Effect of a Simulated Match on Lower Limb Neuromuscular Performance in Youth Footballers—A Two Year Longitudinal Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
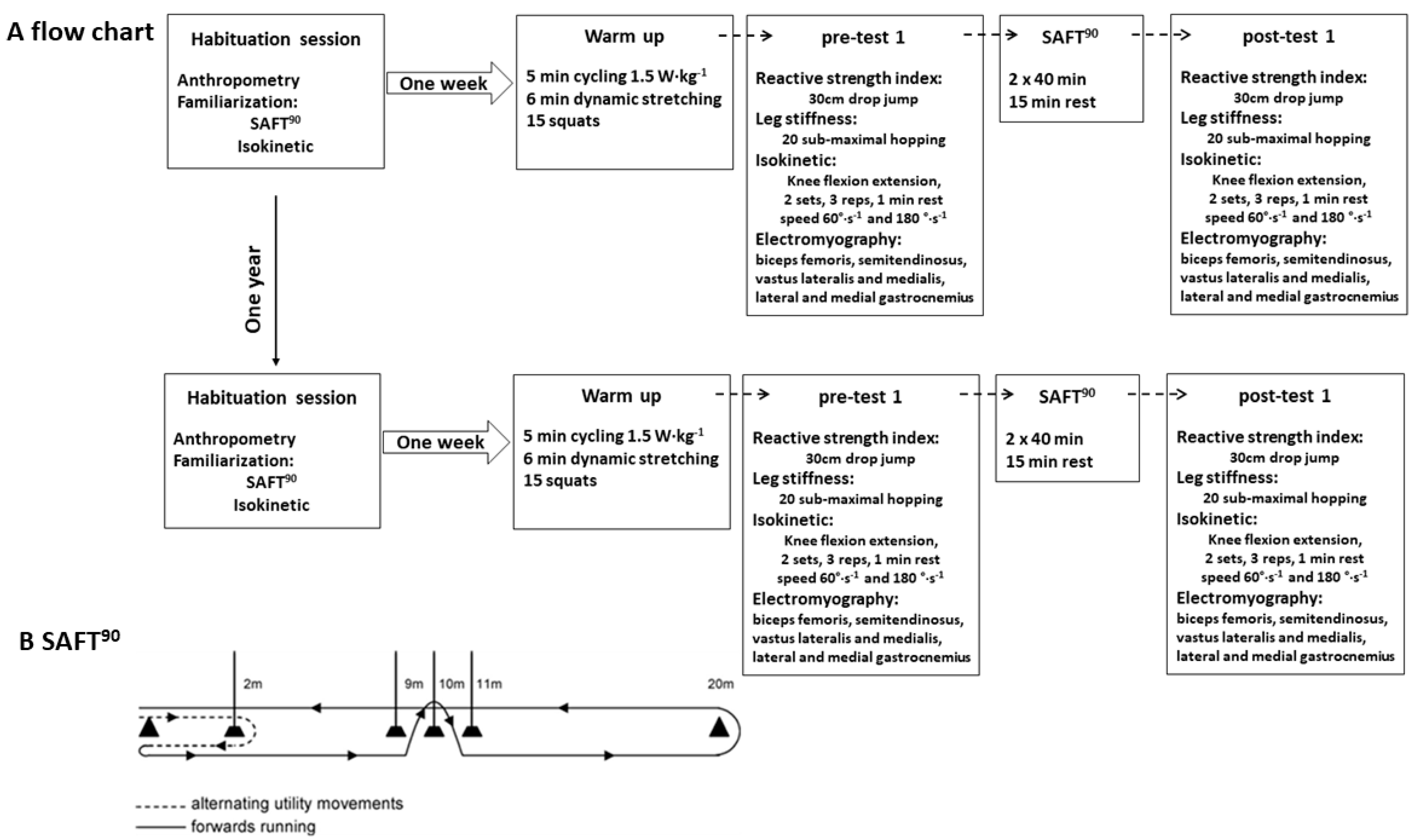
2.2. Procedures
2.3. Isokinetic Dynamometry
2.4. EMG
2.5. Measurements of Reactive Strength Index
2.6. Leg Stiffness
2.7. Fatigue Protocol
2.8. Statistical Analysis
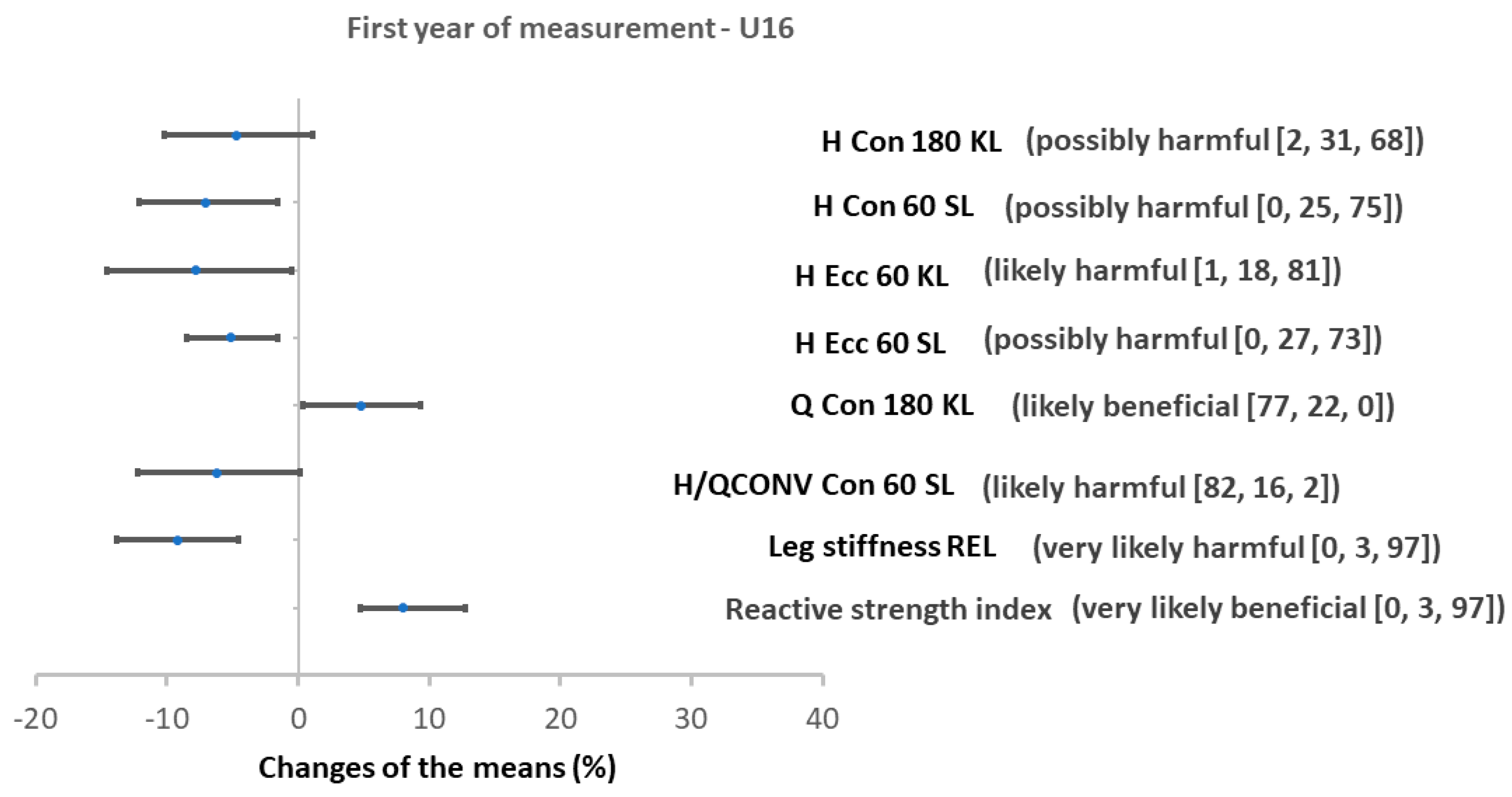
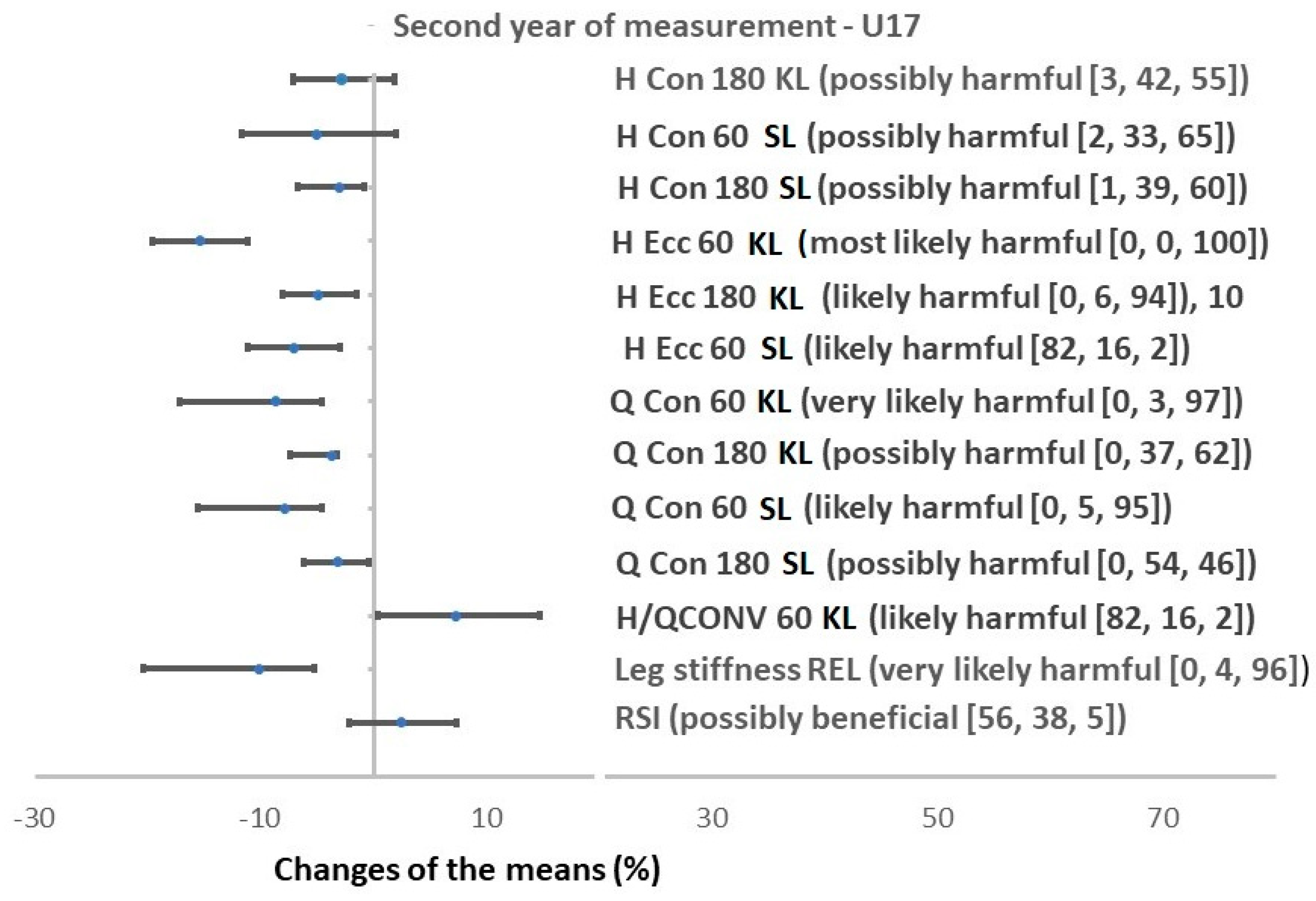
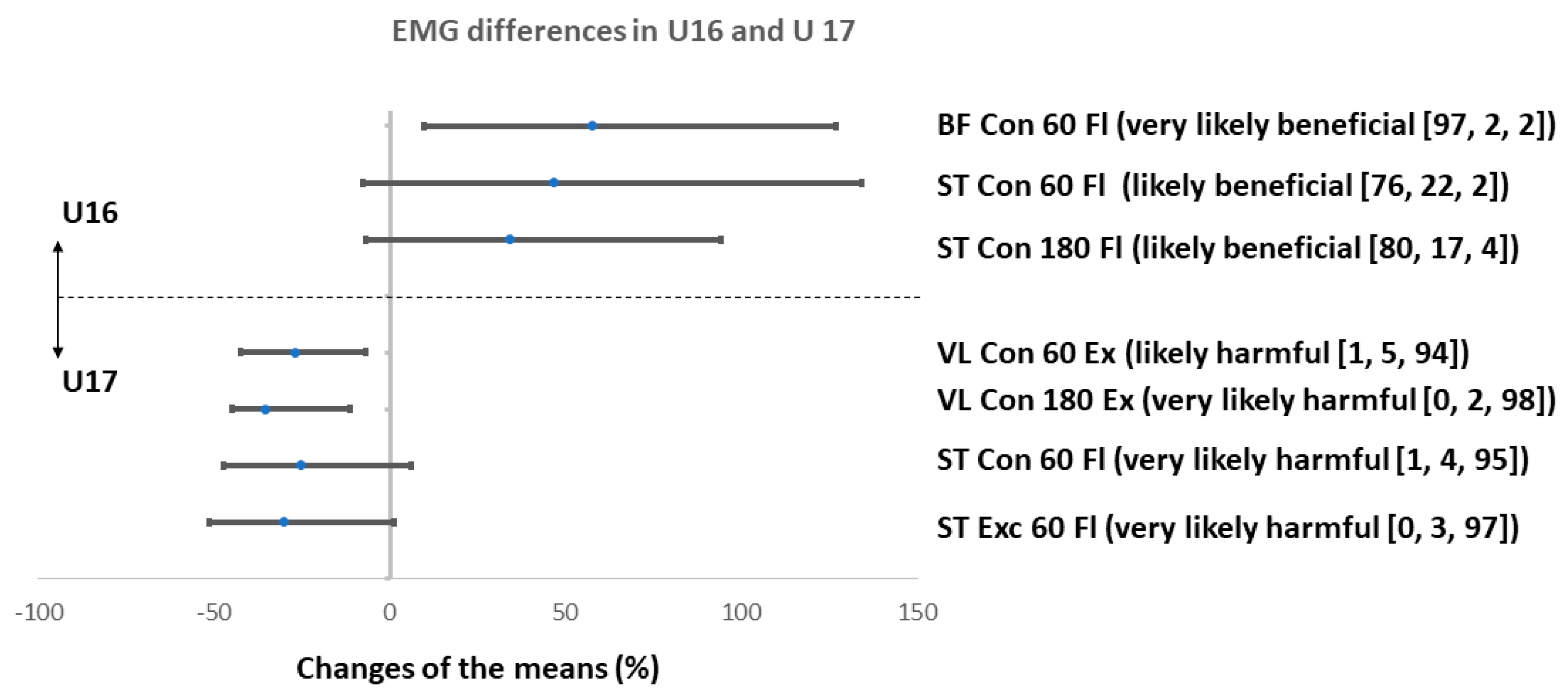
3. Results
4. Discussion
4.1. Changes in Torque Production in Hamstrings
4.2. Changes in Torque Production in Quadriceps
4.3. Changes in H/Q Ratios
4.4. Changes in EMG
4.5. Changes in Leg Stiffness
4.6. Changes in RSI
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Los Arcos Larumbe, A.; Mendiguchia, J.; Yanci, J. Specificity of jumping, acceleration and quick change-of-direction motor abilities in soccer players. Kinesiology 2017, 49, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Malý, T.; Zahálka, F.; Malá, L.; Teplan, J. Profile, correlation and structure of speed in youth elite soccer players. J. Hum. Kinet. 2014, 40, 149–159. [Google Scholar] [CrossRef] [Green Version]
- Stølen, T.; Chamari, K.; Castagna, C.; Wisløff, U. Physiology of soccer: An update. Sports Med. 2005, 35, 501–536. [Google Scholar] [CrossRef] [PubMed]
- Bastos, F.N.; Vanderlei, F.M.; Vanderlei, L.C.M.; Júnior, J.N.; Pastre, C.M. Investigation of characteristics and risk factors of sports injuries in young soccer players: A retrospective study. Int. Arch. Med. 2013, 6, 14. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. An audit of injuries in six English professional soccer academies. J. Sports Sci. 2018, 36, 1542–1548. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Waldén, M.; Hägglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sports Med. 2016, 50, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Waldén, M.; Hägglund, M.; Werner, J.; Ekstrand, J. The epidemiology of anterior cruciate ligament injury in football (soccer): A review of the literature from a gender-related perspective. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of injury incidences in male professional adult and elite youth soccer players: A systematic review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [Green Version]
- Waldén, M.; Hägglund, M.; Magnusson, H.; Ekstrand, J. ACL injuries in men’s professional football: A 15-year prospective study on time trends and return-to-play rates reveals only 65% of players still play at the top level 3 years after ACL rupture. Br. J. Sports Med. 2016, 50, 744–750. [Google Scholar] [CrossRef] [Green Version]
