Children’s Environmental Health: A Systems Approach for Anticipating Impacts from Chemicals


 , and
, and
Abstract
:1. Introduction
2. The Complex Problem
2.1. Global Burden of Environmental Disease
2.2. Children’s Environmental Health in the United States
2.3. Additional Complexity
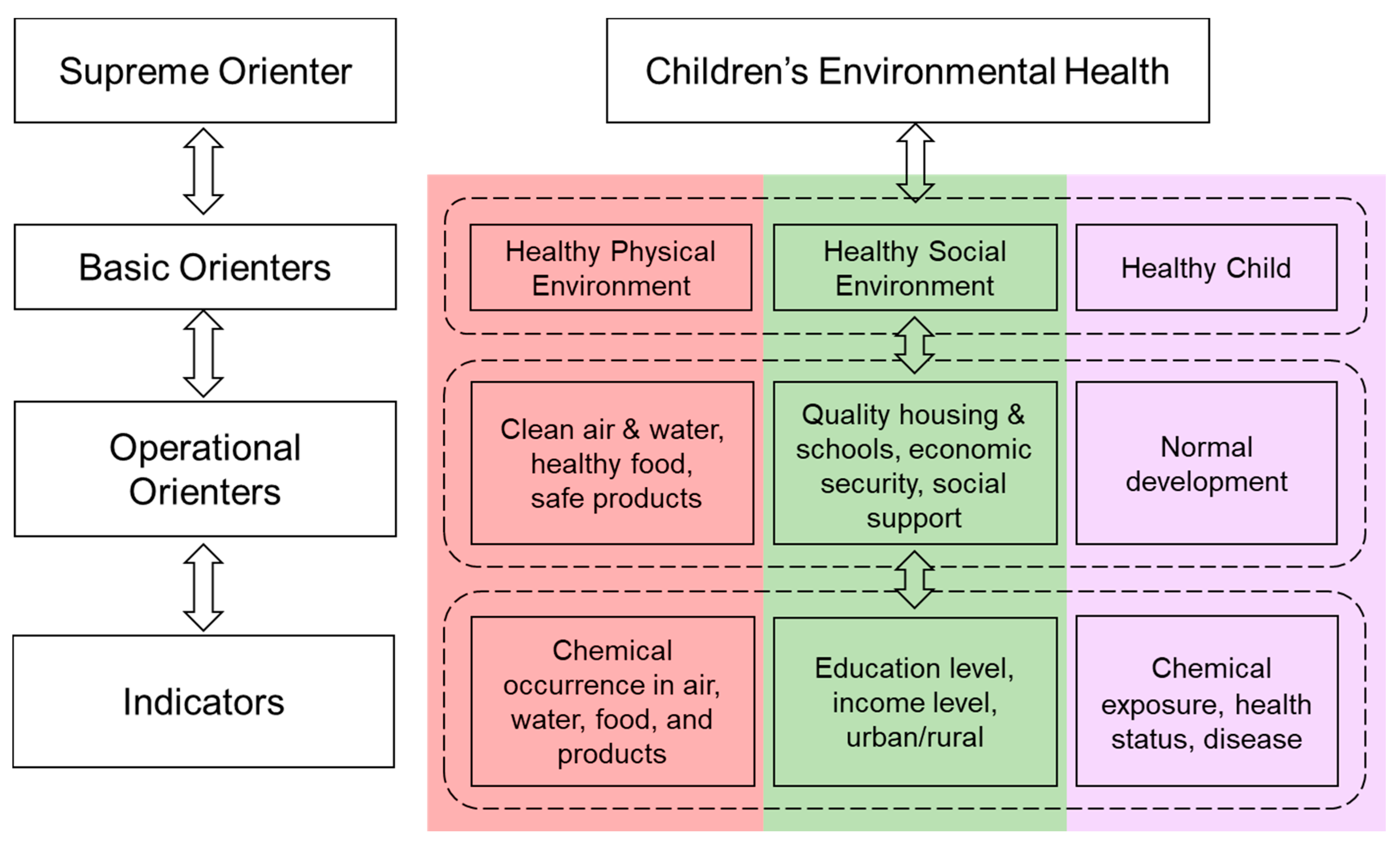
3. Conceptual Model of Children’s Environmental Health
4. A Systems Approach to Evaluate Impacts of Chemicals on Children’s Health
4.1. Children’s Environmental Health System Orienters
4.2. Children’s Environmental Health Indicators
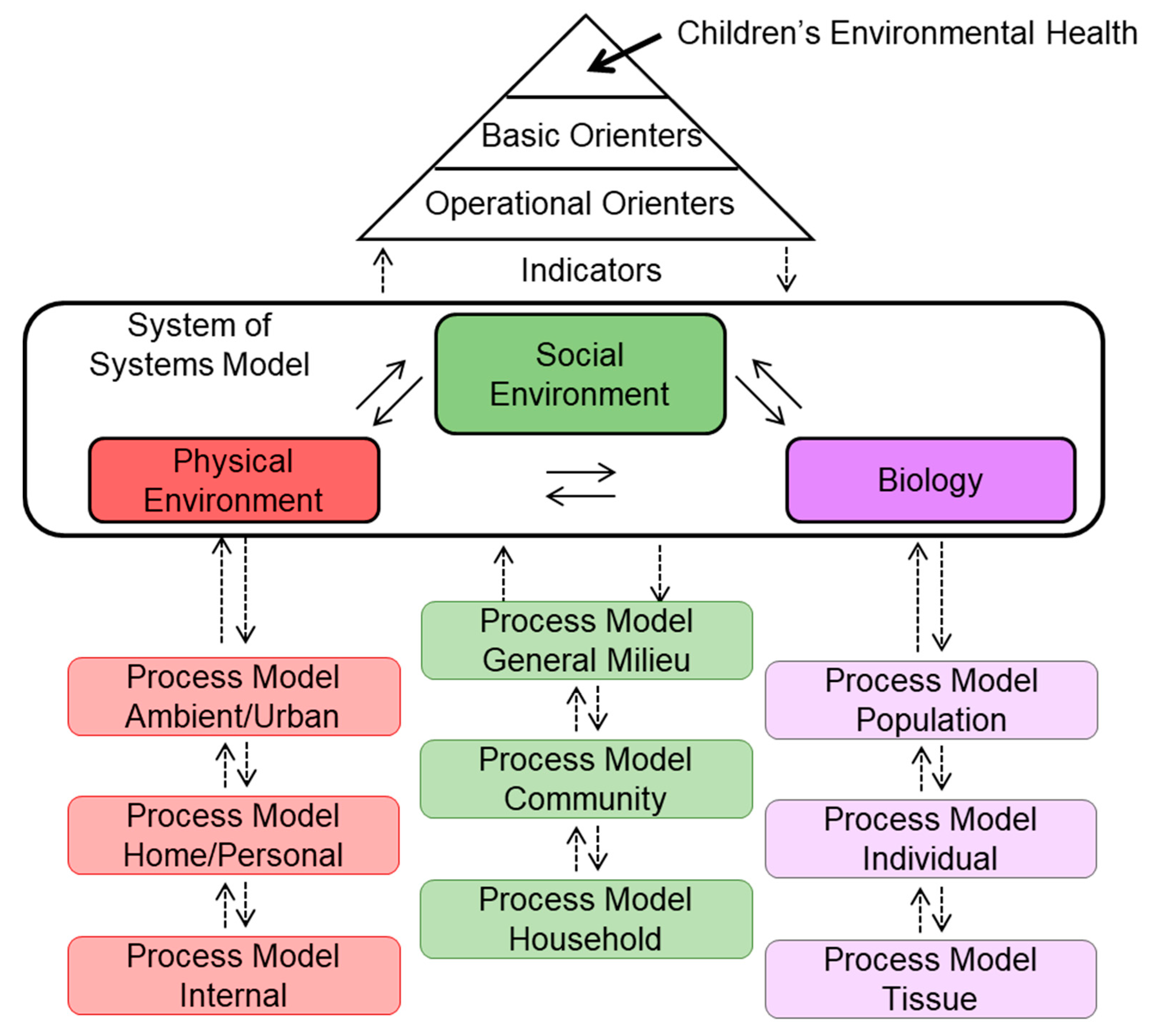
4.3. Implementing a System-Of-Systems Approach for Children’s Environmental Health
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Pool, R.; Rusch, E. Identifying and Reducing Environmental Health Risks of Chemicals in Our Society: Workshop Summary; Institue of Medicine/The National Academic Presses: Washington, DC, USA, 2014; p. 167. [Google Scholar]
- UNEP. Global Chemicals Outlook—Towards Sound Management of Chemicals. In Global Chemicals Outlook; UNEP: Geneva, Switzerland, 2013; p. 266. [Google Scholar]
- US EPA. Comptox Chemicals Dashboard. 2020. Available online: https://comptox.epa.gov/dashboard/chemical_lists (accessed on 21 May 2019).
