A Meta-Analysis of Comparing Intermittent Epidural Boluses and Continuous Epidural Infusion for Labor Analgesia

 ,
,  ,
,  ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
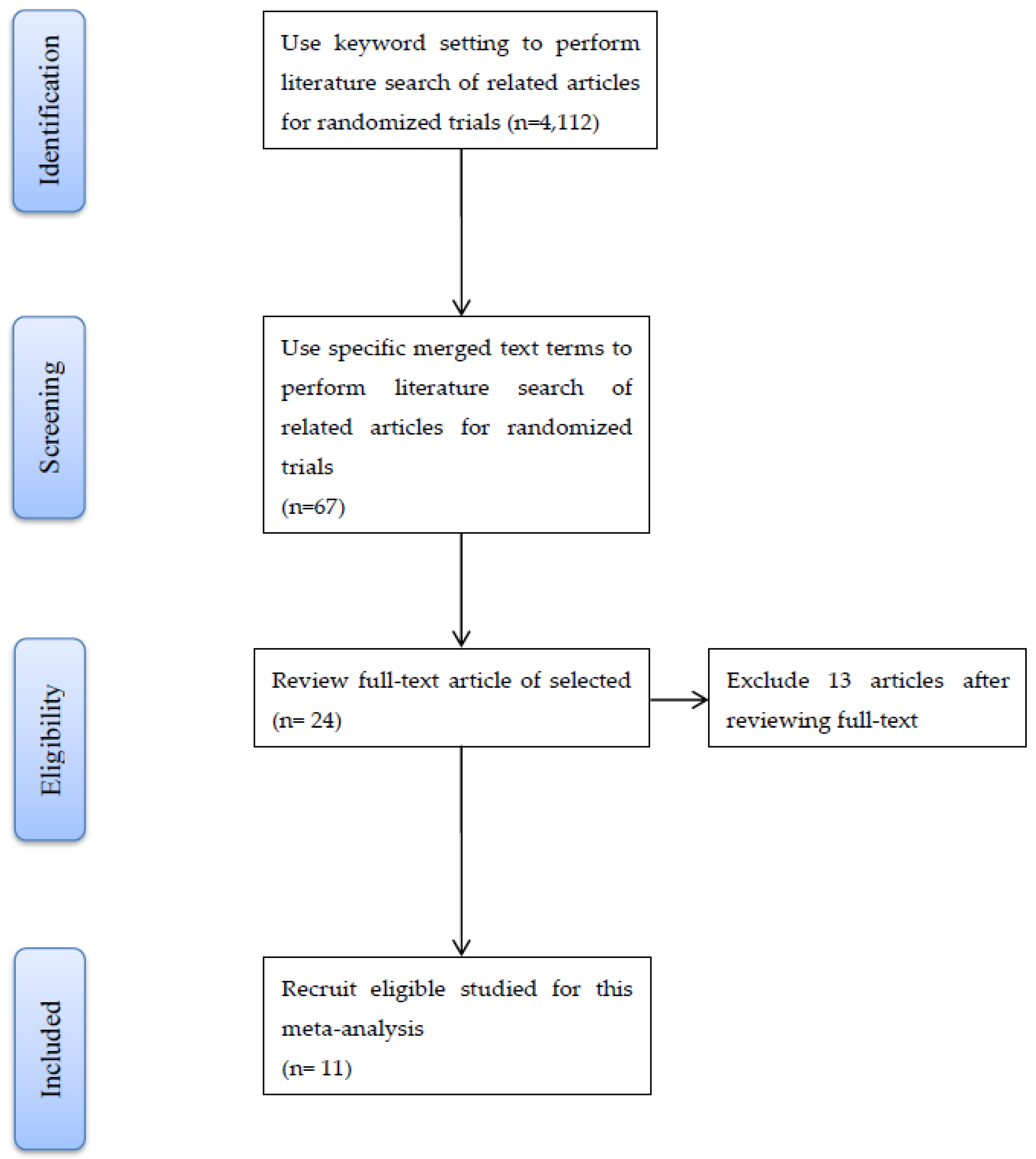
2.1. Identification of Relevant and Eligible Studies
2.2. Procedure of Extraction and Assessment of Eligible Studies
3. Results
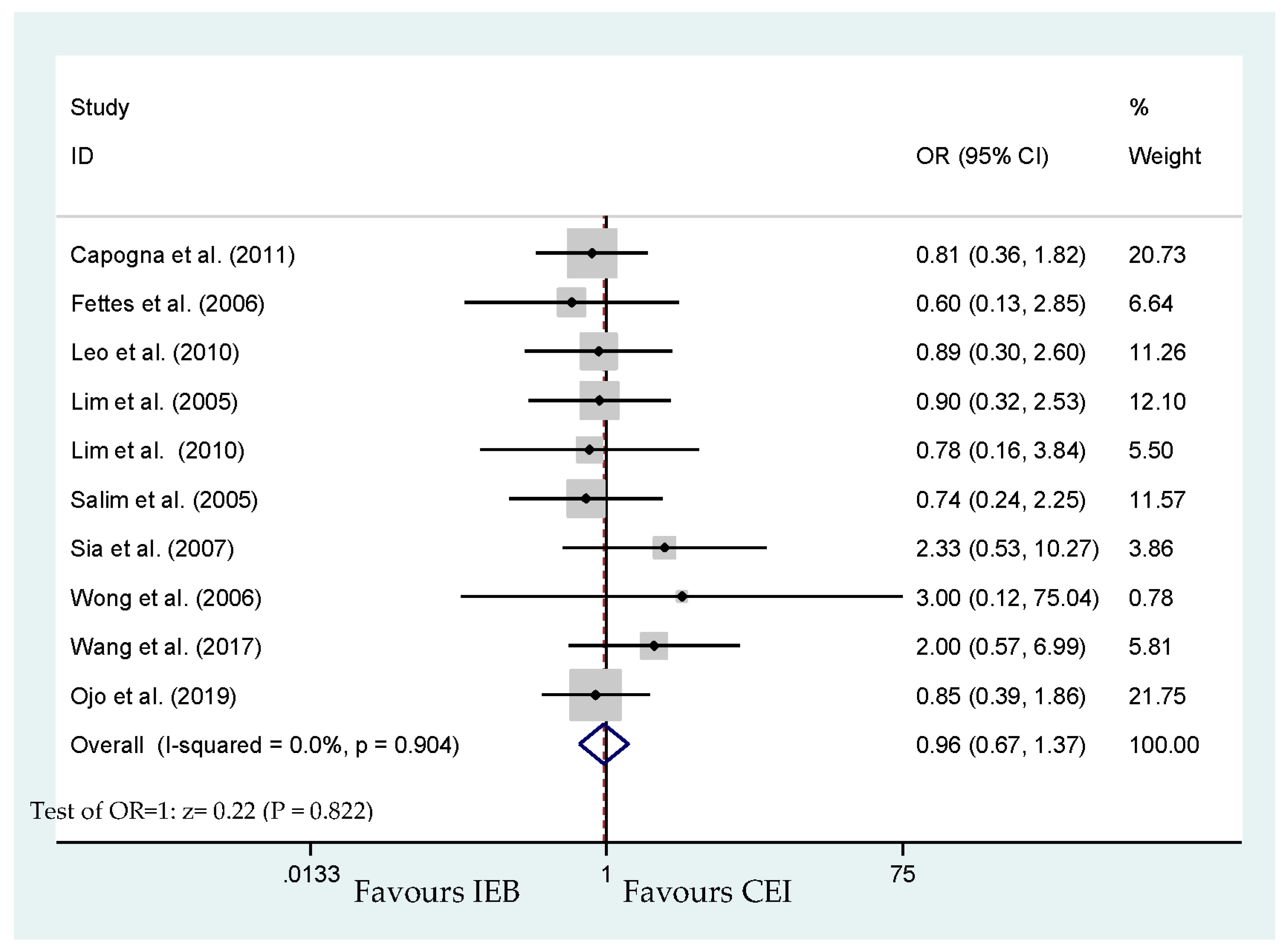
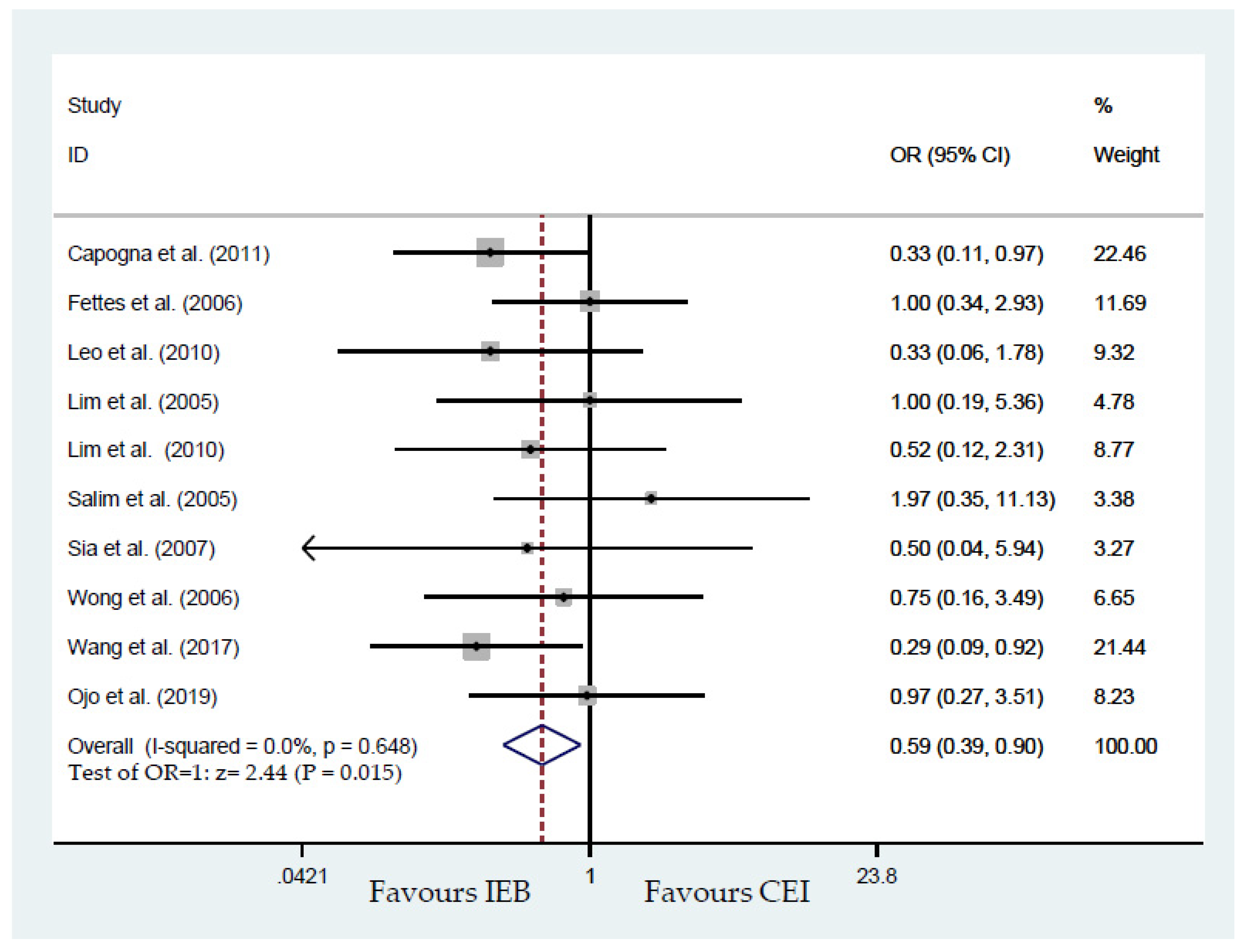
3.1. Delivery Mode
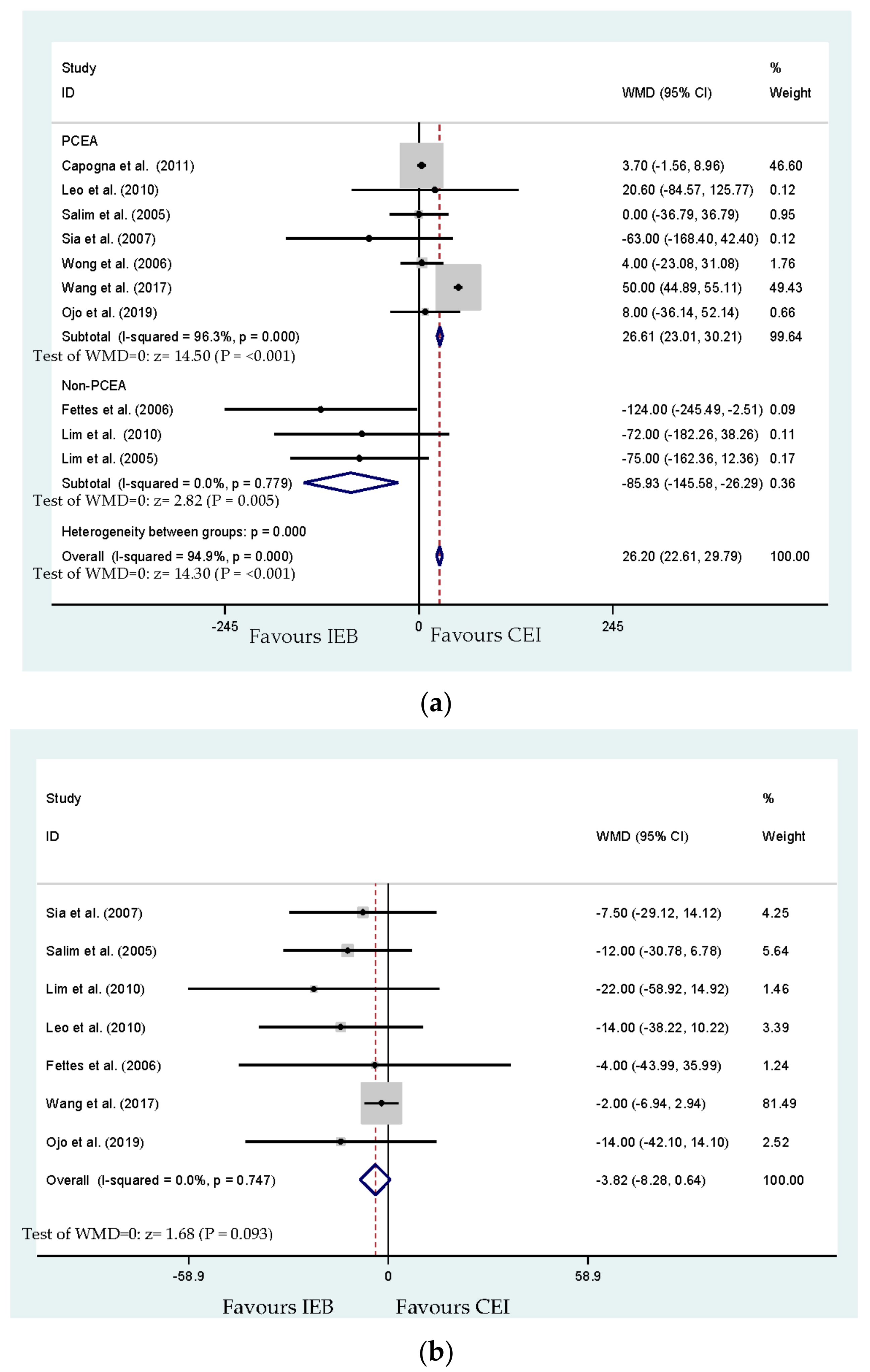
3.2. Labor Duration
3.3. Intervention of Anesthesia
3.4. Local Anesthetic Dosage
3.5. Maternal Satisfaction
3.6. Subgroup Analysis Using PCEA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Babb, M.; Koren, G.; Einarson, A. Treating pain during pregnancy. Can. Fam. Physician 2010, 56, 25–27. [Google Scholar] [PubMed]
- Melzack, R. The myth of painless childbirth (the John J. Bonica lecture). Pain 1984, 19, 321–337. [Google Scholar] [CrossRef]
- Wong, C.A.; Scavone, B.M.; Peaceman, A.M.; McCarthy, R.J.; Sullivan, J.T.; Diaz, N.T.; Yaghmour, E.; Marcus, R.J.; Sherwani, S.S.; Sproviero, M.T.; et al. The risk of cesarean delivery with neuraxial analgesia given early versus late in labor. N. Engl. J. Med. 2005, 352, 655–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambling, D.R.; Yu, P.; Cole, C.; McMorland, G.H.; Palmer, L. A comparative study of patient controlled epidural analgesia (PCEA) and continuous infusion epidural analgesia (CIEA) during labour. Can. J. Anaesth. 1988, 35, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heesen, M.; Böhmer, J.; Klöhr, S.; Hofmann, T.; Rossaint, R.; Straube, S. The effect of adding a background infusion to patient-controlled epidural labor analgesia on labor, maternal, and neonatal outcomes: A systematic review and meta-analysis. Anesth. Analg. 2015, 121, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J.G.; Capogna, G. Reducing likelihood of instrumental delivery with epidural anaesthesia. Lancet 2001, 358, 2. [Google Scholar] [CrossRef]
