Cost-Effectiveness Analysis from a Randomized Controlled Trial of Tailored Exercise Prescription for Women with Breast Cancer with 8-Year Follow-Up

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Intervention and Comparator
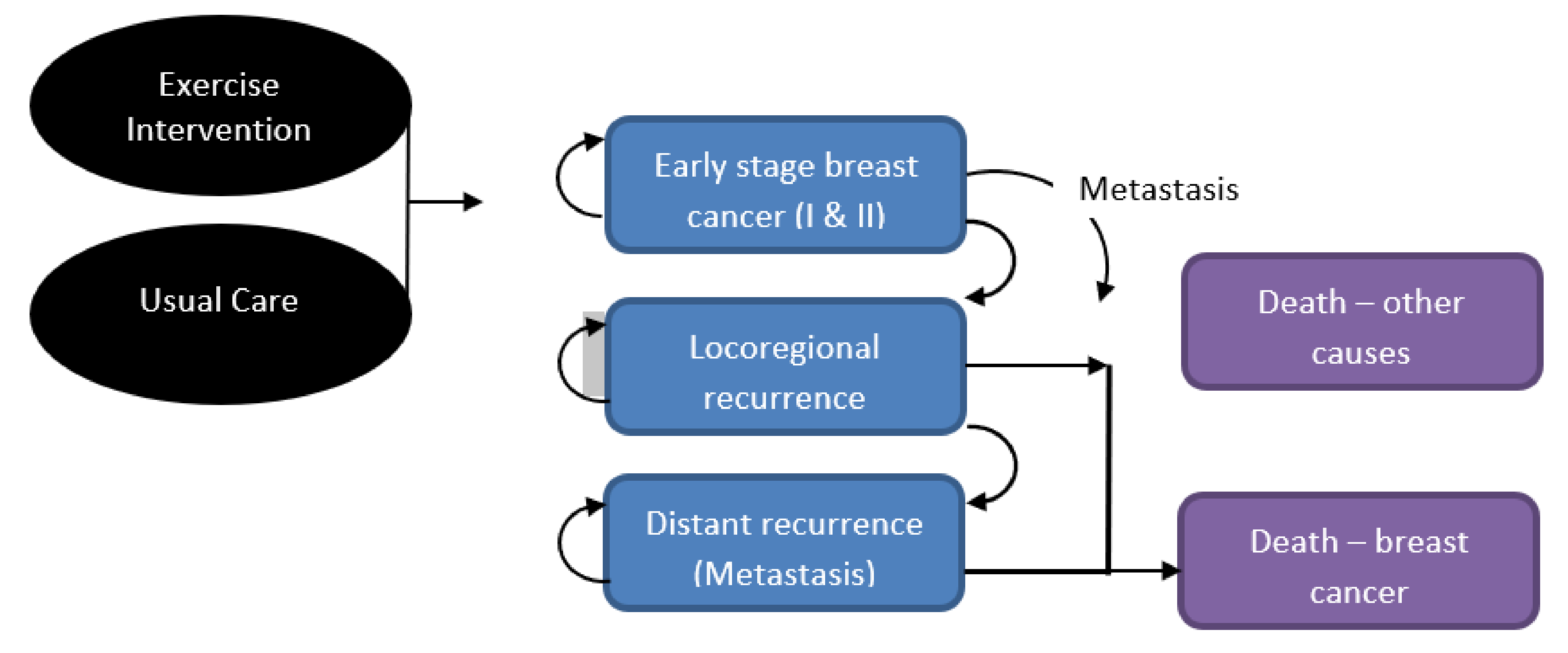
2.3. Model Structure
2.4. Data Inputs
2.5. Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Agency for Research on Cancer (WHO). Global Cancer Observatory; IARC: Lyon, France, 2020. [Google Scholar]
- Australian Institute of Health and Welfare (AIHW). Cancer in Australia: In Brief 2019; AIHW: Canberra, Australia, 2019. [Google Scholar]
- Australian Institute of Health and Welfare (AIHW). Cancer in Australia 2019 Cat. No. CAN 123. Available online: https://meteor.aihw.gov.au/content/index.phtml/itemId/698954 (accessed on 20 October 2020).
