Association between Primary Healthcare and Medical Expenditures in a Context of Hospital-Oriented Healthcare System in China: A National Panel Dataset, 2012–2016

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Resource and Variables
2.2.1. Dependent Variables
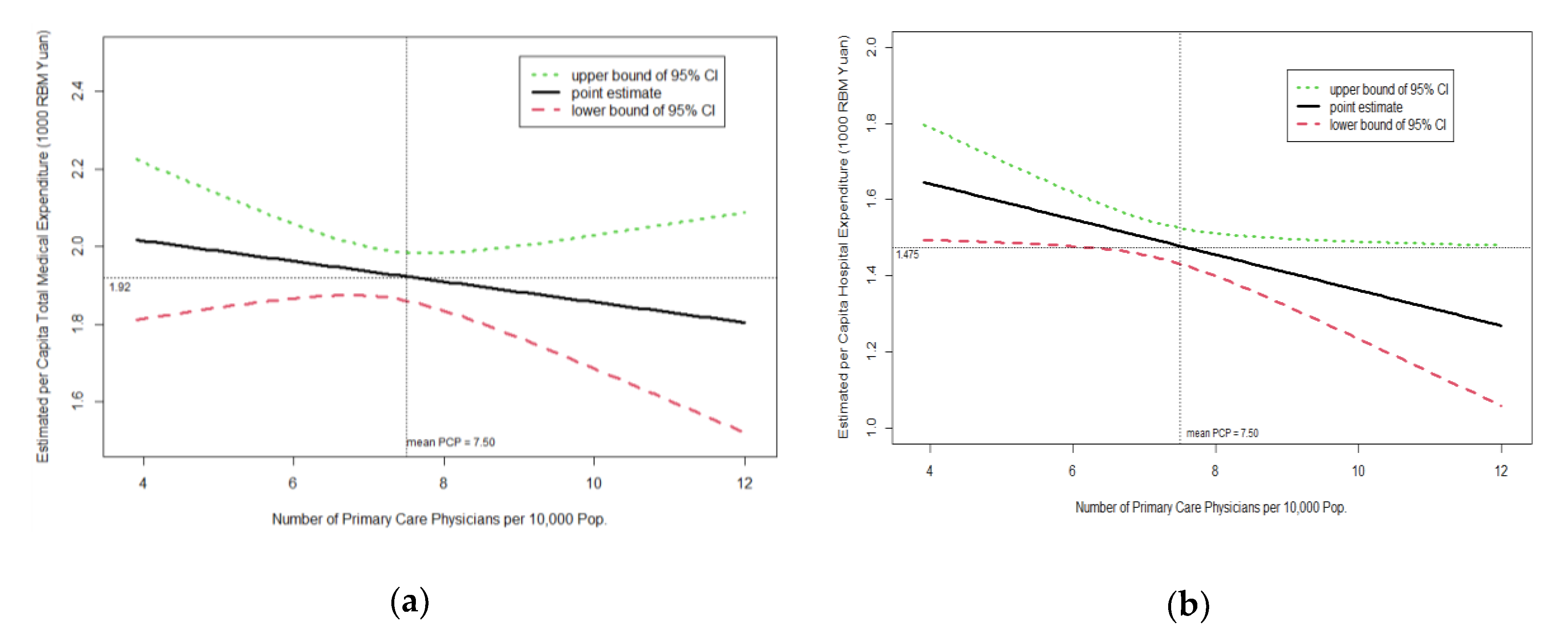
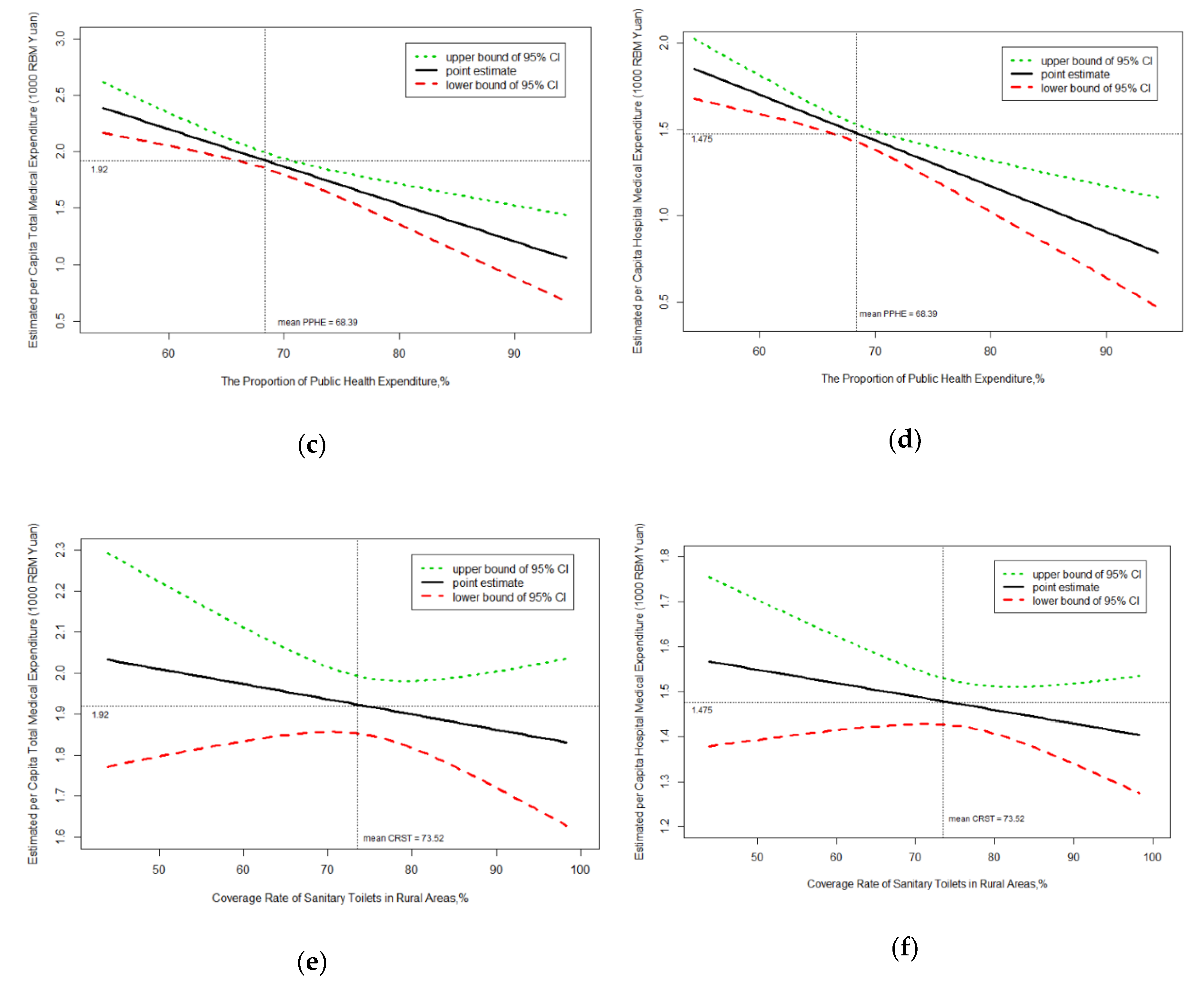
2.2.2. Exposures
2.2.3. Covariates
2.3. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lu, C.; Schneider, M.T.; Gubbins, P.; Leach-Kemon, K.; Jamison, D.; Murray, C.J.L. Public financing of health in developing countries: A cross-national systematic analysis. Lancet 2010, 375, 1375–1387. [Google Scholar] [CrossRef]
- WHO. Global Spending on Health: A World in Transition; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Zhai, T.; Goss, J.; Li, J. Main drivers of health expenditure growth in China: A decomposition analysis. BMC Health Serv. Res. 2017, 17, 185. [Google Scholar] [CrossRef] [Green Version]
- National Health Commission. Statistical Bulletin on the Development of Health Services in China. 2018. Available online: http://www.nhc.gov.cn/guihuaxxs/s10748/201905/9b8d52727cf346049de8acce25ffcbd0.shtml (accessed on 7 May 2020). (In Chinese)
- National Health Commission. Statistical Bulletin on the Development of Health Services in China. 2010. Available online: http://www.nhc.gov.cn/mohwsbwstjxxzx/s7967/201104/51512.shtml (accessed on 7 May 2020). (In Chinese)
- Zhai, T.; Goss, J.; Dmytraczenko, T.; Zhang, Y.; Li, J.; Chai, P. China’s Health Expenditure Projections To 2035: Future Trajectory and The Estimated Impact of Reforms. Health Aff. 2019, 38, 835–843. [Google Scholar] [CrossRef]
- Tang, S.; Tao, J.; Bekedam, H. Controlling cost escalation of healthcare: Making universal health coverage sustainable in China. BMC Public Health 2012, 12, S8. [Google Scholar] [CrossRef] [Green Version]
- Marten, R.; McIntryre, D.; Travassos, C.; Shishkin, S.; Longde, W.; Reddy, K.S.; Vega, J. An assessment of progress towards universal health coverage in Brazil, Russia, India, China, and South Africa (BRICS). Lancet 2014, 384, 2164–2171. [Google Scholar] [CrossRef] [Green Version]
- Stefanini, A.; Aloini, D.; Benevento, E.; Dulmin, R.; Mininno, V. A data-driven methodology for supporting resource planning of health services. Socio-Economic Plan. Sci. 2020, 70, 100744. [Google Scholar] [CrossRef]
- Guo, Y.; Sun, S. Revival of primary health care to realize universal health coverage and sustainable development goals: Viewing the progress of primary health care from Declaration of Alma-Ata and Declaration of Astana. Chin. Rural Health Serv. Adm. 2019, 39, 7–11. [Google Scholar]