- NAS. A Framework to Guide Selection of Chemical Alternatives: Committee on the Design and Evaluation of Safer Chemical Substitutions: A Framework to Inform Government and Industry Decisions; The National Academies Press: Washington, DC, USA, 2014; p. 264. [Google Scholar]
- NAS. Using 21st Century Science to Improve Risk-Related Evaluations; National Academy of the Sciences (NAS): Washington, DC, USA, 2017. [Google Scholar]
- Grandjean, P. Delayed discovery, dissemination, and decisions on intervention in environmental health: A case study on immunotoxicity of perfluorinated alkylate substances. Environ. Health 2018, 17, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, R.S.; Bahadori, T.; Buckley, T.J.; Cowden, J.; Deisenroth, C.; Dionisio, K.L.; Frithsen, J.B.; Grulke, C.M.; Gwinn, M.R.; Harrill, J.A.; et al. The Next Generation Blueprint of Computational Toxicology at the U.S. Environmental Protection Agency. Toxicol. Sci. 2019, 169, 317–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.; Suh, S. Health risks of chemicals in consumer products: A review. Environ. Int. 2019, 123, 580–587. [Google Scholar] [CrossRef]
- Lazarevic, N.; Barnett, A.G.; Sly, P.D.; Knibbs, L.D. Statistical Methodology in Studies of Prenatal Exposure to Mixtures of Endocrine-Disrupting Chemicals: A Review of Existing Approaches and New Alternatives. Environ. Health Perspect. 2019, 127, 026001. [Google Scholar] [CrossRef]
- Grandjean, P.; Landrigan, P.J. Neurobehavioural effects of developmental toxicity. Lancet Neurol. 2014, 13, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Braun, J.M. Early-life exposure to EDCs: Role in childhood obesity and neurodevelopment. Nat. Rev. Endocrinol. 2017, 13, 161–173. [Google Scholar] [CrossRef] [Green Version]
- Moosa, A.; Shu, H.; Sarachana, T.; Hu, V.W. Are endocrine disrupting compounds environmental risk factors for autism spectrum disorder? Horm. Behav. 2018, 101, 13–21. [Google Scholar] [CrossRef]
- Nowak, K.; Jabłońska, E.; Ratajczak-Wrona, W. Immunomodulatory effects of synthetic endocrine disrupting chemicals on the development and functions of human immune cells. Environ. Int. 2019, 125, 350–364. [Google Scholar] [CrossRef]
- Gwinn, M.R.; Axelrad, D.A.; Bahadori, T.; Bussard, D.; Cascio, W.E.; Deener, K.; Dix, D.; Thomas, R.S.; Kavlock, R.J.; Burke, T.A. Chemical Risk Assessment: Traditional vs Public Health Perspectives. Am. J. Public Health 2017, 107, 1032–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tulve, N. Development of a Conceptual Framework Depicting a Childs Total (Built, Natural, Social) Environment in Order to Optimize Health and Well-Being. J. Environ. Health Sci. 2016, 2, 1–8. [Google Scholar] [CrossRef]
- Lang, T.; Rayner, G. Ecological public health: The 21st century’s big idea? An essay by Tim Lang and Geof Rayner. BMJ 2012, 345, e5466. [Google Scholar] [CrossRef] [PubMed]
- Little, J.C.; Hester, E.T.; ElSawah, S.; Filz, G.M.; Sandu, A.; Carey, C.C.; Iwanaga, T.; Jakeman, A.J. A tiered, system-of-systems modeling framework for resolving complex socio-environmental policy issues. Environ. Model. Softw. 2019, 112, 82–94. [Google Scholar] [CrossRef]
- Neira, M.; Prüss-Ustün, A. Preventing Disease through Healthy Environments: A Global Assessment of the Environmental Burden of Disease; World Health Organization: France, Paris, 2016; p. 176. [Google Scholar]
- WHO. The Public Health Impact of Chemicals: Knowns and Unknowns. In International Programme on Chemical Safety; WHO: Geneva, Switzerland, 2016; p. 16. [Google Scholar]
- UNEP. Global Chemicals Outlook II—From Legacies to Innovatie Solutions. In Global Chemicals Outlook; UNEP: Geneva, Switzerland, 2019; p. 102. [Google Scholar]
- US EPA. Children’s Environmental Health Cross-Cutting Research Roadmap; US EPA: Washington, DC, USA, 2015; p. 128.
