The Relationship between Positive Youth Development and Depressive Symptoms among Chinese Early Adolescents: A Three-Year Cross-Lagged Analysis

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedure
2.3. Measurements
2.3.1. Chinese Positive Youth Development Scale
2.3.2. Center for Epidemiologic Studies Depression Scale
2.4. Statistical Analysis
3. Results
3.1. Descriptions of PYD Correlates and Depressive Symptoms between Retained and Dropped Participants
3.2. The Development Trend of Depressive Symptoms and PYD
3.3. Correlations between the Four Second-Order PYD Constructs and Depressive Symptoms
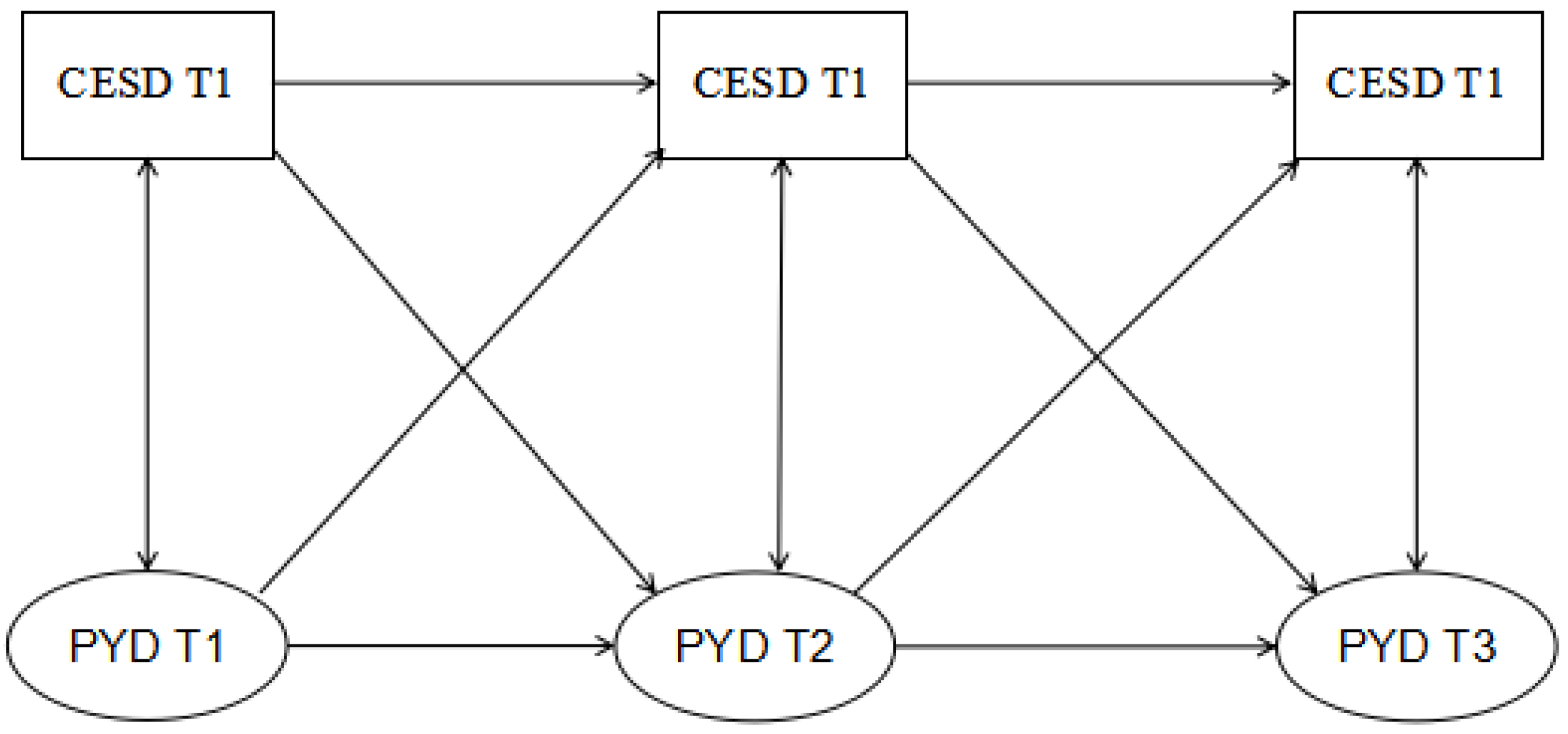
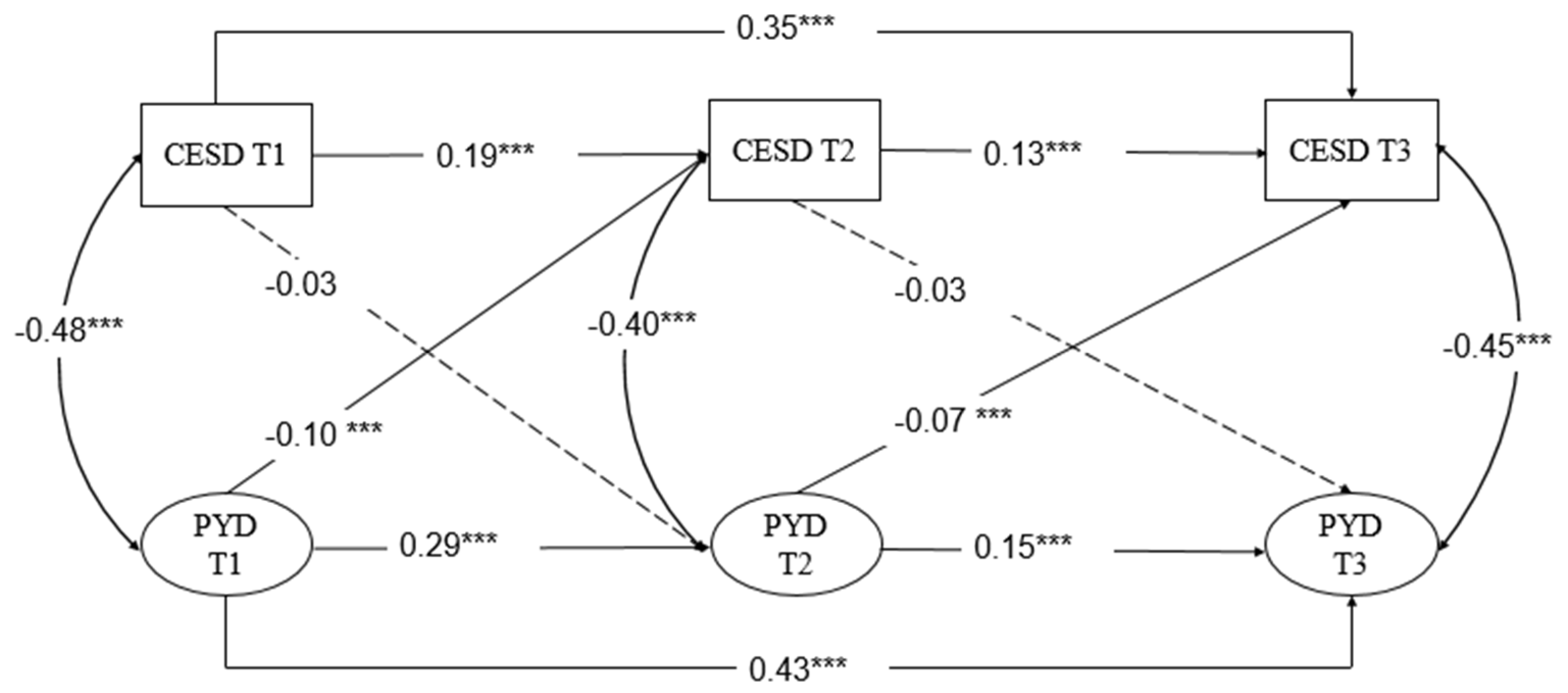
3.4. Cross-Lagged Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kupfer, D.J.; Frank, E.; Phillips, M.L. Major depressive disorder: New clinical, neurobiological, and treatment perspectives. Lancet 2012, 379, 1045–1055. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Tang, S.; Ren, Z.; Wong, D. Prevalence of depressive symptoms among adolescents in secondary school in mainland China: A systematic review and meta-analysis. J. Affect. Disord. 2019, 245, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.H.; Dewa, C.S. Canadian community health survey: Major depressive disorder and suicidality in adolescents. Healthc. Policy 2006, 2, 76. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Walters, E.E. Epidemiology of DSM-III-R major depression and minor depression among adolescents and young adults in the national comorbidity survey. Depress. Anxiety 1998, 7, 3–14. [Google Scholar] [CrossRef]
- Statista. China: Shenzhen City GDP 2018. 2019. Available online: https://www.statista.com/statistics/1025207/china-gdp-of-shenzhen/Schubert (accessed on 1 July 2020).