- Krawczyk, P.; Piwowar, P.; Sałapa, K.; Lonc, T.; Andres, J. Do epidural catheter size and flow rate affect bolus injection pressure in different programmed intermittent epidural bolus regimens? An in vitro study. Anesth. Analg. 2019, 129, 1587–1594. [Google Scholar] [CrossRef]
- Anim-Somuah, M.; Smyth, R.M.; Cyna, A.M.; Cuthbert, A. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database Syst. Rev. 2018, 5, CD000331. [Google Scholar] [CrossRef]
- Halpern, S.H.; Carvalho, B. Patient-controlled epidural analgesia for labor. Anesth. Analg. 2009, 108, 921–928. [Google Scholar] [CrossRef]
- Simmons, S.W.; Taghizadeh, N.; Dennis, A.T.; Hughes, D.; Cyna, A.M. Combined spinal-epidural versus epidural analgesia in labour. Cochrane Database Syst. Rev. 2012, 10, CD003401. [Google Scholar] [CrossRef]
- Van der Vyver, M.; Halpern, S.; Joseph, G. Patient-controlled epidural analgesia versus continuous infusion for labour analgesia: A meta-analysis. Br. J. Anaesth. 2002, 89, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furlan, A.D.; Malmivaara, A.; Chou, R.; Maher, C.G.; Deyo, R.A.; Schoene, M.; Bronfort, G.; van Tulder, M.W. Editorial Board of the Cochrane Back, Neck Group. 2015 updated method guideline for systematic reviews in the Cochrane back and neck group. Spine 2015, 40, 1660–1673. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Capogna, G.; Camorcia, M.; Stirparo, S.; Farcomeni, A. Programmed intermittent epidural bolus versus continuous epidural infusion for labor analgesia: The effects on maternal motor function and labor outcome. A randomized double-blind study in nulliparous women. Anesth. Analg. 2011, 113, 826–831. [Google Scholar] [CrossRef] [Green Version]
- Chua, S.M.; Sia, A.T. Automated intermittent epidural boluses improve analgesia induced by intrathecal fentanyl during labour. Can. J. Anaesth. 2004, 51, 581–585. [Google Scholar] [CrossRef] [Green Version]