- Heer, E.; Harper, A.; Escandor, N.; Sung, H.; McCormack, V.; Fidler-Benaoudia, M.M. Global burden and trends in premenopausal and postmenopausal breast cancer: A population-based study. Lancet Glob. Health 2020, 8, e1027–e1037. [Google Scholar] [CrossRef]
- Kenyon, M.; Mayer, D.K.; Owens, A.K. Late and long-term effects of breast cancer treatment and surveillance management for the general practitioner. J. Obstet. Gynecol. Neonatal. Nurs. 2014, 43, 382–398. [Google Scholar] [CrossRef]
- Islam, T.; Dahlui, M.; Majid, H.A.; Nahar, A.M.; Mohd Taib, N.A.; Su, T.T. Factors associated with return to work of breast cancer survivors: A systematic review. BMC Public Health 2014, 14 (Suppl. S3), S8. [Google Scholar] [CrossRef] [Green Version]
- Demark-Wahnefried, W.; Schmitz, K.H.; Alfano, C.M.; Bail, J.R.; Goodwin, P.J.; Thomson, C.A.; Bradley, D.W.; Courneya, K.S.; Befort, C.A.; Denlinger, C.S.; et al. Weight management and physical activity throughout the cancer care continuum. CA Cancer J. Clin. 2018, 68, 64–89. [Google Scholar] [CrossRef]
- Cormie, P.; Adams, D.; Atkinson, M.; Bucci, L.; Cust, A.E.; Eakin, E.; McCarthy, A.L.; Murnane, A.; Quinn, S.; Hayes, S.C. Exercise as part of routine cancer care. Lancet Oncol. 2018, 19, e432. [Google Scholar] [CrossRef] [Green Version]
- Cormie, P.; Atkinson, M.; Bucci, L.; Cust, A.; Eakin, E.; Hayes, S.; McCarthy, S.; Murnane, A.; Patchell, S.; Adams, D. Clinical Oncology Society of Australia position statement on exercise in cancer care. Med. J. Aust. 2018, 209, 184–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvão, D.A. The Exercise and Sports Science Australia position statement: Exercise medicine in cancer management. J. Sci. Med. Sport. 2019, 22, 1175–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E.; et al. American College of Sports Medicine Roundtable Report on Physical Activity, Sedentary Behavior, and Cancer Prevention and Control. Med. Sci. Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical Activity and Mortality in Cancer Survivors: A Systematic Review and Meta-Analysis. JNCI Cancer Spectr. 2020, 4, pkz080. [Google Scholar] [CrossRef] [PubMed]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies. Acta Oncol. 2015, 54, 635–654. [Google Scholar] [CrossRef]
- Schmid, D.; Leitzmann, M.F. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: A systematic review and meta-analysis. Ann. Oncol. 2014, 25, 1293–1311. [Google Scholar] [CrossRef] [PubMed]