- WHO. Building the Economic Case for Primary Health Care: A Scoping Review; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Ayanian, J.Z.; Hamel, M.B. Transforming Primary Care—We Get What We Pay For. N. Engl. J. Med. 2016, 374, 2390–2392. [Google Scholar] [CrossRef]
- WHO. Declaration of Alma-Ata; World Health Organization: Geneva, Switzerland, 1978. [Google Scholar]
- WHO. The World Health Report 2008—Primary Health Care: Now More than Ever; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Friedrich, M. Declaration of Astana Emphasizes Primary Care as Key to World Health. JAMA 2018, 320, 2412. [Google Scholar] [CrossRef]
- WHO. A Vision for Primary Health Care in the 21st Century: Towards Universal Health Coverage and the Sustainable Development Goals; World Health Organization and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2018. [Google Scholar]
- Basu, S.; Berkowitz, S.A.; Phillips, R.L.; Bitton, A.; Landon, B.E.; Phillips, R.S. Association of Primary Care Physician Supply With Population Mortality in the United States, 2005–2015. JAMA Intern. Med. 2019, 179, 506. [Google Scholar] [CrossRef]
- Fairall, L.R.; Bateman, E.; Cornick, R.; Faris, G.; Timmerman, V.; Folb, N.; Bachmann, M.O.; Zwarenstein, M.; Smith, R. Innovating to improve primary care in less developed countries: Towards a global model. BMJ Innov. 2015, 1, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Atun, R. What Are the Advantages and Disadvantages of Restructuring a Health Care System to Be More Focused on Primary Care Services? WHO Regional Office for Europe’s Health Evidence Network: Copenhagen, Denmark, 2004. [Google Scholar]
- Kruk, M.E.; Porignon, D.; Rockers, P.C.; Van Lerberghe, W. The contribution of primary care to health and health systems in low- and middle-income countries: A critical review of major primary care initiatives. Soc. Sci. Med. 2010, 70, 904–911. [Google Scholar] [CrossRef] [Green Version]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of Primary Care to Health Systems and Health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef]
- Li, H.; Gu, J.; Qiao, Y.; Liu, K.; Zhang, Y.; Sun, X. The development and impact of primary health care in China from 1949 to 2015: A focused review. Int. J. Health Plan. Manag. 2017, 32, 339–350. [Google Scholar] [CrossRef]