- Greig, M. The influence of soccer-specific fatigue on peak isokinetic torque production of the knee flexors and extensors. Am. J. Sports Med. 2008, 36, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Padua, D.A.; Arnold, B.L.; Perrin, D.H.; Gansneder, B.M.; Carcia, C.R.; Granata, K.P. Fatigue, vertical leg stiffness, and stiffness control strategies in males and females. J. Athl. Train. 2006, 41, 294–304. [Google Scholar] [PubMed]
- Maly, T.; Sugimoto, D.; Izovska, J.; Zahalka, F.; Mala, L. Effect of muscular strength, asymmetries and fatigue on kicking performance in soccer players. Int. J. Sports Med. 2018, 39, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Freckleton, G.; Pizzari, T. Risk factors for hamstring muscle strain injury in sport: A systematic review and meta-analysis. Br. J. Sports Med. 2013, 47, 351–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, J.F.; Akenhead, R.; Russell, M.; Hicks, K.M.; Hayes, P.R. Sensitivity and reproducibility of a fatigue response in elite youth football players. Sci. Med. Footb. 2019, 3, 214–220. [Google Scholar] [CrossRef]
- Huygaerts, S.; Cos, F.; Cohen, D.D.; Calleja-González, J.; Guitart, M.; Blazevich, A.J.; Alcaraz, P.E. Mechanisms of hamstring strain injury: Interactions between fatigue, muscle activation and function. Sports 2020, 8, 65. [Google Scholar] [CrossRef] [PubMed]
- Maly, T.; Zahalka, F.; Mala, L. Unilateral and ipsilateral strength asymmetries in elite youth soccer players with respect to muscle group and limb dominance. Int. J. Morphol. 2016, 34, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- McCall, A.; Carling, C.; Davison, M.; Nedelec, M.; Le Gall, F.; Berthoin, S.; Dupont, G. Injury risk factors, screening tests and preventative strategies: A systematic review of the evidence that underpins the perceptions and practices of 44 football (soccer) teams from various premier leagues. Br. J. Sports Med. 2015, 49, 583–589. [Google Scholar] [CrossRef]
- Hughes, G.; Watkins, J. A risk-factor model for anterior cruciate ligament injury. Sports Med. 2006, 36, 411–428. [Google Scholar] [CrossRef]
- Osternig, L.R. Assessing human performance. In Isokinetics in Human Performance; Brown, E., Ed.; Human Kinetics: Champaign, IL, USA, 2000; pp. 77–96. [Google Scholar]
- Alentorn-Geli, E.; Myer, G.D.; Silvers, H.J.; Samitier, G.; Romero, D.; Lázaro-Haro, C.; Cugat, R. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 705–729. [Google Scholar] [CrossRef]