- Spei, M.E.; Samoli, E.; Bravi, F.; La Vecchia, C.; Bamia, C.; Benetou, V. Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast. 2019, 44, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Eakin, E.G.; Lawler, S.P.; Winkler, E.A.; Hayes, S.C. A randomized trial of a telephone-delivered exercise intervention for non-urban dwelling women newly diagnosed with breast cancer: Exercise for health. Ann. Behav. Med. 2012, 43, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, S.C.; Rye, S.; Disipio, T.; Yates, P.; Bashford, J.; Pyke, C.; Saunders, C.; Battistutta, D.; Eakin, E. Exercise for health: A randomized, controlled trial evaluating the impact of a pragmatic, translational exercise intervention on the quality of life, function and treatment-related side effects following breast cancer. Breast Cancer Res. Treat. 2013, 137, 175–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, S.C.; Steele, M.L.; Spence, R.R.; Gordon, L.; Battistutta, D.; Bashford, J.; Pyke, C.; Saunders, C.; Eakin, E. Exercise following breast cancer: Exploratory survival analyses of two randomised, controlled trials. Breast Cancer Res. Treat. 2018, 167, 505–514. [Google Scholar] [CrossRef]
- Khan, K.A.; Mazuquin, B.; Canaway, A.; Petrou, S.; Bruce, J. Systematic review of economic evaluations of exercise and physiotherapy for patients treated for breast cancer. Breast Cancer Res. Treat. 2019, 176, 37–52. [Google Scholar] [CrossRef] [Green Version]
- Gordon, L.G.; DiSipio, T.; Battistutta, D.; Yates, P.; Bashford, J.; Pyke, C.; Eakin, E.; Hayes, S.C. Cost-effectiveness of a pragmatic exercise intervention for women with breast cancer: Results from a randomized controlled trial. Psychooncology. 2017, 26, 649–655. [Google Scholar] [CrossRef]
- Haines, T.P.; Sinnamon, P.; Wetzig, N.G.; Lehman, M.; Walpole, E.; Pratt, T.; Smith, A. Multimodal exercise improves quality of life of women being treated for breast cancer, but at what cost? Randomized trial with economic evaluation. Breast Cancer Res. Treat. 2010, 124, 163–175. [Google Scholar] [CrossRef]
- May, A.M.; Bosch, M.J.; Velthuis, M.J.; van der Wall, E.; Steins Bisschop, C.N.; Los, M.; Erdkamp, F.; Bloemendal, H.J.; de Roos, M.A.; Verhaar, M.; et al. Cost-effectiveness analysis of an 18-week exercise programme for patients with breast and colon cancer undergoing adjuvant chemotherapy: The randomised PACT study. BMJ Open. 2017, 7, e012187. [Google Scholar] [CrossRef] [Green Version]
- Mewes, J.C.; Steuten, L.M.; Ijzerman, M.J.; van Harten, W.H. Effectiveness of multidimensional cancer survivor rehabilitation and cost-effectiveness of cancer rehabilitation in general: A systematic review. Oncologist 2012, 17, 1581–1593. [Google Scholar] [CrossRef] [Green Version]
