Effectiveness of “Hand Hygiene Fun Month” for Kindergarten Children: A Pilot Quasi-Experimental Study


Abstract
:1. Background
2. Methods
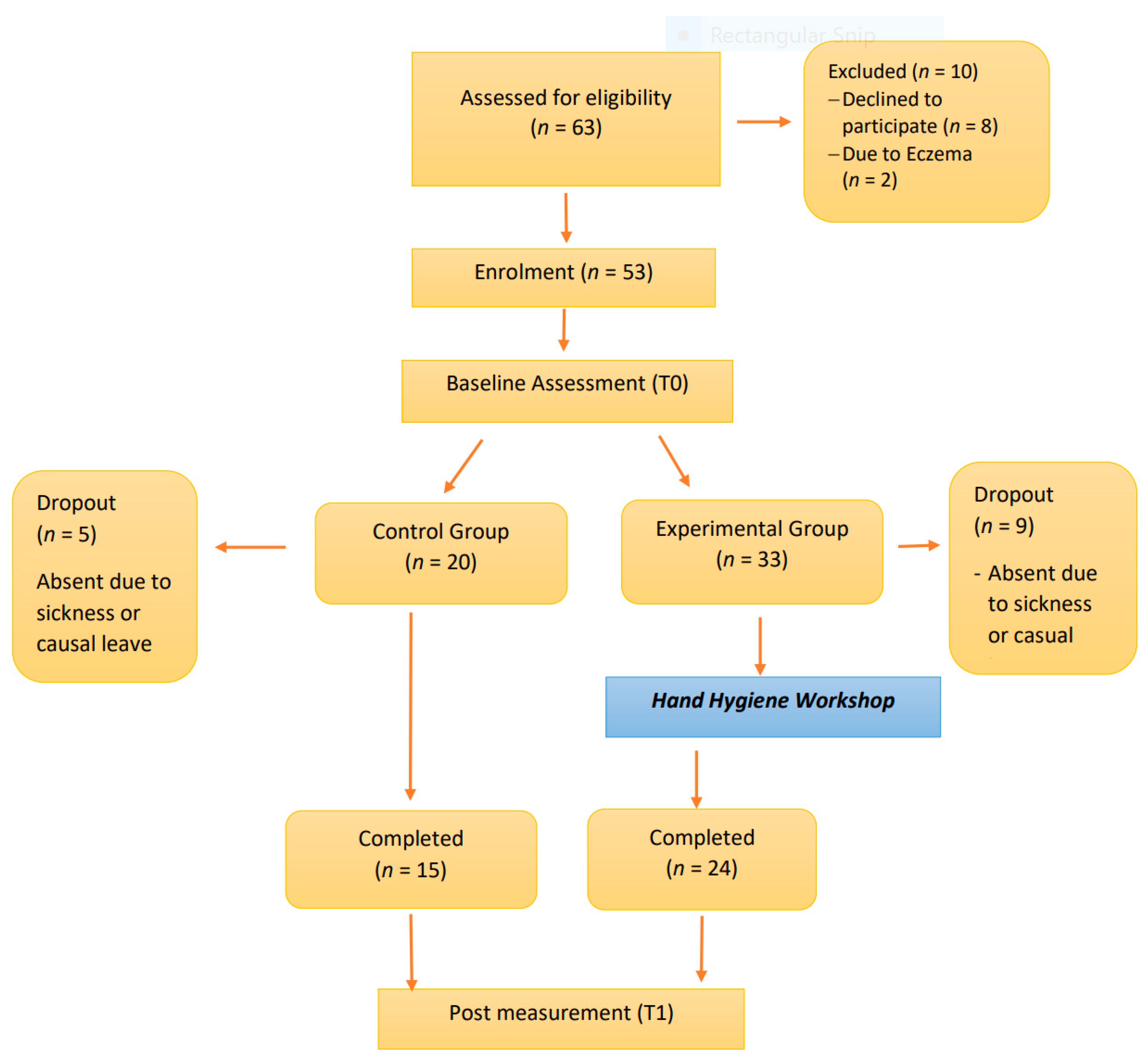
2.1. Participants
2.2. Instruments
i) Hand Hygiene Knowledge Questionnaire for Children
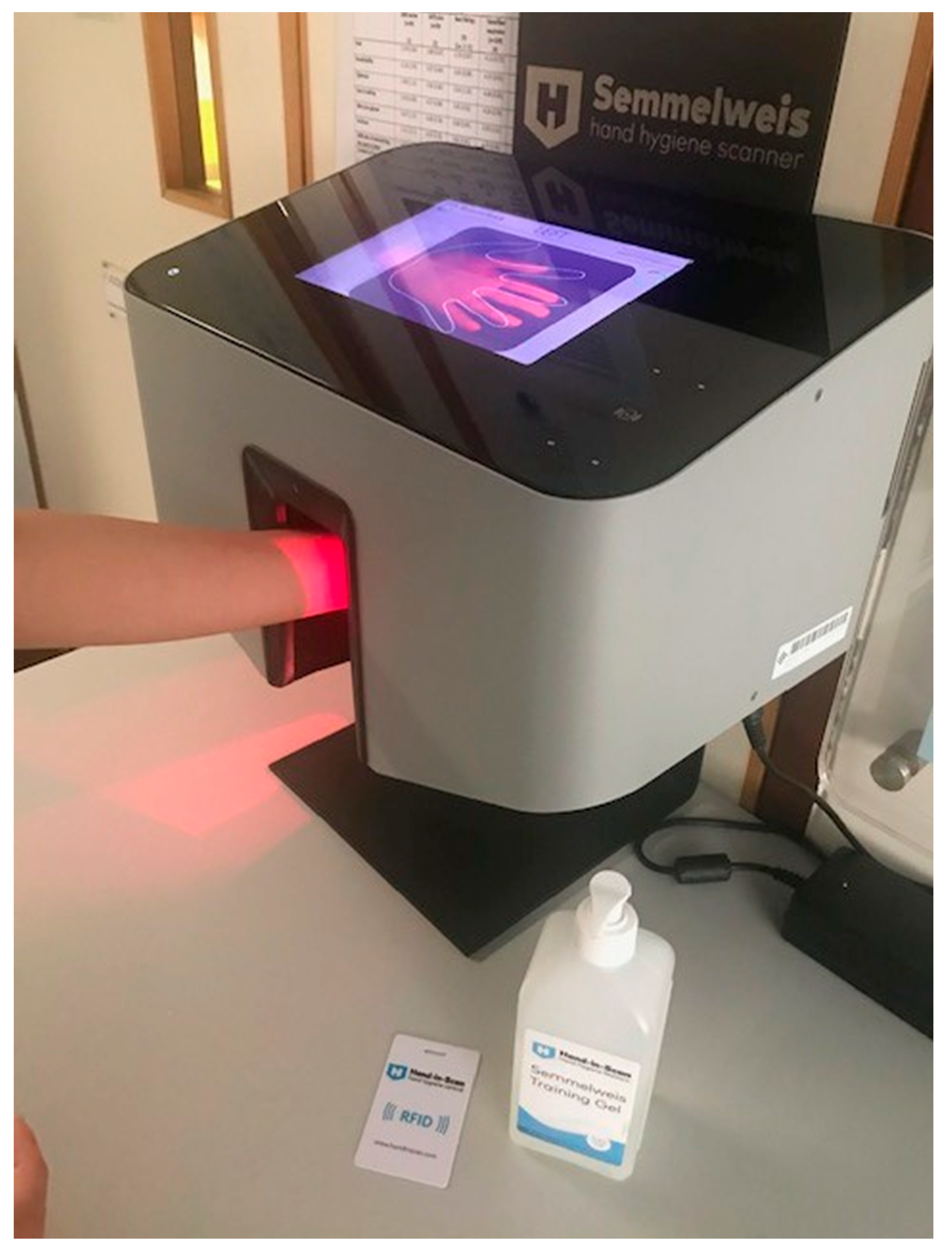
ii) Use of Hand Scanner for Assessing the Coverage of Hand Sanitizer
2.3. Procedures
Elements of the Hand Hygiene Educational Program
i) First Session
ii) Second Session
iii) Third Session
iv) Fourth Session
2.4. Data Analyses
3. Results
3.1. Knowledge Level Towards Hand Hygiene Behaviors
3.2. Hand Coverage by Hand Sanitizer
4. Discussion
4.1. Age-Appropriate Creative Approaches for Teachings Important HH Concepts
4.2. Limitations
5. Conclusions
Implications for Public Health
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Azor-Martinez, E.; Cobos-Carrascos, E.; Seijas-Vazquez, M.L.; Fernandez-Sanchez, C.; Strizzi, J.M.; Torres-Alegre, P.; et al. Hand hygiene program decreases school absenteeism due to upper respiratory infections. J. Sch. Health. 2016, 86, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Mbakaya, B.C.; Lee, P.H.; Lee, R.L.T. Hand hygiene intervention strategies to reduce diarrhoea and respiratory infections among schoolchildren in developing countries: A systematic review. Int. J. Environ. Res. Public Health 2017, 14, 371. [Google Scholar] [CrossRef] [PubMed]
- McCutcheon, H.; Fitzgerald, M. The public health problem of acute respiratory illness in childcare. J. Clin. Nurs. 2001, 10, 305–310. [Google Scholar] [CrossRef] [PubMed]
- van Beeck, A.H.E.; Zomer, T.P.; van Beeck, E.F.; Richardus, J.H.; Voeten, H.A.C.M.; Erasmus, V. Children’s hand hygiene behavior and available facilities: An observational study in Dutch day care centres. Euro J. Public Health. 2015, 26, 297–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guinan, M.; McGuckin, M.; Ali, Y. The effect of a comprehensive handwashing program on absenteeism in elementary schools. Am. J. Infect. Control. 2002, 30, 217–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- My Diffability Australia. They Won’t (or Can’t) Stop Putting Things in Their Mouths!–Supporting Kids in The Classroom. Available online: https://bit.ly/2NygQpW (accessed on 10 November 2019).