- Dauty, M.; Potiron-Josse, M.; Rochcongar, P. Identification of previous hamstring muscle injury by isokinetic concentric and eccentric torque measurement in elite soccer player. Isokinet. Exerc. Sci. 2003, 11, 139–144. [Google Scholar] [CrossRef]
- Chappell, J.D.; Creighton, R.A.; Giuliani, C.; Yu, B.; Garrett, W.E. Kinematics and electromyography of landing preparation in vertical stop-jump: Risks for noncontact anterior cruciate ligament injury. Am. J. Sports Med. 2007, 35, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Woods, C.; Hawkins, R.D.; Maltby, S.; Hulse, M.; Thomas, A.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football—Analysis of hamstring injuries. Br. J. Sports Med. 2004, 38, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahnama, N.; Reilly, T.; Lees, A.; Graham-Smith, P. Muscle fatigue induced by exercise simulating the work rate of competitive soccer. J. Sports Sci. 2003, 21, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Morgan, D.L.; Brockett, C.L.; Percival, P. Identifying athletes at risk of hamstring strains and how to protect them. Clin. Exp. Pharmacol. Physiol. 2004, 31, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Croisier, J.L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef]
- Verrall, G.M.; Slavotinek, J.P.; Barnes, P.G.; Fon, G.T.; Spriggins, A.J. Clinical risk factors for hamstring muscle strain injury: A prospective study with correlation of injury by magnetic resonance imaging. Br. J. Sports Med. 2001, 35, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Melnyk, M.; Gollhofer, A. Submaximal fatigue of the hamstrings impairs specific reflex components and knee stability. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 525–532. [Google Scholar] [CrossRef]
- Rozzi, S.L.; Lephart, S.M.; Fu, F.H. Effects of muscular fatigue on knee joint laxity and neuromuscular characteristics of male and female athletes. J. Athl. Train. 1999, 34, 106–114. [Google Scholar]
- Booysen, M.J.; West, N.; Constantinou, D. P-85 The relationships of eccentric and concentric isokinetic strength with sprinting speed in male sub-elite footballers. Br. J. Sports Med. 2016, 50, A79. [Google Scholar] [CrossRef]
