Effect of Different Timings of Implant Insertion on the Bone Remodeling Volume around Patients’ Maxillary Single Implants: A 2–3 Years Follow-Up

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.1.1. Inclusion Criteria
- Adult patients (greater than or equal to 18 years);
- Patients underwent single-tooth extraction of the incisor or premolar tooth due to caries, endodontic failure, periodontal disease without reported defect of bony wall;
- Patients underwent immediate or delayed dental implant placement with delayed prosthetic rehabilitation;
- Patients with a full set of preoperative (before tooth extraction) and postoperative 3D imaging.
2.1.2. Exclusion Criteria
- Metal corrupted CBCT scans;
- Patients who had received irradiation and/or bone resection as part of a cancer treatment plan;
- Patients who received bisphosphonates (intravenous and/or oral).
2.2. Surgical Procedure
2.2.1. Immediate Placement
2.2.2. Delayed Placement
2.3. Prosthetic Procedure
2.4. Variables
2.4.1. Anatomical Variables
2.4.2. Primary Predictor Variable
2.4.3. Secondary Predictor Variable
2.4.4. Outcome Variables
2.5. Statistical Analysis
3. Results
3.1. Loading Procedure
3.2. Time of Implant Placement
3.3. Implant position
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Bressan, E.; Grusovin, M.G.; D’Avenia, F.; Neumann, K.; Sbricoli, L.; Luongo, G.; Esposito, M. The influence of repeated abutment changes on peri-implant tissue stability: 3-year post-loading results from a multicentrerandomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 373–390. [Google Scholar] [PubMed]
- Huynh-Ba, G.; Meister, D.J.; Hoders, A.B.; Mealey, B.L.; Mills, M.P.; Oates, T.W.; Cochran, D.L.; Prihoda, T.J.; McMahan, C.A. Esthetic, clinical and patient-centered outcomes of immediately placed implants (Type 1) and early placed implants (Type 2): Preliminary 3-month results of an ongoing randomized controlled clinical trial. Clin. Oral Implants Res. 2016, 27, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Bramanti, E.; Norcia, A.; Cicci, M.; Matacena, G.; Cervino, G.; Troiano, G.; Zhurakivska, K.; Laino, L. Postextraction Dental Implant in the Aesthetic Zone, Socket Shield Technique Versus Conventional Protocol. J.Craniofac. Surg. 2018, 29, 1037–1041. [Google Scholar] [CrossRef] [PubMed]