- Macinko, J.; Starfield, B.; Shi, L. The Contribution of Primary Care Systems to Health Outcomes within Organization for Economic Cooperation and Development (OECD) Countries, 1970–1998. Health Serv. Res. 2003, 38, 831–865. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Lu, J.; Hu, S.; Cheng, K.K.; De Maeseneer, J.; Meng, Q.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.; et al. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- Yip, W.C.-M.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of the People’s Republic of China. China Statistical Yearbook on Health 2019; China Union Medical College Publishing House: Beijing, China, 2019. (In Chinese) [Google Scholar]
- State Council. Guidance of the State Council on Establishing the General Practitioner System. 2011. Available online: http://www.nhc.gov.cn/wjw/gfxwj/201304/b77fdc4825954db68bb436276005bba3.shtml (accessed on 7 May 2020). (In Chinese)
- Primary Health Department. Notice on Doing Well the National Basic Public Health Service Program of 2019. Available online: http://www.nhc.gov.cn/jws/s7881/201909/83012210b4564f26a163408599072379.shtml (accessed on 9 May 2020). (In Chinese)
- Souliotis, K.; Kartzi, G.; Athanasakis, K.; Golna, C.; Yfantopoulos, J. Determinants of health care expenditure in Greece: Can primary health care impact on their evolution? Int. J. Pharm. Sci. Res. 2014, 5, 383–391. [Google Scholar]
- Wang, L.; Wang, Z.; Ma, Q.; Fang, G.; Yang, J. The development and reform of public health in China from 1949 to 2019. Glob. Health 2019, 15, 45. [Google Scholar] [CrossRef]
- Hansen, P.; King, A. The determinants of health care expenditure: A cointegration approach. J. Health Econ. 1996, 15, 127–137. [Google Scholar] [CrossRef]
- Kea, X.; Saksenaa, P.; Holly, A. The Determinants of Health Expenditure: A Country-Level Panel Data Analysis; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Matteo, L.D. The macro determinants of health expenditure in the United States and Canada: Assessing the impact of income, age distribution and time. Health Policy 2005, 71, 23–42. [Google Scholar] [CrossRef] [PubMed]
- Baicker, K.; Chandra, A. Medicare Spending, The Physician Workforce, And Beneficiaries’ Quality Of Care. Health Aff. 2004, 23, W4-184. [Google Scholar] [CrossRef] [PubMed]
- Dusheiko, M.; Gravelle, H.; Martin, S.; Rice, N.; Smith, P. Does better disease management in primary care reduce hospital costs? Evidence from English primary care. J. Health Econ. 2011, 30, 919–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diomidous, M.; Gougoumati, K.; Kalokairinou, A. Cost-effectiveness in primary health care in Greece. Stud. Health Technol. Inform. 2013, 190, 225–227. [Google Scholar]