- Fettes, P.D.; Moore, C.S.; Whiteside, J.B.; McLeod, G.A.; Wildsmith, J.A. Intermittent vs. continuous administration of epidural ropivacaine with fentanyl for analgesia during labour. Br. J. Anaesth. 2006, 97, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Leo, S.; Ocampo, C.E.; Lim, Y.; Sia, A.T. A randomized comparison of automated intermittent mandatory boluses with a basal infusion in combination with patient-controlled epidural analgesia for labor and delivery. Int. J. Obstet. Anesth. 2010, 19, 357–364. [Google Scholar] [CrossRef]
- Lim, Y.; Sia, A.T.; Ocampo, C. Automated regular boluses for epidural analgesia: A comparison with continuous infusion. Int. J. Obstet. Anesth. 2005, 14, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Chakravarty, S.; Ocampo, C.E.; Sia, A.T. Comparison of automated intermittent low volume bolus with continuous infusion for labour epidural analgesia. Anaesth. Intensive Care 2010, 38, 894–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salim, R.; Nachum, Z.; Moscovici, R.; Lavee, M.; Shalev, E. Continuous compared with intermittent epidural infusion on progress of labor and patient satisfaction. Obstet. Gynecol. 2005, 106, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Sia, A.T.; Lim, Y.; Ocampo, C. A comparison of a basal infusion with automated mandatory boluses in parturient-controlled epidural analgesia during labor. Anesth. Analg. 2007, 104, 673–678. [Google Scholar] [CrossRef]
- Wong, C.A.; Ratliff, J.T.; Sullivan, J.T.; Scavone, B.M.; Toledo, P.; McCarthy, R.J. A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia. Anesth. Analg. 2006, 102, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Feng, S.; Shiqin, X.; Zhang, P.; Wang, N.; Shen, X. Comparison of programmed intermittent epidural bolus with continuous epidural infusion at different time intervals for epidural labor analgesia. J. Clin. Anesthesiol. 2017, 33, 755–759. [Google Scholar]