- Gjelvold, B.; Kisch, J.; Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Clinical and radiographic outcome following immediate loading and delayed loading of single-tooth implants: Randomized clinical trial. Clin. Implant Dent.Relat. Res. 2017, 19, 549–558. [Google Scholar] [CrossRef]
- Testori, T.; Weinstein, T.; Scutellà, F.; Wang, H.L.; Zucchelli, G. Implant placement in the esthetic area: Criteria for positioning single and multiple implants. Periodontol 2000 2018, 77, 176–196. [Google Scholar] [CrossRef]
- Cannizzaro, G.; Felice, P.; Leone, M.; Checchi, V.; Esposito, M. Flapless versus open flap implant surgery in partially edentulous patients subjected to immediate loading: 1-year results from a split-mouth randomised controlled trial. Eur. J. Oral Implantol. 2011, 4, 177–188. [Google Scholar]
- Clementini, M.; Tiravia, L.; De Risi, V.; VittoriniOrgeas, G.; Mannocci, A.; de Sanctis, M. Dimensional changes after immediate implant placement with or without simultaneous regenerative procedures: A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 666–677. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gastaldi, G.; Gherlone, E.F. Buccal-Lingual Bone Remodeling in Immediately Loaded Fresh Socket Implants: A Cone Beam Computed Tomography Study. Int. J. Periodontics Restor. Dent. 2018, 35, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Crespi, R.; Fabris, G.B.M.; Crespi, G.; Toti, P.; Marconcini, S.; Covani, U. Effects of different loading protocols on the bone remodeling volume of immediate maxillary single implants: A 2- to 3-year follow-up. Int. J. Oral Maxillofac. Implants 2019, 34, 953–962. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Martuscelli, R.; Guidetti, F.; Porzio, M.; Sbordone, L. Evaluation of volumetric dimensional changes in posterior extraction sites with and without ARP using a novel imaging device. Clin. Implant Dent. Relat. Res. 2017, 19, 1044–1053. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Martuscelli, R.; Guidetti, F.; Ramaglia, L.; Sbordone, L. Retrospective volume analysis of bone remodeling after tooth extraction with and without deproteinized bovine bone mineral insertion. Clin. Oral Implants Res. 2016, 27, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Capparè, P.; Gherlone, E.F. Electrical mallet in implants placed in fresh extraction sockets with simultaneous osteotome sinus floor elevation. Int. J. Oral Maxillofac. Implants 2013, 28, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Romeo, E.; Lops, D.; Margutti, E.; Ghisolfi, M.; Chiapasco, M.; Vogel, G. Long-term survival and success of oral implants in the treatment of full and partial arches: A 7-year prospective study with the ITI dental implant system. Int. J. Oral Maxillofac. Implants 2004, 19, 247–259. [Google Scholar] [PubMed]
- Guarnieri, R.; Belleggia, F.; Grande, M. Immediate versus Delayed Treatment in the Anterior Maxilla Using Single Implants with a Laser-Microtextured Collar: 3-Year Results of a Case Series on Hard- and Soft-Tissue Response and Esthetics. J. Prosthodont 2016, 25, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Eghbali, A.; De Bruyn, H.; De Rouck, T.; Cleymaet, R.; Wyn, I.; Cosyn, J. Single implant treatment in healing versus healed sites of the anterior maxilla: A clinical and radiographic evaluation. Clin. Implant Dent Relat. Res. 2012, 14, 336–346. [Google Scholar] [CrossRef]
- Den Hartog, L.; Huddleston Slater, J.J.R.; Vissink, A.; Meijer, H.J.A.; Raghoebar, G.M. Treatment outcome of immediate, early and conventional single-tooth implants in the aesthetic zone: A systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. J. Clin. Periodontol. 2008, 35, 1073–1086. [Google Scholar] [CrossRef]
- Schropp, L.; Isidor, F. Timing of implant placement relative to tooth extraction. J. Oral Rehabil. 2008, 35, 33–43. [Google Scholar] [CrossRef]
- Bruschi, E.; Manicone, P.F.; De Angelis, P.; Papetti, L.; Pastorino, R.; D’Addona, A. Comparison of Marginal Bone Loss Around Axial and Tilted Implants: A Retrospective CBCT Analysis of Up to 24 Months. Int. J. Periodontics Restor. Dent. 2019, 39, 675–684. [Google Scholar] [CrossRef]
- Quaranta, A.; Perrotti, V.; Putignano, A.; Malchiodi, L.; Vozza, I.; CalvoGuirado, J.L. Anatomical Remodeling of Buccal Bone Plate in 35 Premaxillary Post-Extraction Immediately Restored Single TPS Implants: 10-Year Radiographic Investigation. Implant Dent. 2016, 25, 186–192. [Google Scholar] [CrossRef]