- Starfield, B.; Shi, L. Policy relevant determinants of health: An international perspective. Health Policy 2002, 60, 201–218. [Google Scholar] [CrossRef]
- Davis, K. Slowing the Growth of Health Care Costs—Learning from International Experience. N. Engl. J. Med. 2008, 359, 1751–1755. [Google Scholar] [CrossRef]
- Bertakis, K.D.; Azari, R. Patient-Centered Care is Associated with Decreased Health Care Utilization. J. Am. Board Fam. Med. 2011, 24, 229–239. [Google Scholar] [CrossRef] [Green Version]
- Bertakis, K.D.; Azari, R. Determinants and outcomes of patient-centered care. Patient Educ. Couns. 2011, 85, 46–52. [Google Scholar] [CrossRef]
- Bruin, S.R.; Versnel, N.; Lemmens, L.C.; Molema, C.C.; Schellevis, F.G.; Nijpels, G.; Baan, C.A. Comprehensive care programs for patients with multiple chronic conditions: A systematic literature review. Health Policy 2012, 107, 108–145. [Google Scholar] [CrossRef] [Green Version]
- Forrest, C.B.; Starfield, B. The effect of first-contact care with primary care clinicians on ambulatory health care expenditures. J. Fam. Pract. 1996, 43, 40–48. [Google Scholar]
- Rosano, A.; Loha, C.A.; Falvo, R.; Van Der Zee, J.; Ricciardi, W.; Guasticchi, G.; De Belvis, A.G. The relationship between avoidable hospitalization and accessibility to primary care: A systematic review. Eur. J. Public Health 2012, 23, 356–360. [Google Scholar] [CrossRef] [Green Version]
- Kruk, M.E.; Galea, S.; Prescott, M.; Freedman, L.P. Health care financing and utilization of maternal health services in developing countries. Health Policy Plan. 2007, 22, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Novignon, J.; Olakojo, S.A.; Nonvignon, J. The effects of public and private health care expenditure on health status in sub-Saharan Africa: New evidence from panel data analysis. Health Econ. Rev. 2012, 2, 22. [Google Scholar] [CrossRef] [Green Version]
- Rad, E.H.; Vahedi, S.; Teimourizad, A.; Esmaeilzadeh, F.; Hadian, M.; Pour, A.T. Comparison of the Effects of Public and Private Health Expenditures on the Health Status: A Panel Data Analysis in Eastern Mediterranean Countries. Int. J. Heal. Policy Manag. 2013, 1, 163–167. [Google Scholar] [CrossRef]
- Asiskovitch, S. Gender and health outcomes: The impact of healthcare systems and their financing on life expectancies of women and men. Soc. Sci. Med. 2010, 70, 886–895. [Google Scholar] [CrossRef]
- Bricker, N. Reducing the Geographic Variance in Medical Expenditures: The Benefits of a Primary-Care Oriented Health System. Undergrad. Econ. Rev. 2015, 11, 6. [Google Scholar]