- Cotte, T.; Chatard, J.C. Isokinetic strength and sprint times in English Premier League football players. Biol. Sport 2011, 28, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Wollin, M.; Thorborg, K.; Pizzari, T. The acute effect of match play on hamstring strength and lower limb flexibility in elite youth football players. Scand. J. Med. Sci. Sports 2017, 27, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Sangnier, S.; Tourny-Chollet, C. Comparison of the decrease in strength between hamstrings and quadriceps during isokinetic fatigue testing in semiprofessional soccer players. Int. J. Sports Med. 2007, 28, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Small, K.; McNaughton, L.; Greig, M.; Lovell, R. The effects of multidirectional soccer-specific fatigue on markers of hamstring injury risk. J. Sci. Med. Sport 2010, 13, 120–125. [Google Scholar] [CrossRef]
- Delextrat, A.; Gregory, J.; Cohen, D. The use of the functional H:Q ratio to assess fatigue in soccer. Int. J. Sports Med. 2010, 31, 192–197. [Google Scholar] [CrossRef]
- Lehnert, M.; De Ste Croix, M.; Xaverova, Z.; Botek, M.; Varekova, R.; Zaatar, A.; Lastovicka, O.; Stastny, P. Changes in injury risk mechanisms after soccer-specific fatigue in male youth soccer players. J. Hum. Kinet. 2018, 62, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Lehnert, M.; De Ste Croix, M.; Zaatar, A.; Hughes, J.; Varekova, R.; Lastovicka, O. Muscular and neuromuscular control following soccer-specific exercise in male youth: Changes in injury risk mechanisms. Scand. J. Med. Sci. Sports 2017, 27, 975–982. [Google Scholar] [CrossRef]
- Toumi, H.; Poumarat, G.; Best, T.M.; Martin, A.; Fairclough, J.; Benjamin, M. Fatigue and muscle-tendon stiffness after stretch-shortening cycle and isometric exercise. Appl. Physiol. Nutr. Metab. 2006, 31, 565–572. [Google Scholar] [CrossRef]
- Shultz, S.J.; Perrin, D.H. Using surface electromyography to assess sex differences in neuromuscular response characteristics. J. Athl. Train. 1999, 34, 165–176. [Google Scholar]
- De Luca, C.J. The use of surface electromyography in biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef] [Green Version]
- Thongpanja, S.; Phinyomark, A.; Phukpattaranont, P.; Limsakul, C. Mean and median frequency of EMG signal to determine muscle force based on time dependent power spectrum. Elektron. Elektrotech. 2013, 19, 51–56. [Google Scholar] [CrossRef]
- De Ste Croix, M.; Lehnert, M.; Maixnerova, E.; Zaatar, A.; Svoboda, Z.; Botek, M.; Varekova, R.; Stastny, P. Does maturation influence neuromuscular performance and muscle damage after competitive match-play in youth male soccer players? Eur. J. Sport Sci. 2019, 19, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Riemann, B.L.; Myers, J.B.; Lephart, S.M. Comparison of the ankle, knee, hip, and trunk corrective action shown during single-leg stance on firm, foam, and multiaxial surfaces. Arch. Phys. Med. Rehabil. 