- Barone, A.; Rispoli, L.; Vozza, I.; Quaranta, A.; Covani, U. Immediate restoration of single implants placed immediately after tooth extraction. J. Periodontol. 2006, 77, 1914–1920. [Google Scholar] [CrossRef]
- Slagter, K.W.; den Hartog, L.; Bakker, N.A.; Vissink, A.; Meijer, H.J.; Raghoebar, G.M. Immediate placement of dental implants in the esthetic zone: A systematic review and pooled analysis. J. Periodontol. 2014, 85, e241–e250. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla—A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29, 186–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mello, C.C.; Lemos, C.A.A.; Verri, F.R.; Dos Santos, D.M.; Goiato, M.C.; Pellizzer, E.P. Immediate implant placement into fresh extraction sockets versus delayed implants into healed sockets: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1162–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellicer-Chover, H.; Peñarrocha-Oltra, D.; Bagán, L.; Fichy-Fernandez, A.J.; Canullo, L.; Peñarrocha-Diago, M. Single-blind randomized clinical trial to evaluate clinical and radiological outcomes after one year of immediate versus delayed implant placement supporting full-arch prostheses. Med. Oral Patol. Oral Cir.Bucal. 2014, 19, e295–e301. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Cortellini, P.; Pellegrini, G.; Nieri, M.; Bonaccini, D.; Allegri, M.; Bouchard, P.; Cairo, F.; Conforti, G.; Fourmousis, I.; et al. Xenogenic collagen matrix or autologous connective tissue graft as adjunct to coronally advanced flaps for coverage of multiple adjacent gingival recession: Randomized trial assessing non-inferiority in root coverage and superiority in oral health-related quality of life. J. Clin. Periodontol. 2018, 45, 78–88. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Procedure | Immediate | Delayed | |||||
|---|---|---|---|---|---|---|---|
| sample size | 9 | 10 | |||||
| genders ratio (male/female) | 3/6 | 4/6 | |||||
| incisor/bicuspid | 5/4 | 6/4 | |||||
| Procedure | Immediate | Delayed | |||||
| Variable | Size | psw | Size | psw | pw Immediate vs. Delayed | ||
| Overall | |||||||