- Fisher, E.S.; Wennberg, D.E.; Stukel, T.A.; Gottlieb, D.J.; Lucas, F.L.; Pinder, É.L. The Implications of Regional Variations in Medicare Spending. Part 1: The Content, Quality, and Accessibility of Care. Ann. Intern. Med. 2003, 138, 273. [Google Scholar] [CrossRef] [Green Version]
- Mark, D.H.; Gottlieb, M.S.; Zellner, B.B.; Chetty, V.K.; Midtling, J.E. Medicare costs in urban areas and the supply of primary care physicians. J. Fam. Pract. 1996, 43, 33–39. [Google Scholar]
- NHFPC. China Statistical Yearbook on Health 2018; China Union Medical College Publishing House: Beijing, China, 2018. (In Chinese) [Google Scholar]
- Cheng, S.; Li, Z.; Uddin, S.M.N.; Mang, H.-P.; Zhou, X.; Zhang, J.; Zheng, L.; Zhang, L. Toilet revolution in China. J. Environ. Manag. 2018, 216, 347–356. [Google Scholar] [CrossRef]
- Han, K.; Cho, M.; Chun, K. Determinants of Health Care Expenditures and the Contribution of Associated Factors: 16 Cities and Provinces in Korea, 2003–2010. J. Prev. Med. Public Health 2013, 46, 300–308. [Google Scholar] [CrossRef]
- Seshamani, M.; Gray, A. Health care expenditures and ageing: An international comparison. Appl. Health Econ. Health Policy 2003, 2, 9–16. [Google Scholar] [PubMed]
- Samadi, A.; Homaie, R.E. Determinants of Healthcare Expenditure in Economic Cooperation Organization (ECO) Countries: Evidence from Panel Cointegration Tests. Int. J. Health Policy Manag. 2013, 1, 63–68. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | 2012 | 2013 | 2014 | 2015 | 2016 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Per capita total medical expenditures (1000 Yuan) | 1.39 | 0.28 | 1.58 | 0.33 | 1.74 | 0.38 | 1.96 | 0.43 | 2.22 | 0.48 |
| Per capita hospital medical expenditures (1000 Yuan) | 1.07 | 0.26 | 1.22 | 0.30 | 1.35 | 0.33 | 1.52 | 0.37 | 1.74 | 0.41 |
| Primary care physicians per 10,000 population | 7.15 | 1.38 | 7.38 | 1.35 | 7.44 | 1.33 | 7.66 | 1.40 | 7.90 | 1.45 |
| The proportion of public health expenditure, % | 65.51 | 7.51 | 66.49 | 7.36 | 68.25 | 7.00 | 70.34 | 6.39 | 71.34 | 6.05 |
| Popularity rate of sanitary toilets in rural areas, % | 68.83 | 13.63 | 71.46 | 13.74 | 73.27 | 13.76 | 76.21 | 12.32 | 77.82 | 11.74 |
| Specialty care physicians per 10,000 population | 10.29 | 2.01 | 11.04 | 2.01 | 11.53 | 1.98 | 12.27 | 1.97 | 12.95 | 2.04 |
| GDP per capital (10,000 Yuan) | 3.85 | 1.37 | 4.20 | 1.45 | 4.53 | 1.55 | 4.73 | 1.64 | 4.97 | 1.72 |