- Li, H.L.; Zhang, W.X. Adolescent academic stress and depression: Buffering effect of peer support. Chin. Spec. Educ. 2014, 10, 87–91. [Google Scholar]
- Chi, X.; Liu, X.; Huang, Q.; Huang, L.; Zhang, P.; Chen, X. Depression in Chinese adolescents: Prevalence, changes, and social-demographic correlates. J. Affect. Disord. 2020. [Google Scholar] [CrossRef]
- Liu, J.; Bullock, A.; Coplan, R.J.; Chen, X.; Li, D.; Zhou, Y. Developmental cascade models linking peer victimization, depression, and academic achievement in Chinese children. Br. J. Dev. Psychol. 2017, 36, 47–63. [Google Scholar] [CrossRef]
- Dozois, D.J.A.; Dobson, K.S. The Prevention of Anxiety and Depression: Theory, Research, and Practice; American Psychological Association: Washington, DC, USA, 2004; p. 344. [Google Scholar]
- Zubrick, S.R.; Hafekost, J.; Johnson, S.E.; Sawyer, M.G.; Patton, G.; Lawrence, D. The continuity and duration of depression and its relationship to non-suicidal self-harm and suicidal ideation and behavior in adolescents 12–17. J. Affect. Disord. 2017, 220, 49–56. [Google Scholar] [CrossRef]
- Naicker, K.; Galambos, N.L.; Zeng, Y.; Senthilselvan, A.; Colman, I. Social, demographic, and health outcomes in the 10 years following adolescent depression. J. Adolesc. Health 2013, 52, 533–538. [Google Scholar] [CrossRef]
- Mcleod, G.F.H.; Horwood, L.J.; Fergusson, D.M. Adolescent depression, adult mental health and psychosocial outcomes at 30 and 35 years. Psychol. Med. 2016, 46, 1401–1412. [Google Scholar] [CrossRef]
- McWhinnie, C.; Abela, J.R.Z.; Hilmy, N.; Ferrer, I. Positive youth development programs: An alternative approach to the prevention of depression in children and adolescents. In Handbook of Depression in Children and Adolescents; Abela, J.R.Z., Hankin, B.L., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 354–373. [Google Scholar]
- Netherlands, S. Positive youth development program. Encycl. Qual. Life Well Being Res. 2014, 4938. [Google Scholar] [CrossRef]
- Santos, V.; Paes, F.; Pereira, V.; Arias-Carrión, O.; Silva, A.C.; Carta, M.G.; Nardi, A.E.; Machado, S. The role of positive emotion and contributions of positive psychology in depression treatment: Systematic review. Clin. Pract. Epidemiol. Ment. Health 2013, 9, 221–237. [Google Scholar] [CrossRef] [Green Version]
- Bao, Y.; Li, L.; Guan, Y.; Wang, W.; Liu, Y.; Wang, P.; Huang, X.; Tao, S.; Wang, Y. Prevalence and associated positive psychological variables of anxiety and depression among patients with central nervous system tumors in China: A cross-sectional study. Psychooncology 2017, 26, 262–269. [Google Scholar] [CrossRef]
- Pérez-González, A.; Guilera, G.; Pereda, N.; Jarne, A. Protective factors promoting resilience in the relation between child sexual victimization and internalizing and externalizing symptoms. Child Abus. Negl. 2017, 72, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Atkiss, K.; Moyer, M.; Desai, M.; Roland, M. Positive youth development: An integration of the developmental assets theory and the socio-ecological model. Am. J. Health Educ. 2011, 42, 171–180. [Google Scholar] [CrossRef] [Green Version]
- Damon, W. What is positive youth development? Ann. Am. Acad. Political Soc. Sci. 2004, 591, 13–24. [Google Scholar] [CrossRef]
- Roth, J.L.; Brooks-Gunn, J. Youth development programs: Risk, prevention and policy. J. Adolesc. Health 2003, 32, 170–182. [Google Scholar] [CrossRef]