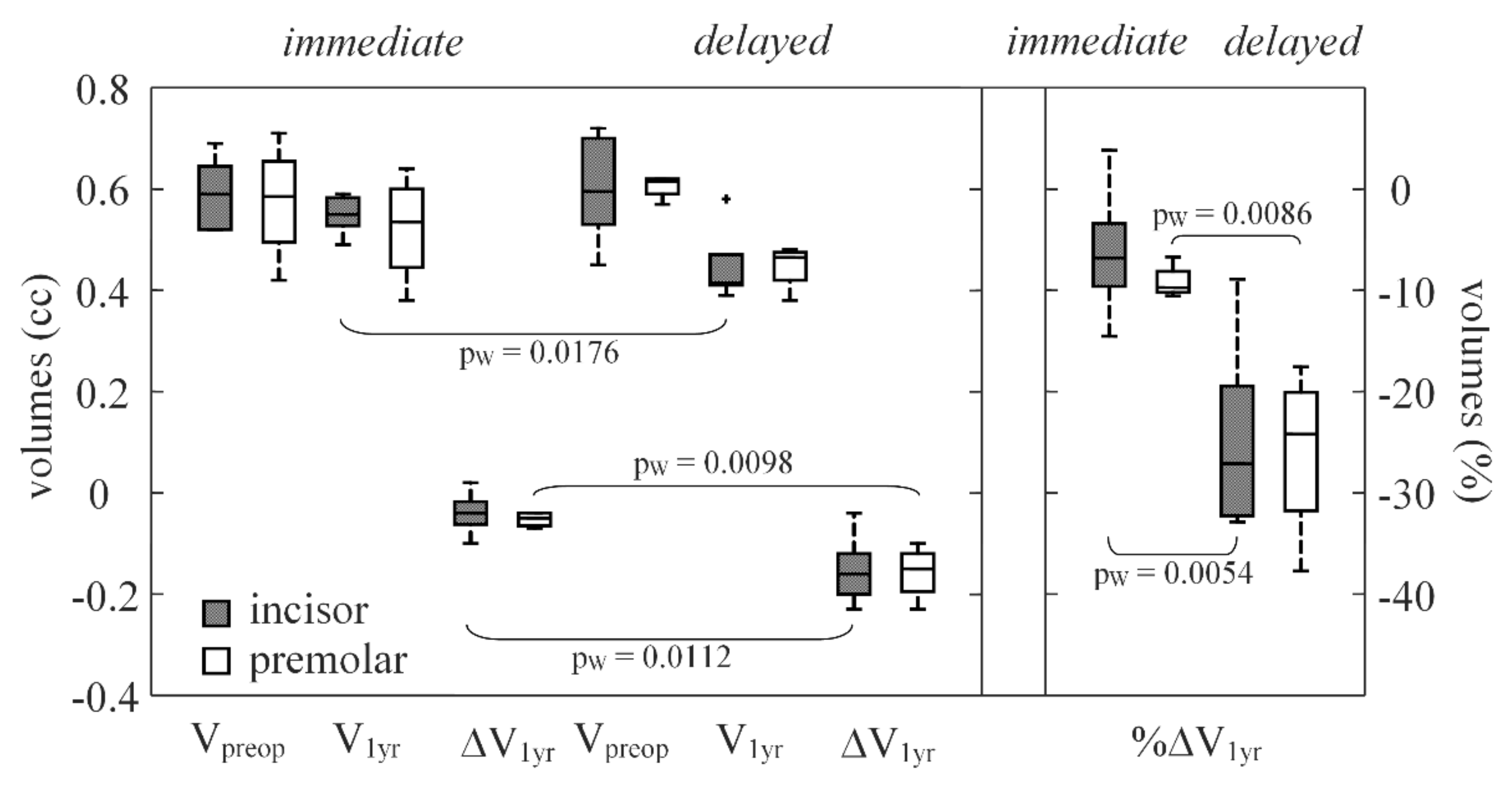
| (mm3) | 9 | 0.59(0.11) | 0.8799 | 10 | 0.61(0.05) | 0.6422 | 0.6526 |
| (mm3) | 9 | 0.54(0.07) | 0.2777 | 10 | 0.44(0.06) | 0.0994 | 0.0084 |
| ΔV (mm3) preop→1 year | 9 | −0.04(0.02) | 0.2282 | 10 | −0.15(0.07) | 0.7607 | 0.0002 |
| %ΔVpreop→1 year | 9 | −7.5(3.1) | 0.0465 | 10 | −24.2(12.0) | 0.8311 | <0.0001 |
| Procedure | Immediate | Delayed | |||||
|---|---|---|---|---|---|---|---|
| sample size | 11 | 11 | |||||
| genders ratio (male/female) | 4/7 | 5/6 | |||||
| incisor/bicuspid | 7/4 | 6/5 | |||||
| Procedure | Immediate | Delayed | |||||
| Variable | Size | psw | Size | psw | pW Immediate vs. Delayed | ||
| Overall | |||||||
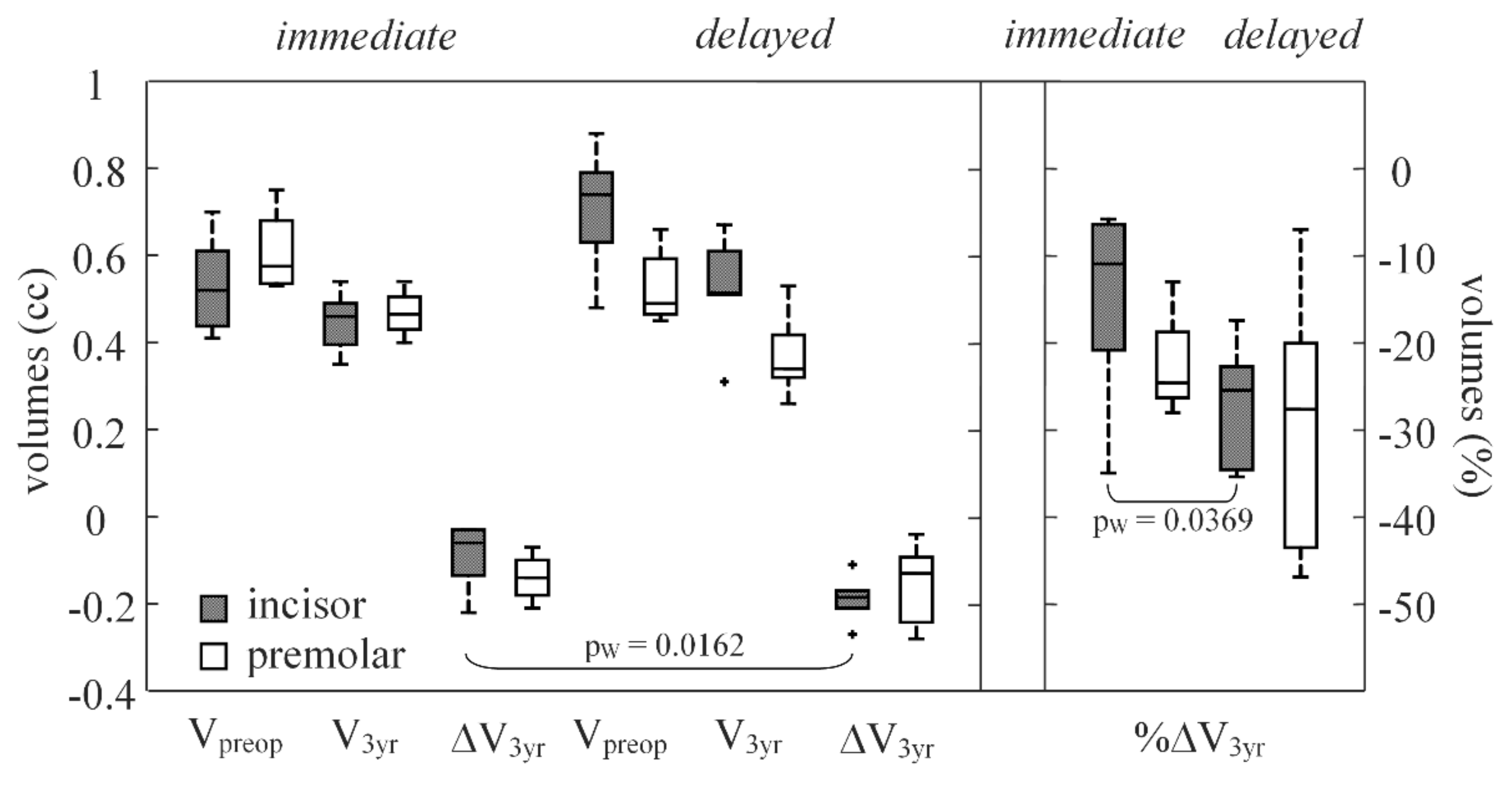
| (mm3) | 11 | 0.54(0.12) | 0.7472 | 11 | 0.63(0.26) | 0.3601 | 0.2297 |
| (mm3) | 11 | 0.46(0.09) | 0.6381 | 11 | 0.51(0.19) | 0.4537 | 0.9676 |
| ΔV (mm3) preop→3 year | 11 | −0.07(0.11) | 0.0452 | 11 | −0.18(0.10) | 0.8955 | 0.035 |
| %ΔVpreop→3 year | 11 | −14.6(15.5) | 0.3206 | 11 | −27.1(11.7) | 0.9334 | 0.0291 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menchini-Fabris, G.B.; Toti, P.; Crespi, G.; Covani, U.; Furlotti, L.; Crespi, R. Effect of Different Timings of Implant Insertion on the Bone Remodeling Volume around Patients’ Maxillary Single Implants: A 2–3 Years Follow-Up. Int. J. Environ. Res. Public Health 2020, 17, 6790. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186790
Menchini-Fabris GB, Toti P, Crespi G, Covani U, Furlotti L, Crespi R. Effect of Different Timings of Implant Insertion on the Bone Remodeling Volume around Patients’ Maxillary Single Implants: A 2–3 Years Follow-Up. International Journal of Environmental Research and Public Health. 2020; 17(18):6790. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186790
Chicago/Turabian StyleMenchini-Fabris, Giovanni Battista, Paolo Toti, Giovanni Crespi, Ugo Covani, Luca Furlotti, and Roberto Crespi. 2020. "Effect of Different Timings of Implant Insertion on the Bone Remodeling Volume around Patients’ Maxillary Single Implants: A 2–3 Years Follow-Up" International Journal of Environmental Research and Public Health 17, no. 18: 6790. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186790