| Proportion of the population aged ≥65, % | 8.76 | 1.60 | 9.01 | 1.67 | 9.35 | 1.85 | 9.78 | 1.87 | 10.06 | 2.10 |
| Proportion of illiterate population aged 15 and above, % | 17.24 | 3.63 | 17.14 | 3.48 | 17.18 | 3.58 | 17.31 | 3.73 | 17.33 | 3.67 |
| Registered urban unemployment rate, % | 3.40 | 0.54 | 3.35 | 0.57 | 3.30 | 0.56 | 3.28 | 0.59 | 3.27 | 0.59 |
| Variable | Per Capita Total Medical Expenditure (1000 Yuan) | Per Capita Hospital Medical Expenditure (1000 Yuan) |
|---|---|---|
| Primary care physicians per 10,000 population | −0.026 (−0.088 to 0.035) | −0.046 * (−0.092 to −0.001) |
| The proportion of public health expenditure, % | −0.033 *** (−0.049 to −0.018) | −0.026 ** (−0.039 to −0.014) |
| Popularity rate of sanitary toilets in rural areas, % | −0.004 (−0.012 to 0.005) | −0.003 (−0.009 to 0.003) |
| Specialty care physicians per 10,000 population | 0.103 * (0.013 to 0.193) | 0.102 * (0.027 to 0.176) |
| GDP per capital (10,000 Yuan) | 0.132 * (0.019 to 0.245) | 0.118 * (0.014 to 0.221) |
| Proportion of the population aged ≥65, % | 0.025 (−0.027 to 0.077) | 0.020 (−0.024 to 0.065) |
| Proportion of illiterate population aged 15 and above, % | 0.001 (−0.027 to 0.023) | −0.001 (−0.015 to 0.014) |
| Registered urban unemployment rate, % | −0.008 (−0.138 to 0.123) | 0.003 (−0.100 to 0.106) |
| Constant | 2.855 * (1.323 to 4.388) | 2.109 (0.995 to 3.222) |
| Observations | 135 | 135 |
| Number of provinces | 27 | 27 |
| R-squared (within) | 0.939 | 0.931 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, M.; Liao, J.; Hu, N.; Kuang, L. Association between Primary Healthcare and Medical Expenditures in a Context of Hospital-Oriented Healthcare System in China: A National Panel Dataset, 2012–2016. Int. J. Environ. Res. Public Health 2020, 17, 6917. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186917
Zhou M, Liao J, Hu N, Kuang L. Association between Primary Healthcare and Medical Expenditures in a Context of Hospital-Oriented Healthcare System in China: A National Panel Dataset, 2012–2016. International Journal of Environmental Research and Public Health. 2020; 17(18):6917. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186917
Chicago/Turabian StyleZhou, Mengping, Jingyi Liao, Nan Hu, and Li Kuang. 2020. "Association between Primary Healthcare and Medical Expenditures in a Context of Hospital-Oriented Healthcare System in China: A National Panel Dataset, 2012–2016" International Journal of Environmental Research and Public Health 17, no. 18: 6917. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186917