- Perrier, L.; Foucaut, A.M.; Morelle, M.; Touillaud, M.; Kempf-Lépine, A.S.; Heinz, D.; Gomez, F.; Meyrand, R.; Baudinet, C.; Berthouze, S.; et al. Cost-effectiveness of an exercise and nutritional intervention versus usual nutritional care during adjuvant treatment for localized breast cancer: The PASAPAS randomized controlled trial. Support. Care Cancer. 2020, 28, 2829–2842. [Google Scholar] [CrossRef] [PubMed]
- van Waart, H.; van Dongen, J.M.; van Harten, W.H.; Stuiver, M.M.; Huijsmans, R.; Hellendoorn-van Vreeswijk, J.; Sonke, G.S.; Aaronson, N.K. Cost-utility and cost-effectiveness of physical exercise during adjuvant chemotherapy. Eur. J. Health Econ. 2018, 19, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Value Health. 2013, 16, e1–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philips, Z.; Bojke, L.; Sculpher, M.; Claxton, K.; Golder, S. Good practice guidelines for decision-analytic modelling in health technology assessment: A review and consolidation of quality assessment. Pharmacoeconomics 2006, 24, 355–371. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.; Rye, S.; Battistutta, D.; Yates, P.; Pyke, C.; Bashford, J.; Eakin, E. Design and implementation of the Exercise for Health trial—A pragmatic exercise intervention for women with breast cancer. Contemp. Clin. Trials. 2011, 32, 577–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Baig, A.; Kasymjanova, G.; Kafi, K.; Holcroft, C.; Mekouar, H.; Carbonneau, A.; Bahoric, B.; Sultanem, K.; Muanza, T. Pattern of Local Recurrence and Distant Metastasis in Breast Cancer By Molecular Subtype. Cureus 2016, 8, e924. [Google Scholar] [CrossRef] [Green Version]
- Wapnir, I.L.; Anderson, S.J.; Mamounas, E.P.; Geyer, C.E., Jr.; Jeong, J.H.; Tan-Chiu, E.; Fisher, B.; Wolmark, N. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in five National Surgical Adjuvant Breast and Bowel Project node-positive adjuvant breast cancer trials. J. Clin. Oncol. 2006, 24, 2028–2037. [Google Scholar] [CrossRef]
- Anderson, S.J.; Wapnir, I.; Dignam, J.J.; Fisher, B.; Mamounas, E.P.; Jeong, J.H.; Geyer, C.E., Jr.; Wickerham, D.L.; Costantino, J.P.; Wolmark, N. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in patients treated by breast-conserving therapy in five National Surgical Adjuvant Breast and Bowel Project protocols of node-negative breast cancer. J. Clin. Oncol. 2009, 27, 2466–2473. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Life Tables, States, Territories and Australia, 2016-2018 Cat. No. 3302.0.55.001; Commonwealth of Australia: Canberra, Australia, 2019. [Google Scholar]
- Surveillance, Epidemiology and End Results Program. Cancer Statistics, Cancer Stat. Facts: Female Breast Cancer; National Cancer Institute: Bethesda, Maryland, USA, 2020. [Google Scholar]