- CDC. Data & Statistics on Birth Defects. 23 January 2020. Available online: https://www.cdc.gov/ncbddd/birthdefects/data.html (accessed on 16 June 2020).
- Dadvand, P.; Parker, J.; Bell, M.L.; Bonzini, M.; Brauer, M.; Darrow, L.A.; Gehring, U.; Glinianaia, S.V.; Gouveia, N.; Ha, E.-H.; et al. Maternal Exposure to Particulate Air Pollution and Term Birth Weight: A Multi-Country Evaluation of Effect and Heterogeneity. Environ. Health Perspect. 2013, 121, 267–373. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, N.L.; Merialdi, M.; Van Donkelaar, A.; Vadillo-Ortega, F.; Martin, R.V.; Betran, A.P.; Souza, J.P.; O’neill, M.S. Outdoor Air Pollution, Preterm Birth, and Low Birth Weight: Analysis of the World Health Organization Global Survey on Maternal and Perinatal Health. Environ. Health Perspect. 2014, 122, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Boekelheide, K.; Blumberg, B.; Chapin, R.E.; Cote, I.; Graziano, J.H.; Janesick, A.; Lane, R.; Lillycrop, K.; Myatt, L.; States, J.C.; et al. Predicting Later-Life Outcomes of Early-Life Exposures. Environ. Health Perspect. 2012, 120, 1353–1361. [Google Scholar] [CrossRef]
- Gorini, F.; Chiappa, E.; Gargani, L.; Picano, E. Potential Effects of Environmental Chemical Contamination in Congenital Heart Disease. Pediatr. Cardiol. 2014, 35, 559–568. [Google Scholar] [CrossRef]
- CDC. Most Recent Asthma Data. 25 March 2019. Available online: https://www.cdc.gov/asthma/most_recent_data.htm (accessed on 16 June 2020).
- Dick, S.; Doust, E.; Cowie, H.; Ayres, J.G.; Turner, S. Associations between environmental exposures and asthma control and exacerbations in young children: A systematic review. BMJ Open 2014, 4, e003827. [Google Scholar] [CrossRef]
- Selgrade, M.K.; Blain, R.B.; Fedak, K.M.; Cawley, M.A. Potential risk of asthma associated with in utero exposure to xenobiotics. Birth Defects Res. Part C Embryo Today Rev. 2013, 99, 1–13. [Google Scholar] [CrossRef]
- Rigoli, L.; Briuglia, S.; Caimmi, S.; Ferraú, V.; Gallizzi, R.; Leonardi, S.; La Rosa, M.; Salpietro, C. Gene-environment interaction in childhood asthma. Int. J. Immunopathol. Pharmacol. 2011, 24, 41–47. [Google Scholar] [CrossRef] [Green Version]
- MacIntyre, E.A.; Gehring, U.; Moelter, A.; Fuertes, E.; Kluemper, C.; Kraemer, U.; Quass, U.; Hoffmann, B.; Gascon, M.; Brunekreef, B.; et al. Air Pollution and Respiratory Infections during Early Childhood: An Analysis of 10 European Birth Cohorts within the ESCAPE Project. Environ. Health Perspect. 2014, 122, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Kabesch, M. Epigenetics in asthma and allergy. Curr. Opin. Allergy Clin. Immunol. 2014, 14, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Salam, M.T.; Zhang, Y.; Begum, K. Epigenetics and childhood asthma: Current evidence and future research directions. Epigenomics 2012, 4, 415–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC. Key Findings: Trends in the Prevalence of Developmental Disabilities in U.S. Children, 1997–2008. Developmental Disabilities 9 April 2018. Available online: https://www.cdc.gov/ncbddd/developmentaldisabilities/features/birthdefects-dd-keyfindings.html (accessed on 16 June 2020).
