Montgomery, G.H.; Erblich, J.; Winkel, G.; Bovbjerg, D.H. A model of disease-specific worry in heritable disease: The influence of family history, perceived risk and worry about other illnesses. J. Behav. Med. 2006, 29, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; O’Neill, S.M.; Rothrock, N.; Gramling, R.; Sen, A.; Acheson, L.S.; Rubinstein, W.S.; Nease, D.E., Jr.; Ruffin, M.T. Comparison of risk perceptions and beliefs across common chronic diseases. Prev. Med. 2009, 48, 197–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmón-Mulanovich, G.; Powell, A.R.; Hartinger-Peña, S.M.; Schwarz, L.; Bausch, D.G.; Paz-Soldán, V.A. Community perceptions of health and rodent-borne diseases along the Inter-Oceanic Highway in Madre de Dios, Peru. BMC Public Health 2016, 16, 755. [Google Scholar] [CrossRef] [PubMed] [Green Version]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sukeri, S.; Zahiruddin, W.M.; Shafei, M.N.; Hamat, R.A.; Osman, M.; Jamaluddin, T.Z.M.T.; Daud, A.B. Perceived Severity and Susceptibility towards Leptospirosis Infection in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 6362. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176362
Sukeri S, Zahiruddin WM, Shafei MN, Hamat RA, Osman M, Jamaluddin TZMT, Daud AB. Perceived Severity and Susceptibility towards Leptospirosis Infection in Malaysia. International Journal of Environmental Research and Public Health. 2020; 17(17):6362. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176362
Chicago/Turabian StyleSukeri, Surianti, Wan Mohd Zahiruddin, Mohd Nazri Shafei, Rukman Awang Hamat, Malina Osman, Tengku Zetty Maztura Tengku Jamaluddin, and Aziah Binti Daud. 2020. "Perceived Severity and Susceptibility towards Leptospirosis Infection in Malaysia" International Journal of Environmental Research and Public Health 17, no. 17: 6362. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176362