- Witteveen, A.; Kwast, A.B.; Sonke, G.S.; MJ, I.J.; Siesling, S. Survival after locoregional recurrence or second primary breast cancer: Impact of the disease-free interval. PLoS ONE. 2015, 10, e0120832. [Google Scholar] [CrossRef] [Green Version]
- Verry, H.; Lord, S.J.; Martin, A.; Gill, G.; Lee, C.K.; Howard, K.; Wetzig, N.; Simes, J. Effectiveness and cost-effectiveness of sentinel lymph node biopsy compared with axillary node dissection in patients with early-stage breast cancer: A decision model analysis. Br. J. Cancer. 2012, 106, 1045–1052. [Google Scholar] [CrossRef] [Green Version]
- Cancer Australia. Clinical Practice Guidelines: Recommendations for Follow-Up for Women with Early Breast Cancer; Cancer Australia: Sydney, Australia, 2011. [Google Scholar]
- Reeve, R.; Srasuebkul, P.; Langton, J.M.; Haas, M.; Viney, R.; Pearson, S.A. Health care use and costs at the end of life: A comparison of elderly Australian decedents with and without a cancer history. BMC Palliat. Care 2017, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Deloitte Access Economics. Financial Impact of Breast Cancer in Australia. A report for Breast Cancer Network Australia; Deloitte Access Economics: Sydney, Australia, 2016. [Google Scholar]
- Carter, H.E.; Schofield, D.J.; Shrestha, R. The Productivity Costs of Premature Mortality Due to Cancer in Australia: Evidence from a Microsimulation Model. PLoS ONE 2016, 11, e0167521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Government. Employee Earnings and Hours, Australia Jan 2019; Australian Government: Canberra, Australia, 2019. [Google Scholar]
- Paracha, N.; Thuresson, P.O.; Moreno, S.G.; MacGilchrist, K.S. Health state utility values in locally advanced and metastatic breast cancer by treatment line: A systematic review. Expert Rev. Pharm. Outcomes Res. 2016, 16, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Fleurence, R.L.; Hollenbeak, C.S. Rates and probabilities in economic modelling: Transformation, translation and appropriate application. Pharmacoeconomics 2007, 25, 3–6. [Google Scholar] [CrossRef]
- Government, A. The Pharmaceutical Benefits Advisory Committee Guidelines Version 5.0; Australian Government: Canberra, Australia, 2016. [Google Scholar]
- Ibrahim, E.M.; Al-Homaidh, A. Physical activity and survival after breast cancer diagnosis: Meta-analysis of published studies. Med. Oncol. 2011, 28, 753–765. [Google Scholar] [CrossRef]
- Cavarretta, E.; Mastroiacovo, G.; Lupieri, A.; Frati, G.; Peruzzi, M. The Positive Effects of Exercise in Chemotherapy-Related Cardiomyopathy. Adv. Exp. Med. Biol 2017, 1000, 103–129. [Google Scholar] [CrossRef]