- Ojo, O.A.; Mehdiratta, J.E.; Gamez, B.H.; Hunting, J.; Habib, A.S. Comparison of Programmed Intermittent Epidural Boluses With Continuous Epidural Infusion for the Maintenance of Labor Analgesia: A Randomized, Controlled, Double-Blind Study. Anesth. Analg. 2020, 130, 426–435. [Google Scholar] [CrossRef]
- Gambling, D.R.; McMorland, G.H.; Yu, P.; Laszlo, C. Comparison of patient-controlled epidural analgesia and conventional intermittent “top-up” injections during labor. Anesth. Analg. 1990, 70, 256–261. [Google Scholar]
- Halonen, P.; Sarvela, J.; Saisto, T.; Soikkeli, A.; Halmesmäki, E.; Korttila, K. Patient-controlled epidural technique improves analgesia for labor but increases cesarean delivery rate compared with the intermittent bolus technique. Acta Anaesthesiol. Scand. 2004, 48, 732–737. [Google Scholar] [CrossRef]
- Hicks, J.A.; Jenkins, J.G.; Newton, M.C.; Findley, I.L. Continuous epidural infusion of 0.075% bupivacaine for pain relief in labour. A comparison with intermittent top-ups of 0.5% bupivacaine. Anaesthesia 1988, 43, 289–292. [Google Scholar] [CrossRef]
- Hopp, H.; Schmitz, P.; Heinrich, J. Continuous peridural anesthesia--results of fractionated application in comparison to catheter infusion. Z. Geburtshilfe. Perinatol. 1982, 186, 279–283. [Google Scholar] [PubMed]
- Lamont, R.F.; Pinney, D.; Rodgers, P.; Bryant, T.N. Continuous versus intermittent epidural analgesia. A randomised trial to observe obstetric outcome. Anaesthesia 1989, 44, 893–896. [Google Scholar] [CrossRef]
- Li, D.F.; Rees, G.A.; Rosen, M. Continuous extradural infusion of 0.0625% or 0.125% bupivacaine for pain relief in primigravid labour. Br. J. Anaesth. 1985, 57, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Nikkola, E.; Läärä, A.; Hinkka, S.; Ekblad, U.; Kero, P.; Salonen, M. Patient-controlled epidural analgesia in labor does not always improve maternal satisfaction. Acta Obstet. Gynecol. Scand. 