- Lerner, R.M.; Lerner, J.V.; Almerigi, J.B.; Theokas, C.; Phelps, E.; Gestsdottir, S.; Naudeau, S.; Jelicic, H.; Alberts, A.; Ma, L.; et al. Positive youth development, participation community youth development programs, and community contributions of fifith-grade adolescents: Findings from the first wave of 4-H study of positive youth development. J. Early Adolesc. 2005, 25, 17–71. [Google Scholar] [CrossRef]
- Benson, P.L.; Scales, P.C.; Hamilton, S.F.; Sesma, A., Jr. Positive youth development: Theory, research, and applications. In Handbook of Child Psychology, 6th ed.; Volume 1: Theoretical models of human, development; Lerner, R.M., Damon, W., Lerner, R.M., Eds.; Wiley: Hoboken, NJ, USA, 2006; pp. 894–941. [Google Scholar]
- Catalano, R.F.; Berglund, M.L.; Ryan, J.A.; Lonczak, H.S.; Hawkins, J.D. Positive youth development in the United States: Research findings on evaluations of positive youth development programs. Ann. Am. Acad. Political Soc. Sci. 2004, 591, 98–124. [Google Scholar] [CrossRef]
- Bowers, E.P.; Li, Y.; Kiely, M.K.; Brittian, A.; Lerner, J.V.; Lerner, R.M. The five Cs model of positive youth development: A longitudinal analysis of confirmatory factor structure and measurement invariance. J. Youth Adolesc. 2010, 39, 720–735. [Google Scholar] [CrossRef]
- Taylor, R.D.; Oberle, E.; Durlak, J.A.; Weissberg, R.P. Promoting positive youth development through school-based social and emotional learning interventions: A meta-analysis of follow-up effects. Child Dev. 2017, 88, 1156–1171. [Google Scholar] [CrossRef]
- Milot Travers, A.S.; Mahalik, J.R. Positive youth development as a protective factor for adolescents at risk for depression and alcohol use. Appl. Dev. Sci. 2019, 1–10. [Google Scholar] [CrossRef]
- Chi, X.; Huang, L.; Wang, J.; Zhang, P. The Prevalence and Socio-Demographic Correlates of Depressive Symptoms in Early Adolescents in China: Differences in Only Child and Non-Only Child Groups. Int. J. Environ. Res. Public Health 2019, 17, 438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelicic, H.; Bobek, D.L.; Phelps, E.D.; Lerner, R.M.; Lerner, J.V. Using Positive Youth Development to Predict Contribution and Risk Behaviors in Early Adolescence: Findings from the First Two Waves of the 4-H Study of Positive Youth Development. Int. J. Behav. Dev. 2007, 31, 263–273. [Google Scholar] [CrossRef]
- Shek, D.T.; Sun, R.C. Positive youth development (PYD) and adolescent development: Reflection on related research findings and programs. In Student Well-Being in Chinese Adolescents in Hong Kong; Springer: Singapore, 2015; pp. 325–337. [Google Scholar]
- Zhou, Z.; Shek, D.T.L.; Zhu, X.; Dou, D. Positive youth development and adolescent depression: A longitudinal study based on mainland chinese high school students. Int. J. Environ. Res. Public Health 2020, 17, 4457. [Google Scholar] [CrossRef] [PubMed]
- Manna, G.; Falgares, G.; Ingoglia, S.; Como, M.R.; De Santis, S. The relationship between self-esteem, depression and anxiety: Comparing vulnerability and scar model in the Italian context. Mediterr. J. Clin. Psychol. 2016, 4. [Google Scholar] [CrossRef]
- Allemand, M.; Grünenfelder-Steiger, A.E.; Flückiger, C. Scar Model. Encycl. Personal. Individ. Differ. 2020, 4552–4555. [Google Scholar] [CrossRef]
- Del Vecchio, P. The Good News about Preventing Adolescent Depression. Prev. Sci. 2018, 19, 112–114. [Google Scholar] [CrossRef] [Green Version]
- Rohde, P.; Lewinsohn, P.M.; Seeley, J.R. Are people changed by the experience of having an episode of depression? A further test of the scar hypothesis. J. Abnorm. Psychol. 1990, 99, 264–271. [Google Scholar] [CrossRef]