- Bellinger, D.C. Prenatal Exposures to Environmental Chemicals and Children’s Neurodevelopment: An Update. Saf. Health Work 2013, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Choi, A.L.; Sun, G.; Zhang, Y.; Grandjean, P. Developmental Fluoride Neurotoxicity: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2012, 120, 1362–1368. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.R.; Harden, F.; Toms, L.-M.L.; Norman, R.E. Health consequences of exposure to brominated flame retardants: A systematic review. Chemosphere 2014, 106, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Barranco, M.; Lacasaña, M.; Aguilar-Garduño, C.; Alguacil, J.; Gil, F.; González-Alzaga, B.; Rojas-García, A. Association of arsenic, cadmium and manganese exposure with neurodevelopment and behavioural disorders in children: A systematic review and meta-analysis. Sci. Total Environ. 2013, 454–455, 562–577. [Google Scholar] [CrossRef]
- Perera, F.; Herbstman, J. Prenatal environmental exposures, epigenetics, and disease. Reprod. Toxicol. 2011, 31, 363–373. [Google Scholar] [CrossRef] [Green Version]
- Perera, F.P.; Tang, D.; Wang, S.; Vishnevetsky, J.; Zhang, B.; Diaz, D.; Camann, D.; Rauh, V. Prenatal Polycyclic Aromatic Hydrocarbon (PAH) Exposure and Child Behavior at Age 6–7 Years. Environ. Health Perspect. 2012, 120, 921–926. [Google Scholar] [CrossRef] [Green Version]
- Nilsen, F.M.; Tulve, N.S. A systematic review and meta-analysis examining the interrelationships between chemical and non-chemical stressors and inherent characteristics in children with ADHD. Environ. Res. 2020, 180, 108884. [Google Scholar] [CrossRef]
- CDC. Prevalence of Childhood Obesity in the United States. Overweight and Obestiy: Childhood Obesity Facts 24 June 2019. Available online: https://www.cdc.gov/obesity/data/childhood.html (accessed on 16 June 2020).
- Gaston, S.A.; Tulve, N.S.; Ferguson, T.F. Abdominal obesity, metabolic dysfunction, and metabolic syndrome in U.S. adolescents: National Health and Nutrition Examination Survey 2011–2016. Ann. Epidemiol. 2019, 30, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Lichtveld, K.; Thomas, K.; Tulve, N.S. Chemical and non-chemical stressors affecting childhood obesity: A systematic scoping review. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hines, R.N.; Sargent, D.; Autrup, H.; Birnbaum, L.S.; Brent, R.L.; Doerrer, N.G.; Hubal, E.A.C.; Juberg, D.R.; Laurent, C.; Luebke, R.; et al. Approaches for Assessing Risks to Sensitive Populations: Lessons Learned from Evaluating Risks in the Pediatric Population. Toxicol. Sci. 2009, 113, 4–26. [Google Scholar] [CrossRef] [PubMed]
- Selevan, S.G.; Kimmel, C.A.; Mendola, P. Identifying critical windows of exposure for children’s health. Environ. Health Perspect. 2000, 108, 451–455. [Google Scholar] [CrossRef]
- Wright, R.O. Environment, susceptibility windows, development, and child health. Curr. Opin. Pediatr. 2017, 29, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubal, E.A.C.; De Wet, T.; Du Toit, L.; Firestone, M.P.; Ruchirawat, M.; Van Engelen, J.; Vickers, C. Identifying important life stages for monitoring and assessing risks from exposures to environmental contaminants: Results of a World Health Organization review. Regul. Toxicol. Pharmacol. 2014, 69, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Defur, P.L.; Evans, G.W.; Hubal, E.A.C.; Kyle, A.D.; Morello-Frosch, R.; Williams, D.R. Vulnerability as a Function of Individual and Group Resources in Cumulative Risk Assessment. Environ. Health Perspect. 2007, 115, 817–824. [Google Scholar] [CrossRef]