- Express. Shock Number of Children Cannot Use Knife and Fork and Would Rather Eat with Their Hands. Available online: https://bit.ly/34L39JN (accessed on 10 November 2019).
- Rock, A. How to Stop Nose Picking in Preschoolers. Available online: https://www.verywellfamily.com/how-to-stop-nose-picking-in-preschoolers-2764835 (accessed on 10 November 2019).
- Liu, X.; Hou, W.; Zhao, Z.; Cheng, J.; Beeck, E.F.; Peng, X.; Jones, K.; Fu, X.; Zhou, Y.; Zhang, Z.; et al. A hand hygiene intervention to decrease hand, foot and mouth disease and absence due to sickness among kindergarteners in China: A cluster-randomized controlled trial. J. Infect. 2019, 78, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CHP. Hand, Foot and Mouth Disease. In Centre for Health Protection, Department of Health, The Government of the Hong Kong Special Administrative Region. Available online: https://www.chp.gov.hk/en/healthtopics/content/24/23.htm# (accessed on 24 September 2020).
- Koh, W.M.; Bogich, T.; Siegel, K.; Jin, J.; Chong, E.Y.; Tan, C.Y.; Chen, M.I.C.; Horby, P.; Cook, A.R. The epidemiology of Hand, Foot and Mouse Disease in Asia: A systematic review and analysis. Pediatr. Infect. Dis. J. 2016, 35, e285–e300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. WHO and UNICEF Launch Hand Hygiene for All Global Initiative. Available online: https://www.unwater.org/who-and-unicerf-launch-hand-hygiene-for-all-global-initiative/ (accessed on 24 September 2020).
- WHO. My 5 Moments for Hand Hygiene. In WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/infection-prevention/campaigns/clean-hands/5moments/en/ (accessed on 24 September 2020).
- Jurs, J.; Mangili, L.; Jurs, S. Preschool children’s attitudes toward health risk behaviours. Psychol. Rep. 1990, 66, 754. [Google Scholar] [CrossRef] [PubMed]
- Rashed, A. The impact of an interactive educational program to improve handwashing compliance among preschoolers in a hungarian kin. Int. J. Med. Res. Health Sci. 2019, 8, 70–74. [Google Scholar]
- BESTLIFE. Childhood Habits that Affect. Your Adult Health. Available online: https://bestlifeonline.com/childhood-habits-that-affect-health (accessed on 24 September 2020).
- Or, P.P.L.; Ching, P.T.Y.; Chung, J.W.Y. Can flu-like absenteeism in kindergartens be reduced through hand hygiene training for both parents and their kindergarteners? J. Prim. Care Commun. Health 2020, 11, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, H.Y.; Lo, A.S.C.; Ma, K.H.H.; Lee, A. Knowledge enrichment would enhance hand hygiene practice in early childhood: An observational study in Hong Kong. Hong Kong J. Paediatr. 2020, 25, 14–158. [Google Scholar]
- Comprehensive School Health Education: Totally Awesome Strategies for Teaching Health, 6th ed.; McGraw-Hill Higher Education: New York, NY, USA, 2009.
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Psychology Notes HQ. Piaget’s Theory of Cognitive Development. Available online: https://www.psychologynoteshq.com/piagetstheory/ (accessed on 9 November 2019).
- The Neurotypical Site. Developmental Stages: Piaget’s Stages. Available online: https://www.theneurotypical.com/piagets-four-stages.html (accessed on 9 November 2019).
- One Stop English. Children’s Development. Available online: http://www.onestopenglish.com/children/methodology/childrens-development/ (accessed on 9 November 2019).