- Deng, H.H.; Chen, H.; Zhong, P.; Liang, Z.B.; Zhang, G.Z. Cross-Lagged Regression Analysis of Relationship between Self-esteem and Depression in Early Adolescents:Test of Vulnerability Model and Scar Model. Psychol. Dev. Educ. 2013, 29, 407–414. (In Chinese) [Google Scholar]
- Derdikman-Eiron, R.U.T.H.; Indredavik, M.S.; Bratberg, G.H.; Taraldsen, G.; Bakken, I.J.; Colton, M. Gender differences in subjective well-being, self-esteem and psychosocial functioning in adolescents with symptoms of anxiety and depression: Findings from the Nord-Trøndelag health study. Scand. J. Psychol. 2011, 52, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, K.D.; Hammen, C.; Burge, D. Interpersonal functioning and depressive symptoms in childhood: Addressing the issues of specificity and comorbidity. J. Abnorm. Child Psychol. 1994, 22, 355. [Google Scholar] [CrossRef] [PubMed]
- Shek, D.T.L.; Siu, A.M.H.; Lee, T.Y. The chinese positive youth development scale: A validation study. Res. Soc. Work Pract. 2007, 17, 380–391. [Google Scholar] [CrossRef]
- Shek, D.T.L.; Ma, C.M.S. Dimensionality of the chinese positive youth development scale: Confirmatory factor analyses. Soc. Indic. Res. 2010, 98, 41–59. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.C.F.; Shek, D.T.L. Life satisfaction, positive youth development, and problem behaviour among chinese adolescents in hong kong. Soc. Indic. Res. 2010, 95, 455–474. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.C.F.; Shek, D.T.L. Positive youth development, life satisfaction and problem behaviour among chinese adolescents in hong kong: A replication. Soc. Indic. Res. 2012, 105, 541–559. [Google Scholar] [CrossRef] [Green Version]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, Z.Y.; Fang, G.; Li, J.; Han, B.X.; Chen, Z.Y. Development of the Chinese age norms of CES-D in urban area. Chin. Ment. Health J. 2010, 24, 139–143. (In Chinese) [Google Scholar]
- Chen, Z.Y.; Yang, X.D.; Li, X.Y. Psychometric features of CES-D in Chinese adolescents. Chin. J. Clin. Psychol. 2009, 17, 443–445. (In Chinese) [Google Scholar]
- Phelps, E.; Zimmerman, S.; Warren, A.E.A.; Jeličić, H.; von Eye, A.; Lerner, R.M. The structure and developmental course of positive youth development (PYD) in early adolescence: Implications for theory and practice. J. Appl. Dev. Psychol. 2009, 30, 571–584. [Google Scholar] [CrossRef]
- Moksnes, U.K.; Moljord, I.E.O.; Espnes, G.A.; Byrne, D.G. The association between stress and emotional states in adolescents: The role of gender and self-esteem. Personal. Individ. Differ. 2010, 49, 430–435. [Google Scholar] [CrossRef]
- Sun, L.P.; Tian, W.W.; Bian, Y.F. Effect of Adolescent Depression and Anxiety on the Development Tendency of Parental Psychological Control: A 3 Years Follow-Up Study. Chin. J. Clin. Psychol. 2018, 26, 730–735. (In Chinese) [Google Scholar]
- Stangor, C.; Walinga, J. 6.3 Adolescence: Developing Independence and Identity. In Introduction to Psychology; Open Textbooks for Hong Kong: Hong Kong, China, 2010; Available online: http://www.opentextbooks.org.hk/ditatopic/26943 (accessed on 3 July 2020).
- Zhang, F.L. Erikson’s Theory of Psychosocial Development. Int. Encycl. Soc. Behav. Sci. 2015, 7, 938–946. [Google Scholar] [CrossRef]
- Salmela-Aro, K. Stages of adolescence. Encycl. Adolesc. 2011, 1, 360–368. [Google Scholar] [CrossRef]