2003, 84, 90–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, J.L.; De Ste Croix, M.B.A.; Lloyd, R.S.; Williams, C.A. Altered neuromuscular control of leg stiffness following soccer-specific exercise. Eur. J. Appl. Physiol. 2014, 114, 2241–2249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehnert, M.; De Ste Croix, M.; Šťastný, P.; Maixnerová, E.; Zaatar, A.; Botek, M.; Vařeková, R.; Hůlka, K.; Petr, M.; Elfmark, M.; et al. The Influence of Fatigue on Injury Risk in Male Youth Soccer; Palacky University Olomouc: Olomouc, Czech Republic, 2019; p. 182. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Oliver, J.L.; Hughes, M.G.; Williams, C.A. Reliability and validity of field-based measures of leg stiffness and reactive strength index in youths. J. Sports Sci. 2009, 27, 1565–1573. [Google Scholar] [CrossRef]
- Flanagan, E.P.; Comyns, T.M. The use of contact time and the reactive strength index to optimize fast stretch-shortening cycle training. Str. Cond. J. 2008, 30, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Young, W. Laboratory strength assessment of athletes. New Stud. Athl. 1995, 10, 88–96. [Google Scholar]
- Raschner, C.; Platzer, H.P.; Patterson, C.; Werner, I.; Huber, R.; Hildebrandt, C. The relationship between ACL injuries and physical fitness in young competitive ski racers: A 10-year longitudinal study. Br. J. Sports Med. 2012, 46, 1065–1071. [Google Scholar] [CrossRef]
- Parkkari, J.; Pasanen, K.; Manila, V.M.; Kannus, P.; Rimpelä, A. The risk for a cruciate ligament injury of the knee in adolescents and young adults: A population-based cohort study of 46 500 people with a 9 year follow-up. Br. J. Sports Med. 2008, 42, 422–426. [Google Scholar] [CrossRef]
- Flanagan, E.P.; Ebben, W.P.; Jensen, R.L. Reliability of the reactive strength index and time to stabilization during depth jumps. J. Strength Cond. Res. 2008, 22, 1677–1682. [Google Scholar] [CrossRef] [Green Version]
- Van Der Sluis, A.; Elferink-Gemser, M.T.; Coelho-E-Silva, M.J.; Nijboer, J.A.; Brink, M.S.; Visscher, C. Sport injuries aligned to peak height velocity in talented pubertal soccer players. Int. J. Sports Med. 2014, 35, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Rumpf, M.C.; Cronin, J. Injury incidence, body site, and severity in soccer players aged 6–18 years: Implications for injury prevention. Strength Cond. J. 2012, 34, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Shea, K.G.; Pfeiffer, R.; Jo, H.W.; Curtin, M.; Apel, P.J. Anterior cruciate ligament injury in pediatric and adolescent soccer players: An analysis of insurance data. J. Pediatr. Orthop. 2004, 24, 623–628. [Google Scholar] [CrossRef] [PubMed]