- Lee, R.L.T.; Leung, C.; Tong, W.K.; Chen, H.; Lee, P.H. Comparative efficacy of a simplified handwashing program for improvement in hand hygiene and reduction of school absenteeism among children with intellectual disability. Am. J. Infect. Control 2015, 43, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Au, W.H.; Suen, L.K.P.; Kwok, Y.L. Handwashing programme in kindergarten: A pilot study. Health Educ. 2010, 110, 5–16. [Google Scholar] [CrossRef]
- Konicki, T.; Miller, E. Use of a simulation intervention to examine differences in nursing students’ hand hygiene knowledge, beliefs, and behaviors. Nurse Educ. Today 2016, 45, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Johnson, H.D.; Sholcosky, D.; Gabello, K.; Ragni, R.; Ogonosky, N. Sex differences in public restroom handwashing behaviour associated with visual behaviour prompts. Percept. Mot. Ski. 2003, 97, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Suen, L.K.P.; Wong, J.W.S.; Lo, K.Y.K.; Lai, T.K.H. The use of hand scanner to enhance hand hygiene practice among nursing students: A single-blinded feasibility study. Nurse Educ. Today 2019, 76, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Suen, L.K.P.; So, Z.Y.Y.; Yeung, S.K.W.; Lo, K.Y.K.; Lam, S.C. Epidemiological investigation on hand hygiene knowledge and behaviours: A cross-sectional study on gender disparity. BMC Public Health 2019, 19, 401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aunger, R.; Greenland, K.; Ploubidis, G.; Schmidt, W.; Oxford, J.; Curtis, V. The determinants of reported personal and household hygiene behavior: A multi-country study. PLoS ONE 2016, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pickering, A.J.; Blum, A.G.; Breiman, R.F.; Ram, P.K.; Davis, J. Video surveillance captures student hand hygiene behavior, reactivity to observation, and peer influence in Kenyan primary schools. PLoS ONE 2014, 9, e92571. [Google Scholar] [CrossRef] [PubMed]
- Narvaes, A. The Importance of Starting Healthy Habits at An Early Age. Available online: https://mountainkidslouisville.com/blog/healthy-habits-early-age/ (accessed on 24 September 2020).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Experimental Group | Control Group | p-Value ◈ |
|---|---|---|---|
| (n = 24) | (n = 15) | ||
| In which of the following situations, hand hygiene must be performed? | Correct responses | ||
| % | |||
| After sneezing ※ | |||
| T0 | 100 | 100 | --- |
| T1 | 100 | 100 | --- |
| After singing | |||
| T0 | 83.3 | 46.7 | 0.031 |
| T1 | 95.8 | 86.7 | 0.547 |
| Before toilet time | |||
| T0 | 52.4 | 53.3 | 1 |
| T1 | 95.8 | 60 | 0.008 ** |
| After toilet time※ | |||
| T0 | 100 | 100 | --- |
| T1 | 100 | 100 | --- |
| Before meal ※ | |||
| T0 | 95.2 | 100 | 1 |
| T1 | 100 | 93.3 | 0.385 |
| After meal | |||
| T0 | 33.3 | 26.7 | 0.734 |
| T1 | 87.5 | 33.3 | 0.001 ** |
| After play time ※ | |||
| T0 | 75 | 93.3 | 0.216 |
| T1 | 95.8 | 93.3 | 1 |
| Before sleep | |||
| T0 | 58.3 | 80 | 0.295 |
| T1 | 95.8 | 86.7 | 0.547 |
| After shower | |||
| T0 | 79.2 | 93.3 | 0.376 |
| T1 | 100 | 86.7 | 0.142 |
| After changing shoes ※ | |||
| T0 | 66.7 | 46.7 | 0.318 |
| T1 | 100 | 53.3 | <0.001 *** |
| After taking off facial masks ※ | |||
| T0 | 100 | 86.7 | 0.142 |
| T1 | 100 | 100 | --- |
| Before watching television | |||
| T0 | 83.3 | 93.3 | 0.631 |
| T1 | 100 | 93.3 | 0.385 |
| Total correct (score) ❖ | |||
| T0 | 9.29 (1.73) | 9.20 (1.66) | 0.7 |
| T1 | 11.71 (0.69) | 9.87 (1.51) | <0.001 *** |