- Canning, J.; Denny, S.; Bullen, P.; Clark, T.; Rossen, F. Influence of positive development opportunities on student well-being, depression and suicide risk: The New Zealand Youth Health and Well-being Survey 2012. Kōtuitui: New Zealand. J. Soc. Sci. Online 2017, 12, 119–133. [Google Scholar] [CrossRef]
- Olson, J.R.; Goddard, H.W. Applying prevention and positive youth development theory to predict depressive symptoms among young people. Youth Soc. 2015, 47, 222–244. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The connor-davidson resilience scale (cd-risc). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Niu, G.F.; Sun, X.J.; Tian, Y.; Fan, C.Y.; Zhou, Z.K. Resilience moderates the relationship between ostracism and depression among Chinese adolescents. Personal. Individ. Differ. 2016, 99, 77–80. [Google Scholar] [CrossRef]
- Yin, H.M.; Niu, X.Q.; Dong, D.; Niu, G.F.; Sun, L.J. The effect of family socioeconomic status on adolescents’ depression: The mediating effect of self-esteem and moderating effect of resilience. Psychol. Res. 2018, 11, 82–88. (In Chinese) [Google Scholar]
- Rutter, M. Resilience: Causal Pathways and Social Ecology. In The Social Ecology of Resilience; Springer: New York, NY, USA, 2012; pp. 33–42. [Google Scholar]
- Khanlou, N.; Wray, R. A whole community approach toward child and youth resilience promotion: A review of resilience literature. Int. J. Ment. Health Addict. 2014, 12, 64–79. [Google Scholar] [CrossRef] [Green Version]
- Waugh, C.E.; Thompson, R.J.; Gotlib, I.H. Flexible emotional responsiveness in trait resilience. Emotion 2011, 11, 1059–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shek, D.T.; Dou, D.; Zhu, X.; Chai, W. Positive youth development: Current perspectives. Adolesc. Health Med. Ther. 2019, 10, 131–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puig-Antich, J.; Lukens, E.P.; Davies, M.; Goetz, D.; Todak, G. Psychosocial functioning in prepubertal major depressive disorders. Arch. Gen. Psychiatry 1985, 42, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, B.C.; Gaudet, C.E.; Dupont-Frechette, J.A.; Tellock, P.P.; Maher, I.D.; Haisley, L.D.; Holler, K.A. Failure to maintain set as a predictor of childhood depression within a children’s psychiatric inpatient sample. Psychiatry Res. 2016, 246, 644–649. [Google Scholar] [CrossRef]
- Martinsen, K.D.; Kendall, P.C.; Stark, K.; Neumer, S.P. Prevention of anxiety and depression in children: Acceptability and feasibility of the transdiagnostic emotion program. Cogn. Behav. Pract. 2016, 23, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Min, J.A.; Jung, Y.E.; Kim, D.J.; Hyeon-Woo, Y. Characteristics associated with low resilience in patients with depression and/or anxiety disorders. Qual. Life Res. 2013, 22, 231–241. [Google Scholar] [CrossRef]
- Reivich, K.; Gillham, J.E.; Chaplin, T.M.; Seligman, M.E.P. From Helplessness to Optimism: The Role of Resilience in Treating and Preventing Depression in Youth. In Handbook of Resilience in Children; Springer: Boston, MA, USA, 2013; pp. 201–214. [Google Scholar] [CrossRef]
- Ge, X.; Natsuaki, M.N.; Conger, R.D. Trajectories of depressive symptoms and stressful life events among, male and female adolescents in divorced and nondivorced families. Dev. Psychopathol. 2016, 18, 253–273. [Google Scholar] [CrossRef]
- HOU, J.; CHEN, Z. The trajectories of adolescent depressive symptoms: Identifying latent subgroups and risk factors. Acta Psychol. Sin. 2016, 48, 957–968. [Google Scholar] [CrossRef]