2006, 85, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Paech, M.J.; Pavy, T.J.; Sims, C.; Westmore, M.D.; Storey, J.M.; White, C. Clinical experience with patient-controlled and staff-administered intermittent bolus epidural analgesia in labour. Anaesth. Intensive Care 1995, 23, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Robert, D.; Kaladji, C.; Charlet, P.; Soufarapis, H.; Quesnel, J.; Bricard, H. Peridural obstetrical anesthesia: Intermittent injections or perfusion of bupivacaine? Cah. Anesthesiol. 1989, 37, 271–277. [Google Scholar]
- Smedstad, K.G.; Morison, D.H. A comparative study of continuous and intermittent epidural analgesia for labour and delivery. Can. J. Anaesth. 1988, 35, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Delgado, C.; Ciliberto, C.; Bollag, L.; Sedensky, M.; Landau, R. Continuous epidural infusion versus programmed intermittent epidural bolus for labor analgesia: Optimal configuration of parameters to reduce physician-administered top-ups. Curr. Med. Res. Opin. 2018, 34, 649–656. [Google Scholar] [CrossRef]
- Vandermeulen, E.P.; Van Aken, H.; Vertommen, J.D. Labor pain relief using bupivacaine and sufentanil: Patient controlled epidural analgesia versus intermittent injections. Eur. J. Obstet. Gynecol. Reprod. Biol. 1995, 59, S47–S54. [Google Scholar] [CrossRef]
- Vertommen, J.D.; Lemmens, E.; Van Aken, H. Comparison of the addition of three different doses of sufentanil to 0.125% bupivacaine given epidurally during labour. Anaesthesia 1994, 49, 678–681. [Google Scholar] [CrossRef]
- Halpern, S.H.; Abdallah, F.W. Effect of labor analgesia on labor outcome. Curr. Opin. Anaesthesiol. 2010, 23, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Angle, P.; Landy, C.K.; Charles, C.; Yee, J.; Watson, J.; Kung, R.; Kronberg, J.; Halpern, S.; Lam, D.; Lie, L.M.; et al. Phase 1 development of an index to measure the quality of neuraxial labour analgesia: Exploring the perspectives of childbearing women. Can. J. Anaesth. 2010, 57, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Hodnett, E.D. Pain and women’s satisfaction with the experience of childbirth: A systematic review. Am. J. Obstet. Gynecol. 2002, 186, S160–S172. [Google Scholar]