- Spence, R.R.; DiSipio, T.; Schmitz, K.; Hayes, S. Is unsupervised exercise following breast cancer safe for all women? Int. J. Phys. Med. Rehabil. 2014, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Crosland, P.; Ananthapavan, J.; Davison, J.; Lambert, M.; Carter, R. The economic cost of preventable disease in Australia: A systematic review of estimates and methods. Aust. N. Z. J. Public Health. 2019, 43, 484–495. [Google Scholar] [CrossRef]
- Gmeinder, M.; Morgan, D.; Mueller, M. How Much Do OECD Countries Spend on Prevention? Organisation for Economic Co-operation and Development: Paris, France, 2017. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Mean | Low | High | Source |
|---|---|---|---|---|
| Age entering the cycle (years) | 52 | 44 | 60 | EfH trial, Hayes 2018 [18] |
| Annual transition probabilities | ||||
| Early stage to distant recurrence | 0.018 | 0.016 | 0.019 | Wu 2016 [29] |
| Early stage to local recurrence | 0.007 | 0.006 | 0.007 | As above |
| Local recurrence to distant | 0.0997 | 0.0897 | 0.1097 | Wapnir 2006 [30] & Anderson 2009 [31] |
| Death from all causes (by age) | Table | Values differ by age | Supplementary File, Life tables, female [32] | |
| Death from distant recurrence | 0.230 | 0.207 | 0.253 | SEER data [33] |
| Death from local recurrence | 0.069 | 0.006 | 0.007 | Witteveen 2014 [34] |
| Trial-based probabilities | ||||
| Non-BrC mortality for exercise intvn | 0.0006 | 0.0000 | 0.0032 | EfH trial, Hayes 2018 [18] |
| Non-BrC mortality for usual care | 0.0047 | 0.0015 | 0.0110 | As above |
| BrC mortality for exercise intvn | 0.0059 | 0.0028 | 0.0109 | As above |
| BrC mortality for usual care | 0.0096 | 0.0046 | 0.0176 | As above |
| BrC recurrence in exercise intvn | 0.0072 | 0.0037 | 0.0125 | As above |
| BrC recurrence in usual care | 0.0076 | 0.0033 | 0.0150 | As above |
| Costs (AU$) | ||||
| Exercise intervention | 1344 | 1209 | 1478 | EfH trial, Gordon 2017 [20] |
| Local recurrence | 8679 | 7811 | 9547 | Verry 2012 [35] |
| Distant recurrence | 27,677 | 24,900 | 30,434 | As above |
| BrC survivors’ follow-up care | Table | Values differ by year post dx | Supplementary File [36] | |
| End-of-life—BrC | 25,475 | 22,928 | 28,023 | Reeve 2017 [37] |
| End of life—other causes | 12,122 | 10,910 | 13,334 | As above |
| Out-of-pocket expenses (annual) | 2538 | 797 | 9079 | Deloitte 2016 [38], first 2 years only |
| Costs of productivity losses (AU$) from | ||||
| Premature death from breast cancer | 149,909 | 134,918 | 164,900 | Carter 2016 [39] |