- De Ste Croix, M.B.A.; Priestley, A.M.; Lloyd, R.S.; Oliver, J.L. ACL injury risk in elite female youth soccer: Changes in neuromuscular control of the knee following soccer-specific fatigue. Scand. J. Med. Sci. Sports 2015, 25, e531–e538. [Google Scholar] [CrossRef]
- De Ste Croix, M.B.A. Protect Her Knees—Exploring the Role of Football Specific Fatigue on Dynamic Knee Stability in Female Youth Football Players; Project Report funded by UEFA Research Grant programme; UEFA: Basel, Switzerland, 2012. [Google Scholar]
- Cohen, R.; Mitchell, C.; Dotan, R.; Gabriel, D.; Klentrou, P.; Falk, B. Do neuromuscular adaptations occur in endurance-trained boys and men? Appl. Physiol. Nutr. Metab. 2010, 35, 471–479. [Google Scholar] [CrossRef]
- Oliver, J.L.; Smith, P.M. Neural control of leg stiffness during hopping in boys and men. J. Electromyogr. Kinesiol. 2010, 20, 973–979. [Google Scholar] [CrossRef]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar]
- Dirnberger, J.; Wiesinger, H.P.; Kösters, A.; Müller, E. Reproducibility for isometric and isokinetic maximum knee flexion and extension measurements using the IsoMed 2000-dynamometer. Isokinet. Exerc. Sci. 2012, 20, 149–153. [Google Scholar] [CrossRef]
- De Araujo Ribeiro Alvares, J.B.; Rodrigues, R.; de Azevedo Franke, R.; da Silva, B.G.C.; Pinto, R.S.; Vaz, M.A.; Baroni, B.M. Inter-machine reliability of the Biodex and Cybex isokinetic dynamometers for knee flexor/extensor isometric, concentric and eccentric tests. Phys. Ther. Sport 2015, 16, 59–65. [Google Scholar] [CrossRef]
- Sleivert, G.G.; Wenger, H.A. Reliability of measuring isometric and isokinetic peak torque, rate of torque development, integrated electromyography, and tibial nerve conduction velocity. Arch. Phys. Med. Rehabil. 1994, 75, 1315–1321. [Google Scholar] [CrossRef]
- Konrad, P. The ABC of EMG: A Practical Introduction to Kinesiological Electromyography; Noraxon: Scottsdale, AZ, USA, 2005; p. 61. [Google Scholar]
- Dalleau, G.; Belli, A.; Viale, F.; Lacour, J.R.; Bourdin, M. A simple method for field measurements of leg stiffness in hopping. Int. J. Sports Med. 2004, 25, 170–176. [Google Scholar] [CrossRef] [PubMed]
- De Ste Croix, M.B.A.; Hughes, J.D.; Lloyd, R.S.; Oliver, J.L.; Read, P.J. Leg stiffness in female soccer players: Intersession reliability and the fatiguing effects of soccer-specific exercise. J. Strength Cond. Res. 2017, 31, 3052–3058. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. Spreadsheets for analysis of controlled trials, crossovers and time series. Sportscience 2017, 21, 1–4. [Google Scholar]