| Variables | Experimental Group (n = 24) | Control Group (n = 15) | Comparisons between Groups | ||
|---|---|---|---|---|---|
| Mean (SD) | Within-group p-Value # | Mean (SD) | Within-group p-Value | p-Value ❖ | |
| Palm (Left) (%) T0 T1 | 92.67 (6.35) 94.88 (4.67) | 0.361 | 92.45 (6.29) 89.29 (7.51) | 1.000 | 0.851 0.017 * |
| Dorsum (Left) (%) T0 T1 | 66.79 (26.37) 85.09 (17.56) | 0.001 ** | 46.64 (30.65) 64.65 (30.36) | 1.000 | 0.057 0.030 * |
| Palm (Right) (%) T0 T1 | 92.29 (5.78) 97.36 (2.44) | 0.001 ** | 93.92 (3.20) 92.01 (8.99) | 0.865 | 0.583 0.018 * |
| Dorsum (Right) (%) T0 T1 | 70.58 (27.79) 75.42 (22.60) | 0.304 | 44.32 (30.62) 54.54 (34.34) | 0.427 | 0.015 * 0.126 |
| Overall hand coverage (%) T0 T1 | 80.58 (14.34) 88.19 (10.14) | 0.006 ** | 69.34 (15.83) 75.12 (17.12) | 0.394 | 0.053 0.010 * |
| Variables | All (n = 39) | Experimental Group (n = 24) | Baseline | Post-Measurement | ||||
|---|---|---|---|---|---|---|---|---|
| Control Group (n = 15) | All (n = 39) | Experimental Group (n = 24) | Control Group (n = 15) | |||||
| % | % | % | p-Value ◈ | % | % | % | p-Value ◈ | |
| Palms Missed Covered | 2.6 97.4 | 0.0 100.0 | 6.7 93.3 | 0.385 | 5.1 94.9 | 4.2 95.8 | 6.7 93.3 | 1.000 |
| Back of hands Missed Covered | 94.9 5.1 | 91.7 8.3 | 100.0 0.0 | 0.514 | 84.6 15.4 | 79.2 20.8 | 93.3 6.7 | 0.376 |
| Finger webs Missed Covered | 61.5 38.5 | 54.2 45.8 | 73.3 26.7 | 0.317 | 74.4 25.6 | 66.7 33.3 | 86.7 13.3 | 0.263 |
| Back of fingers Missed Covered | 69.2 30.8 | 58.3 41.7 | 86.7 13.3 | 0.083 | 76.9 23.1 | 75.0 25.0 | 80.0 20.0 | 1.000 |
| Thumbs Missed Covered | 92.3 7.7 | 87.5 12.5 | 100.0 0.0 | 0.271 | 82.1 17.9 | 70.8 29.2 | 100.0 0.0 | 0.031 * |
| Finger tips Missed Covered | 56.4 43.6 | 58.3 41.7 | 53.3 46.7 | 1.000 | 51.3 48.1 | 45.8 54.2 | 60.0 40.0 | 0.514 |
| Variables | Male (n = 16) | Female (n = 23) | Between Group Comparison |
|---|---|---|---|
| M ± SD | M ± SD | p-Value ❖ | |
| Before intervention | |||
| Palm (Left) (%) | 89.73 ± 6.18 | 94.18 ± 5.81 | 0.030 * |
| Dorsum (Left) (%) | 51.37 ± 30.50 | 61.39 ± 29.47 | 0.125 |
| Palm (Right) (%) | 90.90 ± 5.34 | 93.63 ± 4.28 | 0.252 |
| Dorsum (Right) (%) | 54.76 ± 32.24 | 59.51 ± 30.35 | 0.857 |
| Overall hand coverage (%) | 71.69 ± 15.96 | 77.18 ± 15.31 | 0.160 |
| After intervention | |||
| Palm (Left) (%) | 92.35 ± 7.56 | 93.37 ± 6.41 | 0.868 |
| Dorsum (Left) (%) | 72.70 ± 30.73 | 78.73 ± 21.93 | 0.856 |
| Palm (Right) (%) | 92.90 ± 9.04 | 96.31 ± 3.07 | 0.432 |
| Dorsum (Right) (%) | 57.50 ± 35.39 | 72.33 ± 24.62 | 0.283 |
| Overall hand coverage (%) | 78.87 ± 18.06 | 85.19 ± 12.00 | 0.505 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suen, L.K.P.; Cheung, J.P.L. Effectiveness of “Hand Hygiene Fun Month” for Kindergarten Children: A Pilot Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2020, 17, 7264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197264
Suen LKP, Cheung JPL. Effectiveness of “Hand Hygiene Fun Month” for Kindergarten Children: A Pilot Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2020; 17(19):7264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197264
Chicago/Turabian StyleSuen, Lorna Kwai Ping, and Janet Pui Lee Cheung. 2020. "Effectiveness of “Hand Hygiene Fun Month” for Kindergarten Children: A Pilot Quasi-Experimental Study" International Journal of Environmental Research and Public Health 17, no. 19: 7264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197264