- Dickinson, J.E.; Paech, M.J.; McDonald, S.J.; Evans, S.F. Maternal satisfaction with childbirth and intrapartum analgesia in nulliparous labour. Aust. N. Z. J. Obstet. Gynaecol. 2003, 43, 463–468. [Google Scholar] [CrossRef]
- Brokelman, R.B.; Haverkamp, D.; van Loon, C.; Hol, A.; van Kampen, A.; Veth, R. The validation of the visual analogue scale for patient satisfaction after total hip arthroplasty. Eur. Orthop. Traumatol. 2012, 3, 101–105. [Google Scholar] [CrossRef] [Green Version]
- McCrea, B.H.; Wright, M.E. Satisfaction in childbirth and perceptions of personal control in pain relief during labour. J. Adv. Nurs. 1999, 29, 877–884. [Google Scholar] [CrossRef]
- George, R.B.; Allen, T.K.; Habib, A.S. Intermittent epidural bolus compared with continuous epidural infusions for labor analgesia: A systematic review and meta-analysis. Anesth. Analg. 2013, 116, 133–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Zhou, J.; Xiao, H.; Pan, S.; Liu, J.; Shang, Y.; Yao, S. A systematic review and meta-analysis comparing programmed intermittent bolus and continuous infusion as the background infusion for parturient-controlled epidural analgesia. Sci. Rep. 2019, 9, 2583. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Zhang, H.; Zhang, H.; Guo, M.; Gao, Y.; Du, C. Intermittent epidural bolus versus continuous epidural infusions for labor analgesia: A meta-analysis of randomized controlled trials. PLoS ONE 2020, 15, e0234353. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Smith, A.F. Trial sequential analysis: Adding a new dimension to meta-analysis. Anaesthesia 2020, 75, 15–20. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes\Characteristics | Included Studies | No. of Participants | Overall WMD or OR and 95% CI | p-Value | I2 (%) | Forest Plot | Subgroup Analysis Effect (p-Value) |
|---|---|---|---|---|---|---|---|