- Greenland, S. Valid P-Values behave exactly as they should: Some misleading criticisms of P-Values and their resolution with S-Values. Am. Stat. 2019, 73, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.G. A spreadsheet for combining outcomes from several subject groups. Sportscience 2006, 10, 46–50. [Google Scholar]
- Rosenthal, R. Parametric measures of effect size. In The Handbook of Research Synthesis; Cooper, H., Hedges, L.V., Eds.; Russel Sage Foundation: New York, NY, USA, 1994; pp. 231–244. [Google Scholar]
- Hawkins, R.D.; Hulse, M.A.; Wilkinson, C.; Hodson, A.; Gibson, M. The association football medical research programme: An audit of injuries in professional football. Br. J. Sports Med. 2001, 35, 43–47. [Google Scholar] [CrossRef]
- Mair, S.D.; Seaber, A.V.; Glisson, R.R.; Garrett, W.E., Jr. The role of fatigue in susceptibility to acute muscle strain injury. Am. J. Sports Med. 1996, 24, 137–143. [Google Scholar] [CrossRef]
- Coombs, R.; Garbutt, G. Developments in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J. Sports Sci. Med. 2002, 1, 56–62. [Google Scholar]
- Baroni, B.M.; Ruas, C.V.; Ribeiro-Alvares, J.B.; Pinto, R.S. Hamstring-to-quadriceps torque ratios of professional male soccer players: A systematic review. J. Strength Cond. Res. 2020, 34, 2609. [Google Scholar] [CrossRef]
- Camarda, S.R.D.A.; Denadai, B.S. Does muscle imbalance affect fatigue after soccer specific intermittent protocol? J. Sci. Med. Sport 2012, 15, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Ford, K.R.; Myer, G.D.; Hewett, T.E. Longitudinal effects of maturation on lower extremity joint stiffness in adolescent athletes. Am. J. Sports Med. 2010, 38, 1829–1837. [Google Scholar] [CrossRef] [Green Version]
- Brughelli, M.; Cronin, J. A review of research on the mechanical stiffness in running and jumping: Methodology and implications. Scand. J. Med. Sci. Sports 2008, 18, 417–426. [Google Scholar] [CrossRef]
- Komi, P.V. Stretch-shortening cycle: A powerful model to study normal and fatigued muscle. J. Biomech. 2000, 33, 1197–1206. [Google Scholar] [CrossRef] [Green Version]