- De Wilde, E.J.; Kienhorst, C.W.M.; Diekstra, R.F.; Wolters, W.H. Social support, life events, and behavioral characteristics of psychologically distressed adolescents at high risk for attempting suicide. Adolescence 1994, 29, 49. [Google Scholar]
- Vélez, C.E.; Krause, E.D.; McKinnon, A.; Brunwasser, S.M.; Freres, D.R.; Abenavoli, R.M.; Gillham, J.E. Social support seeking and early adolescent depression and anxiety symptoms: The moderating role of rumination. J. Early Adolesc. 2016, 36, 1118–1143. [Google Scholar] [CrossRef] [Green Version]
- Shek, D.T.; Yu, L. Prevention of adolescent problem behavior: Longitudinal impact of the Project P.A.T.H.S. in Hong Kong. Sci. World J. 2011, 11, 546–567. [Google Scholar] [CrossRef] [PubMed]
- Hodge, C.J.; Kanters, M.A.; Forneris, T.; Bocarro, J.N.; Sayre-McCord, R. A Family Thing: Positive Youth Development Outcomes of a Sport-Based Life Skills Program. J. Park Recreat. Adm. 2017, 35, 34–50. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Scales | χ2 | df | CFI | TFI | RMSEA | SRMR | McDonald’s ω | Cronbach’s α | Omega | Avevar |
|---|---|---|---|---|---|---|---|---|---|---|
| CPYD | ||||||||||
| CBC-T1 | 4141.522 | 36 | 0.992 | 0.975 | 0.046 | 0.015 | 0.862 | 0.861 | 0.862 | 0.412 |
| CBC-T2 | 4582.095 | 36 | 0.997 | 0.989 | 0.032 | 0.012 | 0.872 | 0.871 | 0.872 | 0.433 |
| CBC-T3 | 8326.689 | 36 | 0.995 | 0.986 | 0.049 | 0.010 | 0.933 | 0.932 | 0.933 | 0.607 |
| PA-T1 | 1882.882 | 10 | 0.999 | 0.995 | 0.026 | 0.007 | 0.802 | 0.796 | 0.800 | 0.450 |
| PA-T2 | 2110.620 | 15 | 0.998 | 0.993 | 0.028 | 0.007 | 0.785 | 0.780 | 0.780 | 0.420 |
| PA-T3 | 5441.852 | 15 | 0.996 | 0.978 | 0.078 | 0.014 | 0.908 | 0.906 | 0.906 | 0.300 |
| CB-T1a | 3612.898 | 15 | 0.995 | 0.983 | 0.056 | 0.000 | 0.872 | 0.870 | 0.872 | 0.537 |
| CB-T2 | 3872.282 | 15 | 0.992 | 0.970 | 0.077 | 0.014 | 0.882 | 0.881 | 0.882 | 0.558 |
| CB-T3 | 6005.443 | 15 | 0.999 | 0.997 | 0.030 | 0.004 | 0.926 | 0.922 | 0.924 | 0.672 |
| GPYDQ-T1 | 10,425.744 | 190 | 0.933 | 0.917 | 0.059 | 0.042 | 0.914 | 0.913 | 0.913 | 0.346 |
| GPYDQ-T2 | 11,772.895 | 190 | 0.935 | 0.916 | 0.063 | 0.043 | 0.922 | 0.921 | 0.921 | 0.370 |
| GPYDQ-T3 | 19,814.318 | 190 | 0.968 | 0.959 | 0.057 | 0.029 | 0.958 | 0.957 | 0.957 | 0.530 |
| CES-D | ||||||||||
| CES-D-T1 | 8463.780 | 190 | 0.930 | 0.905 | 0.056 | 0.040 | 0.874 | 0.849 | 0.843 | 0.236 |
| CES-D-T2 | 8817.822 | 190 | 0.959 | 0.0942 | 0.045 | 0.029 | 0.878 | 0.853 | 0.847 | 0.243 |
| CES-D-T3 | 12,802.648 | 190 | 0.957 | 0.944 | 0.053 | 0.033 | 0.909 | 0.881 | 0.873 | 0.283 |
| Variable | Follow-up (n = 1301) n/M | %/SD | Loss to Follow-up (n = 243) n/M | %/SD | p |
|---|---|---|---|---|---|
| Gender | 0.12 | ||||
| Male | 666 | 51.2 | 193 | 57.2 | |
| Female | 621 | 47.5 | 104 | 42.8 | |
| Missing data | 14 | 1.1 | _ | _ | |
| Age | 0.01 | ||||
| 11 | 23 | 1.8 | 1 | 0.4 | |
| 12 | 719 | 55.3 | 119 | 49.0 | |
| 13 | 487 | 37.4 | 108 | 44.4 | |
| 14 | 60 | 4.6 | 11 | 4.5 | |
| 15 | 4 | 0.3 | 3 | 1.2 | |
| Missing data | 8 | 0.6 | 1 | 0.4 | |
| CES-D | 13.66 | 9.15 | 15.35 | 9.07 | 0.01 |
| CBC | 4.77 | 0.78 | 3.61 | 0.58 | 0.00 |
| PI | 4.82 | 0.94 | 4.71 | 0.93 | 0.08 |
| PA | 4.11 | 0.74 | 4.06 | 0.74 | 0.35 |
| GPYDQ | 4.85 | 0.71 | 4.84 | 0.69 | 0.76 |
| CES-D M ± SD | CBC M ± SD | PI M ± SD | PA M ± SD | GPYDQ M ± SD | |
|---|---|---|---|---|---|
| T1 | 13.66 ± 9.15 | 4.77 ± 0.78 | 4.82 ± 0.94 | 4.93 ± 0.88 | 4.85 ± 0.71 |
| T2 | 13.76 ± 9.32 | 4.75 ± 0.81 | 4.74 ± 0.98 | 4.93 ± 0.82 | 4.86 ± 0.74 |
| T3 | 12.40 ± 9.31 | 5.03 ± 0.83 | 4.93 ± 0.98 | 5.11 ± 0.87 | 5.10 ± 0.77 |