| Cesarean delivery mode | Capogna et al. [17], Fettes et al. [19], Leo et al. [20], Lim et al. [21], Lim et al. [22], Salim et al. [23], Sia et al. [24], Wong et al. [25], Wang et al. [26], and Ojo et al. [27] | 896 | 0.96 (0.67–1.37) | 0.822 | 0.0 | Figure 2 | No |
| Instrumental delivery mode | Capogna et al. [17], Fettes et al. [19], Leo et al. [20], Lim et al. [21], Lim et al. [22], Salim et al. [23], Sia et al. [24], Wong et al. [25], Wang et al. [26], and Ojo et al. [27] | 896 | 0.59 (0.39–0.90) | 0.015 * | 0.0 | Figure 3 | No |
| Total duration (minutes) of labor analgesia | Capogna et al. [17], Fettes et al. [19], Leo et al. [20], Lim et al. [21], Lim et al. [22], Salim et al. [23], Sia et al. [24], Wong et al. [25], Wang et al. [26], and Ojo et al. [27] | 896 | 26.20 (22.61–29.79) | <0.001 * | 94.9 | Figure 4a | 26.61 (<0.001 *) for PCEA ([17], [20], [23], [24], [25], [26], and [27]) −85.93 (0.005 *) for non-PCEA ([19], [21], and [22]) |
| Duration (minutes) of second stage of labor analgesia | Fettes et al. [19], Leo et al. [20], Lim et al. [22], Salim et al. [23], Sia et al. [24], Wang et al. [26] and Ojo et al. [27] | 565 | −3.82 (−8.28 to 0.64) | 0.093 | 0.0 | Figure 4b | No |
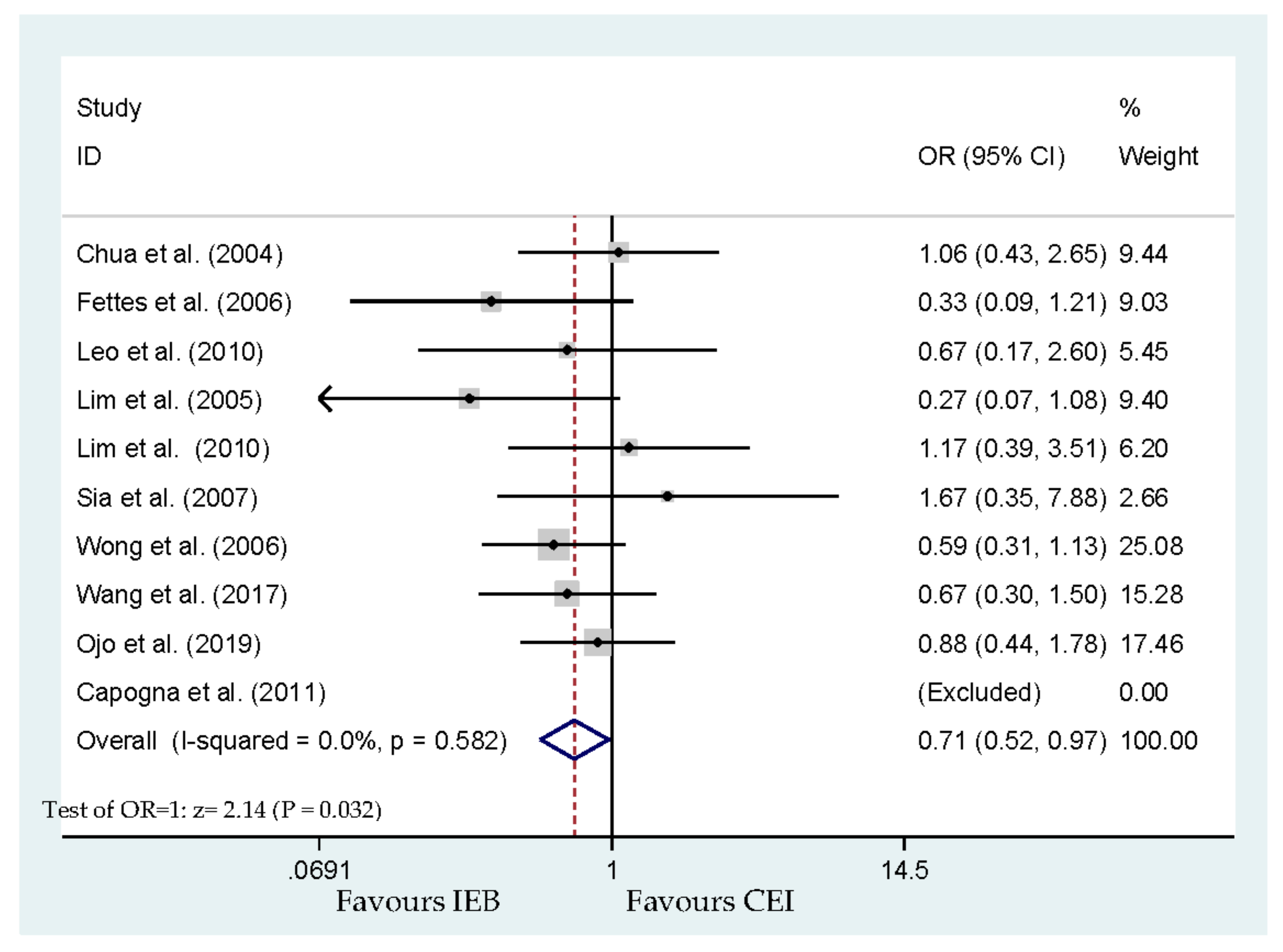
| Requirement of anesthetic interventions | Capogna et al. [17], Chua et al. [18], Fettes et al. [19], Leo et al. [20], Lim et al. [21], Lim et al. [22], Sia et al. [24], Wong et al. [25], Wang et al. [26] and Ojo et al. [27] | 811 | 0.71 (0.52–0.97) | 0.032 * | 0.0 | Figure 5 | No |
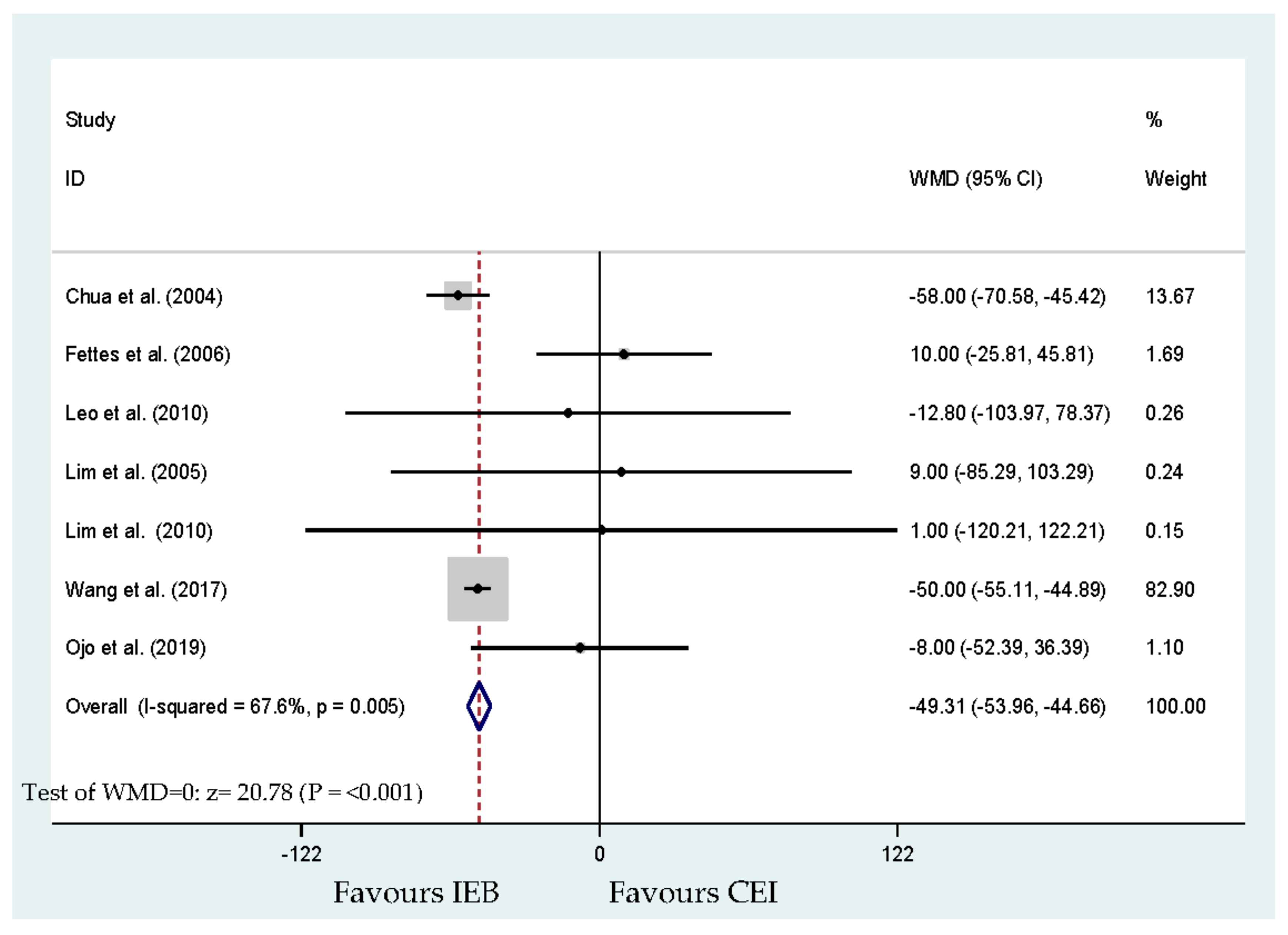
| Time (minutes) to first requirement of anesthetic intervention | Chua et al. [18], Fettes et al. [19], Leo et al. [20], Lim et al. [21], Lim et al. [22], Wang et al. [26] and Ojo et al. [27] | 465 | −49.31 (−53.96 to −44.66) | <0.001 * | 67.6 | Figure 6 | No |
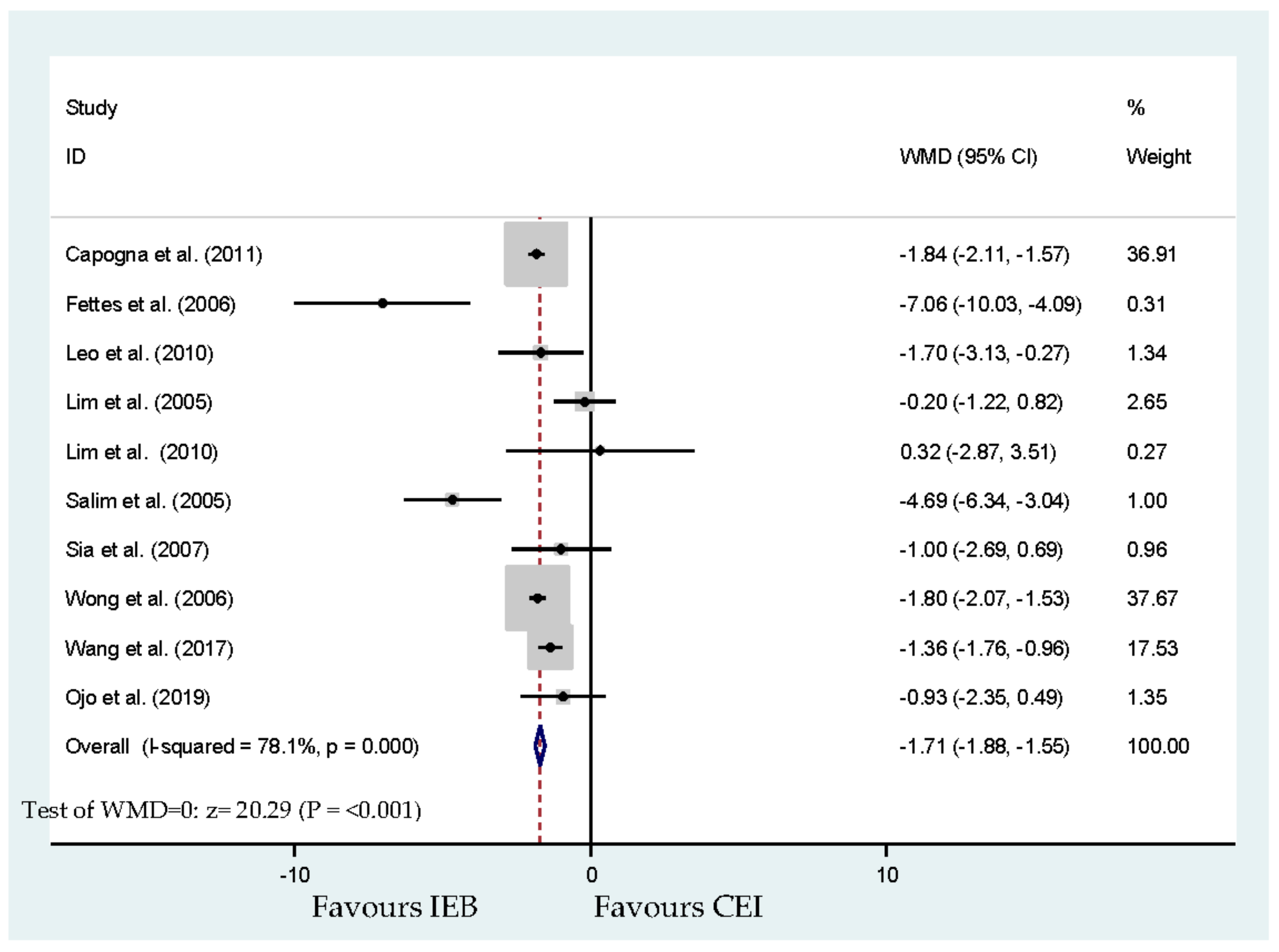
| Delivered dosage (milligrams per hour) of local anesthetic (bupivacaine equivalents) | Capogna et al. [17], Fettes et al. [19], Leo et al. [20], Lim et al. [21], Lim et al. [22], Salim et al. [23], Sia et al. [24], Wong et al. [25], Wang et al. [26] and Ojo et al. [27] | 896 | −1.71 (−1.88 to −1.55 | <0.001 * | 78.1 | Figure 7 | No |