- Heindel, J.J.; Skalla, L.A.; Joubert, B.R.; Dilworth, C.H.; Gray, K.A. Review of developmental origins of health and disease publications in environmental epidemiology. Reprod. Toxicol. 2017, 68, 34–48. [Google Scholar] [CrossRef]
- Bossel, H. Systems and Models: Complexity, Dynamics, Evolution, Sustainability; BoD–Books on Demand: Norderstedt, Germany, 2007. [Google Scholar]
- Little, J.C.; Hester, E.T.; Carey, C.C. Assessing and Enhancing Environmental Sustainability: A Conceptual Review. Environ. Sci. Technol. 2016, 50, 6830–6845. [Google Scholar] [CrossRef]
- Bossel, H. Indicators for Sustainable Development: Theory, Method, Applications; International Institute for Sustainable Development: Winnipeg, MB, Canada, 1999. [Google Scholar]
- Fraser, E.D.; Dougill, A.J.; Mabee, W.E.; Reed, M.; McAlpine, P. Bottom up and top down: Analysis of participatory processes for sustainability indicator identification as a pathway to community empowerment and sustainable environmental management. J. Environ. Manag. 2006, 78, 114–127. [Google Scholar] [CrossRef]
- Paracchini, M.L.; Pacini, C.; Jones, M.L.M.; Pérez-Soba, M.; Pacini, G.C. An aggregation framework to link indicators associated with multifunctional land use to the stakeholder evaluation of policy options. Ecol. Indic. 2011, 11, 71–80. [Google Scholar] [CrossRef]
- Bossel, H. Deriving indicators of sustainable development. Environ. Model. Assess. 1996, 1, 193–218. [Google Scholar] [CrossRef]
- EPA’s Report on the Environment (ROE). 2019. Available online: https://www.epa.gov/report-environment (accessed on 20 September 2019).
- U.S. EPA. America’s Children and the Environment. United States Environmental Protection Agency. 2013. Available online: https://www.epa.gov/americaschildrenenvironment (accessed on 9 November 2020).
- U.S. EPA. Comptox Chemicals Dashboard. 2020. Available online: https://comptox.epa.gov/dashboard (accessed on 21 May 2019).
- Comparative Toxicogenomics Database (CTD). Available online: https://ctdbase.org/ (accessed on 9 November 2020).
- EnviroAtlas. EPA: Environmental Protection. 2019. Available online: https://www.epa.gov/enviroatlas (accessed on 9 November 2020).
- ToxPi: Toxicological Prioritization Index. 2020. Available online: https://toxpi.org/ (accessed on 9 November 2020).
- Marvel, S.W.; To, K.; Grimm, F.A.; Wright, F.A.; Rusyn, I.; Reif, D.M. ToxPi Graphical User Interface 2.0: Dynamic exploration, visualization, and sharing of integrated data models. BMC Bioinform. 2018, 19, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gangwal, S.; Reif, D.; Mosher, S.; Egeghy, P.P.; Wambaugh, J.F.; Judson, R.S.; Hubal, E.A.C. Incorporating exposure information into the toxicological prioritization index decision support framework. Sci. Total Environ. 2012, 435–436, 316–325. [Google Scholar] [CrossRef]
- Sipes, N.S.; Martin, M.T.; Reif, D.M.; Kleinstreuer, N.C.; Judson, R.S.; Singh, A.V.; Chandler, K.J.; Dix, D.J.; Kavlock, R.J.; Knudsen, T.B. Predictive Models of Prenatal Developmental Toxicity from ToxCast High-Throughput Screening Data. Toxicol. Sci. 2011, 124, 109–127. [Google Scholar] [CrossRef]
- Smith, M.N.; Hubal, E.A.C.; Faustman, E.M. A Case study on the utility of predictive toxicology tools in alternatives assessments for hazardous chemicals in children’s consumer products. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 160–170. [Google Scholar] [CrossRef]
- Kids Count Data Center: North Carolina Indicators. Available online: https://datacenter.kidscount.org/data#NC/2/0/char/0 (accessed on 28 October 2020).