- Hewett, T.E.; Myer, G.D.; Ford, K.R. Anterior cruciate ligament injuries in female athletes: Part 1, mechanisms and risk factors. Am. J. Sports Med. 2006, 34, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.S.; Oliver, J.L.; Hughes, M.G.; Williams, C.A. Age-related differences in the neural regulation of stretch-shortening cycle activities in male youths during maximal and sub-maximal hopping. J. Electromyogr. Kinesiol. 2012, 22, 37–43. [Google Scholar] [CrossRef]
- Campa, F.; Silva, A.M.; Iannuzzi, V.; Mascherini, G.; Benedetti, L.; Toselli, S. The role of somatic maturation on bioimpedance patterns and body composition in male elite youth soccer players. Int. J. Environ. Res. Public Health 2019, 16, 4711. [Google Scholar] [CrossRef] [Green Version]
- Toselli, S.; Marini, E.; Maietta Latessa, P.; Benedetti, L.; Campa, F. Maturity related differences in body composition assessed by classic and specific bioimpedance vector analysis among male elite youth soccer players. Int. J. Environ. Res. Public Health 2020, 17, 729. [Google Scholar] [CrossRef] [Green Version]
- Barrett, S.; Guard, A.; Lovell, R.J. Elite-youth and university-level versions of SAFT90 simulate the internal and external loads of competitive soccer. In Science and Football VII; Nunome, H., Drust, B., Dawson, B., Eds.; Routledge: Abingdon, UK, 2013; pp. 95–100. [Google Scholar]
- Botek, M.; Krejčí, J.; McKune, A.J.; Klimešová, I. Somatic, endurance performance and heart rate variability profiles of professional soccer players grouped according to age. J. Hum. Kinet. 2016, 54, 65–74. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Age (y) | PHV Offset (y) | Stature (cm) | Body Mass (kg) |
|---|---|---|---|---|
| U16 year 1 | 16.0 ± 0.4 | +2.24 ± 0.71 | 178.8 ± 6.4 | 67.5 ± 7.8 |
| U17 year 2 | 17.0 ± 0.4 | +3.31 ± 0.57 | 180.9 ± 5.7 | 71.4 ± 6.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehnert, M.; De Ste Croix, M.; Zaatar, A.; Lipinska, P.; Stastny, P. Effect of a Simulated Match on Lower Limb Neuromuscular Performance in Youth Footballers—A Two Year Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 8579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228579
Lehnert M, De Ste Croix M, Zaatar A, Lipinska P, Stastny P. Effect of a Simulated Match on Lower Limb Neuromuscular Performance in Youth Footballers—A Two Year Longitudinal Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228579
Chicago/Turabian StyleLehnert, Michal, Mark De Ste Croix, Amr Zaatar, Patrycja Lipinska, and Petr Stastny. 2020. "Effect of a Simulated Match on Lower Limb Neuromuscular Performance in Youth Footballers—A Two Year Longitudinal Study" International Journal of Environmental Research and Public Health 17, no. 22: 8579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228579