| Distant recurrence | 34,719 | 31,248 | 38,191 | Deloitte 2016 [38,40] |
| Local recurrence | 22,785 | 20,506 | 25,063 | As above |
| BrC early stage | 10,850 | 9765 | 11,935 | As above |
| Carers for metastases | 56,419 | 50,777 | 62,061 | As above |
| Carers for locoregional cancer | 29,295 | 26,365 | 32,224 | As above |
| Carers for no recurrence/early stage | 2170 | 1953 | 2387 | As above |
| Health utilities (quality of life) | ||||
| Utility for women at baseline | 0.818 | 0.718 | 0.918 | Paracha 2016 [41] |
| Additional utility with exercise program | 0.070 | 0.040 | 0.10 | EfH trial, Gordon 2017 [20], first year only |
| Additional utility with usual care | 0.020 | 0.000 | 0.06 | As above |
| Utility for local recurrence | 0.670 | 0.567 | 0.767 | Paracha 2016 [41] |
| Utility for distant recurrence | 0.640 | 0.540 | 0.74 | “ |
| Utility for terminal BrC | 0.514 | 0.414 | 0.614 | “ |
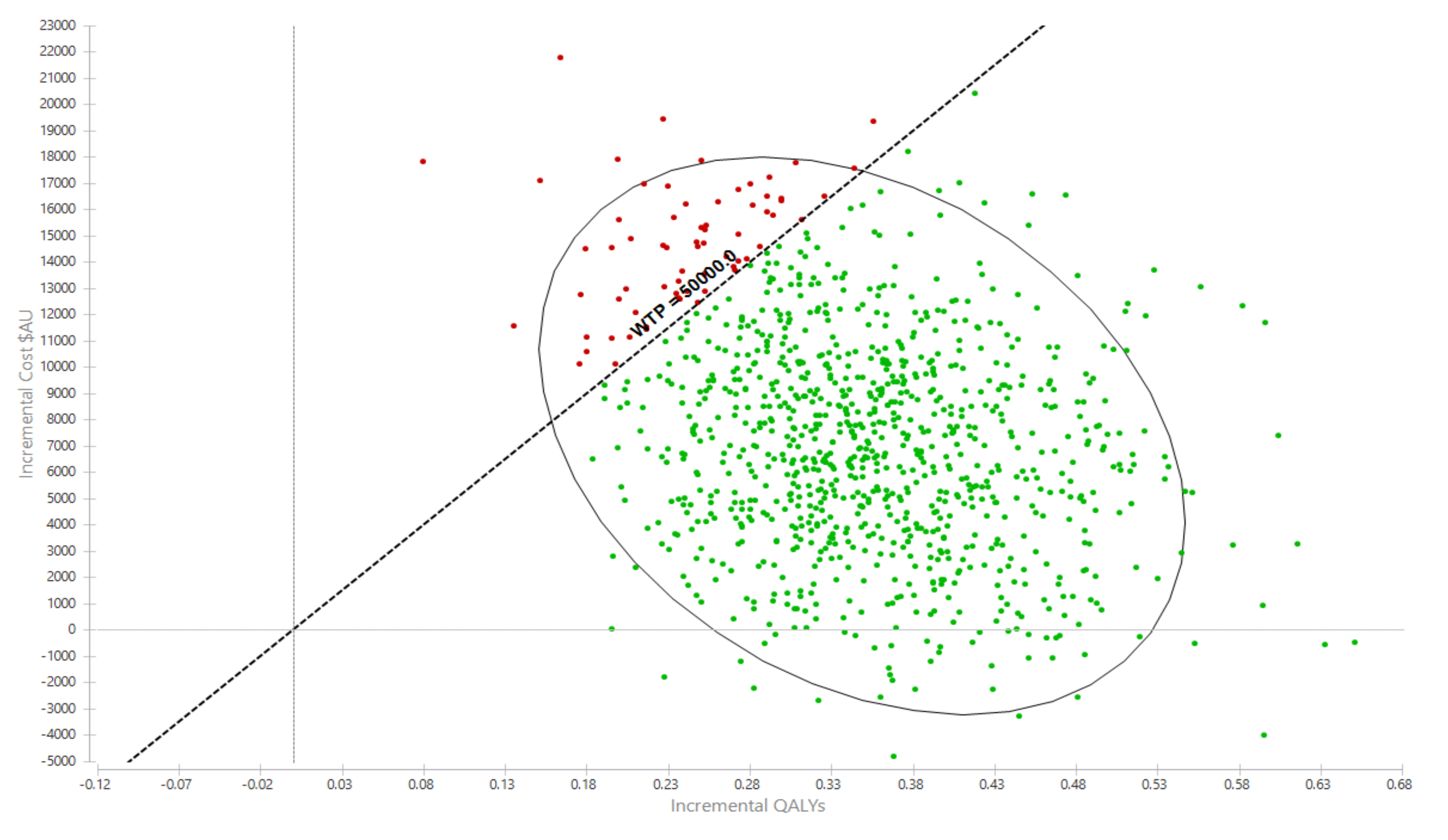
| Exercise | Usual Care | Incremental | 95% UI | |
|---|---|---|---|---|
| Mean | Mean | Difference | ||
| Costs | $281,445 | $274,035 | $7409 | Cost-saving, $16,275 |
| QALYs | 10.97 | 10.63 | 0.35 | 0.20, 0.52 |
| Life-years | 25.64 | 24.82 | 0.82 | 0.39, 1.4 |
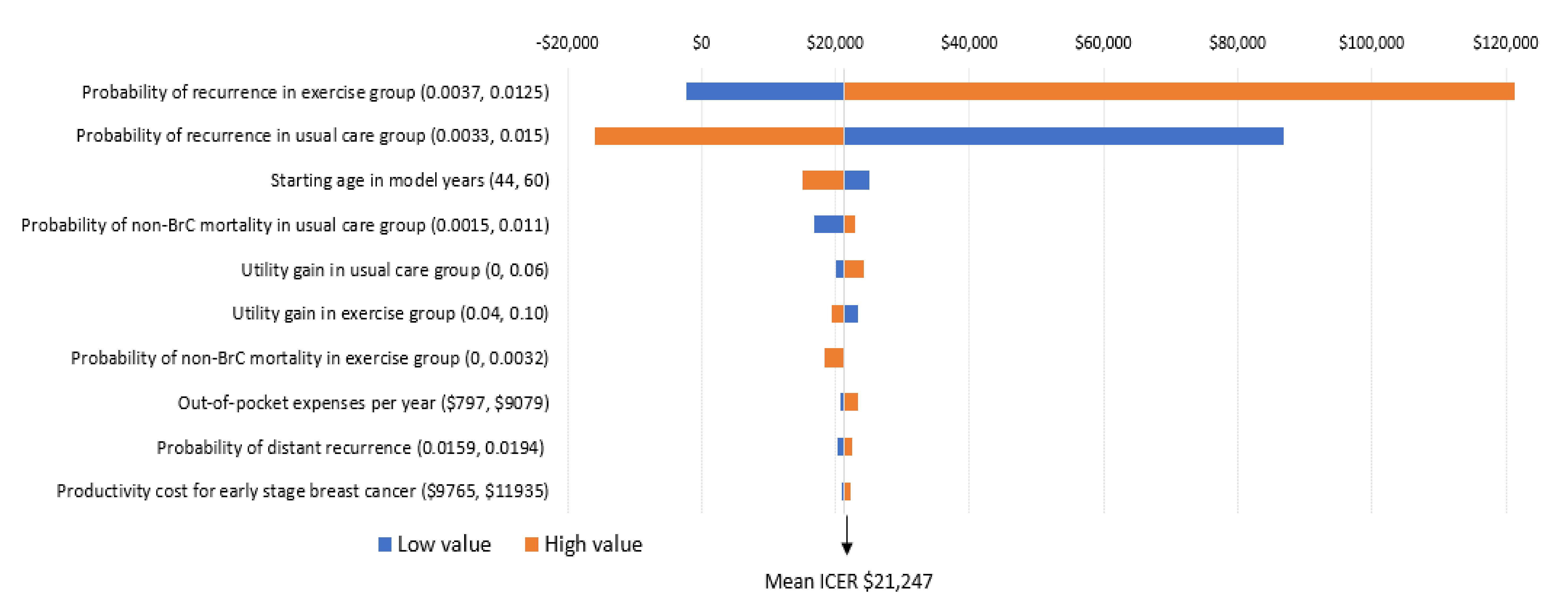
| Incremental cost per QALY | - | - | $21,247 | Dominant 1, $31,398 |
| Incremental cost per life-year saved | - | - | $8894 | Dominant 1, $11,769 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gordon, L.G.; Eakin, E.G.; Spence, R.R.; Pyke, C.; Bashford, J.; Saunders, C.; Hayes, S.C. Cost-Effectiveness Analysis from a Randomized Controlled Trial of Tailored Exercise Prescription for Women with Breast Cancer with 8-Year Follow-Up. Int. J. Environ. Res. Public Health 2020, 17, 8608. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228608
Gordon LG, Eakin EG, Spence RR, Pyke C, Bashford J, Saunders C, Hayes SC. Cost-Effectiveness Analysis from a Randomized Controlled Trial of Tailored Exercise Prescription for Women with Breast Cancer with 8-Year Follow-Up. International Journal of Environmental Research and Public Health. 2020; 17(22):8608. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228608
Chicago/Turabian StyleGordon, Louisa G., Elizabeth G. Eakin, Rosalind R. Spence, Christopher Pyke, John Bashford, Christobel Saunders, and Sandra C. Hayes. 2020. "Cost-Effectiveness Analysis from a Randomized Controlled Trial of Tailored Exercise Prescription for Women with Breast Cancer with 8-Year Follow-Up" International Journal of Environmental Research and Public Health 17, no. 22: 8608. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228608