- EPA, U.S. TRI Data and Tools. 2020. Available online: https://www.epa.gov/toxics-release-inventory-tri-program/tri-data-and-tools (accessed on 12 November 2019).
- EPA, U.S. Superfund: National Priorities List (NPL). 2020. Available online: https://www.epa.gov/superfund/superfund-national-priorities-list-npl (accessed on 12 November 2019).
- Explorer, S. Social Explorer Maps: All United States Data. 2020. Available online: https://www.socialexplorer.com/explore-maps (accessed on 10 September 2020).
- ElSawah, S.; Filatova, T.; Jakeman, A.J.; Kettner, A.J.; Zellner, M.L.; Athanasiadis, I.N.; Hamilton, S.H.; Axtell, R.L.; Brown, D.G.; Gilligan, J.M.; et al. Eight grand challenges in socio-environmental systems modeling. Socio Environ. Syst. Model. 2020, 2, 16226. [Google Scholar] [CrossRef] [Green Version]
- Sterman, J.D. System Dynamics Modeling: Tools for Learning in a Complex World. Calif. Manag. Rev. 2001, 43, 8–25. [Google Scholar] [CrossRef]
- Sterman, J.D. Sustaining Sustainability: Creating a Systems Science in a Fragmented Academy and Polarized World: Sustainability Science: The Emerging Paradigm and the Urban Environment; Springer Science and Business Media LLC: New York, NY, USA, 2012; pp. 21–58. [Google Scholar]
- Krueger, T.; Page, T.; Hubacek, K.; Smith, L.; Hiscock, K. The role of expert opinion in environmental modelling. Environ. Model. Softw. 2012, 36, 4–18. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resource | Description |
|---|---|
| Report on the Environment (ROE), US EPA [58] | The ROE shows how the condition of the US environment and human health is changing over time. The purpose of the 80+ ROE indicators is to help answer 23 questions critical to US EPA’s mission of protecting the environment and human health. |
| America’s Children and the Environment (ACE), US EPA, 3rd edition [59] | The ACE reports data on children’s environmental health. ACE brings together information from a variety of sources to provide national indicators in the following areas: Environments and Contaminants, Biomonitoring, and Health. |
| EPA CompTox Chemicals Dashboard [60] | A web-based resource for identifying available information on chemicals. It provides access to thousands of chemicals and associated experimental and predicted properties, high-throughput bioactivity data, links to existing Adverse Outcome Pathways (AOPs), and product and functional use data for thousands of chemicals. |
| CTD (Comparative Toxicogenomics Database) [61] | The CTD is a robust, publicly available database that provides manually curated information about chemical–gene/protein interactions and chemical–disease and gene–disease relationships. These data are integrated with functional and pathway data. The goal is to advance understanding of how environmental exposures impact human health. |
| EnviroAtlas [62] | EnviroAtlas is a web-based tool that provides geospatial data, integrated indicators, and other resources related to ecosystem services, chemical and nonchemical stressors impacting the environment, and human health. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cohen Hubal, E.A.; Reif, D.M.; Slover, R.; Mullikin, A.; Little, J.C. Children’s Environmental Health: A Systems Approach for Anticipating Impacts from Chemicals. Int. J. Environ. Res. Public Health 2020, 17, 8337. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228337
Cohen Hubal EA, Reif DM, Slover R, Mullikin A, Little JC. Children’s Environmental Health: A Systems Approach for Anticipating Impacts from Chemicals. International Journal of Environmental Research and Public Health. 2020; 17(22):8337. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228337
Chicago/Turabian StyleCohen Hubal, Elaine A., David M. Reif, Rachel Slover, Ashley Mullikin, and John C. Little. 2020. "Children’s Environmental Health: A Systems Approach for Anticipating Impacts from Chemicals" International Journal of Environmental Research and Public Health 17, no. 22: 8337. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228337