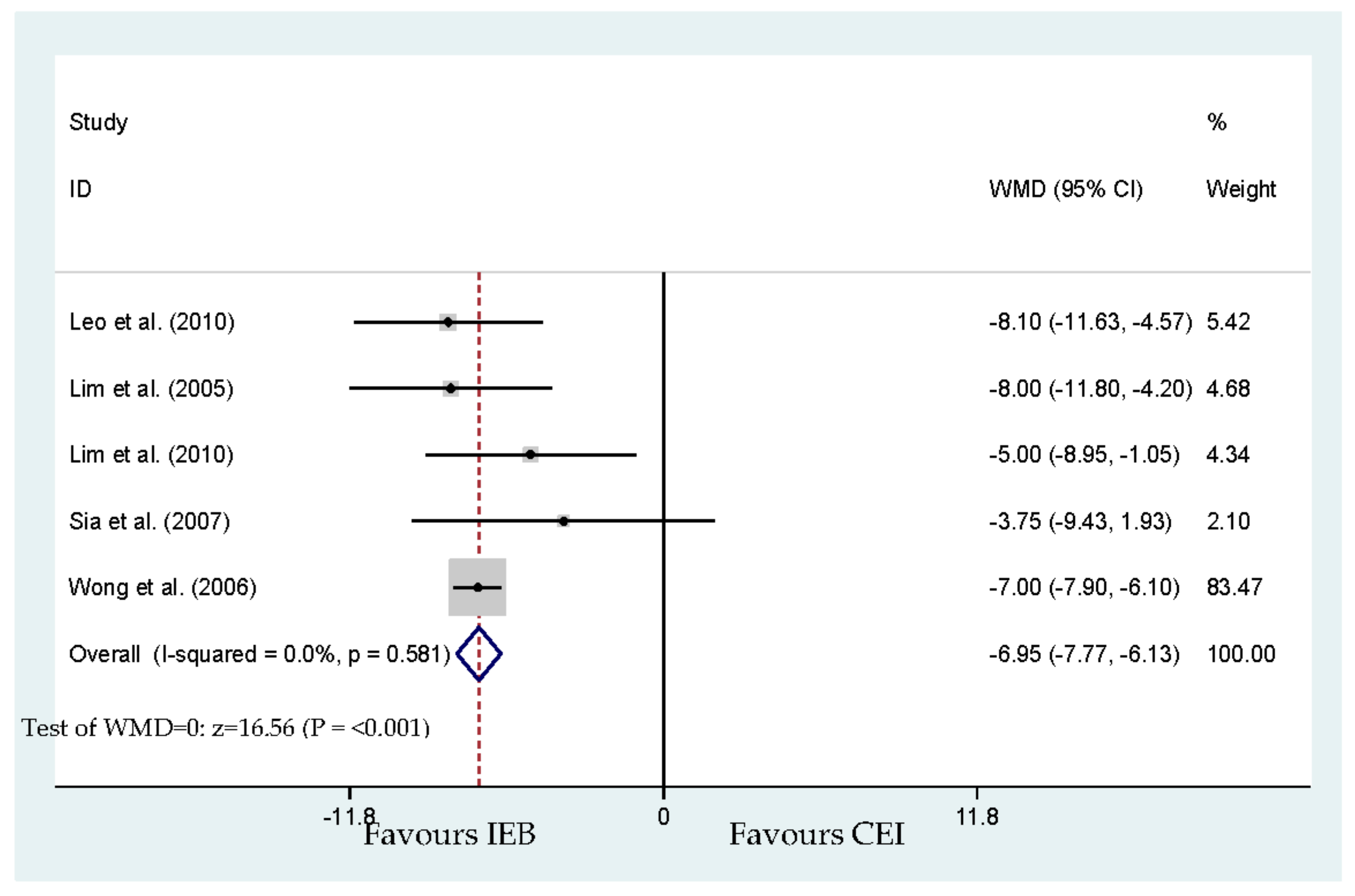
| Maternal satisfaction (visual analog scale from 0 to 100) | Leo et al. [20] Lim et al. [21] Lim et al. [22] Sia et al. [24] Wong et al. [25] | 340 | −6.95 (−7.77 to −6.13) | <0.001 * | 0.0 | Figure 8 | No |
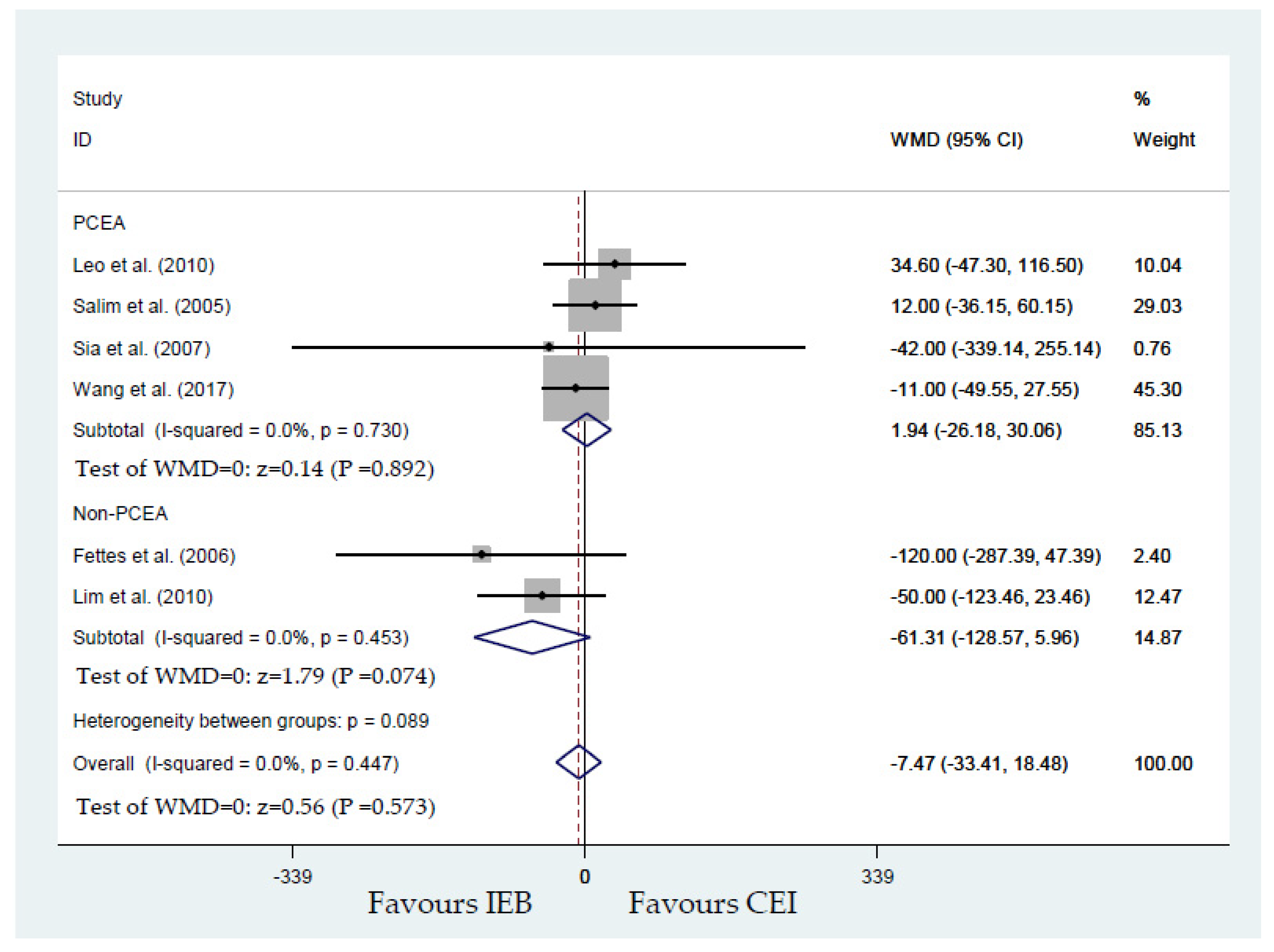
| Duration (minutes) of first stage of labor analgesia | Fettes et al. [19], Leo et al. [20], Lim et al. [22], Salim et al. [23], Sia et al. [24], and Wong et al. [25] | 445 | −7.47 (−33.41 to 18.48) | 0.573 | 0.0 | Figure 9 | 1.94 (0.892) for PCEA ([20], [23], [24] and [25]) −61.31 (0.074) for non-PCEA ([19] and [22]) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzeng, I.-S.; Kao, M.-C.; Pan, P.-T.; Chen, C.-T.; Lin, H.-Y.; Hsieh, P.-C.; Kuo, C.-Y.; Hsieh, T.-H.; Kung, W.-M.; Cheng, C.-H.; et al. A Meta-Analysis of Comparing Intermittent Epidural Boluses and Continuous Epidural Infusion for Labor Analgesia. Int. J. Environ. Res. Public Health 2020, 17, 7082. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197082
Tzeng I-S, Kao M-C, Pan P-T, Chen C-T, Lin H-Y, Hsieh P-C, Kuo C-Y, Hsieh T-H, Kung W-M, Cheng C-H, et al. A Meta-Analysis of Comparing Intermittent Epidural Boluses and Continuous Epidural Infusion for Labor Analgesia. International Journal of Environmental Research and Public Health. 2020; 17(19):7082. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197082
Chicago/Turabian StyleTzeng, I-Shiang, Ming-Chang Kao, Po-Ting Pan, Chu-Ting Chen, Han-Yu Lin, Po-Chun Hsieh, Chan-Yen Kuo, Tsung-Han Hsieh, Woon-Man Kung, Chu-Hsuan Cheng, and et al. 2020. "A Meta-Analysis of Comparing Intermittent Epidural Boluses and Continuous Epidural Infusion for Labor Analgesia" International Journal of Environmental Research and Public Health 17, no. 19: 7082. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197082