| F | 12.53 *** | 66.07 *** | 20.03 *** | 26.91 *** | 70.05 *** |
| η2 | 0.01 | 0.05 | 0.01 | 0.02 | 0.05 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. CES-D-T1 | 1.00 | - | |||||||||||||
| 2. CES-D-T2 | 0.25 *** | 1.00 | - | ||||||||||||
| 3. CES-D-T3 | 0.42 *** | 0.25 *** | 1.00 | - | |||||||||||
| 4. CBC-T1 | −0.33 *** | −0.15 *** | −0.22 *** | 1.00 | - | ||||||||||
| 5. PI-T1 | −0.45 *** | −0.19 *** | −0.33 *** | 0.70 *** | 1.00 | - | |||||||||
| 6. PA-T1 | −0.33 *** | −0.15 *** | −0.20 *** | 0.57 *** | 0.64 *** | 1.00 | - | ||||||||
| 7. GPYDQ-T1 | −0.45 *** | −0.17 *** | −0.29 *** | 0.77 *** | 0.72 *** | 0.69 *** | 1.00 | - | |||||||
| 8. CBC-T2 | −0.13 *** | −0.32 *** | −0.14 *** | 0.25 *** | 0.21 *** | 0.18 *** | 0.24 *** | 1.00 | - | ||||||
| 9. PI-T2 | −0.17 *** | −0.40 *** | −0.18 *** | 0.21 *** | 0.24 *** | 0.18 *** | 0.22 *** | 0.74 *** | 1.00 | - | |||||
| 10. PA-T2 | −0.13 *** | −0.30 ** | −0.12 *** | 0.18 *** | 0.18 *** | 0.21 *** | 0.21 *** | 0.60 *** | 0.65 ** | 1.00 | - | ||||
| 11. GPYDQ-T2 | −0.17 *** | −0.41 *** | −0.18 *** | 0.22 *** | 0.23 *** | 0.21 *** | 0.27 *** | 0.78 *** | 0.74 *** | 0.69 *** | 1.00 | - | |||
| 12. CBC-T3 | −0.23 *** | −0.12 *** | −0.44 *** | 0.38 *** | 0.40 *** | 0.30 *** | 0.39 *** | 0.20 *** | 0.20 *** | 0.16 *** | 0.23 *** | 1.00 | - | ||
| 13. PI-T3 | −0.28 *** | −0.17 *** | −0.54 *** | 0.34 *** | 0.43 *** | 0.29 *** | 0.37 *** | 0.21 *** | 0.26 *** | 0.17 *** | 0.24 *** | 0.78 *** | 1.00 | - | |
| 14. PA-T3 | −0.24 *** | −0.14 *** | −0.42 *** | 0.30 *** | 0.37 *** | 0.33 *** | 0.38 *** | 0.16 *** | 0.18 *** | 0.21 *** | 0.22 *** | 0.72 *** | 0.73 *** | 1.00 | - |
| 15. GPYDQ-T3 | −0.29 *** | −0.16 *** | −0.51 *** | 0.36 *** | 0.42 *** | 0.33 *** | 0.44 *** | 0.20 *** | 0.24 *** | 0.21 *** | 0.26 *** | 0.88 *** | 0.81 *** | 0.83 *** | 1.00 |
| 90% CI for RMSEA | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Model | χ2 | df | CFI | SRMR | AIC | BIC | RMSEA | Low | UP |
| baseline model | 1453.87 | 112 | 0.90 | 0.12 | 54,276.85 | 54,559.00 | 0.10 | 0.09 | 0.10 |
| unidirectional model A | 987.98 | 106 | 0.93 | 0.11 | 54,822.95 | 541,27.02 | 0.08 | 0.08 | 0.09 |
| unidirectional model B | 964.16 | 106 | 0.94 | 0.07 | 53,799.13 | 53,915.79 | 0.08 | 0.075 | 0.084 |
| bidirectional model | 1014.02 | 100 | 0.93 | 0.06 | 53,863.00 | 54,203.15 | 0.085 | 0.08 | 0.09 |
| modified model | 821.20 | 98 | 0.95 | 0.04 | 53,672.17 | 54,017.48 | 0.08 | 0.07 | 0.08 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chi, X.; Liu, X.; Huang, Q.; Cui, X.; Lin, L. The Relationship between Positive Youth Development and Depressive Symptoms among Chinese Early Adolescents: A Three-Year Cross-Lagged Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6404. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176404
Chi X, Liu X, Huang Q, Cui X, Lin L. The Relationship between Positive Youth Development and Depressive Symptoms among Chinese Early Adolescents: A Three-Year Cross-Lagged Analysis. International Journal of Environmental Research and Public Health. 2020; 17(17):6404. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176404
Chicago/Turabian StyleChi, Xinli, Xiaofeng Liu, Qiaomin Huang, Xiumin Cui, and Li Lin. 2020. "The Relationship between Positive Youth Development and Depressive Symptoms among Chinese Early Adolescents: A Three-Year Cross-Lagged Analysis" International Journal of Environmental Research and Public Health 17, no. 17: 6404. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176404